

Abstract
Background
The aim of this study was to evaluate the impact of mental health attributes, such as the presence of psychiatric comorbidities or psychological comorbidities (low resilience), on outcomes after rotator cuff repair (RCR) and total shoulder arthroplasty (TSA).
Methods
PubMed, Cochrane, and Google Scholar (results pages 1–20) were searched up to November 2023. Mental health problems of interest included the presence of psychiatric comorbidities (depression, anxiety) or indicators of poor psychological functioning, such as low resilience or the presence of distress. Patients were assigned to poor or good mental health groups in this study based on their grouping in the original study.
Results
Fourteen studies were included in the meta-analysis. Patients with good mental health had greater improvements in postoperative American Shoulder and Elbow Surgeons and Simple Shoulder Test scores in the TSA cohort (P=0.003 and P=0.01), RCR cohort (P<0.001), and the combined TSA and RCR cohort (P<0.001). No difference was found in visual analog scale score, satisfaction, external rotation, or flexion between the two mental health groups. Patients with poor mental health undergoing RCR experienced higher rates of adverse events and transfusions (P<0.001). Patients with poor mental health also had greater rates of revision and emergency department visits in the TSA cohort (P<0.001), RCR cohort (P=0.05 and P=0.03), and combined cohort (P<0.001). Patients with poor mental health undergoing TSA had a higher rate of re-admission (P<0.001).
Conclusions
Patients with poor preoperative mental health showed inferior patient-reported outcome scores and increased rates of adverse events, revisions, and re-admissions.
Level of evidence
III.
Keywords: Mental health, Rotator cuff repair, Total shoulder arthroplasty, Patient reported outcomes, Adverse events
INTRODUCTION
The prevalence of mental health disorders is alarmingly high, surpassing 15%–20% globally according to the most recent estimates from the World Health Organization [1]. Particularly in the context of the coronavirus disease 2019 pandemic, which was found to have exacerbated mental health burdens, it is imperative to explore how psychiatric comorbidities may influence patient outcomes after elective surgery [2]. In fact, mental health disorders impact the lives of roughly one billion individuals worldwide [1]. With advancing age, there is a notable increase in the susceptibility to mental health disorders, especially in mood and substance use disorders, which exhibit a pronounced age-related escalation in risk [3]. Orthopedic surgeons often encounter postoperative experiences that elude clear explanation, and these situations can frequently be explained by patient-related factors [4-7]. A growing body of literature has emerged to shed light on the effects of mental health on outcomes after elective orthopedic surgery. Many studies indicate preoperative mental health diagnosis and/or lower preoperative scores on validated mental health surveys as predictors for increased postoperative opioid usage and worse patient-reported outcomes (PROs) [8-17].
Recent research has also sought to clarify the relationship between resilience and surgical outcomes. Multiple studies have shown that higher levels of preoperative and early postoperative resilience, as calculated using validated questionnaires like the Pain Self-efficacy Questionnaire, correlate with improved postoperative functional outcomes and PROs [18-22]. In addition, highly resilient patients have been shown to achieve greater success in same-day discharge programs following total joint arthroplasty and to require shorter hospital stays [19,20]. In fact, resilience is often referred to as a part of mental health; as such, for the purpose of this study, it will be examined alongside other mental health entities [23].
In line with the broader orthopedic surgery literature, there is a growing body of evidence in the field of shoulder surgery that suggests similar effects. Several studies of patients undergoing various surgical treatments of the shoulder have reported lower PROs among patients with mental health conditions compared to patients without such conditions [24-28]. Furthermore, other studies have shown that higher preoperative mental health survey scores may correlate with a faster return to work following rotator cuff repair (RCR) and reduced rates of complications and re-admissions following total shoulder arthroplasty (TSA) [29,30]. Thus, the objective of this meta-analysis was to assess the impact of mental health on RCR and TSA outcomes. For the sake of consistency, patients with a psychiatric comorbidity or poor psychological function will be referred to as having poor mental health; otherwise, they will be referred to as having good mental health. We hypothesize that patients with poor mental health will have worse outcomes postoperatively compared to patients with good mental health preoperatively undergoing the same surgeries.
METHODS
Search Strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, PubMed, Cochrane, and Google Scholar (results pages 1–20) were searched up to November 2023. The following keywords and Boolean terms were used to find studies assessing the impact of preoperative mental health on the outcomes of shoulder replacement and RCR: “mental health,” “psych,” “resilience,” “shoulder,” “replacement,” “arthroplasty,” and “rotator cuff.” Additional studies were identified by manually searching through the reference lists of identified papers and by Internet searches. One author extracted the data and another confirmed the choice of articles. The process is summarized in Fig. 1.
Fig. 1.
