

Abstract
Background
In recent years, popularity of Biofield energy healing therapy has increased tremendously parallel to conventional therapy. However, due to insufficient scientific studies on biofield therapies, authors planned this clinical trial to examine the safety and effectiveness of biofield therapy in treating symptoms of psychological and mental health and to explore parameters for its effectiveness.
Methods
One hundred fourteen participants (55 male, 59 female) underwent clinical trials. This trial was randomized, placebo-controlled, three parallel-groups, double-blind, and single-center with subjects who have one or more psychological and mental symptoms. Two sessions of distant (virtual) biofield energy attunement were given on days 0 and 90 for about 5 minutes to the subjects of biofield intervention group (n=39). Besides, control (n=35) and sham control (n=40) group subjects also received kind of treatment in a similar manner to nullify baseline responses. Subjects were assessed by psychological questionnaire scoring using standard scale of assessment and safety parameters.
Results
Perceived psychological symptoms/scores (fatigue/tiredness, sleep disturbances, stress, cognitive impairment, loss of memory, mental restlessness, emotional trauma, anxiety, depression, confusion, financial crises and dissatisfaction, low libido, motivation, confidence, lack of perception, relationship, and social behaviors, etc.) were significantly (p <.0001) improved in biofield intervention group compared to the naïve control and sham control groups. Besides, biofield intervention did not show any study-related adverse effects in all three groups throughout the trial.
Conclusions
The distant (virtual) biofield energy healing therapy significantly improved psychological and mental health-related symptoms without affecting safety concerns, and improved overall health and quality of life.
Keywords: Complementary therapy, Biofield therapy, Psychological symptoms, Mental disorder
Introduction
The United States National Institutes of Health (US-NIH) categorized complementary and alternative medicine (CAM) into five broad classes, viz. mind-body therapies (meditation, Yoga, Biofeedback, hypnosis, Tai Chi, etc.), biological therapies (dietary supplements, botanicals, special foods, diets, etc.), biofield therapies (healing touch®, therapeutic touch, Reiki, external Qigong, prayer, blessing, etc.), body-based therapies (massage, reflexology, chiropractic, etc.), and whole medicine systems (traditional Chinese medicine, Ayurvedic, Homeopathic, Naturopathic, etc.).1 In this study, the authors focus on biofield therapy as an intervention. Scientists believe that a form of energy is the infrastructure of the body’s electromagnetic and physiological systems. However, they cannot be detected with modern scientific instruments, have no gravity, and are referred to as “subtle energies”. Conceptions of this, such life force energies have played a central role in the healing of various disorders. Three main subtle energy systems are chakras from the Indian Vedas, meridian systems from ancient Chinese medicine, and auras described in various religious traditions and scientifically studied as “biofields”.2 In conventional medicine, electromagnetic energy is widely used for diagnosis and curative purposes. For example, transcranial magnetic stimulation (TMS),3 magnetic resonance imaging (MRI),4 tumor treatment,5 fracture healing,6 and promotes modulation of neuronal activity for the treatment of depression. In these practices, living beings are infused with a subtle form of energy, and the balance of this energy determines their health. It is suggested that some energy healing practitioners can access these energies in various ways for therapeutic interventions.7 The Trivedi Effect® is one of the fastest growing scientific phenomena in this field in which renowned biofield energy healing practitioners can harness this subtle form of energy from the universe and transmit it to living organisms for balance/restore the flow of energy and non-living objects for structural alteration.8,9 In the last 15 years, the Trivedi Effect® tremendously completed many preclinical experiments and some clinical trials, published in reputed peer-reviewed scientific journals, and established a milestone for the scientific community regarding the safety and effectiveness of biofield energy healing therapy.10,11 Based on the authors’ previous studies, it is hypothesized that distant/virtual healing could be effective for the improvement of psychological behaviors and mental health-related symptoms in adult subjects.
Materials and Methods
Ethical consideration
This study involved a randomized, placebo-controlled, double-blind, three parallel-groups, single-center trial. The study was conducted according to ethical principles and good clinical practices from the declaration of Helsinki.12 The clinical study protocol, informed consent documents, and all other relevant study documentation were reviewed and approved by the Institutional Ethics Committee (IEC) of Riddhi Medical Nursing Home, Gujarat, India (ECR/886/Inst/GJ/2016/RR-19). This study was approved by Clinical Trials Registry – India (CTRI) with clinical trial registration number - CTRI/2022/07/043943.
Experimental
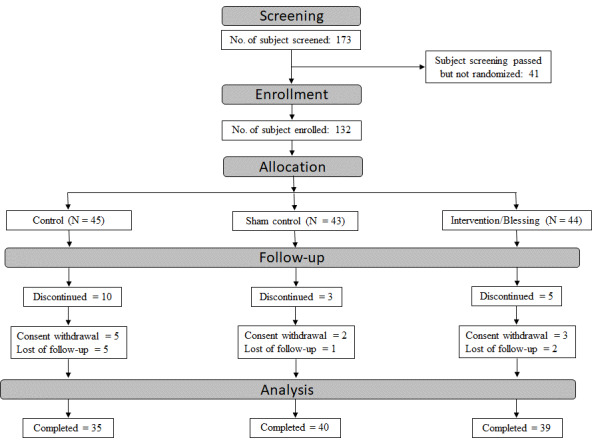
A total of 173 subjects were screened, and 132 subjects meeting eligibility criteria were enrolled (1:1:1 ratio) in order to achieve 114 completed subjects (Figures 1 and 2). The eligible subjects were randomly assigned to the three groups, viz. control (45), sham control (43), and biofield intervention group (44) (1:1:1). To generate the random allocation sequence, a simple randomization technique (allocation concealment mechanism) was utilised with the help of using SAS software (v9.4; SAS Institute Inc., Cary, USA). The randomization schedule was maintained under controlled access. The personnel involved in distributing investigational therapy was accountable for ensuring compliance with the randomization schedule. This study was double-blind, meaning the treatments were blinded to the subjects and principal investigator/physician. In this study, the biofield energy treatments were done virtually for the participants on days 0 and 90. However, the staffs involved in laboratory procedures and collecting objective data were blinded to the subjects under evaluation to maintain the study’s integrity. The sample size for the study was determined using a power analysis. The researchers predicted a Cohen’s d effect size of 0.8 for the biofield intervention group. They estimated that 105 participants, accounting for a 10% drop-out rate, would be needed to achieve a power of 80% and a type 1% error rate (alpha) of 5%.
Figure 1. Schematic diagram of study design.
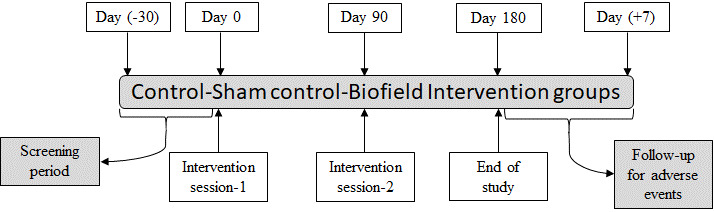
Figure 2. The consolidated standards of reporting trials (CONSORT) flowchart representation of subject disposition.
