

Abstract
BACKGROUND:
India is one of the world’s developing countries, and its population is ageing, that is, increasing, which increases the demand for health care. Ageing is a natural process. Quality of life (QoL) and self-efficacy are two of the most important factors in human development. This is a study to assess the effectiveness of selected interventions on QoL and self-efficacy among elderly.
MATERIALS AND METHODS:
A community-based survey was used to select samples in a rural community. Data were collected between March 25 and April 23, 2022 using a quasi-experimental, one-group pre- and post-test research design. This survey was conducted among the elderly, of whom 60 were selected using simple random sampling techniques. Selected interventions were administered. The WHOQOL BREF (standardized tool) and GSE scales were used to assess the QoL and self-efficacy among the elderly.
RESULTS:
The study findings revealed that at the baseline level of QoL and self-efficacy, none of the subjects had good QoL and high self-efficacy, whereas after implementation of the selected interventions, the majority of the elderly had average QoL (98.3%) and 81.7% had high self-efficacy. The baseline mean score for QoL was 48.3% and that for self-efficacy was 61.3%, with post-test scores of 65.8% and 80.7%, respectively, and there was a statistical difference at P < 0.001.
CONCLUSION:
The study findings evidenced that selected interventions (education, reminiscence therapy, and demonstration of exercise) were effective in improving the QoL and self-efficacy among the elderly. Aged populations need to maintain their active, healthy, and happy living. Studies recommend these interventions are beneficial for elderly populations.
Keywords: Education, exercise, quality of life (QoL), reminiscence therapy, self-efficacy
Introduction
Ageing is a natural, unavoidable, biological, and universal process that results in a variety of changes in physical, psychological, hormonal, and social status.[1] The concept of “quality of life” (QoL) is the way individuals live and their perception of their position in their lives in respect to culture, values, and systems.[2]
An individual’s self-efficacy can be determined through their own effectiveness.[3] Self-efficacy also involves a generative capability that deals with cognitive, social, and behavioral skills.[4]
As per the data of the present century, the population belongs to the age group above 60 years; survey shows that the population of the elderly has been increasing.[5] There are approximately >600 million elderly people worldwide. According to projections, the number of people aged 65 years and older will more than double to 2 billion by 2050. With 7.7% of its population over 60, India is classified as an “aging nation.”[6]
According to recent data in India, the elderly population size has increased compared to the past decade. The estimated population increased from 24.71 million in the year 1961 to 104 million in the year 2011; the percentage increased from 5.6% to 8.6% of the total population. The population of the elderly is expected to increase 2011 from 8.6% in 2011 to 11.6% by 2026.[7]
A recent study shows that the elderly are less aware of QoL and have decreased QoL, so inclusionary measures such as participation in social clubs and awareness programs should be carried out at the community level to enhance QoL among the elderly.[8]
According to the study’s findings, the rural elderly population has a lower QoL in terms of social relations (55.92) than environmental quality (57.13). Hence, there is a need for health education for the elderly in relation to their social, physical, and group recreational activities, which help to construct their self-confidence and improve their QoL.[9]
According to the findings of this survey, health and care managers should pay more attention to health promotion, develop a continuous training program, and increase public health for the elderly, which could improve their QoL and self-efficacy.[10]
QoL has two important aspects, that is, objective and subjective. The majority of the elderly will evaluate their QoL in a positive way.[11] Socio-demographic factors, which are age, education, marital status, occupation, family income, and family structure, influence the QoL among the elderly.[12,13]
An experimental study was conducted on 80 elderly people. Intervention educational programs were conducted according to the PRECEDE model. The study results reveal that after the interventions, the mean score of QoL increased from 47.72 to 58.90. Hence, it concluded that using the PRECEDE model helps to increase the QoL in elderly.[14]
An experimental study was conducted on 60 adults. The exercises included a 5–10 minute circulatory warm-up, a 15 minute walking, and a 5–10 minute stretching/cool-down period. Exercises were performed under supervision of an expertise. This study concluded that an exercise program has a significant impact in QoL and self-efficacy in older adults.[15]
As per data, the demography of the elderly population is increasing globally and in the Indian context. Because of changes in physical, physiological, and psychological parameters, the ageing population faces numerous challenges in daily life. Elderly care is one of the most priority areas in India as this population ratio is high compared to the past decade. Every individual in the society has a responsibility to create a safe and healthy environment for the elderly out of concern and respect for this population. Normally, QoL decreases for the older population as ageing continues. In Western countries, more activities and programs are organized for this population to promote active and healthy living. The Government of India has also adopted a national policy on ageing. There are numerous programs and schemes for the elderly, but the health-care system still has gaps. Above all, not much research work has been carried out on this topic in India; therefore, this topic has become of concern. Hence, the researcher chooses the selected interventions to improve the QoL and self-efficacy among the elderly.
