

Abstract
Background and Objectives
It remains unknown whether the associations between protective lifestyles and sporadic dementia risk reported in observational studies also affect age at symptom onset (AAO) in autosomal dominant Alzheimer disease (ADAD) with predominant genetic influences. We investigated the associations between resilience-related life experiences and interindividual AAO variability in ADAD.
Methods
We performed a longitudinal and confirmatory analysis of the Dominantly Inherited Alzheimer Network prospective observational cohort (January 2009–June 2018, follow-up duration 2.13 ± 2.22 years), involving clinical, CSF, and lifestyle/behavioral assessments. We performed a 2-pronged comprehensive resilience assessment in each cohort. Cohort 1, incorporating the general resilience definition (cognitive maintenance [Clinical Dementia Rating = 0] despite high pathology), included carriers during the periods of significant CSFp-tau181 variability and grouped into resilience/resistance outcome bins according to the dichotomous pathologic and cognitive statuses, subcategorized by the estimated years from expected symptom onset (EYO). Cohort 2, focused on ADAD-specific genetically determined time frame characterizing the onset predictability, included asymptomatic participants with available preclinical lifestyle data and AAO outcomes and grouped into delayed or earlier AAO relative to the parental AAO. Associations of cognitive, CSFp-tau181, and lifestyle/behavioral predictors with binary outcomes were investigated using logistic regression.
Results
Of 320 carriers (age 38.19 ± 10.94 years, female 56.25%), cohort 1 included 218 participants (39.00 ± 9.37 years, 57.34%) and cohort 2 included 28 participants (43.34 ± 7.40 years, 71.43%). In cohort 1, 218 carriers after −20 EYO, when the interindividual variability (SD) of CSFp-tau181 first became more than twice greater in carriers than in noncarriers, were grouped into low-risk control (asymptomatic, low pathology, n = 103), high-resilience (asymptomatic despite high pathology, n = 60), low-resilience (symptomatic despite low pathology, n = 15), and susceptible control (symptomatic, high pathology, n = 40) groups. Multivariable predictors of high resilience, controlling for age and depression, included higher conscientiousness (odds ratio 1.051 [95% CI 1.016–1.086], p = 0.004), openness to experience (1.068 [1.005–1.135], p = 0.03) (vs. susceptible controls), and agreeableness (1.082 [1.015–1.153], p = 0.02) (vs. low resilience). From 1 to 3 years before parental AAO (cohort 2), the multivariable predictor of delayed AAO, controlling for CSFp-tau181, was higher conscientiousness (0.916 [0.845–0.994], p = 0.036).
Discussion
Among the cognitively and socially integrated life experiences associated with resilience, measures of conscientiousness were useful indicators for evaluating resilience and predicting future dementia onset in late preclinical ADAD.
Introduction
In autosomal dominant Alzheimer disease (ADAD), the age at symptom onset (AAO) is similar across generations, enabling the prediction of an individual's AAO based on that of their parent. In a systematic review investigating the factors influencing AAO in 387 ADAD families, a substantial proportion of the observed interindividual variability in AAO was explained by family pathogenic variation type (eAppendix 1, 2 and eFigure 1).1 However, in the Spanish GENODEM study of 162 ADAD probands, discrepancies in AAO between siblings were within 5 years in 44% of families, 6–10 years in 29%, and over 10 years in 27%,2 suggesting that both genetic and nongenetic modifiers contribute to interindividual variability in AAO. Grounded in Stern's concept,3 resilience implies an individual's ability to maintain cognition despite significant pathology, contrasting with resistance, which involves lower-than-expected pathology levels by clearance mechanisms.3,4 There is interest in identifying the neurobiological mechanisms underlying resilience and the associated nongenetic lifestyle contributors that can be reinforced through an individual's own will and effort.
After the current challenges of pharmacologic trials targeting AD pathology, the focus of AD health care policies has shifted to resilience-promoting lifestyle interventions in at-risk populations, which have cost and safety advantages and are applicable in low-income countries. Numerous observational studies5-12 and far fewer randomized controlled trials (RCTs)13-15 have reported promising associations between protective lifestyles and dementia risk in nondemented older populations (eAppendix 1, 3 and eFigure 2). Meta-analyses and large-scale studies have established that objectively measurable lifestyle variables—cognitive5 and leisure activities,6,7 exercise,8,9 social engagement,10 personality,11,12 and combined lifestyles13-15—are associated with a reduced dementia risk. Although some observational studies included participants with ongoing neurodegeneration, potentially causing reverse causality effect on the lifestyle of interest, participation in leisure activities was still protective against dementia risk after excluding participants with preclinical dementia.6 However, it remains unknown whether the associations between resilience-promoting lifestyles and dementia risk also affect dementia onset (measured here as AAO) in a younger population with predominant genetic influences (e.g., those with ADAD) (eAppendix 1, 4). Emerging research highlighted associations between healthy lifestyles and decreased sporadic dementia risk, even in subgroups with high genetic risk.16 Therefore, we hypothesized that although genetic influence predominates in determining AAO in ADAD, it may possibly be offset by modifiable lifestyle that individuals can change. The Dominantly Inherited Alzheimer Network (DIAN) is a privileged population for studying resilience due to the destined cascade of biomarker progression leading to symptomatic AD and the predictability of onset. Accordingly, we conducted a comprehensive assessment of resilience in the context of ADAD within each cohort, incorporating both the general resilience definition3,4 and the ADAD-specific genetically determined time frame. Although resilience is broadly defined as the capacity to maintain cognitive function despite adversity, in the context of ADAD, adversity not only encompasses high pathology but also extends being within the at-risk, expected postclinical period, when the participant's age at assessment exceeds the parental AAO, indicating the vulnerable period beyond the estimated years from expected symptom onset (EYO >0). Participants in cohort 1 were stratified into subgroups representing varying degrees of resilience or resistance based on the amount of tau pathology and symptomatic status and further subcategorized by their placement within the expected preclinical or postclinical periods, as indicated by their EYO. Resilience in cohort 1 was defined by cognitive maintenance (Clinical Dementia Rating [CDR] = 0) despite severe pathology while resistance was the state of lower-than-expected level of pathology. Specifically, participants in the EYO >0 period who exhibited high resilience/resistance were classified as having “very high” resilience/resistance. Despite the acknowledged clinical significance of onset predictability in ADAD, our investigation into cohort 2 aims to validate the contribution of nongenetic lifestyle to the observed AAO variability in ADAD, which was not attributable solely to family pathogenic variation. Resilience in cohort 2 was defined by a delayed AAO relative to parental AAO, assessed during an at-risk period with progressive pathology preceding onset. In this investigation, we pursued an overarching previous hypothesis confirming the nongenetic modifiable lifestyle contributor to ADAD within a 2-pronged conceptual framework. Within cohort 1, through comparative analyses of groups distinguished by high vs low levels of resilience or resistance, we aimed to confirm the impact of nongenetic lifestyle contributors more prominently associated with participants exhibiting higher resilience or resistance than with their less resilient or resistant counterparts. Proceeding to cohort 2, we aimed to validate that such nongenetic protective lifestyles, identified as significantly enhancing resilience in cohort 1, also contributed to delaying AAO despite the high pathologic load in ADAD.
Methods
Study Design and Participants
This prospective, longitudinal, and confirmatory study analyzed the DIAN observational cohort freeze 13 data (data/tissue ID: D1934) between January 26, 2009, and June 27, 2018. This cohort included participants (aged 18 years and older) from families with confirmed pathogenic variations in APP, PSEN1, and PSEN2 from 20 sites in 10 countries (National Institute on Aging grant no. U19AG032438; dian.wustl.edu; ClinicalTrials.gov no. NCT00869817).17,18 As a preliminary analysis, we commenced our study with presenting visualizations from the rawest 3-dimensional longitudinal lifestyle data level to determine the time frame with the most frequent and uniformly distributed visits among participants and selected representative lifestyle data for cohort 1 and 2 analyses. Observing the persistent divergence in modifiable lifestyle levels between asymptomatic and symptomatic carriers during the expected preclinical periods, we focused on analyzing preclinical lifestyle data in subsequent evaluations. In our study, we implemented 2 main methodological strategies, involving multivariable comparisons within cohorts 1 and 2. For cohort 1, we excluded symptomatic carriers whose first visit was >3 years from onset and included carriers during periods of significant interindividual variability in CSFp-tau181. We grouped them into discrete outcome bins representing different resilience/resistance statuses based on dichotomous pathologic and cognitive statuses, further subcategorized by expected pre/postclinical status. For cohort 2, the primary outcome was a binary AAO outcome: a delayed AAO (positive) or an AAO equal to or earlier than the parental AAO (negative). The eligibility criteria included (1) being asymptomatic at baseline, (2) having available preclinical lifestyle data, (3) having parental AAO information, and (4) having known AAO outcome information relative to the parental AAO, further divided into (4-1) participants who converted into symptomatic status during the enrollment period (thereby providing individual AAO information) and (4-2) those who remained asymptomatic throughout the enrollment period (thus lacking individual AAO information) but whose age at the last visit exceeded the parental AAO. We excluded (1) participants without preclinical lifestyle data (already symptomatic at baseline enrollment), (2) those who visited only after the parental AAO (EYO >0), and (3) those who were asymptomatic but had not reached their parental AAO (i.e., unknown AAO outcome).
Standard Protocol Approvals, Registrations, and Patient Consents
The Institutional Review Boards at Washington University in St. Louis and all participating sites approved the study protocol, which was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from each participant.
Clinical and Biochemical Evaluations
Participants underwent clinical and neuropsychological evaluation and genetic and biofluid examinations at each visit.17 Clinicians were blinded to biomarker and genetic statuses. Dementia status was determined using the CDR (symptomatic, CDR ≥0.5). Participants completed the Mini-Mental State Examination (MMSE), a comprehensive neuropsychological battery assessing memory, attention, executive function, visuospatial function, and language, and the Functional Assessment Questionnaire.17 Parental AAO was determined by a semistructured interview with family members about parental age at initial progressive cognitive decline. The estimated years from EYO was calculated by subtracting the parent's AAO from the participant's age at assessment.17 CSFtau phosphorylated at threonine-181 (CSFp-tau181) was measured by automated immunoassay (LUMIPULSEG1200, Fujirebio, Malverne, PA).17
Exercise and Personality Assessment
Exercise and personality were measured at each visit. Participants completed a self-reported questionnaire assessing the average weekly minutes spent on 10 different leisure-time physical activities over the past 12 months, weighted with metabolic equivalents (1 MET = resting energy expenditure rate) following the World Health Organization19 and the American College of Sports Medicine guidelines.20 Total physical activity volume (MET-minutes per week) was calculated by summing the average “minutes/week” weighted with a MET for each exercise item. Following the 2011 Compendium of Physical Activities recommendations,21 participant physical activity was categorized by intensity (MET): moderate intensity (MET 3.0–5.9) (e.g., Wii Fit [3.8 MET] and walking for pleasure [3.5 MET]) and high intensity (MET of ≥6.0) (e.g., swimming [6.0 MET], tennis [7.3 MET], and running [8.3 MET]). Structural elements of social lifestyles (marital status, living arrangements) were evaluated using collateral-reported social contact data. The quantitative measurements of personality traits were assessed with the International Personality Item Pool (IPIP-NEO-120),22 a 120-item questionnaire derived from a 5-factor model rated on a 5-point scale (1 = very inaccurate, 5 = very accurate). Self-reported or collateral-reported responses to individual items were summed into 5 major domains (neuroticism, extraversion, openness, agreeableness, and conscientiousness), each subdivided into 6 facets. The domain and facet scores (not individual items) were used in these analyses.