Inclusion criteria
The South Asian population (India; male and female) who met all the following criteria were included as appropriate participants in the trial, such as those who were 20 to 55 years old at the time of written informed consent. Subjects with a complaint with at least one or more symptoms viz. tiredness, fatigue, pain, exhaustion, sleep disturbances (insomnia, grogginess), stress, anxiety, sadness, hopelessness, irritability, depression, cognition impairment, poor memory, poor attention, confusion, mental restlessness, mind chattering, emotional trauma, suicidal tendencies, lack of self-worth, feeling of satisfaction, pleasure in life, love, affection, status of job/income/business, future/ongoing negative thoughts, etc. were included in this trial. Body mass index (BMI) should be 18.5 to 35.0 kg/m2, calculated as weight in kg / (height in meters).2 Females of childbearing age agreed to use an acceptable form of birth control during the study. They were agreed to provide written informed consent and able to follow the study directions to participate in the study and complete all follow-up processes. They agreed to comply with the study requirements and procedures as per study protocol. Before enrolment, all subjects were screened by the principal investigator and physician for eligibility.
Exclusion criteria
Any participant meeting any of the following criteria was ineligible as: (a) previously or currently having any alcohol dependence or drug abuse; (b) significant diseases or clinically significant abnormal findings in medical history, physical examination, laboratory evaluations, etc., during screening; (c) regular vigorous aerobic/endurance exercise (>3 vigorous bouts/week); (d) known history of positive human immunodeficiency virus (HIV), hepatitis C virus (HCV), hepatitis B surface antigen (HBsAg), or venereal disease research laboratory/ rapid plasma reagin (VDRL/RPR); (e) subjects with non-healthy, non-homogenous, damaged over the skin; (f) subjects with birthmarks or excessive hair over the skin; (g) subjects with the usage of self-tanning agents for at least ten days before screening; and (h) female subjects who demonstrate a positive pregnancy test or currently breast-feeding or planning pregnancy.
Withdrawal criteria
The investigator might withdraw a subject from the study for any of the following reasons: (a) if the subject withdrew his or her self-consent for any reason; (b) if the subject’s condition had worsened to the degree that the investigator feels, it was unsafe for the subject to continue in the study; (c) if the subject has taken any medication; (d) if an adverse effect occurred for which the subject desired to discontinue treatment or the investigator determined that it was in the subject’s best interest to be discontinued; (e) if there was any types of significant protocol deviation; (f) if a concomitant therapy was reported or required which was liable to interfere with the results of the study; (g) if the subject was lost to follow-up; and (h) administrative reasons.
Biofield intervention modalities
The eligible subjects were assigned to the control (no intervention), sham control (sham healer’s intervention), and biofield practitioner’s intervention/treatment groups. The biofield intervention group subjects received two sessions of distant/remote biofield energy treatment (blessing/prayer) by an experienced (> 15 years), renowned spiritual healing practitioner on day 0 and day 90 under the standard clinical laboratory setting. Briefly, the Biofield Energy Healing Therapy/Blessing Therapy was provided by the healing practitioner remotely from Florida, United States of America via an online web-conferencing platform for about 5 minutes through his unique inherent thought transmission process (channeling universal life force energy) via laying his hands to the intervention group of volunteers presented at Cliantha Research Limited, Ahmedabad, Gujarat, India. Blessing therapy’s start and end times were recorded in the electronic case report forms (eCRF). The Trivedi Effect® is a unique and scientifically proven phenomenon in which a healer can harness the inherent intelligent energy from the universal energy field and transmit it anywhere on the planet through instantaneous communication at the quantum level.10,13 Besides, the sham control group subjects also similarly received kind of attunement by the sham person who did not have any type of knowledge of healing practice so as to nullify the baseline responses.
Assessment of perceived psychological symptoms
Perceived changes for psychological and mental health symptoms/complaints were assessed based on psychological questionnaire scoring (PQS). The psychological questionnaire items were used in each category based on the 5-point Likert scale of scoring, ranging from 0-4 (0-none, 1-none to mild, 2-mild to moderate, 3-moderate to severe, and 4-severe to very severe).14 These psychological questionnaire items were prepared in-house with few modifications based on the standard scientific literature done by renowned experienced psychologists and psychiatrists, who were involved in this clinical trial. These questionnaires were checked for content validity (content validity ratio was 0.85), reliability, and internal consistency (Cronbach’s alpha = 0.88) by statisticians and established as in-house PQS documents, which have been routinely used in various clinical trial projects. These psychological questionnaire items were assessed using various symptoms of twelve (12) health categories (Ref. Annexure 1) related to physical health, sleep, stress, cognition and memory, mental health, emotional health, psychological health, perception, relationship and social, sexual health, occupation/finances, and menstrual cycle with a 5-points scoring scale.15 Each subject’s scores were calculated, resulting in total symptoms/perception scores in each category. Total scoring in each category of symptom in the biofield intervention group was compared with the control and sham control groups. Questionnaire-based evaluation of all the symptoms was evaluated at days 0, 90, and 180.
Safety assessment
An adult population was selected, and the chances of interference of concurrent diseases were very unlikely. Safety was determined by monitoring adverse effects (AEs) and medical history, which were classified using the latest version of Medical Dictionary for Regulatory Activities (MedDRA) terminology,16 biochemical parameters, and urine samples. A complete pre-medical history, including a complete review of all current and past diseases and their respective treatments, was taken prior to starting study therapy. Our previous publications and other researchers had already established the safety profile of biofield energy treatment on the human population.10,11,17 Various safety-related biochemical parameters were analyzed at days 0, 90, and 180 in all three groups. Kidney function-related biomarkers such as blood urea nitrogen (BUN) (mg/dL, CAT# 08P16), creatinine (mg/dL, CAT# 07P99), uric acid (mg/dL, CAT# 08P56), urea (mg/dL); heart function-related biomarkers like lactate dehydrogenase (LDH) (U/L, CAT# 07P74) and creatine kinase-MB (CK-MB) (U/L, CAT# 09P95); liver function-related biomarkers viz. alkaline phosphatase (ALP) (U/L, CAT# 08P20), serum glutamic pyruvic transaminase (SGPT) (U/L, CAT# 07P98), serum glutamic-oxaloacetic transaminase (SGOT) (U/L, CAT# 08P17), bilirubin (mg/dL, CAT# 04V51); lipid profile such as total cholesterol (mg/dL, CAT# 07P76), low-density lipoproteins (LDL) (mg/dL), very low density lipoprotein (VLDL) (mg/dL), high-density lipoprotein (HDL) (mg/dL, CAT# 07P75), triglyceride (mg/dL, CAT# 07P77), oxidized-LDL (pg/mL); metabolic biomarkers like glycated haemoglobin (HbA1c) (%, CAT# 08P43), insulin (mU/L), homeostatic model assessment for insulin resistance (HOMA-IR), HOMA-β (%), glucose (mg/dL, CAT# 07P55); and other biomarkers, albumin (g/dL, CAT# 08P02) and total protein (g/dL, CAT# 07P52) to evaluate the adverse effects. All the biochemical parameters were measured using Alinity ci series, Abbott Laboratories Diagnostics Division, USA, using commercially available kits except CK-MB kit obtained from Sentinel, Italy. Besides, oxidized LDL was estimated using Human OxLDL ELISA Kit (CAT# E-EL-H0124), Elabscience Biotechnology Inc, USA, with the help of Microplate Readers (SpectraMax 190, Spectramax M2e), Molecular Devices, USA. Safety-related urine samples were analyzed at days 0, 90, and 180 in all the three groups. Physical examination (color, quantity, specific gravity, odor, appearance, and pH reaction), microscopic examination (pus cells, red blood cells, epithelial cells, crystals, casts, amorphous material, bacteria, trichomonas, and monilia), and chemical examination (albumin, bilirubin, ketone bodies, sugar, and urobilinogen) were performed in all the subjects and the findings are reported in Table 4. All the components in urine samples were measured using Cobas u411 Instrument, Roche Diagnostics GmbH, Switzerland, using commercially available kits, Combur 10 Tesm M (CAT # 11379208191) from Roche Diagnostics GmbH, Germany.
