

Abstract
The absence or decrease in sleep time can affect different mechanisms associated with changes in body composition and physical exercise performance. However, it is unclear in the literature how chronically sleep-restricted individuals respond to strength training. Thus, this study aimed to evaluate the effects of reducing between one and two hours of recommended sleep time (7 hours) on the response to resistance training. The study included 12 subjects who slept on average 2 hours less than the recommended 7 hours per day (42 ± 8 years; 84.9 ± 11.6 kg; 27.9 ± 3.5 kg/m 2 ; 6:17 ± 22 total sleep time/day and 5: 47 ± 29 sleep time/night) and 12 subjects with recommended sleep time (38 ± 11 years; 78.3 ± 9.5 kg; 25.1 ± 3.5 kg/m 2 ; 7:47 ± 38 total sleep time/day and 7:16 ± 54 sleep time/night) and a control group (42 ± 7 years; 81 ± 12.2 kg; 26.2 ± 4.0 kg/m 2 ; 7:30 ± 40 total sleep time/day and 7: 17 ± 51 sleep time/night) that did not perform resistance training. A total of 16 resistance training sessions were performed, 3 times a week (Sessions= 4 exercises; 2 sets; maximum repetitions to failure). The maximum number of repetitions, arm circumference, and arm muscle area increased, while triceps skinfold decreased after training in the experimental groups ( p < 0.05), with no changes for the control group. There was no difference in muscle mass, body mass index, or sleep variables (sleep time, latency, efficiency) after the training period in either group (p> 0.05). Thus, the chronic 1–2-hour reduction in average recommended sleep time was not able to affect the positive effects of resistance training.
Keywords: recovery, adaptation, performance
Introduction
It is already well established in the literature that resistance training increases muscle strength, lean body mass, and other adaptations in body composition. 1 There are different means of resistance training, but the most used include specific equipment (i.e., gym machines), free weights (barbells, weight plates, and dumbbells), and elastic bands that generate resistance against movement when extended. Although the effects on strength and body composition are similar, 2 3 elastic bands have the advantage of being easily transported and used in different places (e.g., school, home, or work), and at a lower cost.
On the other hand, a decrease in sleep time can negatively interfere with adaptations to physical training. There are currently many individuals with sleep restrictions, especially among workers in urban areas. 4 5 Research has indicated that a large part of the population (∼30%) sleeps less than 6 hours a day and that the total sleep time has decreased over the decades. 6 7 Decreases in sleep time over the years seem to be a reality in modern society. For example, previous research has shown that there has been a decline of between 1.5 and 2 hours of sleep time in the U.S over the past 50 years. 7 Data from 690,747 young people aged 5–18 from 20 countries indicated a reduction of more than 1 hour of sleep per night between the period 1905–2008. 8 A study performed with residents of a large Brazilian city showed that 28% of the 2618 respondents slept less than 6 hours or less a day. 9
Studies have shown that a long sleep deprivation period can affect the neuroendocrine system and muscle tissue. Dattilo et al. (2012) 10 found a reduction in mass and cross-sectional area of the tibialis anterior muscle, a reduction in testosterone, and an increase in corticosterone in rats after 96 hours of sleep deprivation. Mônico-Neto et al. (2015) 11 also found a reduction in the cross-sectional area of the long flexor finger muscles, tibialis anterior, and gastrocnemius in rats with 96 hours of sleep deprivation. Giampa et al. (2016) 12 found similar results, where there was a reduction in the anabolic hormones IGF-1 and testosterone and an increase in the catabolic hormone corticosterone after 96 hours of sleep deprivation in rats.
Evidence for the negative effects of sleep deprivation also applies to humans. Dattilo et al. (2020) 13 showed that 48 hours of sleep deprivation followed by 12 hours of sleep did not modify muscle recovery but modified the inflammatory (IL-6) and hormonal (IGF-1 and cortisol) response after an eccentric action resistance exercise. Nedeltcheva et al. (2010) 14 found a greater reduction in muscle mass and less reduction in fat mass in subjects who slept 5.5 hours, compared with 8.5 hours of sleep at the end of 14 days. In addition, previous studies indicate that individuals with changes in bedtime and restricted sleep have a higher prevalence of overweight and obesity. 15
In addition to the worsening of some neuroendocrine mechanisms and changes in body composition, the sleep recovery role can be indirectly perceived by the increase in the fatigue state, decrease in vigor and performance in different physical exercise protocols after a reduction of 3 or more hours of sleep per night and one or more days of sleep deprivation. 16 In general, worsening in these performance parameters would be related to greater difficulty in accessing energy sources, vital for exercise and metabolic balance. 17 For example, Leproult and Van-Cuter (2011) 18 found a reduction of around 10–15% in circulating testosterone after a 3-hour reduction in usual sleep time in healthy adults, suggesting that negative effects do not only apply to complete sleep deprivation. Therefore, despite not being a concession, the decrease in sleep time can lead to a state of incomplete recovery and consequently impair adaptations to physical exercise (Fullagar et al., 2015). 16
As seen, the literature is rich regarding the effects of an acute deprivation period and on the physiological adaptations to exercise, but it is scarce regarding the chronic effects in individuals with light sleep restriction (∼2 hours), which is considered a more frequent type of sleep restriction 6 17 in response to resistance training. Thus, studies regarding sleep duration have become of great importance in public health. Today, researchers and health professionals consider the value of 7 hours as the lower limit for quality and restorative sleep and health maintenance. 19 However, an important part of the world population, probably due to their work needs, has a total daily sleep time below the recommended value of 7 hours. 5 6 Thus, it is not yet known whether the reduction of close to 2 hours in the recommended sleep time interferes with the benefits of physical training. Therefore, the objective of this study is to verify whether the chronic reduction of around 2 hours of sleep from the recommended amount of 7 hours interferes with strength and body composition responses to resistance training.
Material and Methods
Participants
Thirty-six men were given written consent for research. The sample size was determined a priori using the GPower software program (version 3.1.2; Franz Faul, Universitat Kiel, Germany), considering the following specifications: effect size f = 0.3; α = 0.05; (1-β) = 0.8; test family= Anova with repeated measures inside and outside the group and interaction. The subjects who accepted to be part of the study were then considered participants if they met the following inclusion criteria: a) have an adequate health status as suggested by the PAR-Q questionnaire to point out possible limitations regarding the practice of physical exercises; b) subjects who do not practice or have regularly practiced resistance training in the last year, or any other systematic program of physical exercise or manual work; c) volunteers who do not present possible sleep disorders as suggested by the Pittsburgh questionnaire; and d) volunteers who do not have limitations to practice the aforementioned exercises. Participants who: a) for some reason had some difficulty performing the exercise protocol during the intervention period; b) did not attend at least 90% of the training sessions; or c) maintained a frequency of two or fewer times a week were excluded from the study.
