

Abstract
Background
Robot-Assisted Gait Training (RAGT) is a novel technology widely employed in the field of neurological rehabilitation for patients with subacute stroke. However, the effectiveness of RAGT compared to conventional gait training (CGT) in improving lower extremity function remains a topic of debate. This study aimed to investigate and compare the effects of RAGT and CGT on lower extremity movement in patients with subacute stroke.
Methods
Comprehensive search was conducted across multiple databases, including PubMed, Web of Science, Cochrane Library, EBSCO, Embase, Scopus, China National Knowledge Infrastructure, Wan Fang, SinoMed and Vip Journal Integration Platform. The database retrieval was performed up until July 9, 2024. Meta-analysis was conducted using RevMan 5.4 software.
Results
A total of 24 RCTs were included in the analysis. The results indicate that, compared with CGT, RAGT led to significant improvements in the Fugl-Meyer Assessment for Lower Extremity [MD = 2.10, 95%CI (0.62, 3.59), P = 0.005], Functional Ambulation Category[MD = 0.44, 95%CI (0.23, 0.65), P < 0.001], Berg Balance Scale [MD = 4.55, 95%CI (3.00, 6.11), P < 0.001], Timed Up and Go test [MD = −4.05, 95%CI (−5.12, −2.98), P < 0.001], and 6-Minute Walk Test [MD = 30.66, 95%CI (22.36, 38.97), P < 0.001] for patients with subacute stroke. However, it did not show a significant effect on the 10-Meter Walk Test [MD = 0.06, 95%CI (−0.01, 0.14), P = 0.08].
Conclusions
This study provides evidence that RAGT can enhance lower extremity function, balance function, walking ability, and endurance levels compared to CGT. However, the quality of evidence for improvements in gait speed remains low.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12984-024-01463-1.
Keywords: Gait, Lower Extremity, Meta-analysis, Robotics, Stroke, Walking Speed
Background
Stroke is a neurological disorder caused by either a rupture or blockage of cerebral blood vessels, resulting in high morbidity, disability, and a substantial social burden [1]. Globally, there were approximately 12.2 million incident cases of stroke, 101 million prevalent cases of stroke, and 6.55 million deaths attributed to stroke [2]. Stroke survivors usually experience physical dysfunction, notably affecting walking, which increases their risk of falling due to compromised gait and balance. This not only directly jeopardizes mobility and daily life, but also significantly diminishes their quality of life [3, 4]. Regaining the ability to walk is a critical milestone in the recovery of stroke survivors [5]. Physical rehabilitation plays a crucial role in improving motor function, mobility, and performance in daily life for stroke patients, particularly those with lingering movement disorders, and aiming to enhance their function, independence, and participation [6].
Conventional gait training (CGT) methods encompassing conventional floor gait training, stair gait training, and treadmill training, have been widely utilized in the rehabilitation of stroke survivors. CGT methods provided by therapists can improve gait speed and endurance, and other functional aspects for stroke survivors. Despite its benefits, CGT has several limitations, for example, the therapist ‘s physical limitations, vulnerable to interference from the outside environment, etc [5, 7]. Confronted with the huge rehabilitation needs of stroke patients, more effective treatment methods should be taken [8]. Robot-assisted gait training (RAGT) is widely used as a novel neurorehabilitation training technique. The robot equipment can include end-effector and exoskeleton systems [9], which are more effective in improving mobility than traditional therapy because they can provide a higher volume and more intensive treatment options [10]. These technologies are particularly effective in minimizing environmental disturbances during the rehabilitation process [11]. However, the efficacy of RAGT in the comprehensive rehabilitation of stroke survivors has yet to reach full satisfaction, indicating the need for further refinement and research in this area.
Existing studies point out that RAGT surpasses CGT in enhancing gait ability, balance function, and overall quality of life [12–14]. However, some studies challenge this view, suggesting that RAGT is not superior to traditional gait training in some respects [15, 16]. Amidst this backdrop, there are currently ongoing systematic evaluations or Meta-analyses with mixed results. For instance, Calafiore et al [17]. showed that robotic exoskeletons may have a potential role in walking ability recovery among subacute stroke patients. Conversely, Wang et al [18]. indicated that RAGT is an effective intervention to improve balance function in stroke survivors. Nedergård et al [19]. found no significant differences on step speed, treadmill frequency, stride length, and spatial asymmetries between the RAGT and the control group, leading to meta-analyses that also report no significant advantage of RAGT over CGT. The discrepancy in findings underscores the complexity of stroke rehabilitation and the variable effectiveness of RAGT. Therefore, this study aimed to delve into the effect of RAGT on the lower extremity function of subacute stroke patients through a Meta-analysis. By focusing on the subacute stage of stroke recovery, which is critical for rehabilitation, this study seeks to clarify the role of RAGT in enhancing the lower extremity function of stroke survivors, thereby offering valuable insights for clinical rehabilitation practices.
Method
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines were followed for the methodology of this study (See supplementary material 1). This study was registered on the international system evaluation registration platform PROSPERO (CRD42023453035).