Table 1. Summary of demographic characteristics (safety population).
| Demographic Characteristics | Control (N=45) |
Sham Control (N=43) | Biofield Energy Therapy (N=44) |
|---|---|---|---|
| Age (Years) | |||
| Mean ± SD | 37.5 ± 7.15 | 35.6 ± 6.71 | 32.5 ± 7.78 |
| Median | 38.00 | 36.00 | 32.00 |
| Min, Max | 21, 54 | 23, 49 | 20, 49 |
| p value: 0.0172 | |||
| Sex [n (%)] | |||
| Male | 22 (48.89) | 21 (48.84) | 21 (47.73) |
| Female | 23 (51.11) | 22 (51.16) | 23 (52.27) |
| p value: 0.9924 | |||
| Race [n (%)] | |||
| South Asian | 45 (100) | 43 (100) | 44 (100) |
| Other | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| p value: NE | |||
| Height (cm) | |||
| Mean ± SD | 158.5 ± 10.60 | 160.2 ± 11.25 | 158.1 ± 9.36 |
| Median | 159.00 | 162.00 | 158.00 |
| Min, Max | 137, 182 | 138, 180 | 141, 178 |
| p value: 0.8103 | |||
| Weight (kg) | |||
| Mean ± SD | 61.894 ± 9.16 | 65.285 ± 14.28 | 61.888 ± 10.05 |
| Median | 61.65 | 62.00 | 61.83 |
| Min, Max | 43.45, 85.60 | 44.1, 93.50 | 37.1, 89.05 |
| p value: 0.4608 | |||
| BMI (kg/m2) | |||
| Mean ± SD | 24.78 ± 3.83 | 25.37 ± 4.51 | 24.86 ± 4.31 |
| Median | 24.50 | 24.30 | 24.65 |
| Min, Max | 18.8, 32.20 | 18.8, 34.60 | 18.6, 34.80 |
| p value: 0.9191 | |||
| Marital Status [n (%)] | |||
| Divorced | 3 (6.67) | 1 (2.33) | 1 (2.27) |
| Married | 34 (75.56) | 38 (88.37) | 29 (65.91) |
| Married but separated | 1 (2.22) | 1 (2.33) | 2 (4.55) |
| Single | 5 (11.11) | 3 (6.98) | 10 (22.73) |
| Widow | 2 (4.44) | 0 (0.00) | 0 (0.00) |
| Widower | 0 (0.00) | 0 (0.00) | 2 (4.55) |
| p value: 0.1240 | |||
| Smoking history [n (%)] | |||
| Previous | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| Current | 0 (0.00) | 0 (0.00) | 0 (0.00) |
| Never | 0 (0.00) | 1 (2.33) | 0 (0.00) |
| p value: NE | |||
BMI = body mass index; BMI = weight (kg)/height (m2), cm = centimeter; kg = kilogram; N = number of subjects in the specified treatment group; Max = maximum; Min = minimum; n = number of subjects in the specified category; SD = standard deviation; NE = not estimable. The percentages were based on number of subjects in the specified treatment group. For continuous variables, the p-value was calculated by using one-way Analysis of Variance (ANOVA) and for categorical variables, the p-value was calculated by using the Chi square test.
Table 2. Self-reported changes for psychological symptoms/complaints scores assessed based on the psychological questionnaire (mITT population).
| Parameter | Control (N=35) |
Sham Control (N=40) |
Biofield Energy Therapy (N=39) |
|||
|---|---|---|---|---|---|---|
| Day 90 (Mean$ ± SD) |
Day 180 (Mean$ ± SD) | Day 90 (Mean$ ± SD) | Day 180 (Mean$ ± SD) | Day 90 (Mean$ ± SD) |
Day 180 (Mean$ ± SD) |
|
| Tiredness /fatigue/pain |
-0.2 ± 0.79 | -0.1 ± 0.78 | 0.3 ± 0.99 | 0.2 ± 1.08** | -11.5 ± 1.02****/#### | -15.4 ± 0.55****/#### |
| Sleep disturbances | -0.4 ± 0.74 | -0.1 ± 0.60 | 0.4 ± 1.21 | 0.3 ± 1.28 | -11.3 ± 0.87****/#### | -15.4 ± 0.49****/#### |
| Stress | -0.7 ± 1.05 | -0.1 ± 0.55 | 0.1 ± 0.52 | 0.1 ± 0.55** | -11.1 ± 0.97****/#### | -15.1 ± 0.68****/#### |
| Lack of cognition and memory |
-0.3 ± 0.87 | -0.2 ± 0.82 | 0.4 ± 1.00 | 0.3 ± 1.02 | -11.2 ± 1.02****/#### | -15.3 ± 0.58****/#### |
| Mental restlessness | -0.6 ± 1.09 | -0.2 ± 0.45 | 0.1 ± 0.38* | 0.0 ± 0.42 | -11.3 ± 0.80****/#### | -15.3 ± 0.44****/#### |
| Emotional trauma | -0.5 ± 1.01 | -0.1 ± 0.74 | -0.2 ± 0.50 | -0.2 ± 0.43* | -11.6 ± 1.02****/#### | -15.4 ± 0.50****/#### |
| Lack of inspiration/ motivation/ enthusiasm |
-0.6 ± 0.91 | -0.2 ± 0.38 | 0.1 ± 0.47 | 0.1 ± 0.44 | -11.6 ± 1.09****/#### | -15.4 ± 0.49****/#### |
| Lack of Perception | -0.3 ± 1.15 | 0.1 ± 0.74 | 0.7 ± 2.15 | 0.6 ± 2.17 | -11.2 ± 0.93****/#### | -15.2 ± 0.67****/#### |
| Lack of Relationships & Social | -0.5 ± 1.17 | 15.6 ± 0.65 | -0.1 ± 0.44 | 15.0 ± 0.32** | -11.1 ± 1.07****/#### | 0.1 ± 0.27****/#### |
| Low libido | -0.2 ± 0.80 | -0.0 ± 0.51 | 0.5 ± 1.99 | 0.6 ± 1.97 | -11.3 ± 0.96****/#### | -15.2 ± 0.67****/#### |
| Financial crises & dissatisfaction |
-0.6 ± 0.97 | -0.1 ± 0.68 | 0.0 ± 0.36 | 0.0 ± 0.51** | -10.9 ± 0.97****/#### | -15.0 ± 0.56****/#### |
| Menstrual Disorders | -0.4 ± 1.23 | 0.2 ± 0.81 | 0.2 ± 1.10 | 0.2 ± 1.10 | -11.2 ± 0.70****/#### | -15.3 ± 0.57****/#### |
All the values are represented as Mean ± SD of CFB (change from baseline); $CFB = (post baseline – baseline); N = number of subjects in the respective treatment group. Day 0 considered as the baseline. Statistical significance p-value was calculated for between comparison using one-way Repeated Measure Analysis of Covariance (RM-ANCOVA). *p <.05, **p <.01, and ****p <.0001 vs. control group; ####p <.0001 vs. sham control group.