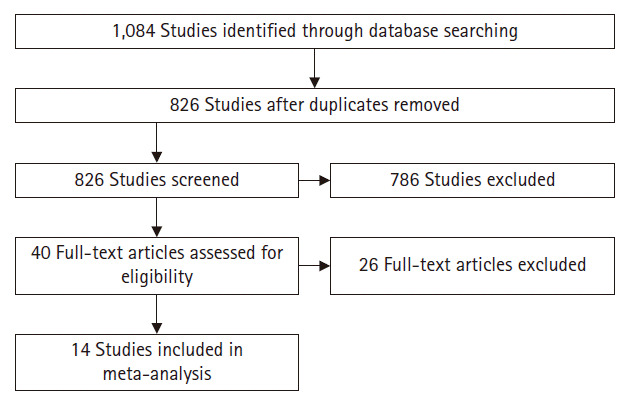
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of article selection.
Comparative studies of patients who had either a TSA or RCR and were separated into two groups based on mental health were included. Mental health problems of interest were psychiatric comorbidities (depression, anxiety) or indicators of poor psychological functioning, such as low resilience or distress. We excluded case reports, narrative or systematic reviews, theoretical research, conference reports, meta-analyses, expert comments, economic analyses, and studies reporting non-relevant outcomes or incomplete outcomes (such as the absence of standard deviations).
Data Extraction
Study eligibility was determined by two reviewers independently. Extracted data consisted of complications, re-admissions, emergency department (ED) visits, revision surgeries, discharge location, transfusions, tendon healing, range of motion (ROM) (external rotation [ER] and flexion), and PROs (American Shoulder and Elbow Surgeons [ASES] score, Simple Shoulder Test [SST] score, visual analog scale [VAS] score, and satisfaction). Any differences between the investigators were resolved by discussion.
Risk-of-Bias Assessment
The ROBINS-I tool was used by the authors to independently assess the risk of bias in the included studies [31]. Studies were excluded if they had a critical risk of bias.
Statistical Analysis
Review Manager 5.4 (Cochrane) was used to perform all statistical analysis. For dichotomous data, the risk ratio and 95% confidence interval were used. For continuous data, mean differences (MDs) with 95% CI values were used. Heterogeneity was evaluated by Q tests and I2 statistics. If considerable heterogeneity was present, as indicated by P≤0.10 or I2 >50%, a random-effects model was used; otherwise, a fixed-effects model was chosen (P>0.10 or I2 <50%). The threshold for statistical significance was set a priori at P≤0.05.
RESULTS
Characteristics of the Included Studies
Fourteen studies [28,30,32-43], including 13 retrospective studies and one prospective study, met the inclusion criteria and were included in the meta-analysis. Seven studies enrolled patients undergoing RCR, including 68,107 patients with good preoperative mental health and 68,547 with poor preoperative mental health. Of these seven studies, three identified patients with a preoperative mood/anxiety disorder, three focused on psychological functioning (resilience, distress), and one studied mental health in general. Another seven studies enrolled patients undergoing TSA, including 560,778 patients with good preoperative mental health and 60,043 with poor preoperative mental health. Of these seven studies, five analyzed patients had a preoperative mood/anxiety disorder and two addressed psychiatric comorbidities in general. The characteristics of the 14 included studies are summarized in Table 1 [25,27,29,32-42].
Table 1.
Main characteristics of the included studies
| Surgery | Study | Methods | Database | Year of data collection | Participants |
Mental health assessment | |
|---|---|---|---|---|---|---|---|
| Poor mental health | Good mental health | ||||||
| Shoulder replacement | Bot et al. (2014) [36] | Retrospective | National hospital discharge survey | 1990–2007 | 24,418 | 324,406 | The presence of a psychiatric comorbidity |
| Colasanti et al. (2023) [28] | Retrospective | Author’s institution | 2011–2020 | 218 | 378 | The presence of anxiety or depression | |
| Diamond et al. (2023) [37] | Retrospective | Pearldiver | 2010–2020 | 4,084 | 20,242 | The presence of depression | |
| Lunati et al. (2021) [38] | Retrospective | Truven MarketScan database | 2009–2017 | 3,209 | 19,414 | The presence of depression | |
| Mollon et al. (2016) [39] | Retrospective | The United States Nationwide Inpatient Sample | 2002–2012 | 27,964 | 196,096 | The presence of depression | |
| Porter et al. (2021) [33] | Retrospective | Author’s institution | 2010–2017 | 62 | 66 | The presence of a psychiatric disorder | |
| Werner et al. (2017) [41] | Retrospective | Author’s institution | 2007–2013 | 88 | 176 | The presence of depression | |
| Rotator cuff repair | Dujeux et al. (2023) [42] | Retrospective | Author’s institution | 2012–2018 | 38 | 181 | The presence of mood and anxiety disorder |
| Freshman et al. (2023) [30] | Retrospective | Pearldiver | 2010–2020 | 68,397 | 67,092 | The presence of a mental health disorder | |
| Johnson et al. (2022) [43] | Retrospective | Author’s institution | 2014–2020 | 232 | 584 | The presence of depression or anxiety | |
| Park et al. (2021) [32] | Retrospective | Author’s institution | Jun–Dec 2017 | 41 | 103 | The presence of depression or anxiety | |
| Porter et al. (2021) [40] | Retrospective | Author’s institution | Jan–Dec 2014 | 5 | 19 | Mild vs. High resilience | |
| Potter et al. (2015) [34] | Retrospective | Author’s institution | 2011–2014 | 26 | 44 | Whether or not the patient is distressed | |
| Thorpe et al. (2018) [35] | Prospective | Author’s institution | 2014–2015 | 40 | 84 | The presence of a poor psychological function | |
Patient-Reported Outcomes
American Shoulder and Elbow Surgeons score
Three studies enrolling 988 subjects undergoing TSA [28,40,41] (368 with poor and 620 with good mental health) and four studies enrolling 362 subjects undergoing RCR [32-35] (112 with poor and 250 with good mental health) reported postoperative ASES scores. Higher postoperative ASES scores were recorded for patients with good mental health undergoing TSA (MD, −9.73; 95% CI, −16.18 to −3.27; P=0.003) (Fig. 2A) and RCR (MD, −10.42; 95% CI, −15.98 to −4.85; P=0.0002) (Fig. 2A). Greater postoperative ASES scores in patients with good mental health were also observed when the cohorts were combined (MD, −9.82; 95% CI, −13.36 to −6.27; P<0.00001) (Fig. 2A).