Statistical Analysis
Demographic and clinical characteristics were compared using independent t tests or Wilcoxon rank-sum tests for continuous variables and χ2 or Fisher exact tests for categorical variables. In each cohort, univariable logistic regressions were used to test the associations of predictors with binary outcomes. We assumed that data were missing at random and created multiple imputed data sets using the Markov chain Monte Carlo algorithm. Variables with p < 0.1 in the univariable regression were included in multivariable models by backward elimination. We constructed multivariable logistic regression models to test the associations of selected predictors with binary outcomes. A 2-sided p value <0.05 was considered statistically significant. Significance levels were determined by Bonferroni correction for multiple comparisons (p < 0.05/4 for pairwise comparisons). Data were analyzed using SAS version 9.4; R version 3.6.1 with ggplot2 and doBy packages; and Python version 3.9.12 with Numpy, Pandas, Matplotlib, Scipy, and Seaborn packages.
Data Availability
All data from this study are available on request from the DIAN at dian.wustl.edu/our-research/observational-study/dianobservationalstudy-investigator-resources/. Analysis codes can be obtained from the corresponding author (J.S.K.).
Results
Study Participants
Figure 1 shows the study profile and outcome group assignment (eTable 1, eFigure 3). We included 209 noncarriers and 320 carriers (age 38.19 ± 10.94 years, female [%] 180 [56.25%]), with 218 in cohort 1 (39.00 ± 9.37 years, 125 [57.34%]) and 28 in cohort 2 (43.34 ± 7.4 years, 20 [71.43%]) (eTable 2). Of the 320 carriers (194 asymptomatic and 105 symptomatic carriers, 21 converters), 240 (75.0%) had PSEN1, 24 (7.5%) had PSEN2, and 56 (17.5%) had APP (eTable 2). Participants were longitudinally followed for an average of 2.13 ± 2.22 years, with 77 (35.3%) having ≥3 visits (eTable 3).
Figure 1. Study Profile.

AAO = age at symptom onset; DIAN = Dominantly Inherited Alzheimer Network; EYO = estimated years from expected symptom onset.
Cohort 1
Different Resilience/Resistance Outcome Subsets by CSFp-tau181, Cognitive, and EYO Statuses
In cohort 1, the −20 EYO time point was identified, after which interindividual variability in longitudinal CSFp-tau181 levels and the SD of the CSFp-tau181 distribution at 2-year EYO intervals first started to be more than twice greater in carriers than in noncarriers (Figure 2, A and B, eTable 4). The CSFp-tau181 pathology cutoff level (51.52 pg/mL) was determined at 2 SDs from the mean level in asymptomatic noncarriers across the entire EYO range. After selecting 1 representative data point per participant at the nearest point from onset, the last preclinical visits in 143 asymptomatic carriers and 20 converters and the first postclinical visits in 55 symptomatic carriers (1.50 ± 1.02 years from onset) and 218 carriers after −20 EYO were grouped into 4 primary outcome subsets based on dichotomous pathologic and cognitive statuses, subcategorized by expected pre/postclinical (EYO) status: 103 low-risk controls (asymptomatic, low pathology, group 1), 60 high-resilience (asymptomatic despite high pathology, group 2), 15 low-resilience (symptomatic despite low pathology, group 3), and 40 susceptible controls (symptomatic, high pathology, group 4) (Table 1, eTables 5 and 6).
Figure 2. Determination of the Analytical Population in Cohort 1 (A and B) and Cohort 2 (C and D).

(A) Cohort 1. Interindividual variability in longitudinal CSFp-tau181 levels plotted against estimated years from expected symptom onset (EYO) in 194 asymptomatic carriers (shown in red, 386 visits), 21 converters (shown in orange, 68 visits), and 64 symptomatic carriers (shown in blue, 161 visits) whose first visits were within 3 years from actual symptom onset and 202 asymptomatic noncarriers (shown in green, 406 visits). The vertical dashed line at 0 years represents the expected point of parental symptom onset. Negative EYO values represent the expected preclinical period. Positive values indicate the expected postclinical period. The vertical solid line at −20 years indicates the time point after which the SD of the distribution of CSFp-tau181 levels at 2-year EYO intervals first started to be more than twice greater in pathogenic variation carriers than in noncarriers, according to the method described in (B). The horizontal dashed line indicates the CSFp-tau181 pathology cutoff level (CSFp-tau181 level of 51.52 pg/mL) at 2 SDs from the mean CSFp-tau181 level in asymptomatic noncarriers across the entire EYO range. (B) Cohort 1. Interindividual variability in longitudinal CSFp-tau181 levels, represented as the SD of the CSFp-tau181 levels at 2-year EYO intervals, was plotted against the EYO for pathogenic variation carriers (194 asymptomatic carriers, 21 converters, and 64 symptomatic carriers) and 202 noncarriers. The vertical dashed line at −20 years indicates the time point from which the SD of the CSFp-tau181 distribution at 2-year EYO intervals first started to be more than twice as high in pathogenic variation carriers than noncarriers. Because of the low number of participants with data points located at the extremes of the graph, the SDs of the CSFp-tau181 levels for these participants in the time frame before the −30 EYO and after the +15 EYO were calculated as −35 EYO to −30 EYO (n = 3) and +15 EYO to +28 EYO (n = 15), respectively (additional data in eTable 4). (C) Cohort 2. The process of selecting the representative visit data for exposure and covariate (lifestyle, clinical, and pathology) variables among the multiple visits of individuals. The EYO range in which visits were most frequently and uniformly distributed before onset was −3.04 ± 3.21 EYO. Visit data from 2 outlier individuals (marked with an asterisk) were excluded from the subsequent analysis. (D) Cohort 2. The selected representative visits among multiple visits per participant included in the final analysis. After excluding visit data from 2 outlier participants (marked with an asterisk in Figure 2C), the EYO range in which visits were most frequently and uniformly distributed before onset was −2.45 ± 2.18 EYO. To minimize interindividual variance in EYO time points, we selected the 1 representative visit per participant nearest to the mean EYO (−2.45 EYO) among −2.45 ± 2.18 EYO; the mean of the chosen visits was −1.80 ± 1.08 EYO. The positive outcome group with 15 participants consisted of 11 asymptomatic carriers (purple dots) whose age at the last visit was equal to or greater than the parental age at symptom onset (AAO) and 4 converters (red dots) whose AAO was later than the parental AAO. The negative outcome group with 13 participants consisted of all converters (blue dots).
Table 1.
Patient Demographic, Clinical, and Lifestyle Characteristics for the 4 Primary Outcome Groups, Determined According to Combinations of Cognitive and Pathologic Statuses (the Low-Risk Control, High-Resilience, Low-Resilience, and High-Risk Susceptible Control Groups) in Cohort 1
| Variable | Low-risk control group (asymptomatic, low pathology; group 1) (n = 103) | High-resilience group (asymptomatic, high pathology; group 2) (n = 60) | Low-resilience group (symptomatic, low pathology; group 3) (n = 15) | High-risk susceptible control group (symptomatic, high pathology; group 4) (n = 40) | p Valuea | p Valueb | p Valuec | p Valued |
| Group 2 vs group 4 | Group 2 vs group 3 | Group 2 vs group 1 | Group 1 vs group 3 | |||||
| Demographic information | ||||||||
| Racee | ||||||||
| Asian | <3 (1.98) | <3 (3.33) | 0 (0) | <3 (5) | 0.19 | 0.75 | 0.94 | 0.76 |
| Black or African American | <3 (0.99) | 0 (0) | 0 (0) | 0 (0) | ||||
| Native Hawaiian or other Pacific Islander | <3 (0.99) | <3 (1.67) | 0 (0) | 0 (0) | ||||
| White | 92 (91.09) | 55 (91.67) | 14 (93.33) | 33 (82.5) | ||||
| Otherf | 5 (4.95) | <3 (3.33) | <3 (6.67) | 5 (12.5) | ||||
| Sex (female) | 57 (55.34) | 38 (63.33) | 10 (66.67) | 20 (50) | 0.19 | 0.81 | 0.32 | 0.41 |
| Visit age, y | 36.77 ± 9.69 | 38.38 ± 7.53 | 44.47 ± 9.61 | 43.63 ± 8.78 | 0.002 | 0.010 | 0.24 | 0.005 |
| Years of education | 15.09 ± 2.97 | 14.07 ± 2.55 | 12.47 ± 3.87 | 13.68 ± 4.03 | 0.50 | 0.14 | 0.03 | 0.009 |
| Occupational score | 3.64 ± 1.55 | 3.52 ± 1.41 | 4.40 ± 1.72 | 4.23 ± 1.76 | 0.04 | 0.07 | 0.77 | 0.11 |
| Genetics | ||||||||
| APOE | ||||||||
| 22, 23 | 10 (9.71) | 6 (10) | <3 (13.33) | 5 (12.5) | 0.56 | 0.25 | 0.32 | 0.63 |
| 33 | 68 (66.02) | 33 (55) | 11 (73.33) | 25 (62.5) | ||||
| 24, 34, 44 | 25 (24.27) | 21 (35) | <3 (13.33) | 10 (25) | ||||
| Family pathogenic variation | ||||||||
| PSEN1 | 64 (62.14) | 51 (85) | 12 (80) | 35 (87.5) | 0.05 | 0.11 | 0.003 | 0.34 |
| PSEN2 | 14 (13.59) | 6 (10) | 0 (0) | 0 (0) | ||||
| APP | 25 (24.27) | 3 (5) | 3 (20) | 5 (12.5) | ||||
| Present illness | ||||||||
| Traumatic brain injury (present) | 13 (12.62) | 5 (8.62) | <3 (14.29) | 3 (7.5) | 1.00 | 0.62 | 0.44 | 1.00 |
| Hypertension (present) | 11 (10.68) | <3 (3.33) | <3 (13.33) | 4 (10) | 0.21 | 0.18 | 0.13 | 0.67 |
| Hypercholesterolemia (present) | 16 (15.69) | 6 (10.53) | 5 (33.33) | 4 (10.53) | 1.00 | 0.04 | 0.37 | 0.14 |