Table 3. Assessment of safety-related biochemical parameters (safety population).
| Parameter | Control (N=45) |
Sham Control (N=43) |
Biofield Energy Therapy (N=44) |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Day 0 (Mean ± SD) | Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
Day 0 (Mean ± SD) |
Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
Day 0 (Mean ± SD) |
Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
|
| Kidney Biomarkers | |||||||||
| BUN (mg/dL) | 7.91 ± 2.50 |
8.17 ± 2.30 |
8.14 ± 2.34 |
8.69 ± 2.19 |
8.03 ± 1.65 |
9.12 ± 2.79 |
7.50 ± 2.25 |
7.28 ± 2.15 |
8.85 ± 2.65 |
| Creatinine (mg/dL) | 0.90 ± 0.20 |
0.80 ± 0.17 |
0.78 ± 0.16 |
0.92 ± 0.16 |
0.76 ± 0.14 |
0.82 ± 0.16 |
0.85 ± 0.17 |
0.73 ± 0.13 |
0.78 ± 0.15 |
| Uric acid (mg/dL) | 4.57 ± 1.34 |
4.51 ± 1.18 |
4.54 ± 1.38 |
4.86 ± 1.08 |
4.70 ± 1.06 |
4.76 ± 0.95 |
4.55 ± 1.00 |
4.62 ± 1.08 |
4.89 ± 0.98 |
| Urea (mg/dL) | 16.92 ± 5.36 | 17.48 ± 4.92 |
17.47 ± 5.01 | 18.59 ± 4.68 | 17.19 ± 3.54 | 17.43 ± 5.01 | 16.04 ± 4.82 | 15.59 ± 4.61 | 18.94 ± 5.66 |
| Heart Biomarkers | |||||||||
| LDH (U/L) | 190.85 ± 30.07 | 189.12 ± 34.87 | 187.24 ± 37.95 | 190.75 ± 32.49 | 184.95 ± 36.19 | 175.10 ± 27.59 | 196.65 ± 30.35 | 187.29 ± 36.40 | 188.69 ± 46.74 |
| CK-MB (U/L) | 32.24 ± 10.47 | 34.99 ± 10.61 | 35.53 ± 14.71 | 28.02 ± 7.52 | 29.65 ± 9.60 | 25.00 ± 7.61 | 30.60 ± 7.91 | 31.73 ± 8.42 | 27.59 ± 6.87 |
| Liver Biomarkers | |||||||||
| ALP (U/L) | 74.50 ± 19.70 | 83.28 ± 21.64 | 78.43 ± 21.27 | 74.34 ± 18.26 | 77.67 ± 19.50 | 72.97 ± 21.40 | 82.09 ± 22.90 | 78.94 ± 25.57 | 81.80 ± 20.80 |
| SGPT (U/L) | 24.06 ± 13.17 | 28.36 ± 17.63 | 26.96 ± 24.04 | 20.18 ± 9.61 | 24.47 ± 15.06 | 21.15 ± 11.73 | 23.71 ± 12.28 | 26.40 ± 12.06 | 29.66 ± 45.38 |
| SGOT (U/L) | 24.20 ± 11.74 | 29.68 ± 18.27 | 28.52 ± 24.21 | 21.42 ± 7.69 | 22.12 ± 8.43 | 20.06 ± 8.00 | 24.41 ± 7.98 | 25.67 ± 10.31 | 30.45 ± 50.03 |
| Bilirubin (mg/dL) | 0.62 ± 0.31 |
0.48 ± 0.31 |
0.50 ± 0.26 |
0.63 ± 0.27 |
0.42 ± 0.25 |
0.48 ± 0.22 |
0.58 ± 0.24 |
0.39 ± 0.16 |
0.50 ± 0.28 |
| Lipid Profile | |||||||||
| Total cholesterol (mg/dL) | 178.54 ± 34.01 | 171.00 ± 20.54 | 168.44 ± 24.12 | 189.92 ± 33.40 | 185.35 ± 28.22 | 184.15 ± 30.65 | 175.41 ± 30.69 | 172.22 ± 34.67 | 177.80 ± 41.14 |
| LDL (mg/dL) | 111.57 ± 29.82 | 101.44 ± 21.33 | 99.14 ± 25.48 | 119.67 ± 29.65 | 111.21 ± 24.20 | 112.51 ± 28.26 | 105.80 ± 25.10 | 99.88 ± 34.27 | 106.01 ± 36.03 |
| VLDL (mg/dL) | 20.30 ± 8.77 | 21.67 ± 11.15 | 2.40 ± 9.11 |
22.00 ± 7.85 | 23.04 ± 10.67 | 21.89 ± 10.67 | 22.59 ± 17.18 | 25.35 ± 14.55 | 26.99 ± 16.76 |
| HDL (mg/dL) | 46.67 ± 16.98 | 47.90 ± 17.01 | 47.41 ± 18.28 | 48.26 ± 13.59 | 51.10 ± 12.52 | 48.84 ± 13.11 | 47.03 ± 11.83 | 47.00 ± 9.97 | 44.80 ± 11.48 |
| Triglyceride (mg/dL) | 101.50 ± 43.86 | 108.33 ± 55.73 | 109.43 ± 53.36 | 109.99 ± 39.26 | 115.22 ± 53.35 | 114.02 ± 56.12 | 112.94 ± 85.89 | 126.73 ± 72.73 | 134.97 ± 83.81 |
| Oxidized LDL (pg/mL) | 2374.29 ± 449.52 | 1594.60 ± 763.72 | 1112.66 ± 523.86 | 1731.95 ± 719.22 | 1630.13 ± 617.44 | 1306.09 ± 609.95 | 1443.44 ± 561.08 | 1954.44 ± 727.38 | 1344.30 ± 691.52 |
| Metabolic Biomarkers | |||||||||
| HbA1c (%) | 5.43 ± 0.28 |
5.46 ± 0.31 |
5.29 ± 0.27 |
5.47 ± 0.53 |
5.46 ± 0.46 |
5.42 ± 0.45 |
5.37 ± 0.33 |
5.41 ± 0.32 |
5.35 ± 0.32 |
| Insulin (mU/L) | 10.00 ± 6.67 | 15.04 ± 14.79 | 8.54 ± 4.73 |
9.34 ± 5.80 |
15.52 ± 13.98 | 13.53 ± 18.03 | 9.83 ± 4.91 |
12.05 ± 10.20 | 13.06 ± 12.59 |
| HOMA-IR | 1.93 ± 1.33 | 2.96 ± 3.71 | 1.67 ± 0.95 | 1.90 ± 1.30 | 3.13 ± 3.19 | 2.94 ± 4.83 | 1.89 ± 1.03 | 2.29 ± 1.95 | 2.70 ± 2.94 |
| HOMA-β (%) | 179.81 ± 430.46 | 1998.08 ± 18561.30 | 219.23 ± 184.40 | 225.15 ± 166.88 | 456.66 ± 528.38 | 339.64 ± 397.01 | 277.34 ± 182.60 | 374.35 ± 441.63 | 209.89 ± 526.84 |
| Glucose (mg/dL) | 80.06 ± 6.47 | 76.98 ± 10.90 | 78.06 ± 6.87 | 80.57 ± 11.55 | 77.21 ± 11.10 | 79.95 ± 10.32 | 78.56 ± 7.28 | 76.36 ± 6.46 | 81.20 ± 8.76 |
| Others Biomarkers | |||||||||
| Albumin (g/dL) | 4.60 ± 0.31 |
4.41 ± 0.27 |
4.39 ± 0.32 |
4.70 ± 0.32 |
4.50 ± 0.30 |
4.43 ± 0.29 |
4.82 ± 0.42 |
4.55 ± 0.40 |
4.53 ± 0.45 |
| Total protein (g/dL) | 7.72 ± 0.47 |
7.72 ± 0.36 |
7.58 ± 0.5 |
7.82 ± 0.39 |
7.78 ± 0.41 |
7.52 ± 0.40 |
7.99 ± 0.59 |
7.76 ± 0.47 |
7.69 ± 0.45 |