Experimental Design
This is an experimental and longitudinal study, in which the volunteers were divided into three groups (12 participants each): a group that sleeps on average less than 7 hours (∼ -2h less) (<7h); group that sleeps a little more than 7 hours (7h); and control (CON) that sleeps on average more than 7 hours and did not perform resistance training. The <7h and 7h groups performed 16 elastic band (EB) resistance training sessions, 3 times a week. The effects of the intervention were evaluated through pre- and post-training measures: a) Body mass; b) Body mass index (BMI); and c) Arm muscle area (AMA) and maximum repetition number (MRN).
Procedures
The participants answered the Pittsburgh Sleep Quality Questionnaire 20 on the first day, and their height, body mass, triceps skinfold, and arm circumference were estimated. Then, an actigraph was placed on their non-dominant arm. Next, they were familiarized with the elastic band exercises. After familiarization, the exercise protocol was performed to determine the pre-training MRN, which consisted of selecting the number and color of the bands that would be used during training for each of the following exercises: a) shoulder abduction, b) seated rowing, and c) bicep curls. In addition to the exercises using the elastic bands, push-ups were added without using elastic bands, in which the participant should perform as many repetitions as possible. Two days later, participants in the <7h and 7h group started training sessions with a frequency of 3 times a week and 48 hours of rest between sessions. The pre-training measurements were performed again by the same evaluator two days after the last session and at the same time as the pre-training assessment. Participants were instructed to maintain their eating and sleeping habits throughout the intervention period. The interventions were performed in the afternoon (2:00–4:00 pm ). The ethics committee on research involving humans, Universidade Federal de Minas Gerais , approved the study (Approval number 1.305.678).
Measurements
Sleep quality was assessed using the Pittsburgh questionnaire, which allows for classifying the individual as having good or poor sleep quality. 20 The sleep time, sleep latency, and sleep efficiency were evaluated using the actigraphy technique. 21 The actigraph remained on the participant's arm during the first and last week of intervention.
Total body mass (kg) was measured with the volunteer wearing light clothes and barefoot (Serene ® digital scale, Brazil). Height was measured by attaching a measuring tape to the wall from the floor to the ceiling. The barefoot participant stood with their back to the wall so that the tape was along their spine. Body mass index (BMI) was calculated by dividing body mass in kg by height in meters squared.
The arm muscle area (AMA) was estimated according to the protocol by Frisancho (1981) 22 in which the arm circumference and the triceps skinfold are the measurements used in the equation: AMA= (c-πT)2/4π; In which: c is the arm circumference in mm and T is the triceps skinfold in mm. The triceps skinfold was measured using a digital adipometer (Cescorf ® , USA). 22 The arm circumference was measured with a measuring tape. All procedures were performed by a single researcher.
Familiarization with Elastic Band Exercises
To familiarize and correct failures in the execution of the exercises by the participants before the exercises to determine the initial training intensity, each exercise was preceded by 10 repetitions with a low-tension elastic band (red color). The purpose of using a “lightweight” elastic band was to avoid a possible fatigue effect and to facilitate the movement.
Maximum Number of Repetitions Pre and Post Training
For the initial training load to be equalized among the participants, the maximum number of target repetitions reached at the point of voluntary failure was determined by combining the amount and color of the elastic bands. The participants performed 10 maximum repetitions (acceptable range of 9–11 repetitions) for the shoulder abduction and elbow flexion exercise, and 20 maximum repetitions (acceptable range of 18 to 22 repetitions) for the seated row exercise. If the participant did not reach the lower limit or exceeded the upper limit of repetitions, the researcher modified the number or changed the color of the elastic band so that the participant reached failure within the accepted repetition range. The push-up exercise was performed without an elastic band and a predetermined maximum number of repetitions until failure due to the load of their body weight. The interval between each attempt per exercise and between exercises was 4 minutes. The exercises were performed lasting 1 second for the concentric phase and 2 seconds for the eccentric phase. The order of the exercises was: 1st shoulder abduction; 2nd arm flexion; 3rd seated row; 4th elbow flexion. More details of the exercises can be seen in Figure 1A-D .
Fig. 1.
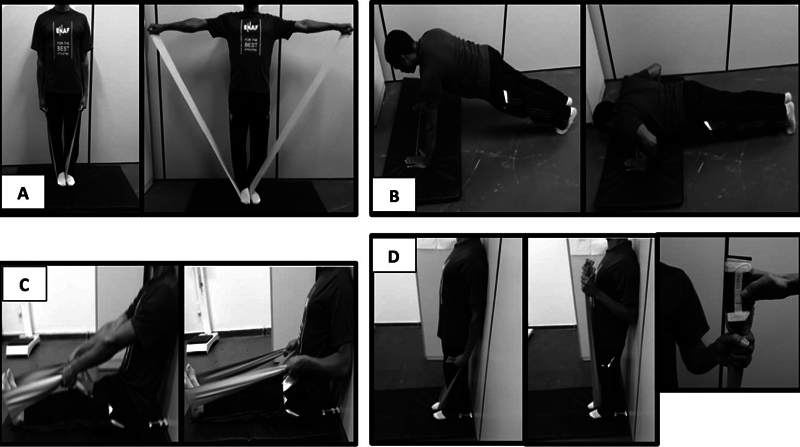
(A) Shoulder abduction; (B) Push-Up; (C) Seat rowing; (D) Biceps curl.
The maximum number of post-training repetitions followed the same protocol and elastic bands used pre-training. Participants were instructed and verbally encouraged to perform as many repetitions as possible. All exercises were performed with TheraBand ® (USA) elastic bands in gold, silver, and black colors. According to the manufacturer, the values at 100% (maximum) stretching are 6.5 kg, 4.6 kg, and 3.3 kg for the gold, silver, and black colors, respectively.