Search strategy
A systematic search of the literature up to July 9, 2024, was conducted in languages limited to English and Chinese. Search databases included China National Knowledge Infrastructure (CNKI), Wan Fang Data Knowledge Service Platform, Vip Journal Integration Platform (VIP), SinoMed Database, Web of Science (WOS), PubMed, EBSCO, Embase, Cochrane Library, and Scopus databases. A combination of thematic and free-word searches was used, and supplemented by manual searches. The search terms were stroke, cerebrovascular accidents, CVA, cerebrovascular apoplexy, robot, robot assisted gait training, robot-assisted gait rehabilitation, randomly, trial, groups, etc. Detailed search strategies are described in Supplementary material 2. The relevant references in included studies and existing systematic reviews were searched manually.
Inclusion criteria and exclusion criteria
Inclusion criteria: [1] Population: Patients with a definite diagnosis of stroke, aged 18 years or older, with disease duration within 6 months, and stable vital signs and conscious; [2] Intervention: robot-assisted gait training; [3] Comparator: conventional gait training (physical therapy, exercise therapy, treadmill training, etc.); [4] Outcomes: Fugl-Meyer Assessment for lower extremity (FMA-LE), 10-Meter Walk Test (10MWT), 6-Minute Walking Test (6MWT), Berg Balance Scale (BBS), Timed Up and Go Test (TUG), Functional Ambulation Category scale (FAC); [5] Study design: Randomized controlled trials published in Chinese and English.
Exclusion criteria: [1] Lack of data on outcome metrics; [2] Duplicate studies and studies with incomplete data; [3] Abstracts, reviews, and conference reports; [4] Studies of too low quality.
Selection process
The retrieved studies were imported into Endnotes 20. Two researchers (MMH and SW) performed independent screening based on predetermined inclusion and exclusion criteria. Duplicate literature was first removed through Endnotes 20. The first screening was carried out according to the title and abstract, and the second screening was carried out after reading the full text. The two evaluators will cross-check the included studies. In the event of disagreement, a third researcher (KPL) will decide whether the study should be included or not.
Data extraction
Two researchers (MMH and SW) independently read the full text and have recorded the name of the first author, year of publication, country, duration of disease, age of patients, sample size, intervention, duration of intervention, type of robot, outcome indicators, and duration of follow-up. When differences arise, they must first be resolved through discussion, and if the disagreement persisted, the decision was made by a third researcher (LD). Articles with incomplete data were obtained by sending an e-mail to the authors.
Quality assessment
The quality assessment was conducted independently by two researchers (MMH and SW) using the Cochrane Risk of Bias Tool 2.0 (RoB2) [20]. The RoB2 sets out five domains of evaluation: bias in the randomization process; bias in deviating from established interventions; bias in missing outcome data; bias in outcome measurement and bias in selective reporting of outcomes. If all elements of the assessment are at low risk, this means that there is little or no risk of bias and the quality is A. If the assessment partially meets the low risk, this means that the risk of bias is medium and the quality is B. If none of the elements meet the low risk, this means that the risk of bias is very high and the quality is C. If there were differences, they were resolved through discussion with a third researcher (LD).
Statistical analyses
Data were combined and tested for statistical heterogeneity using RevMan 5.4 software. The mean difference (MD) and its 95% confidence interval (CI) were used for statistical analysis of effect values. If P > 0.1 and I2 ≤ 50%, the heterogeneity was considered insignificant, and the fixed-effects model was used for meta-analysis. If P < 0.1 and I2 > 50%, the heterogeneity was considered significant, and the random-effects model was used for meta-analysis.
Subgroup analysis was conducted to assess the influence of the following factors on the estimated effect: (1) Duration of the intervention: two, three, four, and eight weeks. We selected these boundaries specifically because they were the most commonly used in the included studies. (2) The robot type: exoskeletons (e.g., Lokomat, BEAR-H1, Hybrid Assistive Limb, etc.) or end-effectors (e.g., Gait Trainer, Gait Master, Morning Walk, etc.).
Sensitivity analyses were used to identify sources of heterogeneity. Publication bias was assessed by using funnel plots and the Egger's test, with p-values less than 0.1 indicating the presence of potential publication bias. The significance level for all analyses was P < 0.05.
Results
Results of literature search
A total of 15,838 pieces of relevant literature were initially retrieved, including 1 piece of grey literature, and 4,502 pieces of duplicate literature were excluded. A total of 220 pieces of literature were included by reading the title and abstract. After further searching and reading the full text, the studies that did not meet the inclusion criteria, including issues related to the duration of disease, intervention group measures, control group measures, and research type were removed, resulting in the inclusion of 24 studies. The literature screening process and results are shown in Fig. 1.
Fig. 1.

Flow diagram of the study selection process
Quality evaluation
According to the Cochrane risk assessment tool RoB2, the quality of the included 24 studies was evaluated, of which 21 were at some risk and 3 were at low risk. The specific evaluation indicators and results are shown in Fig. 2.
Fig. 2.