Fig. 2.

Forest plots showing the difference in postoperative American Shoulder and Elbow Surgeons (ASES) score (A), ASES score improvement (B), postoperative Simple Shoulder Test score (C), postoperative visual analog scale (D), and postoperative satisfaction (E). SD: standard deviation, IV: inverse variance; CI: confidence interval, M-H: Mantel-Haenszel.
When assessing the improvement in ASES (postoperative score−preoperative score), two studies enrolling 860 subjects undergoing TSA [28,41] (306 with poor and 554 with good mental health) and three studies enrolling 338 subjects undergoing RCR [32,34,35] (107 with poor and 231 with good mental health) were included. Greater improvement was seen in the patients with good mental health undergoing TSA (MD, −10.93; 95% CI, −14.46 to −7.40; P<0.00001) (Fig. 2B), while no significant difference was seen in patients undergoing RCR (MD, 2.44; 95% CI, −4.10 to 8.98; P=0.46) (Fig. 2B) or when the cohorts were combined (MD, −2.34; 95% CI, −7.98 to 3.31; P=0.42) (Fig. 2B).
Simple Shoulder Test score
One study of 128 subjects undergoing TSA [40] (62 with poor and 66 with good mental health) and three studies enrolling 238 subjects undergoing RCR [32-34] (72 with poor and 166 with good mental health) reported data on postoperative SST scores. The results showed a greater postoperative improvement in SST scores in patients with good mental health undergoing TSA (MD, −1.20; 95% CI, −2.12 to −0.28; P=0.01; Fig. 2C), RCR (MD, −2.05; 95% CI, −3.17 to −0.93; P=0.0003) (Fig. 2C), and when the cohorts were combined (MD, −1.79; 95% CI, −2.64 to −0.95; P<0.0001) (Fig. 2C).
Visual analog scale
Two studies enrolling 214 subjects undergoing RCR [32,34] (67 with poor and 147 with good mental health) reported data on postoperative VAS scores. The results showed no significant difference between the two groups (MD, 0.66; 95% CI, −0.02 to 1.35; P=0.06) (Fig. 2D).
Satisfaction
Two studies enrolling 860 subjects undergoing TSA [28,41] (306 with poor and 554 with good mental health) reported data on postoperative satisfaction. The results showed no significant difference between the two groups (odds ratio [OR], 0.93; 95% CI, 0.36–2.35; P=0.87) (Fig. 2E).
Range of Motion
Two studies enrolling 724 subjects undergoing TSA [28,40] (280 with poor and 444 with good mental health) and one study enrolling 144 subjects undergoing RCR [32] (41 with poor and 103 with good mental health) reported data on postoperative ROM. The results showed no significant difference in ER or flexion within the TSA cohort (MD, −2.12; 95% CI, −16.81 to 12.58; P=0.78; Fig. 3A) (MD, −2.83; 95% CI,−8.01 to 2.34; P=0.28; Fig. 3B) or the RCR cohort (MD, −0.50; 95% CI, −5.59 to 4.59; P=0.85; Fig. 3A) (MD, −0.30; 95% CI,−4.72 to 4.12; P=0.89; Fig. 3B). In addition, no significant differences were observed when the cohorts were combined (MD, −1.22; 95% CI, −9.01 to 6.57; P=0.84; Fig. 3A) (MD, −1.37; 95% CI, −4.73 to 1.99; P=0.47; Fig. 3B).
Fig. 3.