Materials and Methods
Research design and setting
Quantitative research was performed to assess the effectiveness of selected interventions on QoL and self-efficacy among the elderly. A quasi-experimental one-group pre-test–post-test research design was used. The pre-test was administered on the same day as the intervention, and the post-test was administered 20 days later, making the total duration of data collection 4 weeks. The study was conducted in Dodabastivillage, Bangalore, From March 25 to April 23, 2022.
Study participants and sampling
A house-to-house survey was conducted by a research investigator to find out eligible subjects. A total of 100 elderly were identified out of 60 selected by simple random sampling techniques using the lottery method. Based on the survey, the study was performed, and a selected intervention was carried out among the elderly.
Sample size estimation
The sample size of the study was calculated considering QoL as a primary outcome variable. A similar study was conducted by Majumdar A and Pavithra G. QoL and its associated factors were assessed using WHOQOL-BREF among elderly in urban Puducherry, India (Journal of clinical and diagnostic research: JCDR. 2014 Jan; 8(1):54.).[16] The sample size was estimated using power analysis [α = 5% and power (1-β) = 80%] and an effect size of 0.68. A total of 50 subjects were needed to achieve a significance of 0.05.
Sample size—estimated.
Study required = 50 subjects.
20% added for attrition.
Total samples required: 60.
Data collection and tools and techniques
The study was conducted for a total of 4 weeks. The researcher obtained permission from the concerned authority of the rural community (Sulikere PHC), and informed consent was taken from the sample under study. A community-based survey was conducted in Dodabasti village to identify the elderly. There were a total of 100 elderly people (60 were identified using the lottery method’s simple random sampling technique). The pre-test was conducted by administering standard tools (the WHOBREF scale) to assess the level of QoL and the General Self-Efficacy (GSE) scale to assess self-efficacy. Selected interventions were implemented, which included three components: education (the PRECEDE MODEL), reminiscence therapy, and exercise demonstrations. A 30-minutes education session based on the PRECEDE model was organized around physical activity, nutrition, mental health, leisure time, group activities, and environmental factors, followed by a reminiscence therapy session conducted by stimulating, reflecting, and talking about personal memories related to the events of childhood, work, marriage, social accomplishment, and the most memorable moment for the duration of 15 minutes. There were demonstrations of exercises such as warm-up, walking, range-of-motion exercise, and stretching for the duration of 15 minutes. All the sessions were organized by a research investigator. The demonstrated exercises were to be followed by the participants for 3 weeks, and a post-test was conducted on QoL and self-efficacy among the elderly.