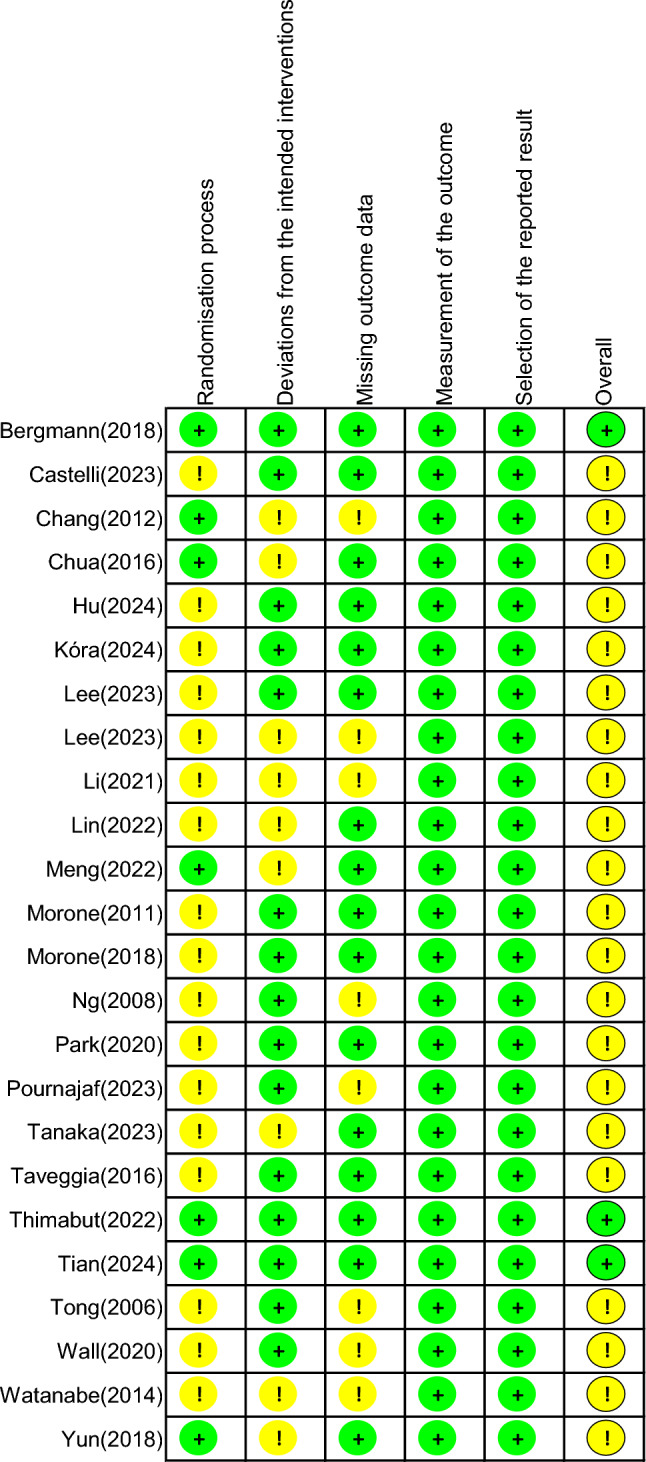
Risk of bias assessment for included studies
Basic characteristics of literature included in the analysis
The basic characteristics of the included studies are shown in Supplementary material 3. 24 studies were included [12, 21–43], with a total of 1103 cases, including 567 cases in the intervention group and 536 cases in the control group. The publication years of the included studies ranged from 2006 to 2024, the disease duration of patients ranged from 2 days to 6 months, the duration of interventions ranged from 2 to 8 weeks, 8 studies were followed up [21, 23, 26, 29, 33–35, 42], 15 studies used exoskeleton robots for interventions [12, 21, 22, 24, 25, 30, 33–37, 39, 40, 42, 43], 7 studies used end-effectors [23, 27–29, 32, 38, 41, 43], 2 studies used both exoskeletons and end-effectors[26, 31], 12 studies used random number tables[12, 21, 23, 28, 29, 32, 36–41], 7 studies had allocation concealment [12, 21–23, 35, 36, 40], and 12 studies had blinded to assessor [12, 21–23, 25, 26, 28, 31, 33, 34, 36, 41].
Results of meta-analysis
FMA-LE
Eight studies reported the effect of RAGT on FMA-LE, as shown in Fig. 3(a), which shows that there was no significant heterogeneity among the studies (P = 0.33, I2 = 13%), and a fixed effect model was used. Meta-analysis showed that the difference was statistically significant [MD = 2.10, 95%CI (0.62, 3.59), P = 0.005].
Fig. 3.

The forest plot of Fugl-Meyer Assessment for Lower Extremity, Functional Ambulation Category Scale and Berg Balance Scale. Figure a shows the forest plot of Fugl-Meyer Assessment for Lower Extremity, Figure b shows the forest plot of Functional Ambulation Category Scale, Figure c shows the forest plot of Berg Balance Scale
FAC
Sixteen studies reported the effect of RAGT on FAC, as shown in Fig. 3(b), which shows that the random effects model was used due to the large heterogeneity of the studies (P = 0.007, I2 = 52%). Meta-analysis results showed that the difference was statistically significant [MD = 0.44, 95%CI (0.23, 0.65), P < 0.001].
BBS
Ten studies reported the effect of RAGT on BBS, as shown in Fig. 3(c), which shows that there was no significant heterogeneity among the studies (P = 0.91, I2 = 0%), and a fixed effect model was used. Meta-analysis showed that the difference was statistically significant [MD = 4.55, 95%CI (3.00, 6.11), P < 0.001].
TUG
Seven studies reported the effect of RAGT on TUG. The study by Meng et al [12]. was not included in the analysis because the TUG test was combined with a dual-task walking test related to motor-cognitive interaction. as shown in Fig. 4(a), which shows that there was no significant heterogeneity among the studies (P = 0.37, I2 = 7%), and a fixed effect model was used. Meta-analysis showed that the difference was statistically significant [MD = −4.05, 95%CI (−5.12, −2.98), P < 0.001].