| Diabetes (present) | <3 (1.94) | 0 (0) | <3 (13.33) | 0 (0) | — | 0.04 | 0.53 | 0.08 |
| Thyroid disease (present) | 8 (8.08) | <3 (1.69) | 0 (0) | <3 (5.26) | 0.56 | 1.00 | 0.16 | 0.59 |
| Psychiatric disease (present) | 11 (10.68) | 8 (13.33) | 4 (26.67) | 6 (15) | 0.81 | 0.24 | 0.61 | 0.10 |
| Depression (present) | 9 (8.74) | 9 (15) | 9 (60) | 22 (55) | <0.001 | 0.001 | 0.22 | <0.001 |
| History of stroke (present) | <3 (0.97) | 0 (0) | 0 (0) | 3 (7.5) | 0.06 | — | 1.00 | 1.00 |
| Hachinski ischemic score | ||||||||
| 0 | 94 (91.26) | 55 (91.67) | 10 (66.67) | 26 (65) | 0.001 | 0.011 | 1.00 | 0.001 |
| 1 | 8 (7.77) | 4 (6.67) | <3 (6.67) | 6 (15) | ||||
| 2–7 | <3 (0.97) | <3 (1.67) | 4 (26.67) | 8 (20) | ||||
| Tobacco 100 (yes) | 38 (36.89) | 33 (55) | 8 (53.33) | 18 (45) | 0.33 | 0.91 | 0.02 | 0.22 |
| Packs per day | ||||||||
| 1 cigarette–0.5 pack | 25 (24.27) | 11 (18.64) | 3 (21.43) | 10 (26.32) | 0.47 | 0.94 | 0.05 | 0.15 |
| 0.5–1 pack | 10 (9.71) | 15 (25.42) | 4 (28.57) | 5 (13.16) | ||||
| 1–1.5 pack | 5 (4.85) | 4 (6.78) | <3 (7.14) | <3 (5.26) | ||||
| N/A | 63 (61.17) | 29 (49.15) | 6 (42.86) | 21 (55.26) | ||||
| Alcohol use (yes) | <3 (1.94) | 5 (8.33) | <3 (13.33) | 3 (7.5) | 1.00 | 0.62 | 0.10 | 0.08 |
| Substance abuse (yes) | 4 (3.88) | 7 (11.67) | 3 (20) | 5 (12.82) | 1.00 | 0.41 | 0.10 | 0.04 |
| Social contact | ||||||||
| Cohabitating (yes) | 72 (69.9) | 42 (70) | 9 (60) | 32 (80) | 0.26 | 0.54 | 0.99 | 0.55 |
| Living status | ||||||||
| Lives alone | 14 (13.59) | 6 (10) | 3 (20) | 4 (10) | 0.95 | 0.21 | 0.49 | 0.06 |
| Lives with spouse or partner | 75 (72.82) | 42 (70) | 7 (46.67) | 27 (67.5) | ||||
| Lives with relative, friend, group, or others | 14 (13.59) | 12 (20) | 5 (33.33) | 9 (22.5) | ||||
| Residency (single family residence) | 102 (99.03) | 59 (98.33) | 14 (93.33) | 38 (95) | 0.56 | 0.36 | 1.00 | 0.24 |
| Able to live independently (yes) | 101 (99.02) | 60 (100) | 12 (80) | 27 (67.5) | <0.001 | 0.007 | 1.00 | 0.006 |
| Marital status | ||||||||
| Married, living as married | 31 (30.10) | 19 (31.67) | 8 (53.33) | 12 (30) | 0.86 | 0.12 | 0.83 | 0.09 |
| Other (widowed, divorced, separated, or never married) | 72 (69.90) | 41 (68.33) | 7 (46.67) | 28 (70) | ||||
| Physical activity | ||||||||
| Total physical activity volume | 3,014.28 ± 4,078.87 | 1,763.08 ± 1,823.14 | 2,030.47 ± 2,573.54 | 2,096.08 ± 2,149.80 | 0.49 | 0.96 | 0.08 | 0.31 |
| Moderate-intensity exercise (3.0–5.9 METs) | 1,497.43 ± 2,182.21 | 869.13 ± 1,455.50 | 652.87 ± 532.08 | 751.30 ± 968.47 | 0.76 | 0.93 | 0.03 | 0.25 |
| High-intensity exercise (≥6.0 METs) | 1,516.84 ± 2,788.39 | 893.95 ± 1,232.77 | 1,377.60 ± 2,184.43 | 1,379.26 ± 1,960.59 | 0.28 | 0.87 | 0.15 | 0.64 |
| IPIP | ||||||||
| Collateral-reported scores | ||||||||
| Neuroticism | 58.26 ± 14.78 | 63.52 ± 18.17 | 70.79 ± 14.54 | 74.03 ± 13.91 | 0.003 | 0.17 | 0.05 | 0.004 |
| Extraversion | 84.17 ± 13.32 | 83.77 ± 11.17 | 77.14 ± 16.87 | 71.74 ± 15.46 | <0.001 | 0.31 | 0.36 | 0.10 |
| Openness to experience | 77.07 ± 11.05 | 74.18 ± 8.74 | 70.64 ± 16.80 | 66.58 ± 10.57 | <0.001 | 0.46 | 0.09 | 0.19 |
| Agreeableness | 97.55 ± 10.50 | 94.18 ± 12.08 | 81.64 ± 14.85 | 91.39 ± 14.81 | 0.42 | 0.004 | 0.09 | <0.001 |
| Conscientiousness | 96.89 ± 12.74 | 92.95 ± 18.12 | 86.50 ± 13.88 | 77.11 ± 20.56 | <0.001 | 0.08 | 0.48 | 0.012 |
Abbreviations: Cohabitating = living with someone else; IPIP = International Personality Item Pool; MET = metabolic equivalent; N/A = not available; Packs per day = average number of packs/day smoked; Tobacco 100 = smoked more than 100 cigarettes in his or her lifetime.
The data are presented as n (%) or mean ± SD. We did not specify data from small groups of participants (<3) to protect participant privacy. Normality of distributions was assessed by the Shapiro‒Wilk test. Demographic data were compared between groups using the t test or Wilcoxon rank-sum test for continuous variables and the χ2 test or Fisher exact test for categorical variables. Statistical significance (p < 0.0125) is indicated by bold font for all pairwise comparisons across groups in accordance with Bonferroni correction for multiple comparisons.
Comparison between the high-resilience group who maintained cognitive function despite high pathology and the high-risk susceptible control group who had dementia with high pathology.
Comparison between the high-resilience group who maintained cognitive function despite high pathology and the low-resilience group who had dementia despite low pathology.
Comparison between the high-resilience group who maintained cognitive function despite high pathology and the cognitively unimpaired group with low pathology.
Comparison between the cognitively unimpaired group with low pathology and the low-resilience group who had dementia despite low pathology.
The demographic information from the DIAN study, including race and ethnicity, is self-reported by the participants.
The “other” category for race includes the following ethnicities: Hispanic, Aboriginal Australian, Aboriginal, Croatian, Australian Indigenous, North African, Libyan, Middle Eastern, Arab, Mediterranean, Mexican American, Native Puerto Rican, and Latin American.
Group Comparison for Resilience (Cohort 1)
Compared with susceptible controls (group 4), multivariable predictors of high resilience (group 2) were higher conscientiousness (odds ratio [OR] 1.051 [95% CI 1.016–1.086], p = 0.004) and openness to experience (1.068 [95% CI 1.005–1.135], p = 0.03), controlling for age and depression (Table 2, facet-level result in eTable 7). Compared with low resilience (group 3), the multivariable predictor of high resilience (group 2) was greater agreeableness (1.082 [95% CI 1.015–1.153], p = 0.02), controlling for age and depression (Table 2).
Table 2.
Univariable and Multivariable Logistic Regression Models for Predictors Showing Associations With the Binary Primary Outcome Status (Comparison Set A: The High-Resilience Group vs the High-Risk Susceptible Control Group; Comparison Set B: The High-Resilience Group vs the Low-Resilience Group) in Cohort 1
| Variable | Comparison set A: The high-resilience group vs the susceptible control group | Comparison set B: The high-resilience group vs the low-resilience group | ||||||||||
| Univariable regression | Multivariable regression | Univariable regression | Multivariable regression | |||||||||
| OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Demographic information | ||||||||||||
| Race | ||||||||||||
| White | Reference | Reference | ||||||||||
| Other | 0.429 | 0.126–1.461 | 0.18 | 1.273 | 0.137–11.786 | 0.83 | ||||||
| Sex (female) | 1.727 | 0.767–3.892 | 0.19 | 0.864 | 0.261–2.853 | 0.81 | ||||||
| Visit age, y | 0.922 | 0.874–0.974 | 0.003a | 0.871 | 0.805–0.942 | 0.001 | 0.916 | 0.852–0.984 | 0.016a | 0.877 | 0.796–0.966 | 0.008 |
| Years of education | 1.04 | 0.915–1.182 | 0.55 | 1.228 | 0.988–1.526 | 0.06a | ||||||
| Occupational score | 0.747 | 0.573–0.974 | 0.03a | 0.676 | 0.458–0.996 | 0.048a | ||||||
| Genetics | ||||||||||||
| APOE | ||||||||||||
| 22, 23 | Reference | 0.56 | Reference | 0.22 | ||||||||
| 33 | 1.1 | 0.301–4.019 | 0.89 | 1 | 0.176–5.696 | 1 | ||||||
| 24, 34, 44 | 1.75 | 0.429–7.136 | 0.44 | 3.5 | 0.404–30.342 | 0.26 | ||||||
| Family pathogenic variation | ||||||||||||
| PSEN1 | Reference | 0.02a | Reference | 0.07a | ||||||||
| PSEN2 | Infinity | 1 | Infinity | 1 | ||||||||
| APP | 0.412 | 0.092–1.835 | 0.25 | 0.235 | 0.042–1.313 | 0.1 | ||||||
| Present illness | ||||||||||||
| Traumatic brain injury (present) | 1.164 | 0.262–5.171 | 0.84 | 0.566 | 0.098–3.275 | 0.53 | ||||||
| Hypertension (present) | 0.31 | 0.054–1.782 | 0.19 | 0.224 | 0.029–1.741 | 0.15 | ||||||
| Hypercholesterolemia (present) | 1 | 0.263–3.81 | 1 | 0.235 | 0.06–0.923 | 0.038a | ||||||
| Psychiatric disease (present) | 0.872 | 0.278–2.735 | 0.81 | 0.423 | 0.108–1.657 | 0.22 | ||||||
| Depression (present) | 0.144 | 0.056–0.371 | <0.001a | 0.166 | 0.051–0.535 | 0.003 | 0.118 | 0.034–0.412 | 0.001a | 0.105 | 0.021–0.514 | 0.005 |
| Hachinski ischemic score | ||||||||||||
| 0 | Reference | 0.001a | Reference | 0.010a | ||||||||
| 1 | 0.315 | 0.082–1.214 | 0.09 | 0.727 | 0.073–7.2 | 0.79 | ||||||
| 2–7 | 0.059 | 0.007–0.498 | 0.009 | 0.045 | 0.005–0.45 | 0.008a | ||||||
| Tobacco 100 (present) | 1.494 | 0.668–3.339 | 0.33 | 1.069 | 0.344–3.326 | 0.91 | ||||||
| Packs per day | ||||||||||||
| 1 cigarette–0.5 pack | Reference | 0.45 | Reference | 0.98 | ||||||||
| 0.5–1 pack | 2.727 | 0.724–10.269 | 0.14 | 1.023 | 0.189–5.526 | 0.98 | ||||||
| 1–1.5 pack | 1.818 | 0.272–12.17 | 0.54 | 1.091 | 0.086–13.778 | 0.95 | ||||||
| N/A | 1.255 | 0.451–3.496 | 0.66 | 1.318 | 0.28–6.21 | 0.73 | ||||||
| Alcohol use (present) | 1.121 | 0.252–4.979 | 0.88 | 0.591 | 0.103–3.393 | 0.56 | ||||||
| Substance abuse (present) | 0.898 | 0.264–3.06 | 0.86 | 0.528 | 0.119–2.346 | 0.4 | ||||||
| Social contact | ||||||||||||
| Cohabitating (yes) | 0.583 | 0.225–1.51 | 0.27 | 1.556 | 0.482–5.019 | 0.46 | ||||||
| Living status | ||||||||||||