Forest plots showing the difference in postoperative external rotation (A) and postoperative flexion (B). SD: standard deviation, IV: inverse variance; M-H: Mantel-Haenszel.
Complications
Adverse events
Six studies enrolling 620,557 subjects undergoing TSA [28,36-40] (59,955 with poor and 560,602 with good mental health) and three studies enrolling 136,524 subjects undergoing RCR [30,42,43] (68,667 with poor and 67,857 with good mental health) reported data on postoperative adverse events (medical and surgical complications). There was no significant difference in the rate of complications in patients undergoing TSA (OR, 1.82; 95% CI, 0.86–3.87; P=0.12) (Fig. 4A). However, a higher rate of adverse events was recorded for patients with poor mental health undergoing RCR (OR, 2.25; 95% CI, 1.84–2.74; P<0.00001) (Fig. 4A) and when the cohorts were combined (OR, 1.84; 95% CI, 1.16–2.94; P=0.01) (Fig. 4A).
Fig. 4.

Forest plots showing the difference in postoperative overall adverse events (A), postoperative medical complications (B), postoperative surgical complications (C), postoperative tendon healing failure (D), postoperative transfusion rate (E), postoperative discharge location (F), postoperative revision rate (G), postoperative re-admission rate within 90 days (H), and postoperative emergency department visit rate within 90 days (I). M-H: Mantel-Haenszel, CI: confidence interval.
When assessing medical and surgical complications separately, four studies on 619,833 subjects undergoing TSA [36-39] (59,675 with poor and 560,158 with good mental health) and one study on 135,489 subjects undergoing RCR [30] (68,397 with poor and 67,092 with good mental health) were included. No significant difference in medical or surgical complications was seen in the TSA cohort (OR, 2.24; 95% CI, 0.26–19.64; P=0.47) (Fig. 4B) (OR, 1.10; 95% CI, 0.47–2.56; P=0.83) (Fig. 4C) or when the cohorts were combined (OR, 2.11; 95% CI, 0.52–8.54; P=0.29) (Fig. 4B) (OR, 1.21; 95% CI, 0.61–2.38; P=0.59) (Fig. 4C). However, a higher rate of medical and surgical complications was identified in patients with poor mental health undergoing RCR (OR, 1.67; 95% CI, 1.63–1.71; P<0.00001) (Fig. 4B) (OR, 1.60; 95% CI, 1.54–1.66; P<0.00001) (Fig. 4C).
Tendon healing failure
Two studies enrolling 363 subjects undergoing RCR [32,42] (79 with poor and 284 with good mental health) reported data on postoperative tendon healing failure. Ultimately, no significant difference was observed (OR, 1.08; 95% CI, 0.27–4.32; P=0.91) (Fig. 4D).
Transfusions
Three studies enrolling 597,210 subjects undergoing TSA [36,37,39] (56,466 with poor and 540,744 with good mental health) and one study of 135,489 subjects undergoing RCR [30] (68,397 with poor and 67,092 with good mental health) reported data on postoperative transfusions. There was no significant difference in the rate of transfusions in patients undergoing TSA (OR, 5.11; 95% CI, 0.61–42.94; P=0.13) (Fig. 4E) and when both cohorts were combined (OR, 3.56; 95% CI, 0.58–21.70; P=0.17) (Fig. 4E). However, a higher rate of transfusions was documented in patients with poor mental health undergoing RCR (OR, 1.2; 95% CI, 1.12–1.28; P<0.00001) (Fig. 4E).
Non-homebound discharge
Three studies enrolling 595,507 subjects undergoing TSA [36,38,39] (55,591 with poor and 539,916 with good mental health) reported data on postoperative discharge location. There was no significant difference between the two groups (OR, 1.34; 95% CI, 0.49–4364; P=0.57) (Fig. 4F).
Revision
Two studies enrolling 23,219 subjects undergoing TSA [28,38] (3,427 with poor and 19,792 with good mental health) and one study of 816 subjects undergoing RCR [43] (232 with poor and 584 with good mental health) reported data on rates of revision surgery. A higher rate of revision was seen in patients with poor mental health undergoing TSA (OR, 2.20; 95% CI, 1.71–2.83; P<0.00001) (Fig. 4G), RCR (OR, 2.02; 95% CI, 0.99–4.13; P=0.05) (Fig. 4G), and when the cohorts were combined (OR, 2.17; 95% CI, 1.71–2.76; P<0.00001) (Fig. 4G).
Re-admission (90 days)
One study of 22,623 subjects undergoing TSA [38] (3,209 with poor and 19,414 with good mental health) and two studies enrolling 136,305 subjects undergoing RCR [30,43] (68,629 with poor and 67,676 with good mental health) reported data on the postoperative rate of re-admissions within 90 days. A higher rate of re-admissions was seen in patients with poor mental health undergoing TSA (OR, 1.70; 95% CI, 1.43–2.00; P<0.00001) (Fig. 4H). Meanwhile, the difference in rates was not significant in patients undergoing RCR (OR, 54.02; 95% CI, 0.00–284,425,501; P=0.61) (Fig. 4H) or when the cohorts were combined (OR, 16.06; 95% CI, 0.01–20529; P=0.66) (Fig. 4H).