The tool used for the study had three sections: Sections A, B, and C. Section A included demographic information regarding age, gender, religion, educational status, marital status, recreational activities, previous occupations, and any health-related problems. Section B, QoL, which was measured by WHOQOLBREF (1995), contains a total of 26 items and is divided into four domains: physical, social, psychological, and environmental. Scoring interpretation of the tool: 50% = Poor QoL, 50–75% = Average QoL, and >75% = Good QoL; a high score indicates good QoL, and a low score below 50% indicates poor QoL. Section-C, self-efficacy, was measured by administering the GSE Scale (1995), which has 10 items and a total score that ranges between 10 and 40. 50% indicates a lack of self-efficacy, 50–75% = moderately high self-efficacy, and >75% = high self-efficacy. A high score indicates high self-efficacy, and a low score below 50% indicates low self-efficacy. The split-half method tool gave reliability values of 0.87 and 0.85. The tool was reliable for this study. (Figure 1 Sample selection and data collection for the study)
Figure 1.
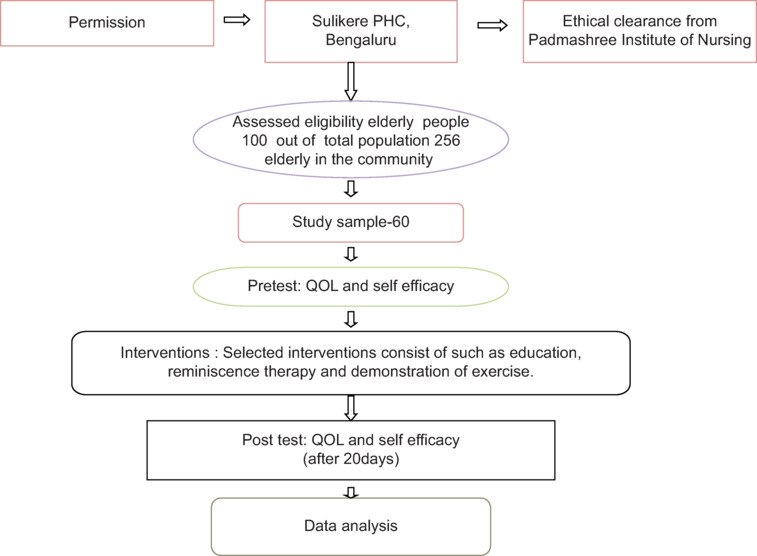
Sample selection and data collection for the study
Ethical consideration
The study was approved by the research ethical committee at the Padmashree Institute of Nursing, and formal permission was obtained from the concerned authority of Sulikere PHC with the registration number 05-N316-119599 on March 25, 2022, and informed consent was obtained from the subjects.
Analysis
The analysis of the data was done through the Statistical Package for Social Science (SPSS) version 20.0. A paired t-test was used to analyze the mean difference in the knowledge score between pre-test and post-test, and P < 0.05 levels were found to be highly significant.
Results
According to Table 1, (Table 1: Demographic characteristics of elderly) a total of 60 subjects were enrolled, with the majority of them (27.5%) belonging to ages between 61 and 65. There were more males (35.58%) than females. The demographic characteristics showed that out of 60, 27 (45%) of the participants had a primary education, and 20 (40%) of the elderly were unemployed.
Table 1.