Fig. 4.

The forest plot of Timed Up and Go Test, 6-Minute Walking Test and 10-Meter Walk Test. Figure a shows the forest plot of Timed Up and Go Test, Figure b shows the forest plot of 6-Minute Walking Test, Figure c shows the forest plot of 10-Meter Walk Test
6MWT
Ten studies reported the effect of RAGT on 6MWT, as shown in Fig. 4(b), which shows that there was no significant heterogeneity among the studies (P = 0.40, I2 = 4%), and a fixed effect model was used. Meta-analysis showed that the difference was statistically significant [MD = 30.66, 95%CI (22.36, 38.97), P < 0.001].
10MWT
Eight studies reported the effect of RAGT on 10MWT, as shown in Fig. 4(c), which shows that there was no significant heterogeneity among the studies (P = 0.14, I2 = 35%), and a fixed effect model was used. The results of the meta-analysis showed that the difference was not statistically significant [MD = 0.06, 95%CI (−0.01, 0.14), P = 0.08].
Subgroup analysis
Duration of intervention
Subgroup analysis of FMA-LE according to duration of intervention was performed, as shown in Fig. 5(a). The analysis showed that at 4 weeks of intervention, RAGT improved the FMA-LE level of patients better than CGT [MD = 2.39, 95%CI (0.41, 4.36), P = 0.02].
Fig. 5.

The results of subgroup analysis based on the duration of intervention. Figure a shows subgroup analysis based on intervention time in Fugl-Meyer Assessment for Lower Extremity. Figure b shows subgroup analysis based on intervention time in Functional Ambulation Category Scale
Subgroup analysis of FAC according to duration of intervention was performed, as shown in Fig. 5(b). The analysis showed that at 4 weeks of intervention, RAGT improved the FAC level of patients better than CGT [MD = 0.57, 95%CI (0.32, 0.82), P < 0.001]. It should be noted that in the study by Pournajaf et al [31], data from 20 intervention sessions could not be combined, and only descriptive analyses were performed, showing that 20 intervention sessions improved FAC levels in patients.
Robot type
Subgroup analysis of the 6MWT was performed according to robot type, see Fig. 6(a). The analysis showed that the exoskeleton RAGT improved the endurance level of patients better than the CGT [MD = 31.26, 95%CI (22.57, 39.95), P < 0.001].
Fig. 6.

The results of subgroup analysis based on the different robot types. Figure a shows subgroup analysis based on the different robot types in 6-Minute Walking Test. Figure b shows subgroup analysis based on the different robot types in 10-Meter Walk Test
Subgroup analysis of the 10MWT was performed according to robot type, see Fig. 6(b). The analysis showed that the exoskeleton RAGT improved the endurance level of patients better than the CGT [MD = 0.16, 95%CI (0.05, 0.27), P = 0.005].
Sensitivity analysis
Sensitivity analysis for the FAC was conducted, which eliminated one study due to its high heterogeneity. After this, the analysis showed no significant heterogeneity (P = 0.09, I2 = 35%), and the fixed-effects model was used for the analysis. The meta-analysis results showed that the MD = 0.42, 95% CI (0.27, 0.56), P < 0.001, and the pooled results were not significantly changed, as shown in Fig. 7.
Fig. 7.

Sensitivity analysis of Functional Ambulation Category Scale
Publication bias analysis
There were at least 10 studies on FAC, BBS, and 6MWT in the literature, and to assess publication bias, we drew funnel plots of FAC, BBS, and 6MWT, as shown in Fig. 8. The results indicated symmetrical distribution of the data, with a smaller offset for published studies. Egger’s test for publication bias yielded P values of 0.945 for FAC, 0.247 for BBS, and 0.250 for 6MWT.
Fig. 8.

Funnel plot. Figure a shows the funnel plot of Functional Ambulation Category Scale, Figure b show the funnel plot of Berg Balance Scale, Figure c shows the funnel plot of 6-Minute Walking Test
Discussion
Lower extremity dysfunction and balance impairment are the key risk factors for accidental falls in stroke patients, severely limiting their mobility and daily activities [44]. Active physical rehabilitation is essential for enhancing their physical activity, facilitating the early recovery, and maximizing their reintegration into society and family life [45]. A retrospective longitudinal cohort study showed that functional improvement was significant within the first 6 months after stroke onset, so the first 6 months after stroke onset is the key to implementing rehabilitation [46]. Despite this, traditional rehabilitation treatments face numerous challenges and limitations. Considering the extensive rehabilitation needs of stroke survivors, there is a pressing demand for more efficacious rehabilitation strategies. RAGT can strengthen weak muscle groups and contribute to the recovery of the nervous system [46]. Furthermore, RAGT eliminates the need for manual placement of paralyzed extremities or assistance with trunk movement, significantly reducing the physical burden of therapists [47]. Nonetheless, the debate continues regarding the effectiveness of RAGT compared to CGT methods. According to the 2020 Canadian Stroke Best Practice recommendation states that RAGT devices may be considered for those who cannot walk. However, they should not replace CGT [48]. Additionally, a narrative review mentions RAGT as a promising alternative to conventional therapy by providing intensive, standardized care [49].
