

Abstract
Carcinosarcoma is a malignancy that occurs very rarely in the renal pelvis[1-3]; thus, only a very limited number of cases has been documented.[2,3] These tumors are composed of both carcinomatous and sarcomatous elements.[1] We report here a case of a carcinosarcoma composed of well-differentiated, keratinizing, squamous carcinoma cells and high-grade sarcoma cells. Differently from the cases described so far, this carcinosarcoma of the renal pelvis was characterized by the quick recurrence, following complete surgical resection, as a highly disseminated high-grade sarcoma.
A 66-year-old male comes to observation with a painless hematuria of 1-month duration.
Case Report
Mr. L, a 66-year-old male, came to observation because of a painless hematuria that had lasted for approximately 1 month. Computerized tomography showed a stone at the left ureteropelvic junction with severe hydronephrosis, and a 10×6 cm tumor in the renal pelvis. A nephroureterectomy with bladder cuff excision was performed in April 2002. The histopathology exam revealed a carcinosarcoma with clear surgical margins and no lymph node metastasis. However, 1.5 months later, the patient developed a fever of unknown origin. A second computerized tomography scan showed that the tumor had recurred, and it now occupied almost all of the left retroperitoneal space with invasion of the abdominal wall. An open biopsy revealed the presence of necrotic tumor tissue. The pathology report identified it as a pure high-grade sarcoma of undetermined phenotype. Regardless of therapeutic interventions, the patient died 4 months following surgery, in August 2002.
Pathologic Findings
Microscopically, the tumor was predominantly composed of undifferentiated neoplastic spindle cells and, partially, of well-differentiated, keratinizing, malignant, squamous cells. Immunohistochemically, the malignant squamous cells showed marked membranous staining for cytokeratin and negative staining for vimentin (Figure 1). Conversely, the sarcomatous pleomorphic tumor cells showed strong positive cytoplasmic staining for vimentin (Figure 2) and negative staining for smooth muscle actin, desmin, and epithelial membrane antigen (EMA/MUC1). The specimen obtained from the open biopsy of the recurrent tumor in the left renal fossa disclosed high-grade sarcoma of undetermined phenotype.
Figure 1.
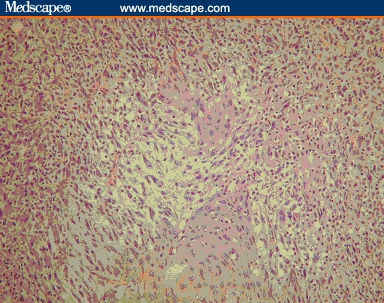
Hematoxylin/eosin (H&E) staining (x100) of the renal pelvis carcinosarcoma. Keratinizing squamous cell carcinomatous cells in the central part of the section are surrounded by neoplastic spindle cells
Figure 2.
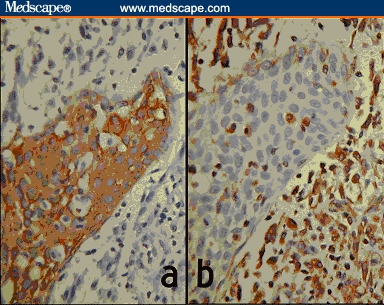
Cytokeratin (a) and vimentin (b) staining (x200) of the renal pelvis carcinosarcoma. Section (a) shows strong positive membranous staining in squamous cells and negative staining of sarcomatous cells. Section (b) shows a reverse staining pattern for vimentin
Discussion
Carcinosarcomas of the renal pelvis are known to be rapid in progression and associated with a poor prognosis.[2,3] They usually metastasize soon after nephroureterectomy, but very little information is available on the histologic types that characterize the recurrent tumors. In this case, we performed open biopsy for the relapsing patient and found that the recurrent tumor was composed only of the sarcomatous elements, a quite unexpected finding.
As mentioned by Petersen,[1] carcinosarcoma can develop as: (a) an undifferentiated cell differentiating along both an epithelial and a mesenchymal pathway; (b) a concomitant differentiation of a transformed epithelial cell and stromal cell within close proximity ultimately producing a single neoplasm; or (c) an established carcinoma inducing malignant transformation in the adjacent stroma, thus resulting in simultaneous proliferation of both elements.
Carcinosarcomas occur more frequently in the breast, larynx, and uterus; more rarely in the bladder, esophagus, lungs, fallopian tubes, and prostate; and they are extremely rare in the renal pelvis.[1,2] The first case, consisting of both transitional carcinoma cells and pleomorphic sarcoma cells, was reported by Fauci and colleagues in 1961. So far, there have been only approximately a dozen cases described in the literature. In Taiwan, there has been only 1 previous case reported, by Tseng and colleagues in 1996.[3]
Contributor Information
Chieh-Hsiao Chen, Department of Urology, China Medical University Hospital, Taichung, Taiwan.
Wen-Chi Chen, Department of Urology, China Medical University Hospital, Taichung, Taiwan.
Hsueh-Fu Lu, Department of Urology, China Medical University Hospital, Taichung, Taiwan.
Chao-Hsiang Chang, Department of Urology, China Medical University Hospital, Taichung, Taiwan; email jerrychen119@lsc.net.tw.
Chi-Long Chen, Department of Pathology, China Medical University Hospital, Taichung, Taiwan.
Hsuan-Hua Huang, Department of Pathology, China Medical University Hospital, Taichung, Taiwan.
References
- 1.Petersen RO. Urologic Pathology. 2nd ed. Philadelphia, Pa: JB Lippincott; 1992. pp. 128–132. [Google Scholar]
- 2.Chen KTK, Workman RD, Flam MS, DeKlotz RJ. Carcinosarcoma of renal pelvis. Urology. 1983;22:429–431. doi: 10.1016/0090-4295(83)90431-4. Abstract. [DOI] [PubMed] [Google Scholar]
- 3.Tseng YJ, Hsu K, Lin JW, Lin CC. Carcinosarcoma of the renal pelvis: a case report with immunohistochemical study. Changgeng Yi Xue Za Zhi. 1996;19:176–180. Abstract. [PubMed] [Google Scholar]