Demographic characteristics of elderly (n=60)
| Demographic variables | Frequency | Percentage |
|---|---|---|
| Age of the elderly (in years) | ||
| a) 61-65 | 27 | 45.0 |
| b) 66-70 | 22 | 36.7 |
| c) Above 70 years | 11 | 18.3 |
| Gender | ||
| a) Male | 35 | 58.3 |
| b) Female | 25 | 41.7 |
| Education | ||
| a) Primary education | 27 | 45.0 |
| b) Secondary education | 22 | 36.7 |
| c) PUC | 7 | 11.7 |
| d) Graduate and above | 4 | 6.7 |
| Religion | ||
| a) Hindu | 17 | 28.3 |
| b) Muslim | 23 | 38.3 |
| c) Christian | 20 | 33.3 |
| Nature of previous occupation | ||
| a) Unemployed | 24 | 40.0 |
| b) Daily wages | 22 | 36.7 |
| c) Government employees | 14 | 23.3 |
| d) Private employee | - | - |
| Marital status | ||
| a) Married | 38 | 63.3 |
| b) Widower/widow | 16 | 26.7 |
| c) Divorce | 6 | 10.0 |
| d) Unmarried | - | |
| Source of income | ||
| a) Pension | 14 | 23.3 |
| b) Children | 23 | 38.3 |
| c) Old age pension | 18 | 30.0 |
| d) Nil | 5 | 8.3 |
| Recreation activities done in daily living | ||
| a) Listening music | 11 | 18.3 |
| b) Gardening | 23 | 38.3 |
| c) Spending time with grand children | 19 | 31.7 |
| d) Watching TV | 7 | 11.7 |
| e) If any other (specify) | - | - |
| Any health-related problem | ||
| a) Yes | 23 | 38.3 |
| b) No | 37 | 61.7 |
| c) If yes specify | - | - |
Level of QoL and self-efficacy in the pre-test and post-test
QoL indicates that the acquired result of the pre-test level of QoL in the elderly with poor QoL shows less than 50% of the frequency level, that is, 75%. Around 25%, that is, 15 of the elderly, had an average QoL. The study shows that none of the elderly had good QoL. On the contrary, the results of the post-test show a great deal of variation, with around 59 (98.3%) having average QoL, 1 (1.7%) having good QoL, and none of the elderly having poor QoL. This shows that after the administration of selected interventions, there was an improvement in the level of QoL as compared with the pre-test results. (Figure 2: Pre and post test level of QOL).
Figure 2.
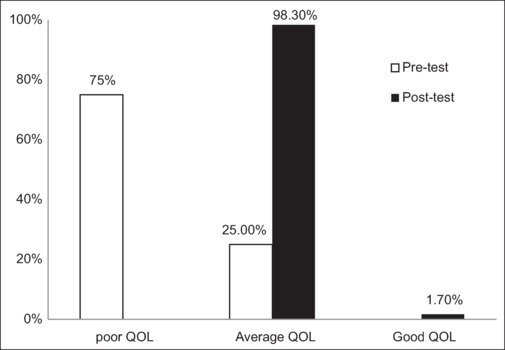
Pre-test and post-test level of QOL
Self-efficacy shows that 60 participants (100%) had moderate self-efficacy in the pre-test, and none had low or high self-efficacy. Following the interventions, the post-test revealed a significant variation, with 49 (81.7%) having high self-efficacy. Eleven (18.3%) of the elderly had moderate self-efficacy, and none of the elderly had low self-efficacy. This shows that after the administration of selected interventions, there was an improvement in the level of self-efficacy as compared with the pre-test results. (Figure 3: Pre and and post test of Self efficacy).
Figure 3.
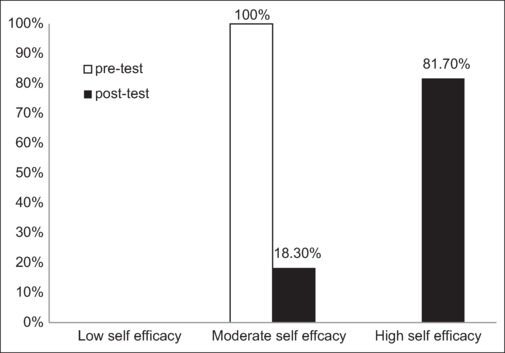
Pre-test and post-test level of self-efficacy
The baseline mean score is 62.78, and the post-test mean score is 85.58. The difference in mean score is 22.8, which indicates that there was an improvement in the level of QoL after the administration of selected interventions among the study population. Selected interventions have a positive impact on increasing the level of QoL, which influences the improvement of QoL among the elder population.
The baseline mean score is 24.52, and the post-test mean score is 32.30. The difference in mean score is 7.78, which indicates that there was an improvement in the level of self-efficacy after administration of selected interventions among the study population. Selected interventions have a positive impact on increasing the level of self-efficacy, which influences the improvement of QoL among the elder population. (Table 2: Range, Mean and SD in the pre and post test).