The current debate on the systematic evaluation of RAGT for lower extremity function in stroke patients is evolving, with an increasing number of original studies being published, highlighting the importance of incorporating the most recent findings into analysis [17, 19]. Therefore, this study has included randomized controlled trials with RAGT as the intervention group and CGT as the control group, and the disease course of subjects was within six months. RAGT can significantly improve outcomes measured by the FMA-LE, FAC, BBS, TUG, and 6MWT of patients with subacute stroke, but has no significant effect on 10MWT scores. These results suggest that while RAGT offers substantial benefits in certain aspects of lower extremity function and balance, its effects on specific walking speed may require further investigation.
Effect of RAGT on lower extremity function in subacute stroke patients
The results of the meta-analysis revealed that RAGT could effectively improve the FME-LE level in patients with subacute stroke compared with the CGT group, and the intervention that lasted for four weeks was the best. Our results showed some differences when compared to those of previous studies, which may be due to the inclusion of the latest randomized controlled trials in this study [50, 51]. This inclusion has increased the quality of evidence and provided a more thorough assessment of the effects of RAGT in patients with subacute stroke.
A study [52] has shown that postural stability can be significantly improved in the first two months after stroke, but it is not directly associated with the recovery of the most affected extremity. Instead, patients tend to utilize the less affected side for functional exercise. RAGT uniquely addresses this issue by encouraging patients to shift their center of gravity towards the more affected side without the fear of falling. Therefore, the patient can carry out rehabilitation treatment with sufficient intensity, thereby enhancing the plasticity of the nerve, and improving the function of the lower extremity [35, 53]. The emphasis on using the more affected side in RAGT helps to balance the rehabilitation focus, potentially offering a more holistic approach to improving the overall function of stroke survivors.
The heterogeneity of the study population, inconsistent training content, and differences in training volume and intensity may have contributed to the findings. A retrospective analysis by Chu et al [54]. identified that the timing of acute care rehabilitation is a predictor of post-stroke walking capability. The FMA-LE was reported in eight studies included in this study, two of which showed that RAGT was not superior to conventional gait training. The study by Wall et al [34]. indicated that the recovery rate of independent walking at 6 months after stroke was higher in younger patients than in older patients, and the association with intervention was not significant. This suggests that while RAGT has potential benefits, its efficacy in improving specific functional mobility measures such as FMA-LE may be affected by the details such as demographic factors. Furthermore, subgroup analysis in this study found that interventions lasting around four weeks showed the most pronounced effects in FMA-LE scores. However, these results still require further validation from higher-quality clinical research.
Effect of RAGT on balance function in subacute stroke patients
Meta-analysis revealed a significant difference in BBS scores between the two groups, with RAGT effectively improving the balance function of patients with subacute stroke [MD = 4.55, 95%CI (3.00, 6.11), P < 0.001]. Similarly, a meta-analysis by Wang et al [18], which included 13 RCTs, concluded that RAGT was beneficial in improving the balance function of patients. Furthermore, A scoped review [55] summarized seven categories of balance rehabilitation interventions in which RAGT can significantly improve trunk control and balance aspects in stroke patients. Baronchelli et al [56] showed inconsistent results, which may be due to the fact that their study population was primarily composed of patients with chronic stroke, and the study only included RCTs that utilized the Lokomat robot equipment for RAGT interventions. A retrospective cohort study [57] showed that recovery of balance during inpatient rehabilitation for subacute stroke was strongly associated with gait achievement without physical assistance at discharge. Patients with subacute stroke experience changes in muscle mass, affecting their balance and lower extremity function [58] Robotic devices can assist patients to complete high-intensity and repetitive gait training tasks and also experience vestibular and proprioceptive stimulation during training, which can improve neuroplasticity and functional recovery of patients [59] Therefore, RAGT is an effective rehabilitation method for patients with balance dysfunction.
Effects of RAGT on walking ability and endurance in subacute stroke patients
The results of the meta-analysis demonstrated that RAGT compared with the CGT can effectively improve patients with subacute stroke of FAC, TUG, 6 MWT, improve the walking ability of patients and endurance. This result is consistent with the results of a meta-analysis of chronic stroke patients conducted by Yang et al [60]. which highlighted that RAGT had a better effect on gait performance and physical endurance than the control group. Postol et al [61]. investigated the impact of lower extremity robotic exoskeletons on the 6MWT and TUG test in patients with acquired brain injuries, noting improvements not attributed to traditional gait interventions. However, their analysis was based on a limited set of five studies, not all focused on stroke-induced cerebral apoplexy. Yu et al [62]. matched two randomized controlled trials and found that there was no difference in the improvement of walking ability between high-intensity and low-intensity RAGT in patients over three months after stroke. This indicated that there may be no difference in the number of leg movement repetitions between the two groups within the same intervention time, which could imply the potential for a reduced gait training period. Nevertheless, because the study by Yu et al. was not a prospective study and the inclusion criteria of the two matched randomized controlled trials were also different, there was a certain deviation. Subgroup analysis within our study found that the best improvement in FAC scores was achieved when the intervention lasting for four weeks. The number of studies in the other two subgroups was small, necessitating further research to explore the optimal duration of robot-assisted gait intervention.