BUN: Blood urea nitrogen, LDH: Lactate dehydrogenase, CK-MB: creatine kinase-myocardial band, ALP: Alkaline phosphatase, SGPT: Serum glutamic-pyruvic transaminase, SGOT: Serum glutamic-oxaloacetic transaminase, LDL: Low density lipoprotein, VLDL: Very low density lipoprotein, HDL: High density lipoprotein, HbA1c: Hemoglobin A1c (glycated haemoglobin), HOMA-IR: Homeostatic model assessment of insulin resistance, HOMA-β: Homeostasis model assessment of β-cell function
Table 4. Summary of urinalysis (safety population).
| Parameter | Result | Control (N=45) |
Sham Control (N=43) |
Biofield Energy Therapy (N=44) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Day 0 (Mean ± SD) | Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
Day 0 (Mean ± SD) |
Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
Day 0 (Mean ± SD) |
Day 90 (Mean ± SD) |
Day 180 (Mean ± SD) |
|||
| Quantity | - | 27.3 ± 4.21 | 29.7 ± 6.57 | 28.4 ± 6.50 | 28.3 ± 4.61 | 29.5 ± 6.60 | 29.0 ± 6.81 | 28.8 ± 3.91 | 31.3 ± 7.33 | 28.3 ± 6.32 | |
| Specific Gravity | - | 1.0090 ± 0.00570 | 1.0157 ± 0.00699 | 1.0101 ± 0.00521 | 1.0095 ± 0.00532 | 1.0127 ± 0.00549 | 1.0109 ± 0.00587 | 1.0075 ± 0.00411 | 1.0120 ± 0.00558 | 1.0122 ± 0.00667 | |
| pH (Reaction) | - | 6.3 ± 1.03 | 6.2 ± 1.24 | 6.1 ± 1.13 | 6.0 ± 1.00 | 6.5 ± 1.13 | 6.0 ± 0.97 | 6.6 ± 1.13 | 6.7 ± 1.19 | 6.1 ± 1.22 | |
| Albumin (Protein) | Negative | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Amorphous Material | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Appearance | Clear | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Bacteria | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Bilirubin | Negative | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Casts | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Colour | Pale yellow | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 39 (90.70) | 44 (100) | 41 (93.18) | 37 (84.09) | |
| Crystals | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Epithelial Cells | 0-1 | 33 (73.33) | 23 (51.11) | 19 (42.22) | 40 (93.02) | 41 (95.35) | 27 (62.79) | 32 (72.73) | 41 (93.18) | 29 (65.91) | |
| 1-2 | 12 (26.67) | 15 (33.33) | 16 (35.56) | 3 (6.98) | 0 (0) | 13 (30.23) | 12 (27.27) | 0 (0) | 10 (22.73) | ||
| Ketones | Negative | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 40 (93.02) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Monilia | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Odour | Aromatic | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 43 (97.73) | 41 (93.18) | 39 (88.64) | |
| Pus Cells (WBCs) | 0-1 | 42 (93.33) | 38 (84.44) | 32 (71.11) | 35 (81.40) | 41 (95.35) | 32 (74.42) | 40 (90.91) | 41 (93.18) | 33 (75.00) | |
| Red Blood Cells | Nil | 45 (100) | 38 (84.44) | 33 (73.33) | 42 (97.67) | 41 (95.35) | 32 (74.42) | 44 (100) | 41 (93.18) | 31 (70.45) | |
| Sugar (Glucose) | Negative | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Trichomonas | Absent | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
| Urobilinogen | Negative | 45 (100) | 38 (84.44) | 35 (77.78) | 43 (100) | 41 (95.35) | 40 (93.02) | 44 (100) | 41 (93.18) | 39 (88.64) | |
Statistical analysis
Continuous variables were expressed by means, medians, and standard deviation (SD) in the descriptive analysis of the sample. For continuous variables, one-way repeated Analysis of Variance (ANOVA), and for categorical variables, Chi-square was used to calculate the p value. The data were represented as mean ± SD/standard error of the mean (SEM) and subjected to statistical analysis. Statistical analysis of perceived psychological assessment scores was performed, and the level of significance (p-value) was determined using one-way Repeated Measure Analysis of Covariance (RM-ANCOVA) with 95% CI of the difference between treatment using SAS® 9.4 (SAS Institute Inc., Cary, USA). The p<0.05 was considered statistically significant. The authors presented psychological score data in the format of the least square mean (LS mean) difference between the groups, 95% confidence interval (CI), and corresponding level of significance, p-value, i.e., (LS mean, 95% CI, p-value). The psychological outcomes of participants, who were randomized and received at least one intervention, were carried out using the intention-to-treat (ITT) analysis. We compared the results of the ITT with that per-protocol (PP) analysis to check whether the results were consistent or not. The statistical results of the ITT and PP population data were the same, and the data is considered reliable. Therefore, the results of the ITT analysis were reported in the manuscript.