Table 2.
Range, Mean, and SD of pre-test and post-test (n=60)
| Domains of QoL | Max score | Pre-test |
Post-test |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Range | Mean | SD | Mean % | Range | Mean | SD | Mean % | ||
| Physical health | 45 | 15-27 | 20.93 | 2.81 | 46.5 | 19-33 | 25.68 | 2.97 | 57.1 |
| Psychological health | 30 | 10-23 | 14.80 | 2.07 | 49.3 | 14-25 | 20-25 | 2.06 | 67.5 |
| Social Relationships | 15 | 5-10 | 7.30 | 1.18 | 48.6 | 9-14 | 11.62 | 1.15 | 77.4 |
| Environment | 40 | 16-25 | 19.75 | 1.91 | 49.6 | 23-33 | 28.03 | 2.20 | 70.1 |
| Overall QoL | 130 | 50-72 | 62.78 | 3.52 | 48.3 | 76-99 | 85.58 | 4.79 | 65.8 |
| Self-efficacy | 40 | 21-28 | 24.52 | 1.77 | 61.3 | 24-36 | 32.3 | 2.6 | 80.7 |
The overall mean difference was 22.80, the standard deviation was 5.25, the mean difference percentage was 17.5%, and the paired t-test value was 33.60. These scores show a highly significant difference at the P < 0.05 level. Furthermore, at the P < 0.05 level, there was statistical significance in all aspects of QoL. The highest mean percentage was identified in the domains of QoL pertaining to social relationships, and the lowest percentage was identified in physical health. This trend shows that most subjects were unaware of physical health, and after selected interventions, the subjects gained a high level of knowledge about QoL. The interventions improved the level of QoL among the elderly. (Table 3: Comparison of QoL and Self efficacy in the pre and post tests).
Table 3.
Comparison of QoL and self-efficacy in the pre- and post-tests (n=60)
| Domains of QoL | Max score | Enhancement |
Paired t-test | P | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean % | ||||
| Physical health | 45 | 4.75 | 3.45 | 10.5 | 10.642* | P<0.05 |
| Psychological health | 30 | 5.45 | 2.45 | 18.2 | 17.165* | P<0.05 |
| Social Relationships | 15 | 4.31 | 1.52 | 29.7 | 21.944* | P<0.05 |
| Environment | 40 | 8.28 | 2.79 | 20.7 | 22.974* | P<0.05 |
| QoL | 130 | 22.80 | 5.25 | 17.5 | 33.604* | P<0.05 |
| Self-efficacy | 40 | 8.16 | 0.39 | 20.4 | 16.212* | P<0.005 |
*Denotes significant (P<0.05) for df=59
The overall mean difference was 8.16, the standard deviation was 0.39, the mean difference percentage was 20.4%, and the paired t-test value was 16.21. These scores show a highly significant difference at the P < 0.005 level. Furthermore, at the P < 0.005 level, there was statistical significance in the level of self-efficacy. The interventions improved the level of self-efficacy among the elderly.
Correlation between QoL and self-efficacy (n = 60)
In reference to the correlation between level of QoL and self-efficacy, the pre-test correlation was 0.342 and the post-test correlation was 0.368, and it was found to be positive. A weak correlation shows an increased QoL and an increased self-efficacy level and is found to be statistically significant (P < 0.05).
Discussion
The study was undertaken to identify the impact of selected interventions on QoL and self-efficacy among the elderly in a rural community. According to data, the prevalence of the elderly in India is increasing.[17] Study results revealed that the selected interventions had improved the level of QoL and self-efficacy; there was a significant improvement in the mean score from 62.78 to 85.58 after administration of the selected interventions (a mean difference of 22.8). At the P < 0.05 level, the selected interventions were statistically significant in terms of post-test knowledge level.