While innovative, the utilization of robotic equipment in rehabilitation is often challenged by its considerable size, complexity, high costs, and the requirement for multiple attendants during operation [53]. There is growing attention on the design of the robot, such as Wu et al [59]. designed a new type of 9 degrees of freedom redundant rehabilitation training robot compared with exoskeleton robots. This robot has the characteristics of lower cost and higher stability and can realize simulating multiple body movements more efficiently. The design incorporates a series–parallel hybrid structure, combining the high load-bearing capacity typical of parallel robots with the added benefit of a parallel guide rail sliding block mechanism for efficient force transmission. This feature facilitates the easier achievement of high-speed movements, addressing some of the limitations of previous designs.
This study encompassed RCTs of RAGT using exoskeletons and end-effectors. Subgroup analysis revealed that exoskeleton-type robots showed superior performance on patient endurance levels measured by the 6MWT. Therefore, if conditions permit, selecting a robotic device that aligns with the specific needs and conditions of the patient could optimize rehabilitation outcomes.
Effects of RAGT on gait speed in subacute stroke patients
The results of the meta-analysis revealed that RAGT could not effectively improve level of 10MWT in patients with subacute stroke compared with CGT, but the subgroup analysis found that the exoskeleton type robot was more effective in improving the walking speed than CGT. Nedergard et al [19]. analyzed the effect of RAGT on objective biomechanical measurements of human gait after stroke and found that RAGT did not have a significant effect compared with non-RAGT treatment, which may be related to the small number of included studies and the higher risk of bias. Similarly, the results of a systematic review [60] also showed that there was no statistically significant difference between the RAGT group and the control group in the 10MWT.
The relationship between leg muscle strength and walking speed is a critical factor in this context [32]. This study included in the two studies show that in the control group at baseline lower limb muscle strength higher than that of intervention group. The final results showed that the intervention group had greater improvement in gait speed, which has certain clinical significance [32, 33]. The minimal clinically important differences (MCID) can be used to interpret the clinical significance of clinical trial results [63]. Using MCID, researchers can judge the substantial improvement of patients' condition after treatment. According to a previous study, the MCID of 10MWT was 0.13 m/s [64]. The findings from the subgroup analysis of this study reveal that the exoskeleton-type robots have demonstrated a significant MD of 0.16 m/s in the 10MWT, surpassing the threshold of the MCID. This outcome underscores the clinical relevance of exoskeleton-type robots in enhancing the gait velocity of individuals recovering from subacute stroke conditions. Xie et al [65]. conducted soft robot exoskeleton intervention on stroke patients and found that the soft robot exoskeleton group was better than the conventional training group in all clinical scores, with the 10MWT and 6MWT values exceeding the MCID.
The meta-analysis of Hsu et al [66]. on the effect of wearable exoskeleton on gait after stroke showed that the exoskeleton training group was superior in gait speed and achieved the MCID. However, their subgroup analysis found that this conclusion was only applicable to chronic stroke patients, and no meaningful results were observed in subacute stroke patients. This differentiation may be explained that the use of external assistance might have an inhibitory effect on individual differences, slowing down the walking speed of patients with stronger walking ability and accelerating it for those with weaker ability. A systematic review [67] of the effects of soft robotic outerwear on the walking ability of stroke patients showed that the included studies all found an improvement in walking speed. Therefore, improvements in walking speed may be related to the characteristics of the participants or the type of robot.
Robot-assisted technology represents a significant advancement in rehabilitation, which can not only improve patients' lower extremity function through gait training but also enhance extremity function through other training methods. For instance, Li et al [68]. performed exoskeleton-assisted sit-to-stand training in patients with subacute stroke and found that this training method could improve lower extremity function after stroke by inducing changes in muscle synergy. Furthermore, robot-assisted technology allows for the customization of device parameters based on the patient’s specific medical condition and muscle status, enhancing the personalization of rehabilitation efforts [69]. However, this customization also causes heterogeneity among various studies, and there is no consensus on the best intervention plan for RAGT. The results of an assessor-blinded RCT conducted by Talat et al [70]. showed that an additional three hours of gait training therapy per week during hospitalization for acute stroke achieved rehabilitation goals and was well-tolerated by patients. However, the sample size of this study was small, and more research is needed to explore the optimal intervention dose of RAGT. Zhang et al [71]. 's network meta-analysis found that combination of robot-assisted training with virtual reality yielded the best intervention for improve BBS and 10MWT scores. Therefore, RAGT combined with CGT or other rehabilitation techniques can be considered to enhance the rehabilitation effect when performing interventions for patients.
Limitations
This study acknowledges certain limitations that must be considered. Firstly, due to the use of the risk assessment tool RoB2 for strict quality evaluation in this study, only three studies were identified as low risk, which limits the robustness of our conclusions. Secondly, this study found that the improvement of FMA-LE and FAC scores effect was greatest when the intervention lasted for four weeks, but the specific training duration per week was varied, and this result also needs to be verified. Thirdly, this study did not analyze the follow-up data of the patients, and it is possible that the effect of the robotic intervention is not immediate, which may influence the conclusions of this study. Future research directions could include exploring optimal parameter settings for robotic devices, investigating the intensity of training, and assessing the efficacy of combining RAGT with other treatment modalities. These endeavors will contribute to further advancements in the field of stroke rehabilitation.
Conclusion
This study highlights that Robot-assisted gait training exhibits promising potential for enhancing lower extremity function, balance function, walking ability, and endurance in patients with subacute stroke. However, the quality of evidence for improvements in gait speed remains low.