ED visits (90 days)
One study of 22,623 subjects undergoing TSA [38] (3,209 with poor and 19,414 with good mental health) and one study of 816 subjects undergoing RCR [43] (232 with poor and 584 with good mental health) reported data on the postoperative rate of ED visits within 90 days. A higher rate of ED visits was recorded in patients with poor mental health undergoing TSA (OR, 1.43; 95% CI, 1.28–1.60; P<0.00001) (Fig. 4I), RCR (OR, 1.90; 95% CI, 1.06–3.41; P=0.03) (Fig. 4I), and when the cohorts were combined (OR, 1.45; 95% CI, 1.30–1.61; P<0.00001) (Fig. 4I).
DISCUSSION
Contradictory results on the impact of preoperative mental health on outcomes after shoulder surgery have been reported. Thus, a meta-analysis was necessary to examine this relationship and produce robust conclusions. Our results revealed better PROs, including ASES and SST scores; fewer adverse events, including reduced numbers of both medical and surgical complications; and lower rates of transfusions, revision surgery, 90-day re-admissions, and ED visits in patients with good preoperative mental health.
Although the postoperative ASES score was statistically better in patients with good preoperative mental health, the difference did not reach clinical significance in the TSA, RCR, or combined cohort. The MDs observed in our cohorts were 9.73 for TSA and 10.42 for RCR, both of which are below the ASES minimal clinically important differences (MCIDs) for patients undergoing TSA (20.9) and RCR (27.1) [44,45]. Furthermore, when assessing the improvement in ASES, only patients with good mental health in the TSA cohort showed significantly better scores, and this finding was not clinically significant. The same pattern of results was seen in SST in that the difference was significant but did not reach the MCID in the TSA (2.4) or RCR (4.3) group [44,45]. No difference in VAS, satisfaction, or ROM between patients with poor and good mental health was seen in either cohort. Thus, although mental health might impact the PROs of RCR and TSA patients, this impact was not of clinical significance, supporting some of the included studies [40,41].
A higher rate of overall complications (both medical and surgical combined) was seen in the group with poor preoperative mental health; however, there was no significant difference in complications when they were divided into medical and surgical complication subgroups. Furthermore, the difference in transfusion rate was not significant when the two cohorts were combined. This discrepancy between the rate of overall complications and the rates of surgical and medical complications separately may be explained by the inclusion of four studies reporting data on overall rather than specific adverse events [28,40,42,43]. Despite these findings, the correlation between psychiatric comorbidities and postoperative complications has not been fully characterized. Additionally, the influence of commonly prescribed psychiatric medications like selective-serotonin re-uptake inhibitors (SSRIs) may influence outcomes after shoulder surgery. Studies have demonstrated that side effects of SSRIs can mimic some of the known adverse events or the negative impact of psychological distress on the immune system [28,38,39]. Furthermore, both overall revisions and ED department visits within 90 days were significantly more common in the poor mental health group. As for the re-admission rate and discharge location, the difference was not significant. This increased rate of revision surgeries could also be well explained by the same reasons justifying the higher rate of complications as well as by the number of adverse events themselves [28,38,39]. Another explanation for the higher revision rate could be the impact of poor mental health on compliance with the postoperative protocol and rehabilitation [46,47]. However, a more in-depth analysis of the underlying mechanisms driving the association between poor mental health and higher adverse events and revision rates is needed to confirm our proposed relationships as these were not explored in our study nor in the literature.
Strengths and Limitations
The main limitation of this study is the high heterogeneity observed among studies, which could be partially explained by the different ways in which preoperative mental health was characterized in the included studies and therefore by the pooling of patients with different psychiatric comorbidities (depression, anxiety) or signs of poor psychological functioning, such as low resilience or distress) into the same group of poor mental health. Furthermore, studies using national databases were included, which could have potentially led to duplicate/overlapping patients. One last limitation is the low number of studies with data for some of the studied parameters.
This study also has several strengths. To our knowledge, it is the first meta-analysis to study the impact of preoperative mental health on the outcomes of shoulder surgery, including TSA and RCR. Moreover, only comparative studies were included, reducing the risk of operative and matching biases, and the selection process was stricter.
CONCLUSIONS
Patients with poor preoperative mental health demonstrated statistically lower ASES and SST scores in the TSA cohort, RCR cohort, and combined cohort, although these findings were not clinically significant. VAS score, satisfaction, ER, and flexion did not differ between the two mental health groups. Increased rates of adverse events and transfusions were observed in RCR patients, while increased re-admission rates were observed in TSA patients. Finally, higher rates of revision surgery and ED visits were observed in both RCR and TSA patients with poor preoperative mental health. Additional research using standardized definitions for good and poor mental health is needed to characterize the relationship between mental health and adverse events. Examining the effects of preoperative screening and treatment of mental health disorders on orthopedic surgical outcomes may also be beneficial.