| Lives alone | Reference | 0.96 | Reference | 0.25 | ||||||||
| Lives with spouse or partner | 1.037 | 0.268–4.018 | 0.96 | 3 | 0.606–14.864 | 0.18 | ||||||
| Lives with relative, friend, group, or others | 0.889 | 0.192–4.114 | 0.88 | 1.2 | 0.212–6.801 | 0.84 | ||||||
| Residency (single family residence)b | 3.105 | 0.272–35.443 | 0.36 | 4.214 | 0.248–71.584 | 0.32 | ||||||
| Marital status (married, living as married)c | 0.925 | 0.388–2.203 | 0.86 | 2.466 | 0.78–7.797 | 0.12 | ||||||
| Physical activity (per 10 METs-min/week increase) | ||||||||||||
| Walking | 1 | 0.996–1.004 | 0.98 | 1.004 | 0.993–1.015 | 0.5 | ||||||
| Jogging | 0.997 | 0.982–1.013 | 0.75 | 1 | 0.976–1.025 | 0.98 | ||||||
| Running | 0.992 | 0.971–1.014 | 0.48 | 1.653 | Infinity | 1 | ||||||
| Biking | 1.003 | 0.994–1.012 | 0.54 | 0.996 | 0.988–1.004 | 0.31 | ||||||
| Tennis | 0.998 | 0.983–1.013 | 0.78 | 0.994 | 0.98–1.007 | 0.37 | ||||||
| Swimming | 0.986 | 0.955–1.018 | 0.39 | 0.977 | 0.944–1.012 | 0.19 | ||||||
| Aerobics | 0.996 | 0.989–1.004 | 0.35 | 1.006 | 0.985–1.027 | 0.58 | ||||||
| Low-intensity exercise | 1.018 | 0.989–1.048 | 0.22 | 1.015 | 0.974–1.058 | 0.48 | ||||||
| Vigorous exercise | 0.998 | 0.995–1.001 | 0.24 | 0.998 | 0.993–1.002 | 0.3 | ||||||
| Weight lifting | 0.983 | 0.955–1.011 | 0.23 | 0.979 | 0.953–1.006 | 0.13 | ||||||
| Total physical activity volume | 0.999 | 0.997–1.001 | 0.41 | 0.999 | 0.997–1.002 | 0.64 | ||||||
| Moderate-intensity exercise (3.0–5.9 METs) | 1.001 | 0.997–1.004 | 0.65 | 1.002 | 0.996–1.008 | 0.58 | ||||||
| High-intensity exercise (≥6.0 METs) | 0.998 | 0.995–1.001 | 0.15 | 0.998 | 0.995–1.001 | 0.27 | ||||||
| IPIP (domain) | ||||||||||||
| Collateral-reported scores | ||||||||||||
| Neuroticism | 0.962 | 0.937–0.989 | 0.005a | 0.976 | 0.943–1.01 | 0.17 | ||||||
| Extraversion | 1.076 | 1.034–1.121 | <0.001a | 1.044 | 0.993–1.096 | 0.09a | ||||||
| Openness to experience | 1.089 | 1.035–1.146 | 0.001a | 1.068 | 1.005–1.135 | 0.03 | 1.031 | 0.976–1.088 | 0.27 | |||
| Agreeableness | 1.016 | 0.985–1.049 | 0.32 | 1.073 | 1.022–1.127 | 0.005a | 1.082 | 1.015–1.153 | 0.02 | |||
| Conscientiousness | 1.042 | 1.018–1.067 | 0.001 a | 1.051 | 1.016–1.086 | 0.004 | 1.02 | 0.988–1.054 | 0.22 | |||
Abbreviations: Cohabitating = living with someone else; IPIP = International Personality Item Pool; MET = metabolic equivalent; N/A = not available; OR = odds ratio; packs per day = average number of packs per day smoked; Tobacco 100 = smoked more than 100 cigarettes in his or her lifetime.
The p values were obtained from univariable and multivariable logistic regression models used to regress the event (asymptomatic, high pathology [high-resilience group], group 2) or control (symptomatic, high pathology, group 4) status (comparison set A), as well as the event (asymptomatic, high pathology [high-resilience group], group 2) or control (symptomatic, low pathology [low-resilience group], group 3) status (comparison set B). The corresponding odds ratios and their 95% CIs are shown. Statistical significance (p < 0.05) is indicated by bold font.
Variables with p < 0.1 in the univariable regression were selected for inclusion in multivariable models by backward stepwise elimination.
The reference category for residency includes others.
The reference category for marital status includes others (widowed, divorced, separated, or never married).
Group Comparison for Resistance (Cohort 1)
Among asymptomatic participants during EYO <0, multivariable predictors (model 1) of high resistance (low pathology, group 1A) were greater volumes of moderate-intensity exercise (1.004 [95% CI 1.001–1.007], p = 0.02), increased years of formal education (1.288 [95% CI 1.110–1.494], p = 0.001), and family pathogenic variation compared with the low-resistance group (high pathology, group 2A), controlling for age and depression (eTable 8). When assessed as individual exercise items, multivariable predictors (model 2) of high resistance were walking (1.004 [95% CI 1.001–1.008], p = 0.02), years of formal education (1.298 [95% CI 1.118–1.508], p = 0.001), and family pathogenic variation, controlling for age and depression (eTable 8). In another comparison for resistance, the multivariable predictor of very high resistance (low pathology, asymptomatic during EYO ≥0, group 1B) was increased moderate-intensity exercise (1.005 [95% CI 1.000–1.010], p = 0.04) compared with the low-resistance group (high pathology during EYO <0, group 2A + 4A), controlling for visit age (eTable 9).
Cohort 2
Selection of Representative Visit Data During the Late Preclinical Period
For the final cohort 2 analysis to identify preclinical lifestyle factors associated with interindividual AAO variability, patient selection considered the time window of exposure measurement and accessibility of outcome status (eFigure 3). We excluded 105 symptomatic carriers with limited preclinical lifestyle data, 176 asymptomatic carriers with unknown AAO outcomes because they had not reached parental AAO, and 9 participants who visited only after EYO >0 (Figure 1). This study design with the binary AAO outcome as the dependent variable allowed us to select representative data from multiple visits per participant. For the remaining 30 participants, the EYO range during which visits were most frequently and uniformly distributed before onset was −3.04 ± 3.21 EYO (Figure 2C) and −2.45 ± 2.18 EYO after excluding 2 outliers. To minimize interindividual variance in EYO time points of the independent variable, we selected 1 representative visit per participant closest to the mean EYO of −2.45. The average of chosen visits was −1.80 ± 1.08 EYO (Figure 2D). Finally, the binary outcome was delayed AAO (positive) or an AAO equal to or earlier than parental AAO (negative) (eTable 10). The positive outcome group with 15 participants consisted of 11 asymptomatic carriers whose last visit age was equal to or greater than the parental AAO and 4 converters whose AAO was later than the parental AAO. The negative outcome group comprised 13 converters.
Multivariable Regression Analysis of Binary AAO Outcome Groups
Among significant variables from univariable models (eTable 11), conscientiousness, education, and MMSE scores were selected through backward elimination and CSFp-tau181 was included for its clinical significance. MMSE scores and education were not included in the same model because of multicollinearity. In the multivariable logistic regression models controlling for CSFp-tau181, the independent predictor of delayed AAO was higher conscientiousness (model 1; 0.916 [95% CI 0.845–0.994], p = 0.04). Conscientiousness was a consistent predictor in other multivariable models, controlling for MMSE scores (model 2; 0.908 [0.835–0.986], p = 0.02), CSFp-tau181 and MMSE scores (model 3; 0.914 [0.836–1.000], p = 0.051), and education (model 4; 0.880 [0.799–0.969], p = 0.009) (Table 3). In the facet-level analysis (eTable 12), the independent predictors of a delayed AAO were greater self-efficacy (0.317 [0.115–0.877], p = 0.03) and self-discipline (0.558 [0.330–0.942], p = 0.03) controlling for CSFp-tau181 (model 1); greater self-efficacy (0.313 [0.112–0.872], p = 0.03), achievement striving (0.585 [0.371–0.923], p = 0.02), and self-discipline (0.523 [0.309–0.886], p = 0.02) controlling for MMSE scores (model 2); greater self-discipline (0.540 [0.306–0.953], p = 0.03) controlling for CSFp-tau181 and MMSE scores (model 3); and greater orderliness (0.552 [0.357–0.855], p = 0.01), dutifulness (0.588 [0.357–0.966], p = 0.04), achievement striving (0.504 [0.289–0.877], p = 0.02), and self-discipline (0.429 [0.220–0.837], p = 0.01) controlling for education (model 4).
Table 3.
Multivariable Logistic Regression Model for Predictors (Domain-Level) Associated With the Binary AAO Outcome in Cohort 2
| Parameter | OR | 95% CI | p Value | |
| Model 1 | ||||
| Pathology | CSF p-tau181 levels | 1.014 | 0.983–1.046 | 0.38 |
| IPIP (collateral-reported) | Conscientiousness | 0.916 | 0.845–0.994 | 0.04 |
| Model 2 | ||||
| Cognition | MMSE scores | 0.376 | 0.139–1.019 | 0.055 |
| IPIP (collateral-reported) | Conscientiousness | 0.908 | 0.835–0.986 | 0.02 |
| Model 3 | ||||
| Cognition | MMSE scores | 0.379 | 0.139–1.029 | 0.057 |
| Pathology | CSF p-tau181 levels | 1.015 | 0.978–1.053 | 0.43 |
| IPIP (collateral-reported) | Conscientiousness | 0.914 | 0.836–1.000 | 0.051 |
| Model 4 | ||||
| Years of education | Years of education | 0.474 | 0.249–0.902 | 0.02 |
| IPIP (collateral-reported) | Conscientiousness | 0.880 | 0.799–0.969 | 0.009 |
Abbreviations: AAO = age at symptom onset; IPIP = International Personality Item Pool; MMSE = Mini-Mental State Examination; OR = odds ratio.
Model 1 was adjusted for CSF p-tau181 levels. Model 2 was adjusted for MMSE scores. Model 3 was adjusted for MMSE scores and CSF p-tau181 levels. Model 4 was adjusted for years of education. The p values were obtained from a multivariable logistic regression model used to regress the event (equal or earlier AAO than parental AAO, negative outcome) or control (delayed AAO, positive outcome) status. Statistical significance (p < 0.05) is indicated by bold font.