Supplementary Information
Acknowledgements
The authors would like to acknowledge all the participants of the study.
Author contributions
MMH: Conceptualization; Data Curation; Formal Analysis; Methodology; Software; Investigation; Validation; Visualization; Writing – Original Draft Preparation. SW: Conceptualization; Data Curation; Formal Analysis; Methodology; Software; Investigation; Validation; Visualization; Writing – Original Draft Preparation. CQW: Resources; Validation; Writing – Review & Editing. KPL: Resources; Validation; Writing – Review & Editing. ZHG: Resources; Funding Acquisition; Validation. GHX: Investigation; Methodology; Project Administration; Supervision; Validation; Funding Acquisition; Writing – Review & Editing. LD: Investigation; Methodology; Project Administration; Supervision; Validation; Funding Acquisition; Writing – Review & Editing. MMH and SW made equal contributions to this manuscript.
Funding
This research was funded by Shanghai University of Traditional Chinese Medicine [KECJ2024015]; Shanghai Clinical Research Center for Rehabilitation Medicine [21MC1930200]; Rehabilitation Medicine Research Center of Huadong Hospital [LCZX2206] and National Natural Science Foundation of China [72104145].
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All the authors approved the publication.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Miao-miao Hu and Shan Wang made equal contributions to this manuscript.
Contributor Information
Guo-hui Xu, Email: pudongxgh@163.com.
Lu Dong, Email: donglux@shutcm.edu.cn.
References
- 1.Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Collaborators GBDS. Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the global burden of disease Study 2019. Lancet Neurol. 2021;20(10):795–820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hornby TG, Reisman DS, Ward IG, Scheets PL, Miller A, Haddad D, et al. Clinical practice guideline to improve locomotor function following chronic stroke, incomplete spinal cord injury, and brain injury. J Neurol Phys Ther. 2020;44(1):49–100. [DOI] [PubMed] [Google Scholar]
- 4.Elameer M, Lumley H, Moore SA, Marshall K, Alton A, Smith FE, et al. A prospective study of MRI biomarkers in the brain and lower limb muscles for prediction of lower limb motor recovery following stroke. Front Neurol. 2023;14:1229681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2016;47(6):e98–169. [DOI] [PubMed] [Google Scholar]
- 6.Kwakkel G, Stinear C, Essers B, Munoz-Novoa M, Branscheidt M, Cabanas-Valdés R, et al. Motor rehabilitation after stroke: european stroke organisation (ESO) consensus-based definition and guiding framework. Eur Stroke J. 2023;8(4):880–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Xue X, Yang X, Deng Z. Efficacy of rehabilitation robot-assisted gait training on lower extremity dyskinesia in patients with Parkinson’s disease: A systematic review and meta-analysis. Ageing Res Rev. 2023;85: 101837. [DOI] [PubMed] [Google Scholar]
- 8.Chang WH, Kim YH. Robot-assisted therapy in stroke rehabilitation. J Stroke. 2013;15(3):174–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Morone G, Paolucci S, Cherubini A, De Angelis D, Venturiero V, Coiro P, et al. Robot-assisted gait training for stroke patients: current state of the art and perspectives of robotics. Neuropsychiatr Dis Treat. 2017;13:1303–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kuo CY, Liu CW, Lai CH, Kang JH, Tseng SH, Su EC. Prediction of robotic neurorehabilitation functional ambulatory outcome in patients with neurological disorders. J Neuroeng Rehabil. 2021;18(1):174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Perju-Dumbrava L, Barsan M, Leucuta DC, Popa LC, Pop C, Tohanean N, et al. Artificial intelligence applications and robotic systems in Parkinson’s disease (Review). Exp Ther Med. 2022;23(2):153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Meng G, Ma X, Chen P, Xu S, Li M, Zhao Y, et al. Effect of early integrated robot-assisted gait training on motor and balance in patients with acute ischemic stroke: a single-blinded randomized controlled trial. Ther Adv Neurol Disord. 2022;15:17562864221123196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yoo HJ, Bae CR, Jeong H, Ko MH, Kang YK, Pyun SB. Clinical efficacy of overground powered exoskeleton for gait training in patients with subacute stroke: a randomized controlled pilot trial. Medicine (Baltimore). 2023;102(4): e32761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Giovannini S, Iacovelli C, Brau F, Loreti C, Fusco A, Caliandro P, et al. RObotic-assisted rehabilitation for balance and gait in Stroke patients (ROAR-S): study protocol for a preliminary randomized controlled trial. Trials. 2022;23(1):872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nam YG, Lee JW, Park JW, Lee HJ, Nam KY, Park JH, et al. Effects of electromechanical exoskeleton-assisted gait training on walking ability of stroke patients: a randomized controlled trial. Arch Phys Med Rehabil. 2019;100(1):26–31. [DOI] [PubMed] [Google Scholar]