Footnotes
Author contributions
Investigation: all authors. Writing – original draft: all authors. Writing Writing – review & editing: all authors.
Conflict of interest
JAA would like to disclose royalties from: DJO Global, Zimmer-Biomet, Smith and Nephew, Stryker, Globus Medical, Inc.; research support as a PI from: Lima Corporation - Italy, Orthofix, Arthrex, OREF; royalties, financial or material support from: Wolters Kluwer; and board member/committee appointments for: American Shoulder and Elbow Society, Pacira. No other potential conflict of interest relevant to this article was reported.
Funding
None.
Data availability
None.
Acknowledgments
None.
REFERENCES
- 1.World Health Organization . World Health Organization; 2022. Mental disorders: key facts [Internet] [cited 2024 Mar 1]. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders. [Google Scholar]
- 2.Barlattani T, D’Amelio C, Capelli F, et al. Suicide and COVID-19: a rapid scoping review. Ann Gen Psychiatry. 2023;22:10. doi: 10.1186/s12991-023-00441-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593–602. doi: 10.1001/archpsyc.62.6.593. [DOI] [PubMed] [Google Scholar]
- 4.Daher M, Fares MY, Boufadel P, Khanna A, Zalaquett Z, Abboud JA. Osteoporosis in the setting of shoulder arthroplasty: a narrative review. Geriatr Orthop Surg Rehabil. 2023;14:21514593231182527. doi: 10.1177/21514593231182527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pearl A, Ismail A, Alsadi T, Crespi Z, Daher M, Saleh K. Frailty and pre-frailty in the setting of total joint arthroplasty: a narrative review. Geriatr Orthop Surg Rehabil. 2023;14:21514593231188864. doi: 10.1177/21514593231188864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Daher M, Zalaquett Z, Fares MY, Boufadel P, Khanna A, Abboud JA. Osteoporosis in the setting of rotator cuff repair: a narrative review. Shoulder Elb. 2023 Oct 17; doi: 10.1177/175857322312073. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hasan A, Pearl A, Daher M, Saleh KJ. Patient genetic heterogeneities acting as indicators of post-operative pain and opioid requirement in orthopedic surgery: a systematic review. J Opioid Manag. 2024;20:77–85. doi: 10.5055/jom.0809. [DOI] [PubMed] [Google Scholar]
- 8.Makanji H, Solomito MJ, Kostyun R, Esmende S. Influence of anxiety and depression on opioid use following lumbar spine fusion: a large database study. Clin Spine Surg. 2024;37:E24–9. doi: 10.1097/BSD.0000000000001505. [DOI] [PubMed] [Google Scholar]
- 9.Lo YT, Lim-Watson M, Seo Y, et al. Long-term opioid prescriptions after spine surgery: a meta-analysis of prevalence and risk factors. World Neurosurg. 2020;141:e894–920. doi: 10.1016/j.wneu.2020.06.081. [DOI] [PubMed] [Google Scholar]
- 10.Kowalski C, Ridenour R, McNutt S, et al. Risk factors for prolonged opioid use after spine surgery. Global Spine J. 2023;13:683–8. doi: 10.1177/21925682211003854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cunningham DJ, LaRose MA, Klifto CS, Gage MJ. Mental health and substance use affect perioperative opioid demand in upper extremity trauma surgery. J Shoulder Elbow Surg. 2021;30:e114–20. doi: 10.1016/j.jse.2020.06.024. [DOI] [PubMed] [Google Scholar]
- 12.Sharma AK, Elbuluk AM, Gkiatas I, Kim JM, Sculco PK, Vigdorchik JM. Mental health in patients undergoing orthopaedic surgery: diagnosis, management, and outcomes. JBJS Rev. 2021;9:e20.00169. doi: 10.2106/JBJS.RVW.20.00169. [DOI] [PubMed] [Google Scholar]
- 13.Chan AK, Shaffrey CI, Park C, et al. Do comorbid self-reported depression and anxiety influence outcomes following surgery for cervical spondylotic myelopathy. J Neurosurg Spine. 2023;39:11–27. doi: 10.3171/2023.2.SPINE22685. [DOI] [PubMed] [Google Scholar]
- 14.Pensak MJ, Carry PM, Entin JM, Lalka A, Shourbaji NA, Scott FA. Depression and anxiety among patients with atraumatic lateral epicondylitis and ulnar-sided wrist pain. J Wrist Surg. 2019;8:295–9. doi: 10.1055/s-0039-1685451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ghoshal A, Bhanvadia S, Singh S, Yaeger L, Haroutounian S. Factors associated with persistent postsurgical pain after total knee or hip joint replacement: a systematic review and meta-analysis. Pain Rep. 2023;8:e1052. doi: 10.1097/PR9.0000000000001052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Park C, Garcia AN, Cook C, Gottfried ON. Effect of change in preoperative depression/anxiety on patient outcomes following lumbar spine surgery. Clin Neurol Neurosurg. 2020;199:106312. doi: 10.1016/j.clineuro.2020.106312. [DOI] [PubMed] [Google Scholar]