3D Visualization of Longitudinal Modifiable Lifestyle Trajectories Over EYO and CSFp-tau181
Three-dimensional visualization of the longitudinal modifiable lifestyle trajectories over EYO and CSFp-tau181 of the entire cohort and high-pathology subsets revealed that asymptomatic carriers exhibited greater overall longitudinal trends in conscientiousness, openness to experience, extraversion, and agreeableness than symptomatic carriers during the expected preclinical period, as grossly estimated from the higher least-squares best-fitting planes in the lifestyle-axis direction (Figure 3, A–H, eFigures 4–6, Video 1 and 2). Significant disparities were observed in longitudinal patterns along the EYO axis between conscientiousness and other personality traits. The persistent divergence in conscientiousness levels between asymptomatic and symptomatic carriers, beginning in the very early preclinical stages and continuing throughout the lifespan, was demonstrated by nonoverlapping best-fitting surface planes between groups during expected preclinical (EYO <0) and postclinical (EYO >0) periods. Conversely, openness to experience, extraversion, and agreeableness exhibited declining trends in asymptomatic carriers and increasing trends in symptomatic carriers, narrowing the initial divergence between groups as the disease progresses, especially in later EYO stages. Asymptomatic carriers exhibited greater overall longitudinal trends in moderate-intensity exercise than symptomatic carriers. Among asymptomatic individuals, those engaging in greater volumes of moderate-intensity exercise tended to have lower CSFp-tau181 levels (Figure 3I).
Figure 3. Three-Dimensional Visualization of Within-Individual Longitudinal Trajectories of Modifiable Life Experiences Over Estimated Years From EYO and CSFp-tau181 Levels of the Entire DIAN Cohort According to the Disease Spectrum (A–D, F, G, and I–K) and the Resilience Status (E and H).
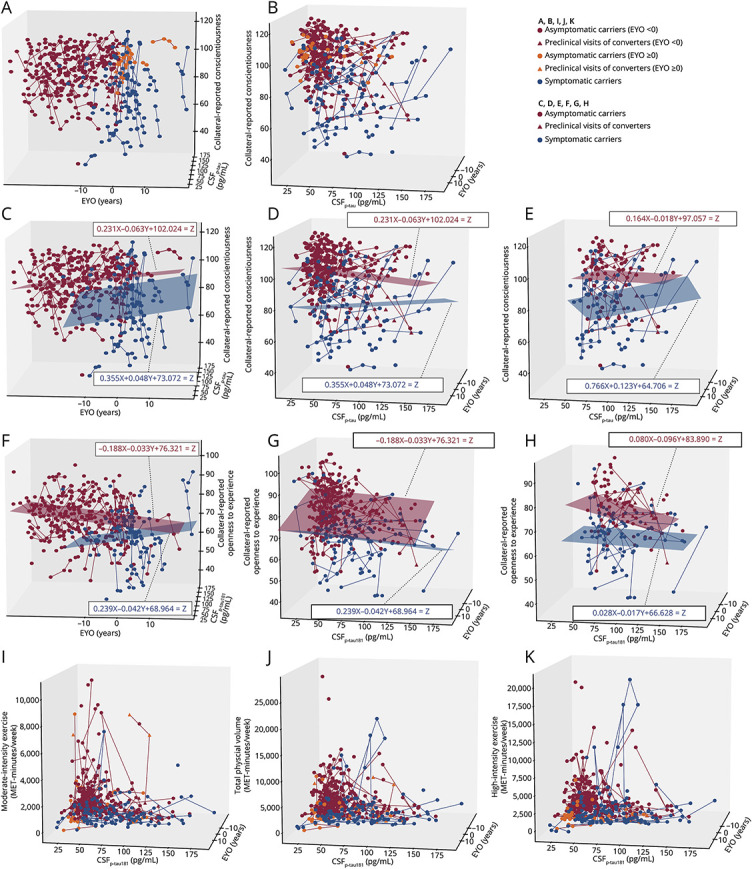
(A–E) Visualization of longitudinal collateral-reported conscientiousness over the estimated years from expected symptom onset (EYO) (A, C) and CSFp-tau181 levels (B, D), with an overlaid least-squares best-fitting plane (C, D) of asymptomatic carriers (red) vs symptomatic carriers (blue). X: EYO, Y: CSFp-tau181 levels, Z: collateral-reported conscientiousness. (E) Visualization of longitudinal collateral-reported conscientiousness over CSFp-tau181 levels and EYO in the high-pathology subset (CSFp-tau181 level ≥51.52 pg/mL) according to the resilience status. (F–H) Three-dimensional (3D) visualization of within-individual longitudinal trajectories of collateral-reported openness to experience over EYO (F) and CSFp-tau181 levels (G), with an overlaid least-squares best-fitting plane, according to the disease spectrum and the resilience status (H). In the entire cohort and the subset of participants with high pathology, asymptomatic carriers showed greater overall longitudinal trends of collateral-reported conscientiousness and openness to experience than symptomatic carriers, during the expected preclinical period, as grossly estimated from a higher least-squares best-fitting plane in the conscientiousness or openness to lifestyle-axis direction. (I–K) Three-dimensional (3D) visualization of within-individual longitudinal trajectories of physical activity over CSFp-tau181 levels and EYO of the entire DIAN cohort according to the disease spectrum. (I) Moderate-intensity (MET 3.0–5.9) exercise volume. (J) Total physical activity volume. (K) High-intensity (MET ≥6.0) exercise volume. For moderate-intensity exercise, asymptomatic carriers showed greater overall longitudinal trends in exercise volume than symptomatic carriers, and among asymptomatic carriers, participants with greater moderate-intensity exercise volume trended toward a lower degree of CSFp-tau181 pathology. By contrast, for high-intensity exercise, because some symptomatic carriers had a high volume of high-intensity exercise that was comparable to or even greater than in asymptomatic carriers, there was no significant difference in exercise volume between asymptomatic and symptomatic carriers, as observed for moderate-intensity exercise. Model fitting was performed using the “Best-fit Surfaces for 3-Dimensional Data” code generating least-squared best-fit planes for 3-dimensional data using linear regression techniques (1st-order polynomials), provided by Patrick J. Wright from Inversion Labs (LLC, Wilson, WY; inversionlabs.com/2016/03/21/best-fit-surfaces-for-3-dimensional-data.html). In the 3D plane where the X-axis is the EYO, the Y-axis is the CSF p-tau level, and the Z-axis is the lifestyle data, the mesh grid surface (X_mg, Y_mg) with a 20*20 matrix size was extracted: . Model fitting to estimate the constants (a, b, c) satisfying the least-squares solution for f(x,y) = Z was performed using the scipy.linalg.lstsq function in Python 3.9.12 and consequently produced surface plots with the estimated X_mg, Y_mg, and Z_linear: .
3D longitudinal conscientiousness over CSFp-tau181 and EYO.Download Supplementary Video 1 (9.3MB, mov) via http://dx.doi.org/10.1212/209766_Video_1
3D longitudinal openness to experience over CSFp-tau181 and EYO.Download Supplementary Video 1 (9.2MB, mov) via http://dx.doi.org/10.1212/209766_Video_2
Discussion
This DIAN observational cohort study demonstrated an association between resilience-related modifiable life experiences and interindividual variability in AAO in ADAD. After −20 EYO time point with significant interindividual variability in CSFp-tau181 levels, resilient individuals who remained with cognitive function despite high pathology were associated with greater engagement in life experiences marked by higher scores in conscientiousness, openness to experience, and agreeableness than controls with dementia. Selected data during the late preclinical period (1–3 years before parental AAO) further confirmed that, among cognitively active and socially integrated life experiences associated with resilience, conscientiousness was an independent predictor of delayed AAO, augmenting resilience while controlling for CSFp-tau181.
As the first attempt to define resiliency in ADAD, our 2-pronged conceptual framework extends Stern's classic resilience definition for coping with pathology3 to an ADAD-specific setting characterizing onset predictability based on parental AAO. In cohort 1, resilience was determined relative to pathology and the genetically determined EYO time frame: the mismatch between pathologic and symptomatic statuses describes resilience while the mismatch between EYO and pathologic statuses describes resistance. Despite the expected challenges in detecting nongenetic impacts in ADAD, cohort 2 results confirmed that modifiable lifestyle factors, linked to the established resilience definition, were also associated with ADAD-inherent resilient AAO outcomes. Among the various methodologies to optimally defining resilience, the residual approach, which provides individual-specific, continuous measures of resilience, is widely implemented.23,24 Our classification-bin approach23 in cohort 1 offers the advantage of applying more direct and fixed judgment criteria with a biological basis (symptomatic, pathologic, and EYO status), addressing the challenges associated with the residual approach, where the accuracy of the prediction model for expected population norms is affected by data-driven regression algorithms and necessitates comprehensive validation of the residual construct.24 Considering the longitudinal rate change in CSFp-tau181 peaks in the late preclinical stage (several years before onset)25 and aligning with our representative data time frame, we chose CSFp-tau181 as a pathologic measure because tau exhibits a closer association with temporal changes in neurodegeneration and cognitive symptoms than amyloid. In the multivariable regression, resilient individuals who evaded cognitive decline despite accumulating pathology were associated with cognitively and socially integrated life experiences—assiduity and responsibilities (conscientiousness), experiential and artistic appreciation (openness to experience), and social support and altruistic cooperation (agreeableness). Controlling for relevant factors possibly influencing participants' lifestyles is a critical issue; all multivariable analyses adjusted for age and depression as covariates, which might reduce participants' inclination for social interactions or leisure activities. We also minimized the time gap of the representative data between the resilient and control groups by selecting the last preclinical visits of asymptomatic carriers and the first visits of symptomatic carriers, which was an early MCI stage that retained ADL integrity (1.50 ± 1.02 years from first CDR conversion to 0.5). Despite the lack of temporal causality, consistent associations between protective lifestyles and resilience, which have not previously been evaluated in a large-sample well-controlled study, improve our understanding of the nongenetic contributors to resilience in ADAD because the selected indicators—conscientiousness, openness to experience, and agreeableness—reflect collaterals' cumulative observations of participants' lifestyle phenotypes and are thus considered modifiable because individuals can voluntarily choose to engage in these experiences.