Training Protocol
The training sessions consisted of the same exercises in the same order and execution time as the MRN tests, however, with 2 sets for each exercise with a one-minute rest between sets and a two-minute interval between exercises. Participants were encouraged to perform as many repetitions as possible during and with each new session. The exercise was interrupted when: a) the participants themselves interrupted the execution; or b) when they could not maintain the exception time/or the range of motion for more than three repetitions. Training sessions lasted 20 to 24 minutes.
Statistical Analysis
Data were expressed as mean ± standard deviation. Data normality was analyzed using the Shapiro-Wilk test. One-way ANOVA was used to characterize the sample by group in terms of body composition variables, maximum number of repetitions, pre-training sleep variables, and total load (kg) imposed by the elastic bands used. Possible differences were identified using the Bonferroni post hoc. The Chi-squared test was used to compare the frequency of sleep quality distribution using the Pittsburgh questionnaire between groups and time (3 × 2). Mixed-model ANOVA was used to compare variables between pre- and post-training groups. If a difference was found, the Bonferroni post hoc was used. The significance level adopted was p < 0.05. The analyses were performed using the SPSS 2.0 program. In addition, the size of Cohen's d effect was calculated by the difference between the pre-and post-training mean values, divided by the pooled standard deviation. The values found were defined as trivial (d< 0.19), small (0.2 < d < 0.49), medium (0.5 < d < 0.79), large (0.8 < d < 1 0.29), or very large (>1.3). 23
Results
Table 1 shows the baseline characteristics of each group regarding body composition, sleep variables, and muscle strength. The values related to sleep refer to the average of the seven initial days of recording by the actigraph. Total sleep time (TST) and mean nighttime sleep time (NS) per week were higher in the 7h and CON groups compared with the <7h group (p> 0.05). The awakening time was longer in the 7h group compared with the <7h group. There was no statistical difference for the other variables.
Table 1. Baseline characteristics of participants according to the group.
| Variables | Groups | ||||
|---|---|---|---|---|---|
| Control (n = 12) | 7h (n = 12) | <7h (n = 12) | F | p | |
| Age (years) | 42 ± 7 | 38 ± 11 | 42 ± 8 | 1.4 | 0.25 |
| Height (m) | 1.75 ± 0.05 | 1.78 ± 0.05 | 1.74 ± 0.04 | 0.89 | 0.40 |
| Body mass (kg) | 81 ± 12.2 | 78.3 ± 9.5 | 84.9 ± 11.6 | 1.0 | 0.38 |
| BMI (kg/h 2 ) | 26.2 ± 4.0 | 25.1 ± 3.5 | 27.9 ± 3.5 | 1.70 | 0.20 |
| Arm circumference (cm) | 33.4 ± 2.6 | 32.2 ± 3.8 | 33.0 ± 4.0 | 0.40 | 0.70 |
| Triceps skinfold (mm) | 11.5 ± 5.3 | 9.8 ± 4.1 | 11.7 ± 4.1 | 1.50 | 0.25 |
| Arm muscle area | 6826 ± 1160 | 6738 ± 1768 | 6985 ± 1878 | 0.07 | 0.93 |
| Actigraphy analyses | |||||
| TST (h: min) | 7: 30 ± 40* | 7: 47 ± 38* | 6: 17 ± 22 | 17.20 | <0.001 |
| NS (h: min) | 7: 17 ± 51* | 7: 16 ± 54* | 5: 47 ± 29 | 15.45 | <0.001 |
| Latency (min) | 12.2 ± 3.6' | 12.0 ± 3.7 | 19. ± 15.9 | 2.1 | 0.15 |
| Efficiency (%) | 83.46 ± 4.6 | 84.0 ± 5.8 | 88.1 ± 5.5 | 1.7 | 0.2 |
| Pittsburgh | |||||
| Good sleepers | 5 (42%) | 9 (75%) | 5 (42%) | χ 2 | |
| Poor sleepers | 7 (58%) | 3 (25%) | 7 (58%) | 2.92 | 0.23 |
| Strength | |||||
| Shoulder abduction (rep. n o ) | 10.7 ± 0.5 | 10.1 ± 0.8 | 10.4 ± 0.5 | 0.67 | 0.51 |
| Push-up (rep. n o ) | 15.9 ± 6.9 | 13.4 ± 4.0 | 11.2 ± 3.5 | 2.88 | 0.07 |
| Seated rowing (rep. n o ) | 20.2 ± 1.7 | 20.0 ± 1.4 | 20.1 ± 1.0 | 0.49 | 0.61 |
| Biceps curl (rep. n o ) | 10.6 ± 0.7 | 10.4 ± 0.7 | 10.2 ± 0.6 | 1.41 | 0.25 |
Abbreviations: BMI, Body mass index; NS, Night sleep; TST, Total sleep time.
(*) Height than <7h. χ 2 = Teste Chi-square. 7h= Group 7 sleep hours. <7h= Group than sleep less 7 hours.
Table 2 shows the distribution of colors and amount of pre-training elastic bands per participant, per exercise, and group. Although the present study does not have data on the degree of elastic band stretching imposed by the participants and that this degree of stretching depends on the participant's limb length, estimated load values will be presented, taking the values at 100% of elastic band stretching presented by the manufacturer as parameters. The aim is to identify the possible differences in the external resistance (in kg) between the groups for the same training load equalized by the maximum number of repetitions. Despite the variations in the amount and color combinations of the elastic bands used, there was no difference in the initial training load between the groups (F= 2.8; p = 0.07).
Table 2. Elastic bands used in training by group.