Results
Disposition of study subjects
A total of 173 subjects were screened; 132 met the eligibility criteria, enrolled in the study, received study intervention, and 114 completed the study. Among these, 35 (18 male + 17 female) subjects were assigned to the control group, 40 (18 male + 22 female) subjects were assigned to the sham control group, and 39 (19 male + 20 female) subjects to the biofield intervention group and continued at the end of the study. A total of 18 subjects were discontinued from the study during the study period. The reason for discontinuation in the control group was consent withdrawal by subject (5) and loss to follow-up (5 subjects). Similarly, in the sham control group, the reason for discontinuation was consent withdrawal by subjects (2) and loss to follow-up (1 subject), and in the biofield intervention group consent withdrawal by subjects (3) and loss to follow-up (2 subjects) (Figure 2).
Demographic and baseline characteristics
South Asian males and females aged between 20 to 55 years were enrolled in the study. Demographic characteristics of study subjects were recorded. The mean age for the subjects enrolled in the control, sham control, and biofield intervention (blessing) groups was 37.5 years, 35.6 years, and 32.5 years, respectively. The mean BMI index for the subjects enrolled in the control group, the sham control group, and the blessing group was 24.78 kg/m2, 25.37 kg/m2, and 24.86 kg/m2, respectively. The male and female subjects’ percentages in the control group (48.89%; 51.11%), the sham control group (48.84%; 51.16%), and the blessing group (47.73%; 52.27%) were comparable. Most enrolled subjects were married (i.e., around 76.52%). No significant difference was noticed on the demographic characteristics such as gender, height, weight, and BMI except for age (p = 0.0172) across study treatment groups (Table 1). The same demographic data were shown in another manuscript to clarify and understand the results.
Assessment of perceived psychological scores
All the data were expressed in the format of the least square mean (LS mean) difference between the groups, 95% confidence interval (CI), and corresponding level of significance, p-value, i.e., (LS mean, 95% CI, p-value). The perceived psychological symptoms/scores of tiredness/fatigue/pain related to physical health were significantly reduced in the biofield intervention group at day 90 (-11.45, (-11.74, -11.16), p <.0001) and day 180 (-15.43, (-15.72, -15.14), p <.0001); while in the sham control group at day 180 (-0.51, (-0.81, -0.20), p =0.0014) as compared to the control group. Moreover, this score was significantly reduced in the biofield intervention group at day 90 (-11.15, (-11.45, -10.86), p <.0001) and day 180 (-14.93, (-15.22, -14.63), p <.0001) as compared to the sham control group. The sleep disturbances score was significantly lowered in the biofield intervention group at day 90 (-11.01, (-11.32, -10.71), p <.0001) and day 180 (-15.32, (-15.62, -15.02), p <.0001) compared to the control group. Additionally, this score was also significantly lowered in the biofield intervention group at day 90 (-11.12, (-11.43, -10.82), p <.0001) and day 180 (-15.05, (-15.35, -14.74), p <.0001) compared to the sham control group. The biofield intervention group showed a significant reduction of the stress score at day 90 (-10.79, (-11.09, -10.49), p <.0001) and day 180 (-15.41, (-15.71, -15.11), p <.0001) with respect to the control group. Further, the stress score was statistically reduced in the biofield intervention group at day 90 (-10.87, (-11.15, -10.59), p <.0001) and day 180 (-14.90, (-15.18, -14.62), p <.0001) with respect to the sham control group. Besides, stress score was significantly reduced in the sham control group at day 180 (-0.52, (-0.84, -0.19), p =0.0018) than control group. There was a significant reduction of lack of cognition and memory scores in the biofield intervention group at day 90 (-10.89, (-11.19, -10.60), p <.0001) and day 180 (-15.22, (-15.52, -14.92), p <.0001) than the control group. This score was also significantly reduced in the biofield intervention group at day 90 (-10.89, (-11.19, -10.60), p <.0001) and day 180 (-15.22, (-15.52, -14.92), p <.0001) than the sham control group. The perceived psychological symptoms/scores of mental restlessness were significantly reduced in the biofield intervention group at day 90 (-10.89, (-11.18, -10.60), p <.0001) and day 180 (-15.30, (-15.58, -15.01), p <.0001); while in the sham control group at day 90 (0.36, (0.06, 0.67), p =.0207) than the control group. Additionally, mental restlessness score was significantly reduced in the biofield intervention group at day 90 (-11.25, (-11.53, -10.98), p <.0001) and day 180 (-15.13, (-15.40, -14.85), p <.0001) than the sham control group. The score of emotional trauma was statistically lowered in the biofield intervention group at day 90 (-11.19, (-11.49, -10.88), p <.0001) and day 180 (-15.46, (-15.76, -15.15), p <.0001); while sham control group at day 180 (-0.41, (-0.73, -0.10), p =0.0104) than the control group. Further, emotional trauma scores were also remarkably lowered in the biofield intervention group at day 90 (-11.15, (-11.45, -10.85), p <.0001) and day 180 (-15.05, (-15.34, -14.75), p <.0001) than the sham control group. The scores of psychological symptoms (lack of inspiration/motivation/enthusiasm) were notably diminished in the biofield intervention group at day 90 (-11.23, (-11.54, -10.93), p <.0001) and day 180 (-15.46, (-15.76, -15.16), p <.0001) compared to the control group. Besides, the scores of psychological symptoms were notably diminished in the biofield intervention group at day 90 (-11.40, (-11.70, -11.10), p <.0001) and day 180 (-15.19, (-15.49, -14.90), p <.0001) compared to the sham control group. The lack of perception scores was outstandingly decreased in the biofield intervention group at day 90 (-10.90, (-11.22, -10.59), p <.0001) and day 180 (-15.32, (-15.64, -15.01), p <.0001) compared to the control group. Furthermore, this lack of perception scores was also outstandingly decreased in the biofield intervention group at day 90 (-11.06, (-11.37, -10.75), p <.0001) and day 180 (-15.11, (-15.42, -14.80), p <.0001) compared to the sham control group. The self-reported scores related to lack of relationships and social was appreciably minimized in the biofield intervention group at day 90 (-10.97, (-11.29, -10.64), p <.0001) and day 180 (-15.39, (-15.71, -15.07), p <.0001); while in the sham control group at day 180 (-0.48, (-0.81, -0.15), p =0.0049) compared to the control group. As well, the lack of relationships and social scores were appreciably minimized in the biofield intervention group at day 90 (-10.86, (-11.16, -10.56), p <.0001) and day 180 (-14.91, (-15.21, -14.61), p <.0001) compared to the sham control group. The scores related to desire for sex (low libido) were pronouncedly brought down in the biofield intervention group at day 90 (-11.09, (-11.44, -10.75), p <.0001) and day 180 (-15.16, (-15.20, -14.82), p <.0001) compared to the control group. Too, the low libido score was impressively reduced in the biofield intervention group at day 90 (-11.38, (-11.72, -11.05), p <.0001) and day 180 (-15.31, (-15.64, -14.97), p <.0001) compared to the sham control group. The scores of financial crises and dissatisfaction were considerably reduced in the biofield intervention group at day 90 (-10.44, (-10.74, -10.15), p <.0001) and day 180 (-15.07, (-15.36, -14.77), p <.0001); while in the sham control group day 90 (0.44, (0.14, 0.74), p =0.0044) compared to the control group. Likewise, the scores of financial crises and dissatisfaction were considerably reduced in the biofield intervention group at day 90 (-10.88, (-11.17, -10.59), p <.0001) and day 180 (-14.91, (-15.19, -14.62), p <.0001) compared to the sham control group. The perceived scores of menstrual disorders-related symptoms were significantly reduced in the biofield intervention group at day 90 (-10.83, (-11.22, -10.44), p <.0001) and day 180 (-15.52, (-15.91, -15.13), p <.0001) compared to the control group. Furthermore, menstrual disorders symptoms-related scores were significantly reduced in the biofield intervention group at day 90 (-11.06, (-11.43, -10.69), p <.0001) and day 180 (-15.16, (-15.53, -14.79), p <.0001) compared to the sham control group (Table 2).