Exercise was not associated with AAO, supporting previous studies highlighting the protective effect of effortful mental activities rather than mere physical activities, against dementia.6 Instead, moderate-intensity exercise (walking) was associated with resistance, consistent with a report that moderate, not vigorous, exercise was related to a lower CSFp-tau/Aβ42 ratio.26 Although questions remain surrounding the biological plausibility of differences in the effects of cognitive vs metabolic lifestyles on brain, moderate-intensity exercise possibly improves cerebral perfusion, facilitating pathology clearance.27 Nevertheless, the lack of an association between exercise and resilience is dubious. The PAGAC assigned the strongest evidence grades for the cognitive benefits of exercise in children and seniors older than 60, but not in young and middle-aged adults (18–50 years).28 Considering the moderating effect of age on the cognitive response to exercise and scant evidence in younger and middle-aged populations,28 we investigated the associations between exercise and AAO in early-onset Alzheimer disease (EOAD), which begins 30–40 years earlier than late-onset Alzheimer disease (LOAD). In Class II RCT evidence, exercise-induced improvements in executive function increase as individuals age (β = 0.018 SD per year).29 Because biomolecules mediating exercise-induced cognitive improvement are dysregulated with aging, LOAD with greater variability in neurodegeneration and functional capacities accumulated over the lifespan may exhibit a greater cognitive response gap between high and low exercisers than EOAD having sufficient reserves regardless of exercise level due to younger age.30
Among mental, physical, and social experiences, which is the most relevant component associated with interindividual AAO variability, the ADAD-specific resilient outcome? In cohort 2, representative data were selected within a narrow time frame (−1.80 ± 1.08 EYO) during the late preclinical period without dementia for both outcome groups, ensuring an appropriate temporal relationship between cause and outcome and minimizing interindividual variance in the lifestyle data time frame. Conscientiousness, an individual's behavioral system of steadily working hard in an organized manner and carefully considering responsibility to others,31 contributes to delaying AAO by augmenting resilience rather than resistance adjusting for cognition or education, a conclusion replicated in several studies,32-34 despite differences in pathologic measures and resilience definitions. Although the Baltimore study35 reported contrasting evidence linking conscientiousness and resistance, this study evaluated only baseline associations between conscientiousness and PET-based pathology, assessed within 1 year, and did not examine the predictive effect on AD conversion. In a clinicopathologic study of 224 autopsies,34 higher baseline conscientiousness, recorded up to 30 years before death (thus eliminating reverse causality), was associated with asymptomatic status with significant neuropathology at death and this association persisted controlling for pathology. Extending previous analyses from the early preclinical period,34 we present the novel perspective that resilience supplied by psychosocial factors remains effective during late preclinical ADAD.
Education has been consistently linked to decreased dementia risk, but not all studies have attributed this association to resilience. Our association between education and resistance against pathologic tau was mirrored in a cross-sectional study reporting that education promoted resistance against Aβ in PREVENT-AD and DIAN.36 This conclusion was replicated in the Framingham Study,37 which reported that lower educational attainment increased the risk of vascular dementia but not AD, suggesting this effect occurs through vascular pathology rather than brain vulnerability to pathology. Regarding the differential influence of separate components of intellectual enrichment (earlier life vs lifelong cognitive engagement), only mid/late-life cognitive engagement, not formal education, was associated with longitudinal changes in cognitive decline.5 Only conscientiousness, not education or neuropsychiatric scores, differed between converters and nonconverters, and none of the AD pathologic biomarkers mediated this association.32 The effects of schooling may wane when cognitive decline begins, whereas conscientiousness, the higher order habitual intelligence consolidated throughout one's lifetime maintaining brain activity and purposefulness, is a useful indicator for evaluating resilience and predicting dementia onset beyond a single test score for a specific cognitive domain or formal education.
Personality changes are recognized in dementia diagnostic criteria,38 yet current clinical assessments primarily emphasize recent personality alterations. The accumulation of pathology long before cognitive decline may influence personality changes, creating uncertainty about whether specific personalities reflect underlying pathology or represent true risk factors of future dementia onset.39 For the first visualization of longitudinal lifestyle changes in ADAD, persistent divergence in conscientiousness between asymptomatic and symptomatic carriers from early preclinical stages and throughout lifespan decreases the likelihood that symptomatic individuals will ever reach the conscientiousness levels of their asymptomatic counterparts at any stage of life. This pattern aligns with statistical results (Table 4) using representative preclinical data, reinforcing the significance of conscientiousness as a life-course protective factor even in genetically predisposed individuals with ADAD. In the Baltimore Longitudinal Study of Aging, which followed 2046 participants for up to 36 years, nonconverters consistently exhibited higher intercept levels of conscientiousness and extraversion, with no difference in the slope of the trajectories, compared with AD converters, demonstrating high rank-order stability throughout the entire preclinical period, including the years immediately preceding disease onset.39 Elevated levels of reliability and responsibility early in life are associated with greater opportunities for higher educational and occupational achievement, enhancing cognitive resilience and reinforcing high levels of conscientiousness that persist into later life stages. Conversely, openness to experience and extraversion tended to increase in symptomatic carriers as the disease progresses, possibly reflecting lifestyle adjustments driven by increased compensatory self-awareness from preventive education during the trial's enrollment.
Table 4.
Life Experience Factors Contributing to Resilience and Resistance in Dominantly Inherited Alzheimer Disease
| Concepts | Resilience | Resistance |
| Definition | Maintaining cognitive function better than expected in the presence of high pathology | Lower-than-expected pathology |
| Contributing life experience factors | Conscientiousnessa,d | Moderate-intensity exercisec |
| Openness to experiencea | Years of formal educationc | |
| Agreeablenessb |
Compared with the susceptible control group (symptomatic, high pathology), the lifestyle contributors for the high-resilience group (asymptomatic, high pathology) were higher level of conscientiousness and openness to experience, controlling for age and depression.
Compared with the low-resilience group (symptomatic, low pathology), the lifestyle contributor for the high-resilience group (asymptomatic, high pathology) was higher level of agreeableness, controlling for age and depression.
Compared with the low-resistance group (high pathology, asymptomatic, estimated years from expected symptom onset [EYO] <0), the lifestyle contributors for high resistance (low pathology, asymptomatic, EYO <0) included more frequent moderate-intensity exercise, more years of formal education, and family pathogenic variation, controlling for age and depression.
a-cAge and depression were also significant multivariable factors. Although all multivariable comparisons were adjusted for age and depression as covariates, they were not included in this table because they do not fall within the scope of modifiable lifestyle factors conceptually.
In the results of cohort 2, conscientiousness was the consistent lifestyle contributor for delaying the onset age compared with that of parents, even after adjusting for CSFp-tau181 levels (model 1), Mini-Mental State Examination (MMSE) scores (model 2), both CSFp-tau181 levels and MMSE scores (model 3), and years of education (model 4).
Conscientiousness, a positive psychological trait that serves as a proxy for life experience, is conceptually encompassed by resilience-enhancing modifiable psychosocial factors,40 given its modifiable nature in that an individual will voluntarily choose and continue such experiences. Contemporary psychological evidence is robust enough to suggest both continuity and changeability in personality, in which biological and environmental influences synergistically interact.41-47 Longitudinal studies on rank-order consistency and slow maturation over a lifespan imply a moderate plasticity of conscientiousness, establishing it as a stable predictor of meaningful life outcomes and actionable targets for purposeful intervention.41-47 In a 1,523-participant RCT,48 a 3-month digital intervention was effective for the intended change in conscientiousness, a finding corroborated in a meta-analysis of over 200 interventional studies.49 The preventive implications and policy relevance of increasing conscientiousness on delaying dementia onset and identifying the optimal time frames for its maximum protective effect on AAO merit verification in future well-controlled RCTs using a life-course approach.
As a limitation, the small sample size in cohort 2 reflects our strict selection criteria. Unlike cohort 1, where outcomes were defined based on the extent of pathology, cohort 2 adjusted for pathology in the multivariable regression but a subgroup analysis was not conducted to examine how lifestyle factors influencing AAO outcomes differ between those with high and low pathologies. Future studies with longer follow-up allowing for the inclusion of the currently excluded 176 asymptomatic participants with unknown AAO outcomes (not reached their parental AAO) could address this issue. In addition, in cohort 1, comparisons may be underpowered when the high-resilience group is compared with 2 different control groups of varying sample size, particularly if the low-resilience group has a relatively small sample size. Furthermore, the lack of racial and ethnic diversity in our predominantly White population limits the generalizability of our results.
Measures of conscientiousness are useful indicators for evaluating resilience and predicting the prognosis for future dementia onset during the late-stage, preclinical period (−1.80 ± 1.08 EYO) with progressive pathology in individuals with ADAD with a clear genetic etiology. Because small delays in AAO have large effects on the general public, our ADAD findings should be evaluated in more diverse populations across a broad spectrum of age groups and socioeconomic/cultural backgrounds in the global context to determine how resilience-promoting life experiences influence the prognosis of biomarker-positive, at-risk individuals from the general population. If individuals with subjective memory impairment or mild cognitive impairment show positive AD biomarkers (amyloid or tau PET), future research can address the clinical question of whether the conscientiousness indicator assessed during this stage may inform individuals' prognosis, including when they will develop symptomatic AD.
Acknowledgment
This article has been reviewed by DIAN Study investigators for scientific content and consistency of data interpretation with previous DIAN study publications. The authors thank the participants and their families and acknowledge the DIAN research and support staff at each of the participating sites for their contributions to this study. The authors additionally thank all the participating researchers in the Dominantly Inherited Alzheimer Network. Especially, the authors express their profound appreciation to Anne M. Fagan, the former DIAN Fluid Biomarker Core Leader, for her devoted efforts in reviewing and offering constructive feedback on our article. The Department of Clinical Epidemiology and Biostatistics of Asan Medical Center was responsible for consultation about statistical approaches.