The finding of the study, supported by a cross-sectional study that included educational interventions such as physical activity, advice on healthy food intake, and other aspects of management, shows an improvement in QoL among the elderly.[18]
Study results revealed that reminiscence therapy had improved the QoL among the elderly; there was a significant improvement in the mean score from 14.6 to 15.71 after the administration of the intervention. The educational program was statistically significant in the post-test level of knowledge at the P < 0.001 level.[19]
A cross-sectional study was conducted to assess the QoL among the elderly, which showed 64.41% had an average QoL, 24.10% had a poor QoL, and 14.45% had a good QoL. Therefore, the study concluded that there is a need for health education for the elderly with respect to their social, physical, and group recreational activities that will help to construct their self-confidence and thereby improve their QoL.[20]
The above result suggests a need to improve QoL and self-efficacy among the elderly by using new strategies. Participants in the interventions program had a better understanding of QoL and self-efficacy.
Most elderly and family members may not be aware of QoL and self-efficacy. As a result, providing an intervention program (education, exercise demonstrations, and reminiscence therapy) to the elderly can help to improve QoL and self-efficacy. Furthermore, promoting knowledge about changes in the elderly among the public helps make the world a better place for the elderly. Educational programs can be conducted in hospitals and other health care settings by involving family members to enhance their knowledge and improve the QoL of the elderly. A similar study can be done with a large sample to validate and generalize the findings. Adequate support, motivation, and encouragement by the management and authorities of an organization can enable various research activities; this could be the quest of many novice nurses.[21,22,23]
Need-based awareness programs can be carried out by involving student nurses in the public in collaboration with voluntary organizations among the elderly population. Nurses can be actively involved in community or elderly self-help groups for the implementation of new strategies. The current study findings support the long-term administration of this intervention, which had a very positive effect on QoL.
Limitations and recommendation
The research study’s small population is its limitation. The level of knowledge can differ based on their educational background. The study focuses on the elderly population. We could not include some factors, like mental health status or the complications of chronic morbid conditions in the elderly. The study cannot be generalized; hence, it involves only one group of people.
Conclusion
The chosen intervention program improved the elderly’s QoL and self-efficacy significantly. Meanwhile, there is an urgency to conduct an educational program in various settings such as hospitals, home care, old age homes, and communities in order to raise and improve the knowledge of the elderly and health care providers as well as to have a positive impact on the health and protection of the elderly.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
Our special gratitude goes to the Padmashree Institute of Nursing, the medical surgical department, the HOD, and all the study participants.
References
- 1.Singh J. Comparative study of quality of life in aged persons. Indian J Appl Res. 2014:1–3. [Google Scholar]
- 2.Whoqol Group The World Health Organization quality of life assessment (WHOQOL): position paper from the World Health Organization. Social science & medicine. 1995;41:1403–9. doi: 10.1016/0277-9536(95)00112-k. [DOI] [PubMed] [Google Scholar]
- 3.Grembowski D, Patrick D, Diehr P, Durham M, Beresford S, Kay E, et al. Self-efficacy and health behavior among older adults. J Health Soc Behav. 1993;34:89–104. [PubMed] [Google Scholar]
- 4.Bandura A. Self-efficacy mechanism in human agency. Am Psychol. 1982;37:122. [Google Scholar]