| Exercise | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Shoulder abduction (10RM) | Seated rowing (20RM) |
Biceps curl (10RM) |
|||||||||
| Band elastic colour | |||||||||||
| Group | Vol. | Gold (n o ) | Silver (n o ) | Black (n o ) | Gold (n o ) | Silver (n o ) | Black (n o ) | Gold (n o ) | Silver (n o ) | Black (n o ) | Carga total (kg) |
| CON | 1 | 1 | 3 | 2 | 1 | – | 2 | 1 | 51 | ||
| 2 | 1 | 3 | 3 | 1 | 2 | 56.1 | |||||
| 3 | 1 | 3 | 2 | 2 | 1 | 51.5 | |||||
| 4 | 1 | 3 | 3 | 1 | 2 | 56.1 | |||||
| 5 | 1 | 3 | 3 | 2 | 1 | 57.4 | |||||
| 6 | 1 | 3 | 2 | 2 | 44.4 | ||||||
| 7 | 1 | 3 | 1 | 1 | 40.4 | ||||||
| 8 | 1 | 3 | 2 | 2 | 57.4 | ||||||
| 9 | 1 | 3 | 4 | 2 | 57.4 | ||||||
| 10 | 1 | 1 | 3 | 4 | 2 | 58.8 | |||||
| 11 | 1 | 3 | 2 | 1 | 1 | 1 | 49.3 | ||||
| 12 | 1 | 3 | 3 | 1 | 1 | 1 | 54.3 | ||||
| Total | 11 | 1 | 1 | 36 | 30 | 5 | 16 | 8 | 3 | 52.8 ± 5.7 | |
| 7h | 1 | 1 | 3 | 2 | 2 | 44.5 | |||||
| 2 | 1 | 1 | 3 | 4 | 2 | 58.8 | |||||
| 3 | 1 | 3 | 3 | 2 | 62 | ||||||
| 4 | 1 | 3 | 3 | 2 | 62 | ||||||
| 5 | 1 | 3 | 2 | 2 | 57.6 | ||||||
| 6 | 1 | 1 | 3 | 3 | 1 | 2 | 1 | – | 62.1 | ||
| 7 | 1 | 3 | 2 | 1 | 2 | 1 | 41.8 | ||||
| 8 | 1 | 3 | 3 | 1 | 2 | 1 | 59.4 | ||||
| 9 | 1 | 3 | 3 | 2 | 52.8 | ||||||
| 10 | 1 | 3 | 1 | 1 | 33.9 | ||||||
| 11 | 1 | 3 | 2 | 2 | 48.2 | ||||||
| 12 | 1 | 3 | 3 | 2 | 52.8 | ||||||
| Total | 10 | 2 | 2 | 36 | 23 | 3 | 18 | 6 | 3 | 52.9 ± 9.2 | |
| <7h | 1 | 1 | 2 | 2 | 1 | 1 | 39.8 | ||||
| 2 | 1 | 2 | 2 | 1 | 1 | 39.8 | |||||
| 3 | 1 | 2 | 2 | 1 | 1 | 38.5 | |||||
| 4 | 1 | 1 | 3 | 3 | 2 | 56.1 | |||||
| 5 | 1 | 1 | 3 | 3 | 1 | 2 | 1 | 60.8 | |||
| 6 | 1 | 1 | 2 | 2 | 1 | 1 | 1 | 33.4 | |||
| 7 | 1 | 3 | 3 | 2 | 1 | 56.1 | |||||
| 8 | 1 | 3 | 1 | 1 | 1 | 1 | 43.7 | ||||
| 9 | 1 | 3 | 1 | 1 | 1 | 1 | 43.7 | ||||
| 10 | 1 | 3 | 2 | 1 | 1 | 1 | 49.6 | ||||
| 11 | 1 | 3 | 2 | 2 | 46.3 | ||||||
| 12 | 1 | 3 | 2 | 2 | 48.2 | ||||||
| Total | 9 | 3 | 3 | 32 | 23 | 5 | 17 | 3 | 6 | 46.3 ± 8.2 | |
Abbreviation: CON, control group.
According to the manufacturer, the values at 100% stretch are 6.5 kg, 4.6 kg and 3.3 kg for the gold, silver and black colors, respectively. 7h= Group 7 sleep hours. <7h= Group than sleep less 7 hours.
Fig. 2 shows the MRN for each exercise between the pre-and post-training groups. The MRN was higher post compared with pre-training for the <7h and 7h groups in the shoulder abduction, biceps curl, push-up, and seated row exercises. At the post-training moment, the MRN in the groups 7h and <7h was higher than CON for the shoulder abduction and biceps curl exercise. There was no difference between the 7h and <7h groups at post-training time. The 7h group had higher MRN in the seated rowing exercise compared with the CON and <7h groups. Moreover, the MRN was higher in the push-up exercise than the CON only for the 7h group.
Fig. 2.
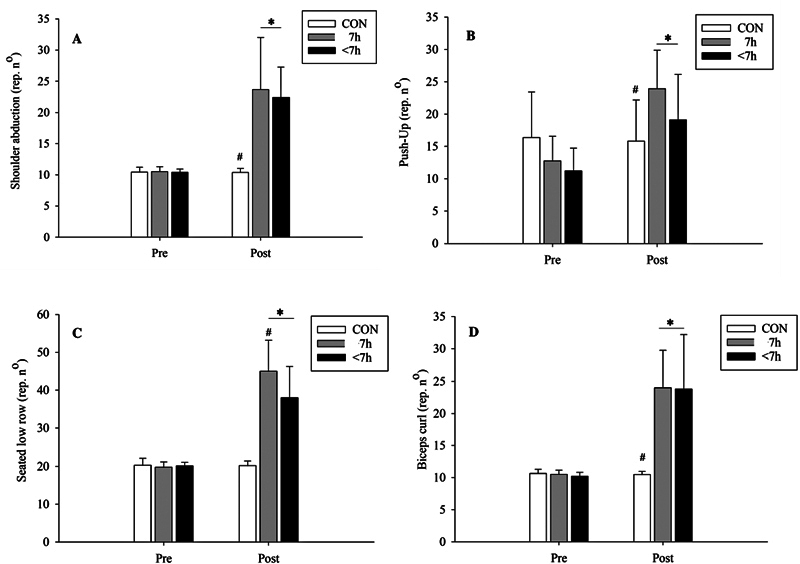
Mean and standard deviation of maximal repetition number. (A) Shoulder abduction pre- and post-training among groups (CON= control group; 7h= Group that sleeps 7 hours; <7h= Group that sleeps less than 7 hours). ANOVA. Interaction: F= 19.6; p< 0.001; 1-β= 1.0. (*) higher than pre-training. ( # ) less than <7h and 7h post-training. (B) Push-Up pre- and post-training among groups. ANOVA. Interaction: F= 19.4; p< 0.001; 1-β= 1.0. (*) higher than pre-training. ( # ) less than 7 hours post-training. (C) Seated low-row pre- and post-training among groups. ANOVA. Interaction: F= 28.4; p< 0.001; 1-β= 1.0. (*) higher than pre-training. ( # ) less than <7h and 7h post-training. (D) Biceps curl pre- and post-training among groups. ANOVA. Interaction: F= 24.8; p< 0.001; 1-β= 1.0. (*) higher than pre-training. ( # ) less than <7h and 7h post-training.