Safety evaluation
No adverse effects (AEs) or death were reported in any of the three groups during the entire study period. Various safety-related biochemical parameters (Table 3) and urine samples (Table 4) were analyzed at days 0, 90, and 180 in all three groups, and the test results were found within the normal range in all the treatment groups.
Discussion
The main goal of biofield energy therapies is to rebalance the body’s energy system, making it more robust in its ability to heal and more resistant to stress. Our body, inside and out, is made of energy. Diseases often originate in the mind, which is a canvas of human consciousness, acting as a holographic representation of the body. Healing aims to improve our energy of consciousness, leading to spiritual healing through biochemical changes. Biofield energy therapy has gained attention for its positive effects on psychological and mental health disorders.10,11 Theoretically, biofield energy therapies work through similar models in physics, like bioelectromagnetism, quantum physics, and superstring theory. Physicists suggested that subtle vibrational energies may aid in determining health and disease.18 As biofield therapy has no side effects and is very low-cost and efficacious, an integrated medical practice may be needed; instead of contradictions between conventional and complementary medicine, both systems must work in tandem. The Trivedi Effect® is a quantum form of biofield energy therapy registered as a trademark in India, 2013. This therapy globally practiced through harnessing intelligent energy from the universal energy field to promote healing and well-being. The therapy positively impacts mental, spiritual, and emotional well-being, and it is proposed to work through quantum entanglement.13 Healing therapy will aid in enhancing clients’ well-being and quality of life, which is the goal of any healthcare professional. Throughout the trial, the authors did not observe any adverse effects in all three groups. Moreover, safety-related biochemical and urine analysis data did not show any significant difference in the biofield intervention group as compared to both naive and sham control groups (Tables 3 and 4). The medical world has recently accepted the importance of patients’ values, beliefs, and philosophical perspectives on life and well-being.19 In this trial, authors aimed to study the impact of a renowned healing practitioner’s biofield energy on psychological and mental well-being in adult subjects through distant (virtual) mode. The finding by Coyne et al., 2012, demonstrated the effect of biofield healing on fatigue in breast cancer survivors and found a statistically significant reduction in total fatigue for the biofield intervention group compared with mock treatment and wait-list groups^.20 Here, biofield therapy also significantly reduced fatigue and tiredness in the biofield intervention group of psychologically compromised adult subjects compared with the control and sham control groups. This data was well corroborated with the literature. Various modalities are used to stimulate energy within the body to restore an energy balance, including hands-on healing, vibration applied to the body, and movement or sound. Sleep is impaired when the body’s energy is imbalanced.21 In this trial, remote hands-on healing significantly (p <.0001) improved sleep quality in the biofield intervention group than control and sham control groups. This finding is well corroborated with the results of Castellar and colleagues in 2014 on breast cancer survivors’ exposure to pranic healing intervention, which observed a significant improvement in sleep disturbances^.22 Biofield energy therapy, like healing touch (HT), significantly improved cognitive function, mood, and depression in the HT treatment group^.23 Current study data showed a significant (p <.0001) improvement in cognition and memory function in adult subjects.
Biofield therapy, like therapeutic touch (TT) significantly decreases the behavioral symptoms of dementia, restlessness, and stress.24 The authors also observed that the biofield intervention group revealed significant improvement in stress and mental restlessness in adult subjects with respect to both control and sham control groups. Our findings also support the results of the other biofield researcher, Wood et al., 2005.24 Rosada et al., 2015, reported that Reiki treatment significantly reduced the emotional exhaustion problems in community mental health clinicians compared to the sham Reiki.25 Different factors can explain how biofield practices affect feelings and perceptions.26 To our knowledge, no studies have investigated the perceptions of personal feelings, like feeling older than his/her actual age, being a successful person or not, either recognizing/getting respect/appreciation or being rejected/ignored by the community, etc. The present study indicates a significant improvement in perception ability, social relationship, low libido, financial stability, and menstrual disorders-related symptoms in the biofield intervention group compared to the control and sham control groups.
Strength and limitation
The current study results significantly improved psychological and mental health-related symptoms in the biofield intervention individuals, which was very promising with respect to both the control and sham control groups. However, in addition to our potential findings, it is also important to review some of this study’s limitations. The study was limited by a smaller sample size in evaluations of group-specific results. Future work with larger samples should clarify reliability and validity within individuals. This study did not give an idea of a specific psychological disorder or gender-specific segregated data analysis; instead, it should investigate the effects of biofield therapies on specific biological and psychological disorders with gender-specific for better visualization. Study outcomes may differ given other biofield healing practitioners and other dosage regimes. In addition, given the absence of information about the exact mechanism of action of distant blessing. Distant (virtual) biofield therapy may be attractive to future researchers who are working on distant blessing.
Conclusion
In conclusion, the present study suggests that the potential benefits of distant/remote (virtual) biofield energy healing were noticed in the psychological and mental health-compromised subjects of the biofield intervention group. In this trial, the renowned healing practitioner successfully transferred the vital force energy to the biofield intervention group subjects and significantly improved psychological and mental health-related symptoms, ultimately improving the quality of life and health well-being.
Corresponding author
Snehasis Jana
Trivedi Science Research Laboratory Pvt. Ltd., Research and Development, Thane (W), Maharashtra, India
Tel: +91-022-25811234
ORCID ID: https://orcid.org/0000-0001-9433-5933
CRediT Author Contribution
M.K.T. and S.J. contributed to the study conception, design, planning, execution, monitoring, and data interpretation. S.M. and D.T. wrote the first draft of the manuscript. A.B. and S.J. contributed to the review and editing. All authors read and approved the final manuscript.
Competing Interests
Authors MKT, AB, and DT were employed by Trivedi Global, Inc. Authors SM and SJ were employed by Trivedi Science Research Laboratory Pvt. Ltd.
Supplementary Material
Acknowledgments
Acknowledgments
The authors are grateful to Cliantha Research Ltd., Gujarat, India, for their assistance and support during the work. The authors also express gratitude to all participants and researchers who participated in this trial for their cooperation.