- 17.Daher M, Boufadel P, Lopez R, Chalhoub R, Fares MY, Abboud JA. Beyond the joint: exploring the interplay between mental health and shoulder arthroplasty outcomes. J Orthop. 2024;52:1–5. doi: 10.1016/j.jor.2024.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.DiSilvestro KJ, Bond D, Alsoof D, et al. Preoperative resilience and early postoperative outcomes following lumbar spinal fusion. World Neurosurg. 2022;163:e573–8. doi: 10.1016/j.wneu.2022.04.030. [DOI] [PubMed] [Google Scholar]
- 19.Zabat MA, Lygrisse KA, Sicat CS, Pope C, Schwarzkopf R, Slover JD. The impact of patient resilience on discharge after total hip arthroplasty. J Arthroplasty. 2022;37(7S):S493–7. doi: 10.1016/j.arth.2022.01.070. [DOI] [PubMed] [Google Scholar]
- 20.Cremeans-Smith JK, Greene K, Delahanty DL. Resilience and recovery from total knee arthroplasty (TKA): a pathway for optimizing patient outcomes. J Behav Med. 2022;45:481–9. doi: 10.1007/s10865-022-00287-5. [DOI] [PubMed] [Google Scholar]
- 21.Magaldi RJ, Staff I, Stovall AE, Stohler SA, Lewis CG. Impact of resilience on outcomes of total knee arthroplasty. J Arthroplasty. 2019;34:2620–3. doi: 10.1016/j.arth.2019.06.008. [DOI] [PubMed] [Google Scholar]
- 22.Mo KC, Gupta A, Movsik J, et al. Pain Self-Efficacy (PSEQ) score of <22 is associated with daily opioid use, back pain, disability, and PROMIS scores in patients presenting for spine surgery. Spine J. 2023;23:723–30. doi: 10.1016/j.spinee.2022.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Srivastava K. Positive mental health and its relationship with resilience. Ind Psychiatry J. 2011;20:75–6. doi: 10.4103/0972-6748.102469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Agarwalla A, Lu Y, Chang E, et al. Influence of mental health on postoperative outcomes in patients following biceps tenodesis. J Shoulder Elbow Surg. 2020;29:2248–56. doi: 10.1016/j.jse.2020.03.020. [DOI] [PubMed] [Google Scholar]
- 25.Rauck RC, Ruzbarsky JJ, Swarup I, et al. Predictors of patient satisfaction after reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2020;29:e67–74. doi: 10.1016/j.jse.2019.07.043. [DOI] [PubMed] [Google Scholar]
- 26.Belayneh R, Haglin J, Lott A, Kugelman D, Konda S, Egol KA. Underlying mental illness and psychosocial factors are predictors of poor outcomes after proximal humerus repair. J Orthop Trauma. 2019;33:e339–44. doi: 10.1097/BOT.0000000000001494. [DOI] [PubMed] [Google Scholar]
- 27.Hines AC, Pill SG, Boes N, et al. Mental health status, not resilience, influences functional recovery after arthroscopic rotator cuff repairs. J Shoulder Elbow Surg. 2022;31(6S):S117–22. doi: 10.1016/j.jse.2022.02.005. [DOI] [PubMed] [Google Scholar]
- 28.Colasanti CA, Lin CC, Anil U, Simovitch RW, Virk MS, Zuckerman JD. Impact of mental health on outcomes after total shoulder arthroplasty. J Shoulder Elbow Surg. 2023;32:980–90. doi: 10.1016/j.jse.2022.10.028. [DOI] [PubMed] [Google Scholar]
- 29.Gowd AK, Cvetanovich GL, Liu JN, et al. Preoperative mental health scores and achieving patient acceptable symptom state are predictive of return to work after arthroscopic rotator cuff repair. Orthop J Sports Med. 2019;7:2325967119878415. doi: 10.1177/2325967119878415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Freshman RD, Oeding JF, Anigwe C, et al. Pre-existing mental health diagnoses are associated with higher rates of postoperative complications, readmissions, and reoperations following arthroscopic rotator cuff repair. Arthroscopy. 2023;39:185–95. doi: 10.1016/j.arthro.2022.06.040. [DOI] [PubMed] [Google Scholar]
- 31.Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Park JH, Rhee SM, Kim HS, Oh JH. Effects of anxiety and depression measured via the hospital anxiety and depression scale on early pain and range of motion after rotator cuff repair. Am J Sports Med. 2021;49:314–20. doi: 10.1177/0363546520976574. [DOI] [PubMed] [Google Scholar]