Fig. 3 shows the effects of the training period on the body composition according to the group. There was no training or group effect for body mass and BMI variables. Arm circumference and AMA were higher posts compared with pre-training in the <7h and 7h groups. Triceps skinfold was lower post compared with pre-training in the <7h and 7h groups and was higher in the <7h compared with the 7h group. However, there was an interaction between the factors (group x moment) for the arm circumference, triceps skinfold thickness, and AMA variables ( p < 0.05). The arm circumference was greater post compared with pre-training in the groups 7h (Pre= 32.2 ± 3.8 versus Post= 33.4 ± 3.7; p < 0.001) and <7h (Pre= 33, 0 ± 4.0 vs Post= 33.7 ± 3.7; p < 0.001). The triceps skinfold thickness was lower post compared to pre-training in the groups 7h (Pre= 10. 8 ± 4.8 versus Post= 9.5, ± 3.8; p = 0.006) and <7h (Pre= 10.5 ± 3.5 versus Post= 8.8 ± 3.1; p < 0.001). AMA was higher post compared to pre-training in the groups 7h (Pre= 6708 ± 782).
Fig. 3.
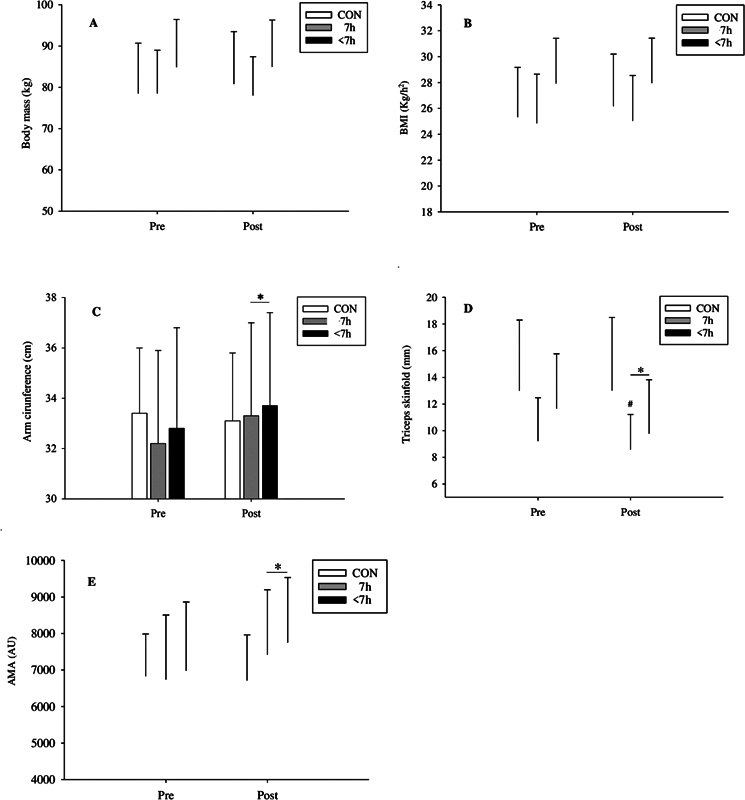
Mean and standard deviation of body composition. (A) Boddy mass pre- and post-training among groups (CON= control group; >7h= Group that sleeps 7 hours; <7h= Group that sleeps less than 7 hours). ANOVA. Interaction: F= 0.89; p = 0.42; 1-β= 0.19. Grupo: F= 0.44; p= 0.65; 1-β= 0.21. Time: F= 0.60; p= 0.44; 1-β= 0.12. (B) BMI pre- and post-training among groups. ANOVA. Interaction: F= 0.53 p= 0.52; 1-β= 0.13. Group: F= 1.81; p= 0.18; 1-β= 0.35. Time: F= 0.76; p= 0.39; 1-β= 0.13. (C) Arm circumference pre- and post-training among groups. ANOVA. Interaction: F= 10.26; p< 0.001; 1-β= 0.98. (*) higher than pre-training. (D) Triceps skinfold pre- and post-training among groups. ANOVA. Interaction: F= 4.83; p= 0.014; 1-β= 0.76. (*) less than pre-training. ( # ) less than 7 hours post-training. (E) Arm muscle area pre- and post-training among groups. ANOVA. Interaction: F= 12.38; p< 0.001; 1-β= 0.99. (*) higher than pre-training.
Table 3 shows the training effect size values for the variables which showed a statistical difference. Training had a small effect on body composition variables and a very large effect on MRN.
Table 3. Effect size according to groups.
| Variables | Groups | ||
|---|---|---|---|
| 7h Value ( d ) | <7h Value ( d ) | Classification | |
| Arm circumference (cm) | 0.41 | 0.31 | Small |
| Triceps skinfold | 0.21 | 0.33 | Small |
| Arm muscle area | 0.46 | 0.45 | Small |
| Shoulder abduction (rep. n o ) | 1.5 | 1.7 | Large |
| Push-up (rep. n o ) | 1.5 | 1.3 | Large |
| Seated rowing (rep. n o ) | 1.8 | 1.6 | Large |
| Biceps curl (rep. n o ) | 1.7 | 1.5 | Large |
d= Cohen effect size.
Discussion
The objective of the present study was to verify if the reduction of up to 2 hours of the recommended period of sleep interferes with the effects of resistance training. The question of the present study was based on evidence that decreased sleep time can affect the ability to perform physical exercise through different mechanisms 13 24 and impair some organ systems associated with adaptation to physical training. 25
It was expected that the <7h group would present a lower adaptive response to the resistance training used, but the results of the present study did not confirm this hypothesis. Some studies point out that sleep is essential for daily physical recovery, and its restriction would be associated with a decrease in the state of recovery. 24 Experiments with an animal model have shown that consecutive days of sleep deprivation are capable of inhibiting neuroendocrine mechanisms associated with adaptation to physical exercise. 12 13 Moreover, sleep-restricted individuals present increased fatigue, decreased vigor and physical performance before and during physical exercise after one or more nights of reduced sleep time. 16 In addition, a study with an increase in habitual sleep time found an improvement in the performance of some sports motor tasks. 26 It should be noted that the cited studies are based on the researcher's manipulation of 3 or more hours of sleep per night and/or more full days of sleep deprivation, and not on the effects of day-to-day and long-term reduction in recommended sleep time on adaptation to physical training. A possible explanation for the no difference between the experimental groups is the fact that the individuals already experienced reduced periods of sleep for a long period. Thus, it can be speculated that the subjects adapted to the present routine, with no abrupt change in sleep time, and consequently little effect on performance and adaptation to physical exercise.