Funding Statement
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
References
- Introducing complementary and alternative therapies. Koithan M. 2009J Nurse Pract. 5(1):18–20. doi: 10.1016/j.nurpra.2008.10.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The energy of energy psychology. Feinstein D. 2022OBM Integr Comp Med. 7(2):015. doi: 10.21926/obm.icm.2202015. doi: 10.21926/obm.icm.2202015. [DOI] [Google Scholar]
- Cumulative effects of single TMS pulses during beta-tACS are stimulation intensity-dependent. Raco V., Bauer R., Norim S.., et al. 2017Brain Stimul. 10:1055–1060. doi: 10.1016/j.brs.2017.07.009. doi: 10.1016/j.brs.2017.07.009. [DOI] [PubMed] [Google Scholar]
- Thermal effects associated with RF exposures in diagnostic MRI: Overview of existing and emerging concepts of protection. Van den Brink J. S. 2019Concepts Magn Reson Part B. 2019:9618680. doi: 10.1155/2019/9618680. [DOI] [Google Scholar]
- Tumour-treating fields (TTFields): Investigations on the mechanism of action by electromagnetic exposure of cells in telophase/cytokinesis. Berkelmann L., Bader A., Meshksar S., et al. 2019Sci Rep. 9(1):7362. doi: 10.1038/s41598-019-43621-9. doi: 10.1038/s41598-019-43621-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effects of local vibration and pulsed electromagnetic field on bone fracture: A comparative study. Bilgin H. M., Çelik F., Gem M.., et al. 2017Bioelectromagnetics. 38(5):339–348. doi: 10.1002/bem.22043. [DOI] [PubMed] [Google Scholar]
- Saad M., de R. Complementary Therapies for the Contemporary Healthcare. InTech; Distant healing by the supposed vital energy – scientific bases. [DOI] [Google Scholar]
- A transcendental to changing metal powder characteristics. Trivedi M.K., Tallapragada R.M. 2008Met Powder Rep. 63(9):22–31. doi: 10.1016/S0026-0657(08)70145-0. [DOI] [Google Scholar]
- Atomic, crystalline and powder characteristics of treated zirconia and silica powders. Trivedi M.K., Patil S., Tallapragada R.M. 2014J Material Sci Eng. 3(144):144. doi: 10.4172/2169-0022.1000144. [DOI] [Google Scholar]
- Evaluate the safety and efficacy of a biofield energy treated proprietary dietary supplement (TRI 360™) on psychological symptoms, mental disorders, emotional well-being, and quality of life in adult subjects. Trivedi M.K., Branton A., Trivedi D.., et al. 2023Altern Ther Health Med. 29(7):104–113. [PubMed] [Google Scholar]
- The role of biofield energy treatment on psychological symptoms, mental health disorders, and stress-related quality of life in adult subjects: A randomized controlled clinical trial. Trivedi M. K., Branton A., Trivedi D.., et al. 2023J Gen Fam Med. 24(3):154–163. doi: 10.1002/jgf2.606. doi: 10.1002/jgf2.606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The importance of Good Clinical Practice guidelines and its role in clinical trials. Vijayananthan A., Nawawi O. 2008Biomed Imaging Interv J. 4(1):e5. doi: 10.2349/biij.4.1.e5. doi: 10.2349/biij.4.1.e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The use of biofield energy therapy as complementary and alternative medicine in human health care system: a narrative review and potential mechanisms. Trivedi M. K., Branton A., Trivedi D.., et al. Apr 3;2024 J Complement Integr Med. :Epubaheadofprint. doi: 10.1515/jcim-2024-0027. doi: 10.1515/jcim-2024-0027. [DOI] [PubMed]
- Coronavirus anxiety scale: A brief mental health screener for COVID-19 related anxiety. Lee S. A. 2020Death Studies. 44(7):393–401. doi: 10.1080/07481187.2020.1748481. [DOI] [PubMed] [Google Scholar]
- COVID-19 Pandemic in the Italian population: validation of a post-traumatic stress disorder questionnaire and prevalence of PTSD symptomatology. Forte G., Favieri F., Tambelli R.., et al. 2020Int J Environ Res Public Health. 17(11):4151. doi: 10.3390/ijerph17114151. doi: 10.3390/ijerph17114151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The medical dictionary for regulatory activities (MedDRA) Brown E.G., Wood L., Wood S. 1999Drug Saf. 20(2):109–117. doi: 10.2165/00002018-199920020-00002. doi: 10.2165/00002018-199920020-00002. [DOI] [PubMed] [Google Scholar]
- Safety and efficacy of biofield therapy in Japan. Suzuki K., Uchida S., Kimura T.., et al. 2009Soc Integr Med Jpn. 2:37–43. [Google Scholar]
- Walleczek J. Electromagnetic Fields. Advances in Chemistry. Vol. 250. ACS Publication; Magnetokinetic effects on radical pairs: A paradigm for magnetic field interactions with biological systems at lower than thermal energy; pp. 395–420. [DOI] [Google Scholar]
- Biofield therapies: Concept and current status. Siotia S., Kannan V. 2022Int J Adv Multidiscip Res. 9(11):69–74. doi: 10.22192/ijamr.2022.09.11.008. [DOI] [Google Scholar]
- Complementary medicine for fatigue and cortisol variability in breast cancer survivors. Coyne J.C., Johansen C., Gorski D. 2012Cancer. 118(18):4635–4637. doi: 10.1002/cncr.27415. doi: 10.1002/cncr.27415. [DOI] [PubMed] [Google Scholar]
- Cacho Valerie, Lum Esther, Chiasson Ann Marie. In: Integrative Sleep Medicine. Cacho Valerie, Lum Esther., editors. Weil Integrative Medicine Library; New York: [2021-5-1]. Energy Medicine and Sleep Disorders; p. 21. [DOI] [Google Scholar]
- Beneficial effects of pranic meditation on the mental health and quality of life of breast cancer survivors. Castellar J. I., Fernandes C. A., Tosta C. E. 2014Integr Cancer Ther. 13(4):341–350. doi: 10.1177/1534735414534730. doi: 10.1177/1534735414534730. [DOI] [PubMed] [Google Scholar]
- Slowing progression of early stages of AD with alternative therapies: a feasibility study. Lu D.F., Hart L.K., Lutgendorf S.K.., et al. 2013Geriatr Nurs. 34(6):457–64. doi: 10.1016/j.gerinurse.2013.07.003. [DOI] [PubMed] [Google Scholar]
- The effect of therapeutic touch on behavioral symptoms of persons with dementia. Woods D. L., Craven R. F., Whitney J. 2005Altern Ther Health Med. 11(1):66–74. [PubMed] [Google Scholar]
- Reiki reduces burnout among community mental health clinicians. Rosada R. M., Rubik B., Mainguy B.., et al. 2015J Altern Complement Med. 21(8):489–95. doi: 10.1089/acm.2014.0403. doi: 10.1089/acm.2014.0403. [DOI] [PubMed] [Google Scholar]
- Human emotions recognition, analysis and transformation by the bioenergy field in smart grid using image processing. Chhabra G., Onyema E. M., Kumar S.., et al. 2022Electronics. 11(23):4059. doi: 10.3390/electronics11234059. doi: 10.3390/electronics11234059. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.