Glossary
- AAO
age at symptom onset
- ADAD
autosomal dominant Alzheimer disease
- CDR
Clinical Dementia Rating
- DIAN
Dominantly Inherited Alzheimer Network
- EOAD
early-onset Alzheimer disease
- EYO
estimated years from expected symptom onset
- IPIP
International Personality Item Pool
- LOAD
late-onset Alzheimer disease
- MET
metabolic equivalent
- MMSE
Mini-Mental State Examination
- OR
odds ratio
- p-tau181
tau phosphorylated at threonine-181
- RCT
randomized controlled trial
Appendix 1. Authors
| Name | Location | Contribution |
| Hye Joo Son, MD, PhD | Department of Nuclear Medicine, Dankook University College of Medicine, Cheonan, Chung Nam, South Korea | Drafting/revision of the manuscript for content, including medical writing for content; major role in the acquisition of data; study concept or design; analysis or interpretation of data |
| Jae Seung Kim, MD, PhD | Department of Nuclear Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea | Major role in the acquisition of data; project administration; supervision; study concept or design; analysis or interpretation of data |
| Randall J. Bateman, MD | Department of Neurology, Washington University School of Medicine, St. Louis, MO | Major role in the acquisition of data |
| Seonok Kim, MS | Department of Clinical Epidemiology and Biostatistics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea | Analysis or interpretation of data |
| Jorge J. Llibre-Guerra, MD, MSc | Department of Neurology, Washington University School of Medicine, St. Louis, MO | Major role in the acquisition of data; analysis or interpretation of data |
| Gregory S. Day, MD, MSc, MSCI | Department of Neurology, Mayo Clinic College of Medicine and Science, Jacksonville | Major role in the acquisition of data; analysis or interpretation of data |
| Jasmeer P. Chhatwal, MD, PhD | Department of Neurology, Massachusetts General Hospital, Harvard Medical School, Boston | Major role in the acquisition of data |
| Sarah B. Berman, MD, PhD | Department of Neurology, University of Pittsburgh School of Medicine, PA | Major role in the acquisition of data; analysis or interpretation of data |
| Peter R. Schofield, PhD, DSc | Neuroscience Research Australia; School of Medical Sciences, University of New South Wales, Sydney, Australia | Major role in the acquisition of data |
| Mathias Jucker, PhD | Department of Cellular Neurology, Hertie Institute for Clinical Brain Research, University of Tübingen; German Center for Neurodegenerative Diseases, Tübingen, Germany | Major role in the acquisition of data |
| Johannes Levin, MD, PhD | Department of Neurology, Ludwig-Maximilians-Universität München; German Center for Neurodegenerative Diseases; Munich Cluster for Systems Neurology (SyNergy), Germany | Major role in the acquisition of data |
| Jae-Hong Lee, MD, PhD | Department of Neurology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, South Korea | Major role in the acquisition of data |
| Richard J. Perrin, MD, PhD | Department of Pathology and Immunology, Knight Alzheimer's Disease Research Center, and Department of Neurology, Washington University in St. Louis, MO | Major role in the acquisition of data |
| John C. Morris, MD | Department of Neurology, Washington University School of Medicine, St. Louis, MO | Major role in the acquisition of data |
| Carlos Cruchaga, PhD | Department of Psychiatry, Washington University School of Medicine, St. Louis, MO | Major role in the acquisition of data |
| Jason Hassenstab, PhD | Knight Alzheimer's Disease Research Center, Department of Neurology, and Department of Psychological and Brain Sciences, Washington University, St. Louis, MO | Major role in the acquisition of data |
| Stephen P. Salloway, MD | Department of Neurology, The Warren Alpert Medical School of Brown University, Butler Hospital, Providence, RI | Major role in the acquisition of data |
| Jai-Hyuen Lee, MD, PhD | Department of Nuclear Medicine, Dankook University College of Medicine, Cheonan, Chung Nam, South Korea | Analysis or interpretation of data |
| Alisha Daniels, MD, MHA | Department of Neurology, Washington University School of Medicine, St. Louis, MO | Major role in the acquisition of data |
Appendix 2. Coinvestigators
| Coinvestigators are listed at Neurology.org. |
Study Funding
Data collection and sharing for this project were supported by the Dominantly Inherited Alzheimer Network (DIAN, U19AG032438 [R.J.B.]) funded by the National Institute on Aging (NIA), the Alzheimer's Association (SG-20-690363-DIAN), the German Center for Neurodegenerative Diseases (DZNE), and the Raul Carrea Institute for Neurological Research (FLENI). This research was partially supported by the Research and Development Grants for Dementia from the Japan Agency for Medical Research and Development, AMED, and the Korea Dementia Research Project through the Korea Dementia Research Center (KDRC), funded by the Ministry of Health & Welfare and Ministry of Science & ICT, South Korea (grant number RS-2024-00344521 [J.-H.L.]), Spanish Institute of Health Carlos III (ISCIII), Canadian Institutes of Health Research (CIHR), Canadian Consortium of Neurodegeneration and Aging, Brain Canada Foundation, and Fonds de Recherche du Québec—Santé. This study was also financially supported by the National Research Foundation of Korea (NRF) grant funded by the Ministry of Science and ICT (MIST), South Korea (grant number, 2021R1F1A1063874 [H.J.S.], 2021R1A2C3009056 [J.S.K.]), and by a grant of the Korea Dementia Research Project through the Korea Dementia Research Center (KDRC), funded by the Ministry of Health & Welfare and Ministry of Science & ICT, Republic of Korea (grant number HU22C0031 [J.S.K.]).
Disclosure
H.J. Son and J.S. Kim report no disclosures relevant to the manuscript. R.J. Bateman has received research funding from the National Institute on Aging (NIA; UFAG032438 [DIAN - grant], R01AG068319 [DIAN-TU Next Generation Tau Trial - grant], UFAG032438 [DIAN - grant], RF1AG061900 [Blood Ab- grant], R56AG061900 [Blood Ab- grant], R21AG067559 [NfL - grant], and R01AG53627/R56AG53627 [DIAN-TU Next Generation Prevention Trial - Research Grant]), the Alzheimer's Association (DIAN-TU-OLE-21-725093 [DIAN-TU Open Label Extension - grant], DIAN-TU-Tau-21-822987 [DIAN-TU Tau Next Generation - grant], Biogen [Tau SILK Consortium member, NfL Consortium member], AbbVie [Tau SILK Consortium member, NfL Consortium member], Bristol Meyer Squibbs [NfL Consortium member], Novartis [Tau SILK Consortium member], NINDS/NIA R01NS095773 [CNS Tau - grant], Investigator Initiated Research Grants for Centene Corporation, Rainwater Foundation, Assn for Frontotemporal Degeneration FTD Biomarkers Initiative, Biogen, BrightFocus Foundation, Cure Alzheimer's Fund, Coins for Alzheimer's Research Trust Fund, Eisai, The Foundation for Barnes-Jewish Hospital, TargetALS, Good Ventures Foundation, DIAN-TU Pharma Consortium [active: Eli Lilly and Company/Avid Radiopharmaceuticals, Hoffman-La Roche/Genentech, Biogen, Eisai, Janssen; previous: Abbvie, Amgen, AstraZeneca, Forum, Mithridion, Novartis, Pfizer, United Neuroscience, Sanofi], Eli Lilly and Company [Tau SILK Consortium Member], Hoffman-La Roche [receipt of drugs and services, NfL Consortium Member], CogState [in-kind support] and Signant [in-kind support]), outside of the submitted work. He has received royalties from C2N Diagnostics, lecture fees from Korean Dementia Association, American Neurological Association, Fondazione Prada, and Weill Cornell Medical College, supports for meeting or travel from Hoffman-La Roche, Alzheimer's Association Roundtable, Duke Margolis Alzheimer's Roundtable, BrightFocus Foundation, Tau Consortium Investigator's Meeting, Fondazione Prada and NAPA Advisory Council on Alzheimer's Research and drugs and services from Eisai (DIAN-TU Next Generation Trial), Janssen (DIAN-TU Next Generation Trial) and Hoffman-La Roche (DIAN-TU Open Label Extension - Gantenerumab), outside of the submitted work. He has served as a Data Safety Monitoring Board for Hoffman-La Roche/Genentech, Biogen - Combination therapy for Alzheimer's disease, UK Dementia Research Institute at University College London, Stanford University, and Next Generation Translational Proteomics for Alzheimer's and Related Dementias and the scientific advisory board for C2N Diagnostics, outside of the submitted work. He has patents (Washington University w/RJB as coinventor) titled “Methods for Measuring the Metabolism of CNS Derived Biomolecules In Vivo” (US nonprovisional patent application 12/267,974), “Methods for Measuring the Metabolism of neurally Derived Biomolecules in vivo” (US nonprovisional patent application 13/005,233), “Plasma based methods for detecting CNS Amyloid Disposition” (US nonprovisional patent application 62/492,718), “Plasma based methods for determining A-Beta Amyloidosis” (US nonprovisional patent application 16/610,428), “Methods of Treating Based on site-specific tau phosphorylation” (US nonprovisional patent application 17/015,985) and “Tau Kinetic Measurements” (US nonprovisional patent application 15/515,909), outside of the submitted work. S. Kim, J.J. Llibre-Guerra, G.S. Day, J. Chhatwal, and S.B. Berman report no disclosures relevant to the manuscript. P.R. Schofield has received research funding from the NIH, Anonymous Foundation, Roth Charitable Foundation, NHMRC (Australia), MRFF (Australia) and NSW Health, outside of the submitted work. He has served as chief executive officer for Neuroscience Research Australia, company director for Neuroscience Research Australia Foundation, The Health-Science Alliance, Australian Association of Medical Research Institutes, the Australian Dementia Network (ADNeT) Ltd, and StandingTall Pty Ltd, company director/chief executive officer for Schizophrenia Research Institute, president for Australasian Neuroscience Society, member/steering committee for Maridulu Budyari Gumal - Sydney Partnership for Health Education, Research and Enterprise (SPHERE), chair/national medical advisory panel for The Judith Jane Mason & Harold Stannett Williams Memorial Foundation and ambassador for Business Events Sydney, outside of the submitted work. M. Jucker reports no disclosures relevant to the manuscript. J. Levin has received research funding from the German Center for Neurodegenerative Diseases (DZNE) and consulting fees from Axon Neuroscience and Biogen, lecture fees from Biogen, Bayer Vital, and Roche, author fees from Thieme medical publishers and W. Kohlhammer GmbH medical publishers, and support for attending meetings from AbbVie and Biogen, outside of the submitted work. He has a pending patent, titled “Pharmaceutical Composition and Methods of Use (EP 22 159 408.8),” filed by MODAG GmbH, and has served as a Data Safety Monitoring Board for Axon Neuroscience and as a part-time CMO for MODAG GmbH, outside of the submitted work. J.H. Lee reports no disclosures relevant to the manuscript. R.J. Perrin and J.C. Morris have received research funding from the NIH (U19 AG032438). J.C. Morris has received research funding from the NIH (P30 AG066444, P01AG003991, P01AG026276), consulting fees from Barcelona Brain Research Center (BBRC) and Native Alzheimer Disease-Related Resource Center in Minority Aging Research (Ext Adv Board) and lecture fees from Montefiore Grand Rounds (NY) and Tetra-Inst ADRC seminar series (Grand Rds, NY), outside of the submitted work. He has served as a Data Safety Monitoring Board for Cure Alzheimer's Fund (the Research Strategy Council), Diverse VCID Observational Study Monitoring Board, and LEADS Advisory Board (Indiana University), outside of the submitted work. C. Cruchaga, J. Hassenstab, S.P. Salloway, J.H. Lee, and A. Daniels report no disclosures relevant to the manuscript. Go to Neurology.org/N for full disclosures.