The training protocol proposed in the present study was able to improve strength and triggered positive adaptations in the participants' body composition. According to Watson et al. (2015) 19 and Ohayon et al. (2017), 27 the minimum time for restorative sleep-in adults is 7 hours per night. Although the groups were different in terms of this reference value, the difference in sleep time between the groups was close to 19% (1h 5min) for total sleep time and 22% (1h31min) for night sleep time. Therefore, it can be concluded that the reduction between 1 and 2 hours of recommended sleep time was not able to impair physical performance and adaptations to the training protocol used. In addition, the results of the present study suggest that the value of 7 hours as a minimum night sleeping time can be relaxed when it comes to a recuperative state related to muscle strength performance.
Previous studies that approached the sleep restriction protocol presented in the present study can be found in the literature. Bougard et al. (2009) 28 found no effects on maximal isometric and isokinetic strength of the knee extensor muscles after a night with sleep restriction of 1.5 hours in adults who usually woke up between 6:30 and 7:30 am , totaling 5 and 6 hours of sleep, respectively. HajSalem et al. (2013) 29 also found no effects on handgrip muscle strength in adult judo athletes after a night with 5 hours of sleep, which corresponded to a sleep restriction of 1.5 to 2 hours less in the usual sleep time. Despite being studies with acute effects, the results are similar to those found in the present study.
The strength level that a subject can achieve and maintain depends on the degree of activation of the central nervous system, the conduction of the nerve impulse to the muscle, and other structures of the muscle itself. 30 Thus, two studies were found in the literature to understand the relationship between sleep deprivation and strength control. They investigated the degree of brain activation and the ability of muscle activation by the brain. Manganotti et al. (2001) 31 investigated cortical activation during thenar muscle activation during 24 hours of sleep deprivation. Data were collected at 9:00, 14:00, 21:00, 00:00, 3:00, 6:00, and 9:00 hours of the following day. The authors found a decrease in cortical activity, an increase in the motor threshold in measurements performed at 3:00 and 6:00 am , and a tendency to decrease peripheral nerve activation, which indicates a depressant effect on cortical activity and difficulty in peripheral neural activation in at least one period of sleep deprivation. On the other hand, the second study by Temesi et al. (2013) 32 found no difference in voluntary cortical activation and voluntary peripheral activation after 40-minute submaximal exercise followed by progressive fatigue testing between groups with and without 24-hour sleep deprivation. These results suggest that the effects of sleep deprivation depend on the characteristics of the physical exercise used and that its effects on the neural mechanisms of muscle contraction control are controversial.
On the other hand, the effects of training with elastic bands in improving strength capacity were found. Calatayud et al. (2015) 2 found an increase of 13% and 17% in the 1RM and 6RM tests, respectively, performed on the bench press after 10 sessions of push-up training with an elastic band. The training was performed twice a week at an intensity equivalent to 6RM until failure. Colado and Triplett (2008) 33 found a 23% increase in MRN in the squat test after 10 training sessions performed twice a week for the same number of target repetitions (20RM) controlled by the rating of perceived exertion (RPE), since the load 20RM became progressively easier, so the number and stretching degree of the bands were modified to maintain the target RPE.
The increase in MRN is probably due to the increase in fatigue tolerance. 34 As the external load remained the same between sessions, a greater number of repetitions was necessary in each new session for fatigue to interrupt the effort. In addition, the increase in MRN can be attributed to improved neural control of muscle contraction such as changes in the activation of sensory receptors (Golgi tendon organs) and reduction in antagonist co-activation, which enables increased expression of agonist muscle strength. 25 35 The result is less energy expenditure and less effort time.
For the metabolic adaptations, the trained muscle probably showed an improvement in its anaerobic capacity, such as the increase in the activity of anaerobic metabolism enzymes and glycogen concentration. 36 Dynamic contractions tend to intermittently occlude blood flow to the exercising muscle. This mechanism may favor adaptations in the ability to tolerate fatigue induced by increased anaerobic energy production by the muscle. 36 However, these observations are speculative and should be interpreted with caution, as no measurements of these mechanisms were performed. In addition, the present study indicated gains in muscle mass at the end of the training protocol (increase in the arm muscle area), suggesting that increases in the repetition number for the same intensity and 5 weeks of training can generate morphological adaptation in the tissue muscle.
Training with elastic bands causes a progressive increase in resistance due to the band stretching, while the external resistance remains the same when using weights. 37 During the concentric action, the tension accumulated in the band tends to increase the resistance torque along the concentric action while increasing the force in the opposite direction, pulling the limb downwards (i.e., the forearm in the elbow flexion exercise). However, when the resistance arm length (horizontal distance from the band's line of action to the elbow joint) was shorter at the beginning and end of the concentric phase (compared with the mid-concentric phase), it created a torque curve with the elastic band, facilitating the lifting movement, even at the end of the concentric phase when the resistance curve of the band is higher. 37 These characteristics perhaps help to explain the non-difference between the electromyography signals between exercises performed with weights and elastic bands. 38
Regarding the body composition variables, it was expected that individuals with less sleep time would have less muscle mass and greater fat mass due to an incomplete recovery state and neuroendocrine changes associated with body fat gain. 14 17 However, the results of the present study showed no difference in body composition between the experimental groups. Thus, it can be concluded that despite the chronic decrease in sleep in the <7h group, the sleep time lost by the participants in this group was not enough to cause negative effects on body composition compared with the 7h group.
Both groups showed gains in muscle circumference and a decrease in triceps skinfold regarding the response to EB resistance training. However, there was no effect of training on BMI or total body mass. The literature presents different results regarding the effects of EB training on muscle mass. A reduction of these variables was found by Neves et al. (2017) 3 after 16 weeks of training with EB interspersed with walking activity in 60 postmenopausal women. In comparing the effects of EB training and other training means, 45 middle-aged women were divided into 3 groups: training with elastic bands, training with machines, and a control group. Both exercise groups trained twice a week for 10 weeks, and the results showed that both exercise groups decreased body fat, increased fat-free mass, and increased the number of repetitions in the knee extension and squat tests. 33
This study indicated that muscle hypertrophy can occur with a few weeks of training and the number of repetitions presented above is recommended. 1 The reduction in muscle mass due to a sedentary lifestyle and aging contributes to reduced strength, balance, joint wear, and bone mineral content. 39 In the long term, these changes reduce the functional capacity of individuals. 39 Therefore, the present study reinforces some positive adaptations resulting from strength training with the use of elastic bands in the health of adult subjects. As seen, one of the ways to minimize this muscle loss is regular exercise with elastic bands.