- 33.Porter A, Hill MA, Harm R, Greiwe RM. Resiliency influences postoperative outcomes following rotator cuff repair. J Shoulder Elbow Surg. 2021;30:1181–5. doi: 10.1016/j.jse.2020.08.024. [DOI] [PubMed] [Google Scholar]
- 34.Potter MQ, Wylie JD, Granger EK, Greis PE, Burks RT, Tashjian RZ. One-year patient-reported outcomes after arthroscopic rotator cuff repair do not correlate with mild to moderate psychological distress. Clin Orthop Relat Res. 2015;473:3501–10. doi: 10.1007/s11999-015-4513-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Thorpe AM, O’Sullivan PB, Mitchell T, et al. Are psychologic factors associated with shoulder scores after rotator cuff surgery. Clin Orthop Relat Res. 2018;476:2062–73. doi: 10.1097/CORR.0000000000000389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bot AG, Menendez ME, Neuhaus V, Ring D. The influence of psychiatric comorbidity on perioperative outcomes after shoulder arthroplasty. J Shoulder Elbow Surg. 2014;23:519–27. doi: 10.1016/j.jse.2013.12.006. [DOI] [PubMed] [Google Scholar]
- 37.Diamond KB, Gordon AM, Sheth BK, Romeo AA, Choueka J. How does depressive disorder impact outcomes in patients with glenohumeral osteoarthritis undergoing primary reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2023;32:1886–92. doi: 10.1016/j.jse.2023.03.013. [DOI] [PubMed] [Google Scholar]
- 38.Lunati MP, Wilson JM, Farley KX, Gottschalk MB, Wagner ER. Preoperative depression is a risk factor for complication and increased health care utilization following total shoulder arthroplasty. J Shoulder Elbow Surg. 2021;30:89–96. doi: 10.1016/j.jse.2020.04.015. [DOI] [PubMed] [Google Scholar]
- 39.Mollon B, Mahure SA, Ding DY, Zuckerman JD, Kwon YW. The influence of a history of clinical depression on peri-operative outcomes in elective total shoulder arthroplasty: a ten-year national analysis. Bone Joint J. 2016;98:818–24. doi: 10.1302/0301-620X.98B6.37208. [DOI] [PubMed] [Google Scholar]
- 40.Porter A, Greiwe RM. Psychological disorders confer poor functional outcomes after reverse total shoulder arthroplasty. JSES Rev Rep Tech. 2021;1:357–60. doi: 10.1016/j.xrrt.2021.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Werner BC, Wong AC, Chang B, et al. Depression and patient-reported outcomes following total shoulder arthroplasty. J Bone Joint Surg Am. 2017;99:688–95. doi: 10.2106/JBJS.16.00541. [DOI] [PubMed] [Google Scholar]
- 42.Dujeux C, Antoni M, Thery C, Eichler D, Meyer N, Clavert P. History of mood and anxiety disorders does not affect the outcomes of arthroscopic rotator cuff repair. Orthop Traumatol Surg Res. 2023;109:103550. doi: 10.1016/j.otsr.2023.103550. [DOI] [PubMed] [Google Scholar]
- 43.Johnson AH, York JJ, Lashgari CJ, Petre BM, Turcotte JJ, Redziniak DE. Effects of preexisting depression and anxiety on postoperative outcomes following arthroscopic rotator cuff repair. JSES Int. 2022;6:984–8. doi: 10.1016/j.jseint.2022.07.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Tashjian RZ, Hung M, Keener JD, et al. Determining the minimal clinically important difference for the American Shoulder and Elbow Surgeons score, Simple Shoulder Test, and visual analog scale (VAS) measuring pain after shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26:144–8. doi: 10.1016/j.jse.2016.06.007. [DOI] [PubMed] [Google Scholar]
- 45.Tashjian RZ, Shin J, Broschinsky K, et al. Minimal clinically important differences in the American Shoulder and Elbow Surgeons, Simple Shoulder Test, and visual analog scale pain scores after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2020;29:1406–11. doi: 10.1016/j.jse.2019.11.018. [DOI] [PubMed] [Google Scholar]
- 46.Paolucci S, Antonucci G, Pratesi L, Traballesi M, Grasso MG, Lubich S. Poststroke depression and its role in rehabilitation of inpatients. Arch Phys Med Rehabil. 1999;80:985–90. doi: 10.1016/s0003-9993(99)90048-5. [DOI] [PubMed] [Google Scholar]
- 47.Ahn DH, Lee YJ, Jeong JH, Kim YR, Park JB. The effect of post-stroke depression on rehabilitation outcome and the impact of caregiver type as a factor of post-stroke depression. Ann Rehabil Med. 2015;39:74–80. doi: 10.5535/arm.2015.39.1.74. [DOI] [PMC free article] [PubMed] [Google Scholar]