References
- 1.Ryman DC, Acosta-Baena N, Aisen PS, et al. Symptom onset in autosomal dominant Alzheimer disease: a systematic review and meta-analysis. Neurology. 2014;83(3):253-260. doi: 10.1212/WNL.0000000000000596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gómez-Tortosa E, Barquero MS, Barón M, et al. Variability of age at onset in siblings with familial Alzheimer disease. Arch Neurol. 2007;64(12):1743-1748. doi: 10.1001/archneur.64.12.1743 [DOI] [PubMed] [Google Scholar]
- 3.Stern Y. Cognitive reserve in ageing and Alzheimer's disease. Lancet Neurol. 2012;11(11):1006-1012. doi: 10.1016/s1474-4422(12)70191-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Arenaza-Urquijo EM, Vemuri P. Resistance vs resilience to Alzheimer disease: clarifying terminology for preclinical studies. Neurology. 2018;90(15):695-703. doi: 10.1212/wnl.0000000000005303 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vemuri P, Lesnick TG, Przybelski SA, et al. Association of lifetime intellectual enrichment with cognitive decline in the older population. JAMA Neurol. 2014;71(8):1017-1024. doi: 10.1001/jamaneurol.2014.963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Verghese J, Lipton RB, Katz MJ, et al. Leisure activities and the risk of dementia in the elderly. N Engl J Med. 2003;348(25):2508-2516. doi: 10.1056/NEJMoa022252 [DOI] [PubMed] [Google Scholar]
- 7.Sommerlad A, Sabia S, Livingston G, Kivimäki M, Lewis G, Singh-Manoux A. Leisure activity participation and risk of dementia: an 18-year follow-up of the Whitehall II study. Neurology. 2020;95(20):e2803-e2815. doi: 10.1212/wnl.0000000000010966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rovio S, Kåreholt I, Helkala EL, et al. Leisure-time physical activity at midlife and the risk of dementia and Alzheimer's disease. Lancet Neurol. 2005;4(11):705-711. doi: 10.1016/s1474-4422(05)70198-8 [DOI] [PubMed] [Google Scholar]
- 9.Blondell SJ, Hammersley-Mather R, Veerman JL. Does physical activity prevent cognitive decline and dementia? A systematic review and meta-analysis of longitudinal studies. BMC Public Health. 2014;14:510. doi: 10.1186/1471-2458-14-510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fratiglioni L, Wang HX, Ericsson K, Maytan M, Winblad B. Influence of social network on occurrence of dementia: a community-based longitudinal study. Lancet. 2000;355(9212):1315-1319. doi: 10.1016/s0140-6736(00)02113-9 [DOI] [PubMed] [Google Scholar]
- 11.Wang HX, Karp A, Herlitz A, et al. Personality and lifestyle in relation to dementia incidence. Neurology. 2009;72(3):253-259. doi: 10.1212/01.wnl.0000339485.39246.87 [DOI] [PubMed] [Google Scholar]
- 12.Beck ED, Yoneda T, James BD, et al. Personality predictors of dementia diagnosis and neuropathological burden: an individual participant data meta-analysis. Alzheimers Dement. 2024;20(3):1497-1514. doi: 10.1002/alz.13523 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255-2263. doi: 10.1016/s0140-6736(15)60461-5 [DOI] [PubMed] [Google Scholar]
- 14.Andrieu S, Guyonnet S, Coley N, et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017;16(5):377-389. doi: 10.1016/s1474-4422(17)30040-6 [DOI] [PubMed] [Google Scholar]
- 15.Moll van Charante EP, Richard E, Eurelings LS, et al. Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): a cluster-randomised controlled trial. Lancet. 2016;388(10046):797-805. doi: 10.1016/s0140-6736(16)30950-3 [DOI] [PubMed] [Google Scholar]
- 16.Lourida I, Hannon E, Littlejohns TJ, et al. Association of lifestyle and genetic risk with incidence of dementia. JAMA. 2019;322(5):430-437. doi: 10.1001/jama.2019.9879 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bateman RJ, Xiong C, Benzinger TL, et al. Clinical and biomarker changes in dominantly inherited Alzheimer's disease. N Engl J Med. 2012;367(9):795-804. doi: 10.1056/NEJMoa1202753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Morris JC, Aisen PS, Bateman RJ, et al. Developing an international network for Alzheimer research: the dominantly inherited Alzheimer network. Clin Investig (Lond). 2012;2(10):975-984. doi: 10.4155/cli.12.93 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.World Health Organization. WHO guidelines approved by the guidelines review committee. In: World Health Organization, ed. Global Recommendations on Physical Activity for Health. WHO Press; 2010:1-60. [Google Scholar]
- 20.Garber CE, Blissmer B, Deschenes MR, et al. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334-1359. doi: 10.1249/MSS.0b013e318213fefb [DOI] [PubMed] [Google Scholar]
- 21.Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(8):1575-1581. doi: 10.1249/MSS.0b013e31821ece12 [DOI] [PubMed] [Google Scholar]
- 22.Johnson JA. Measuring thirty facets of the five factor model with a 120-item public domain inventory: development of the IPIP-NEO-120. J Res Pers. 2014;51:78-89. doi: 10.1016/j.jrp.2014.05.003 [DOI] [Google Scholar]
- 23.Neuner SM, Telpoukhovskaia M, Menon V, O'Connell KMS, Hohman TJ, Kaczorowski CC. Translational approaches to understanding resilience to Alzheimer's disease. Trends Neurosci. 2022;45(5):369-383. doi: 10.1016/j.tins.2022.02.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bocancea DI, Van Loenhoud AC, Groot C, Barkhof F, Van Der Flier WM, Ossenkoppele R. Measuring resilience and resistance in aging and Alzheimer disease using residual methods: a systematic review and meta-analysis. Neurology. 2021;97(10):474-488. doi: 10.1212/wnl.0000000000012499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Barthélemy NR, Li Y, Joseph-Mathurin N, et al. A soluble phosphorylated tau signature links tau, amyloid and the evolution of stages of dominantly inherited Alzheimer's disease. Nat Med. 2020;26(3):398-407. doi: 10.1038/s41591-020-0781-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Law LL, Rol RN, Schultz SA, et al. Moderate intensity physical activity associates with CSF biomarkers in a cohort at risk for Alzheimer's disease. Alzheimers Dement (Amst). 2018;10:188-195. doi: 10.1016/j.dadm.2018.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Trigiani LJ, Hamel E. An endothelial link between the benefits of physical exercise in dementia. J Cereb Blood Flow Metab. 2017;37(8):2649-2664. doi: 10.1177/0271678x17714655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Erickson KI, Hillman C, Stillman CM, et al. Physical activity, cognition, and brain outcomes: a review of the 2018 physical activity guidelines. Med Sci Sports Exerc. 2019;51(6):1242-1251. doi: 10.1249/mss.0000000000001936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Stern Y, MacKay-Brandt A, Lee S, et al. Effect of aerobic exercise on cognition in younger adults: a randomized clinical trial. Neurology. 2019;92(9):e905-e916. doi: 10.1212/wnl.0000000000007003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stillman CM, Esteban-Cornejo I, Brown B, Bender CM, Erickson KI. Effects of exercise on brain and cognition across age groups and health states. Trends Neurosci. 2020;43(7):533-543. doi: 10.1016/j.tins.2020.04.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Roberts BW, Jackson JJ, Fayard JV, Edmonds G, Meints J. Conscientiousness. In: Leary MR, Hoyle RH, eds. Handbook of Individual Differences in Social Behavior. The Guilford Press; 2009:369-381. [Google Scholar]
- 32.Duchek JM, Aschenbrenner AJ, Fagan AM, Benzinger TLS, Morris JC, Balota DA. The relation between personality and biomarkers in sensitivity and conversion to Alzheimer-type dementia. J Int Neuropsychol Soc. 2020;26(6):596-606. doi: 10.1017/s1355617719001358 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Graham EK, James BD, Jackson KL, et al. Associations between personality traits and cognitive resilience in older adults. J Gerontol B Psychol Sci Soc Sci. 2021;76(1):6-19. doi: 10.1093/geronb/gbaa135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Terracciano A, Iacono D, O'Brien RJ, et al. Personality and resilience to Alzheimer's disease neuropathology: a prospective autopsy study. Neurobiol Aging. 2013;34(4):1045-1050. doi: 10.1016/j.neurobiolaging.2012.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Terracciano A, Bilgel M, Aschwanden D, et al. Personality associations with Amyloid and Tau: results from the Baltimore longitudinal study of aging and meta-analysis. Biol Psychiatry. 2022;91(4):359-369. doi: 10.1016/j.biopsych.2021.08.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gonneaud J, Bedetti C, Pichet Binette A, et al. Association of education with Aβ burden in preclinical familial and sporadic Alzheimer disease. Neurology. 2020;95(11):e1554-e1564. doi: 10.1212/wnl.0000000000010314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cobb JL, Wolf PA, Au R, White R, D'Agostino RB. The effect of education on the incidence of dementia and Alzheimer's disease in the Framingham study. Neurology. 1995;45(9):1707-1712. doi: 10.1212/wnl.45.9.1707 [DOI] [PubMed] [Google Scholar]
- 38.McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association Workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):263-269. doi: 10.1016/j.jalz.2011.03.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Terracciano A, An Y, Sutin AR, Thambisetty M, Resnick SM. Personality change in the preclinical phase of Alzheimer disease. JAMA Psychiatry. 2017;74(12):1259-1265. doi: 10.1001/jamapsychiatry.2017.2816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Fratiglioni L, Marseglia A, Dekhtyar S. Ageing without dementia: can stimulating psychosocial and lifestyle experiences make a difference? Lancet Neurol. 2020;19(6):533-543. doi: 10.1016/s1474-4422(20)30039-9 [DOI] [PubMed] [Google Scholar]
- 41.Bleidorn W, Hill PL, Back MD, et al. The policy relevance of personality traits. Am Psychol. 2019;74(9):1056-1067. doi: 10.1037/amp0000503 [DOI] [PubMed] [Google Scholar]
- 42.Caspi A, Roberts BW, Shiner RL. Personality development: stability and change. Annu Rev Psychol. 2005;56:453-484. doi: 10.1146/annurev.psych.55.090902.141913 [DOI] [PubMed] [Google Scholar]
- 43.Costa PT, McCrae RR, Löckenhoff CE. Personality across the life span. Annu Rev Psychol. 2019;70:423-448. doi: 10.1146/annurev-psych-010418-103244 [DOI] [PubMed] [Google Scholar]
- 44.Damian RI, Spengler M, Sutu A, Roberts BW. Sixteen going on sixty-six: a longitudinal study of personality stability and change across 50 years. J Pers Soc Psychol. 2019;117(3):674-695. doi: 10.1037/pspp0000210 [DOI] [PubMed] [Google Scholar]
- 45.McAdams DP, Olson BD. Personality development: continuity and change over the life course. Annu Rev Psychol. 2010;61:517-542. doi: 10.1146/annurev.psych.093008.100507 [DOI] [PubMed] [Google Scholar]
- 46.Roberts BW, DelVecchio WF. The rank-order consistency of personality traits from childhood to old age: a quantitative review of longitudinal studies. Psychol Bull. 2000;126(1):3-25. doi: 10.1037/0033-2909.126.1.3 [DOI] [PubMed] [Google Scholar]
- 47.Roberts BW, Mroczek D. Personality trait change in adulthood. Curr Dir Psychol Sci. 2008;17(1):31-35. doi: 10.1111/j.1467-8721.2008.00543.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Stieger M, Flückiger C, Rüegger D, Kowatsch T, Roberts BW, Allemand M. Changing personality traits with the help of a digital personality change intervention. Proc Natl Acad Sci U S A. 2021;118(8):e2017548118. doi: 10.1073/pnas.2017548118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Roberts BW, Luo J, Briley DA, Chow PI, Su R, Hill PL. A systematic review of personality trait change through intervention. Psychol Bull. 2017;143(2):117-141. doi: 10.1037/bul0000088 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
3D longitudinal conscientiousness over CSFp-tau181 and EYO.Download Supplementary Video 1 (9.3MB, mov) via http://dx.doi.org/10.1212/209766_Video_1
3D longitudinal openness to experience over CSFp-tau181 and EYO.Download Supplementary Video 1 (9.2MB, mov) via http://dx.doi.org/10.1212/209766_Video_2
Data Availability Statement
All data from this study are available on request from the DIAN at dian.wustl.edu/our-research/observational-study/dianobservationalstudy-investigator-resources/. Analysis codes can be obtained from the corresponding author (J.S.K.).