In addition to the positive effects on strength capacity and its adaptations presented above, the choice of using EB as a training medium was due to the possibility of using it in different places and its low cost. The authors believe that the simplicity and lower cost provided by EB could improve adherence to physical training on the part of populations who cannot attend a gym, clubs, or other places traditionally recognized as centers for performing physical exercises due to work or economic demands.
Finally, the present study has some limitations. The method used for muscle strength training with the use of elastic bands does not allow the level of load control of the exercises performed on machines. Thus, small variations in movements by the volunteer may have occurred between training sessions. In addition, recording the training load throughout the sessions was limited to the number of repetitions (volume), since the elastic bands' resistance is difficult to record because it constantly varies throughout the movement and is influenced by the volunteer's limb length. In addition, exercises for the lower limbs were not used due to the difficulty of standardizing the execution of the movement in the exercises. Thus, it was not possible to assess whether the presence of larger muscle volumes could interfere with the investigated variables. Finally, some variables, such as muscle hypertrophy, were not evaluated by the best instrument. Ultrasonography and magnetic resonance are the most reliable methods for analyzing changes in muscle mass.
Regarding sleep characteristics, it is possible that for each group there is any difference in the results if comparing the data between good sleepers vs poor sleepers. It is known that some individuals require less time of sleep than recommended. So, it is expected that their sleep pattern will not affect their performance during physical activity, which helps to understand the non-difference in performance and adaptation to the training presented. In addition, the present study did not analyze the participants' sleep quality at the end of the training protocol, which prevents verifying whether the training affected sleep and, consequently, the improvement in the participants' performance.
Conclusion
A habitual reduction of one to two hours in the daily period of sleep is not able to modify the effects of resistance training with elastic bands. In addition, 16 training sessions were able to increase strength and muscle mass in non-resistance-trained adult subjects.
Acknowledgment
CNPq, CAPES, FEPE-UFMG, UFMG, Mapfre Foundation, ITV, CEPE, CEMSA.
Funding Statement
Funding Mapfre Foundation.
Footnotes
Conflict of Interest No.
References
- 1.Westcott W. ACSM STRENGTH TRAINING GUIDELINES. ACSM's Health Fit J. 2009;13:14–22. [Google Scholar]
- 2.Calatayud J, Borreani S, Colado J C, Martin F, Tella V, Andersen L L. Bench press and push-up at comparable levels of muscle activity results in similar strength gains. J Strength Cond Res. 2015;29(01):246–253. doi: 10.1519/JSC.0000000000000589. [DOI] [PubMed] [Google Scholar]
- 3.Neves L M, Fortaleza A C, Rossi F E et al. Functional training reduces body fat and improves functional fitness and cholesterol levels in postmenopausal women: a randomized clinical trial. J Sports Med Phys Fitness. 2017;57(04):448–456. doi: 10.23736/S0022-4707.17.06062-5. [DOI] [PubMed] [Google Scholar]
- 4.Pires M L, Teixeira C W, Esteves A M et al. Sleep, ageing and night work. Braz J Med Biol Res. 2009;42(09):839–843. doi: 10.1590/s0100-879x2009005000011. [DOI] [PubMed] [Google Scholar]
- 5.Adams R J, Appleton S L, Taylor A W et al. Sleep health of Australian adults in 2016: results of the 2016 Sleep Health Foundation national survey. Sleep Health. 2017;3(01):35–42. doi: 10.1016/j.sleh.2016.11.005. [DOI] [PubMed] [Google Scholar]
- 6.Sunir E.Sleep Fundation:https://www.sleepfoundation.org/how-sleep-works/sleep-facts-statisticsaccessed June 20, 2022
- 7.National Sleep Foundation sleep in America poll. Washington, 2009:https://www.sleepfoundation.org/wp-content/uploads/2018/10/2009-POLL-HIGHLIGHTS.pdfaccessed June 20, 2022
- 8.Matricciani L, Olds T, Petkov J. In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev. 2012;16(03):203–211. doi: 10.1016/j.smrv.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 9.Lima M G, Bergamo Francisco P M, de Azevedo Barros M B. Sleep duration pattern and chronic diseases in Brazilian adults (ISACAMP, 2008/09) Sleep Med. 2012;13(02):139–144. doi: 10.1016/j.sleep.2011.07.011. [DOI] [PubMed] [Google Scholar]
- 10.Dattilo M, Antunes H K, Medeiros A et al. Paradoxical sleep deprivation induces muscle atrophy. Muscle Nerve. 2012;45(03):431–433. doi: 10.1002/mus.22322. [DOI] [PubMed] [Google Scholar]
- 11.Mônico-Neto M, Antunes H K, Lee K S et al. Resistance training minimizes catabolic effects induced by sleep deprivation in rats. Appl Physiol Nutr Metab. 2015;40(11):1143–1150. doi: 10.1139/apnm-2015-0061. [DOI] [PubMed] [Google Scholar]
- 12.Giampá S Q, Mônico-Neto M, de Mello M T et al. Paradoxical Sleep Deprivation Causes Cardiac Dysfunction and the Impairment Is Attenuated by Resistance Training. PLoS One. 2016;11(11):e0167029. doi: 10.1371/journal.pone.0167029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dáttilo M, Antunes H KM, Galbes N MN et al. Effects of Sleep Deprivation on Acute Skeletal Muscle Recovery after Exercise. Med Sci Sports Exerc. 2020;52(02):507–514. doi: 10.1249/MSS.0000000000002137. [DOI] [PubMed] [Google Scholar]