- 5.Verma R, Khanna P. National program of health-care for the elderly in India: A hope for healthy ageing. International journal of preventive medicine. 2013;4:1103. [PMC free article] [PubMed] [Google Scholar]
- 6.Desa U. United nations department of economic and social affairs, population division. World population prospects: The. 2015 [Google Scholar]
- 7.Banerjee S. Determinants of rural-urban differential in healthcare utilization among the elderly population in India. BMC Public Health. 2021;21:939. doi: 10.1186/s12889-021-10773-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Devraj S, D’mello MK. Determinants of quality of life among the elderly population in urban areas of Mangalore, Karnataka. J Geriatr Ment Health. 2019;6:94–8. [Google Scholar]
- 9.Mudey A, Ambekar S, Goyal RC, Agarekar S, Wagh VV. Assessment of quality of life among rural and urban elderly population of Wardha District, Maharashtra, India. Stud Ethno-Med. 2011;5:89–93. [Google Scholar]
- 10.Shaabani J, Rahgoi A, Nourozi K, Rahgozar M, Shaabani M. The relationship between self-efficacy and quality of life among elderly people. Iran J Ageing. 2017;11:518–27. [Google Scholar]
- 11.Netuveli G, Blane D. Quality of life in older ages. Br Med Bull. 2008;85:113–26. doi: 10.1093/bmb/ldn003. [DOI] [PubMed] [Google Scholar]
- 12.Raju SS. Building knowledge base on population ageing in India working paper: 2. United Nations Population Fund; Studies on ageing in India: A review. [Google Scholar]
- 13.Barua A, Mangesh R, Kumar Harsha HN, Mathew S. A cross-sectional study on quality of life in geriatric population. Indian J Community Med. 2007;32:146–7. [Google Scholar]
- 14.Mazloomymahmoodabad S, Masoudy G, Fallahzadeh H, Jalili Z. Education based on precede-proceed on quality of life in elderly. Glob J Health Sci. 2014;6:178–84. doi: 10.5539/gjhs.v6n6p178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lee MK, Oh J. Health-related quality of life in older adults: Its association with health literacy, self-efficacy, social support, and health-promoting behavior. Healthcare (Basel) 2020;8:407. doi: 10.3390/healthcare8040407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vitorino LM, Paskulin LM, Viana LA. Quality of life among older adults resident in long-stay care facilities. Rev Lat Am Enfermagem. 2012;20:1186–95. doi: 10.1590/s0104-11692012000600022. [DOI] [PubMed] [Google Scholar]
- 17.Kumar SG, Majumdar A, G P. Quality of life (QOL) and its associated factors using WHOQOL-BREF among elderly in urban Puducherry, India. J Clin Diagn Res. 2014;8:54–7. doi: 10.7860/JCDR/2014/6996.3917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rana AK, Wahlin A, Lundborg CS, Kabir ZN. Impact of health education on health-related quality of life among elderly persons: Results from a community-based intervention study in rural Bangladesh. Health Promot Int. 2009;24:36–45. doi: 10.1093/heapro/dan042. [DOI] [PubMed] [Google Scholar]
- 19.Devi V. Assess the quality of life among elderly before and after reminiscence therapy in a selected old age home at Chennai (Doctoral dissertation, Padmasree College of Nursing, Walajabad) [Google Scholar]
- 20.Raj D, Swain PK, Pedgaonkar SP. A study on quality of life satisfaction & physical health of elderly people in Varanasi: An urban area of Uttar Pradesh, India. Int J Med Sci Publ Health. 2014;3:616–20. [Google Scholar]
- 21.Dkhar E, Balu V, Kamei S. Effectiveness of educational programme on knowledge regarding abuse and age-related changes among elderly population. J Clin Diagnostic Res. 2022;16:13–8. [Google Scholar]
- 22.Javadzade SH, Sharifirad G, Radjati F, Mostafavi F, Reisi M, Hasanzade A. Relationship between health literacy, health status, and healthy behaviors among older adults in Isfahan, Iran. J Educ Health Promot. 2012;1:31. doi: 10.4103/2277-9531.100160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rezaeian M, Sharifirad G, Mostafavi F, Moodi M, Abbasi MH. The effects of breast cancer educational intervention on knowledge and health beliefs of women 40 years and older, Isfahan, Iran. J Educ Health Promot. 2014;3:43. doi: 10.4103/2277-9531.131929. [DOI] [PMC free article] [PubMed] [Google Scholar]