- 14.Nedeltcheva A V, Kilkus J M, Imperial J, Schoeller D A, Penev P D. Insufficient sleep undermines dietary efforts to reduce adiposity. Ann Intern Med. 2010;153(07):435–441. doi: 10.1059/0003-4819-153-7-201010050-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zimberg I Z, Fernandes Junior S A, Crispim C A, Tufik S, de Mello M T. Metabolic impact of shift work. Work. 2012;41 01:4376–4383. doi: 10.3233/WOR-2012-0733-4376. [DOI] [PubMed] [Google Scholar]
- 16.Fullagar H H, Duffield R, Skorski S, Coutts A J, Julian R, Meyer T. Sleep and Recovery in Team Sport: Current Sleep-Related Issues Facing Professional Team-Sport Athletes. Int J Sports Physiol Perform. 2015;10(08):950–957. doi: 10.1123/ijspp.2014-0565. [DOI] [PubMed] [Google Scholar]
- 17.Van Cauter E, Spiegel K, Tasali E, Leproult R.Metabolic consequences of sleep and sleep loss Sleep Med 20089(0 1, Suppl 1)S23–S28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011;305(21):2173–2174. doi: 10.1001/jama.2011.710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Watson N F, Badr M S, Belenky G et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(06):843–844. doi: 10.5665/sleep.4716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bertolazi A N, Fagondes S C, Hoff L S et al. Validation of the Brazilian Portuguese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2011;12(01):70–75. doi: 10.1016/j.sleep.2010.04.020. [DOI] [PubMed] [Google Scholar]
- 21.Sadeh A. The role and validity of actigraphy in sleep medicine: an update. Sleep Med Rev. 2011;15(04):259–267. doi: 10.1016/j.smrv.2010.10.001. [DOI] [PubMed] [Google Scholar]
- 22.Frisancho A R. New norms of upper limb fat and muscle areas for assessment of nutritional status. Am J Clin Nutr. 1981;34(11):2540–2545. doi: 10.1093/ajcn/34.11.2540. [DOI] [PubMed] [Google Scholar]
- 23.Cohen J. 2 ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. Statistical power analysis for the behavioral sciences; p. 567. [Google Scholar]
- 24.Knowles O E, Drinkwater E J, Urwin C S, Lamon S, Aisbett B. Inadequate sleep and muscle strength: Implications for resistance training. J Sci Med Sport. 2018;21(09):959–968. doi: 10.1016/j.jsams.2018.01.012. [DOI] [PubMed] [Google Scholar]
- 25.Fifel K, Meijer J H, Deboer T.Long-term effects of sleep deprivation on neuronal activity in four hypothalamic areas Neurobiol Dis 2018109(Pt A):54–63. [DOI] [PubMed] [Google Scholar]
- 26.Silva A C, Silva A, Edwards B J et al. Sleep extension in athletes: what we know so far - A systematic review. Sleep Med. 2021;77:128–135. doi: 10.1016/j.sleep.2020.11.028. [DOI] [PubMed] [Google Scholar]
- 27.Ohayon M, Wickwire E M, Hirshkowitz M et al. National Sleep Foundation's sleep quality recommendations: first report. Sleep Health. 2017;3(01):6–19. doi: 10.1016/j.sleh.2016.11.006. [DOI] [PubMed] [Google Scholar]
- 28.Bougard C, Bessot N, Moussay S, Sesboue B, Gauthie A . Effects of waking time and breakfast intakeprior to evaluation of physical performance in the early morning. Chronobiol Int. 2009;26(02):307–323. doi: 10.1080/07420520902774532. [DOI] [PubMed] [Google Scholar]
- 29.HajSalem M, Chtourou H, Aloui A et al. Effects of partial sleep deprivation at the end of the night on anaerobic performances in judokas. Biol Rhythm Res. 2013;44(13):815–821. [Google Scholar]
- 30.Folland J P, Williams A G. The adaptations to strength training : morphological and neurological contributions to increased strength. Sports Med. 2007;37(02):145–168. doi: 10.2165/00007256-200737020-00004. [DOI] [PubMed] [Google Scholar]
- 31.Manganotti P, Palermo A, Patuzzo S, Zanette G, Fiaschi A. Decrease in motor cortical excitability in human subjects after sleep deprivation. Neurosci Lett. 2001;304(03):153–156. doi: 10.1016/s0304-3940(01)01783-9. [DOI] [PubMed] [Google Scholar]
- 32.Temesi J, Arnal P J, Davranche K et al. Does central fatigue explain reduced cycling after complete sleep deprivation? Med Sci Sports Exerc. 2013;45(12):2243–2253. doi: 10.1249/MSS.0b013e31829ce379. [DOI] [PubMed] [Google Scholar]
- 33.Colado J C, Triplett N T. Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. J Strength Cond Res. 2008;22(05):1441–1448. doi: 10.1519/JSC.0b013e31817ae67a. [DOI] [PubMed] [Google Scholar]
- 34.Noakes T D, St Clair Gibson A, Lambert E V. From catastrophe to complexity: a novel model of integrative central neural regulation of effort and fatigue during exercise in humans: summary and conclusions. Br J Sports Med. 2005;39(02):120–124. doi: 10.1136/bjsm.2003.010330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gabriel D A, Kamen G, Frost G. Neural adaptations to resistive exercise: mechanisms and recommendations for training practices. Sports Med. 2006;36(02):133–149. doi: 10.2165/00007256-200636020-00004. [DOI] [PubMed] [Google Scholar]
- 36.Burgomaster K A, Moore D R, Schofield L M, Phillips S M, Sale D G, Gibala M J. Resistance training with vascular occlusion: metabolic adaptations in human muscle. Med Sci Sports Exerc. 2003;35(07):1203–1208. doi: 10.1249/01.MSS.0000074458.71025.71. [DOI] [PubMed] [Google Scholar]
- 37.Aboodarda S J, Page P A, Behm D G. Muscle activation comparisons between elastic and isoinertial resistance: A meta-analysis. Clin Biomech (Bristol, Avon) 2016;39:52–61. doi: 10.1016/j.clinbiomech.2016.09.008. [DOI] [PubMed] [Google Scholar]
- 38.Ebben W P, Jensen R L. Electromyographic and kinetic analysis of traditional, chain, and elastic band squats. J Strength Cond Res. 2002;16(04):547–550. [PubMed] [Google Scholar]
- 39.Feigenbaum M S, Pollock M L. Prescription of resistance training for health and disease. Med Sci Sports Exerc. 1999;31(01):38–45. doi: 10.1097/00005768-199901000-00008. [DOI] [PubMed] [Google Scholar]