- 16.Yu D, Yang Z, Lei L, Chaoming N, Ming W. Robot-assisted gait training plan for patients in poststroke recovery period: a single blind randomized controlled trial. Biomed Res Int. 2021;2021:5820304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Calafiore D, Negrini F, Tottoli N, Ferraro F, Ozyemisci-Taskiran O, de Sire A. Efficacy of robotic exoskeleton for gait rehabilitation in patients with subacute stroke: a systematic review. Eur J Phys Rehabil Med. 2022;58(1):1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wang L, Zheng Y, Dang Y, Teng M, Zhang X, Cheng Y, et al. Effects of robot-assisted training on balance function in patients with stroke: A systematic review and meta-analysis. J Rehabil Med. 2021;53:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Nedergård H, Arumugam A, Sandlund M, Bråndal A, Häger CK. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: a systematic review and meta-analysis. J Neuroeng Rehabil. 2021;18(1):64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898. [DOI] [PubMed] [Google Scholar]
- 21.Bergmann J, Krewer C, Jahn K, Müller F. Robot-assisted gait training to reduce pusher behavior: a randomized controlled trial. Neurology. 2018;91(14):e1319–27. [DOI] [PubMed] [Google Scholar]
- 22.Chang WH, Kim MS, Huh JP, Lee PK, Kim YH. Effects of robot-assisted gait training on cardiopulmonary fitness in subacute stroke patients: a randomized controlled study. Neurorehabil Neural Repair. 2012;26(4):318–24. [DOI] [PubMed] [Google Scholar]
- 23.Chua J, Culpan J, Menon E. Efficacy of an electromechanical gait trainer poststroke in singapore: a randomized controlled trial. Arch Phys Med Rehabil. 2016;97(5):683–90. [DOI] [PubMed] [Google Scholar]
- 24.Lee YH, Ko LW, Hsu CY, Cheng YY. Therapeutic effects of robotic-exoskeleton-assisted gait rehabilitation and predictive factors of significant improvements in stroke patients: a randomized controlled trial. Bioengineering. 2023;10:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Li DX, Zha FB, Long JJ, Liu F, Cao J, Wang YL. Effect of robot assisted gait training on motor and walking function in patients with subacute stroke: a random controlled study. J Stroke Cerebrovasc Dis. 2021;30(7): 105807. [DOI] [PubMed] [Google Scholar]
- 26.Lin YN, Huang SW, Kuan YC, Chen HC, Jian WS, Lin LF. Hybrid robot-assisted gait training for motor function in subacute stroke: a single-blind randomized controlled trial. J Neuroeng Rehabil. 2022;19(1):99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Morone G, Bragoni M, Iosa M, De Angelis D, Venturiero V, Coiro P, et al. Who may benefit from robotic-assisted gait training? A randomized clinical trial in patients with subacute stroke. Neurorehabil Neural Repair. 2011;25(7):636–44. [DOI] [PubMed] [Google Scholar]
- 28.Morone G, Masiero S, Coiro P, De Angelis D, Venturiero V, Paolucci S, et al. Clinical features of patients who might benefit more from walking robotic training. Restor Neurol Neurosci. 2018;36(2):293–9. [DOI] [PubMed] [Google Scholar]
- 29.Ng MF, Tong RK, Li LS. A pilot study of randomized clinical controlled trial of gait training in subacute stroke patients with partial body-weight support electromechanical gait trainer and functional electrical stimulation: six-month follow-up. Stroke. 2008;39(1):154–60. [DOI] [PubMed] [Google Scholar]
- 30.Park C, Oh-Park M, Dohle C, Bialek A, Friel K, Edwards D, et al. Effects of innovative hip-knee-ankle interlimb coordinated robot training on ambulation, cardiopulmonary function, depression, and fall confidence in acute hemiplegia. NeuroRehabilitation. 2020;46(4):577–87. [DOI] [PubMed] [Google Scholar]
- 31.Pournajaf S, Calabrò RS, Naro A, Goffredo M, Aprile I, Tamburella F, et al. Robotic versus conventional overground gait training in subacute stroke survivors a multicenter controlled clinical trial. J Clin Med. 2023;12:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Tanaka N, Yano H, Ebata Y, Ebihara K. Influence of robot-assisted gait training on lower-limb muscle activity in patients with stroke: comparison with conventional gait training. Ann Rehabil Med. 2023;47(3):205–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Taveggia G, Borboni A, Mulé C, Villafañe JH, Negrini S. Conflicting results of robot-assisted versus usual gait training during postacute rehabilitation of stroke patients: a randomized clinical trial. Int J Rehabil Res. 2016;39(1):29–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wall A, Borg J, Vreede K, Palmcrantz S. A randomized controlled study incorporating an electromechanical gait machine, the Hybrid Assistive Limb, in gait training of patients with severe limitations in walking in the subacute phase after stroke. PLoS ONE. 2020;15(2): e0229707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Yun N, Joo MC, Kim SC, Kim MS. Robot-assisted gait training effectively improved lateropulsion in subacute stroke patients: a single-blinded randomized controlled trial. Eur J Phys Rehabil Med. 2018;54(6):827–36. [DOI] [PubMed] [Google Scholar]
- 36.Thimabut N, Yotnuengnit P, Charoenlimprasert J, Sillapachai T, Hirano S, Saitoh E, et al. Effects of the robot-assisted gait training device plus physiotherapy in improving ambulatory functions in patients with subacute stroke with hemiplegia: an assessor-blinded, randomized controlled trial. Arch Phys Med Rehabil. 2022;103(5):843–50. [DOI] [PubMed] [Google Scholar]
- 37.Watanabe H, Tanaka N, Inuta T, Saitou H, Yanagi H. Locomotion improvement using a hybrid assistive limb in recovery phase stroke patients: a randomized controlled pilot study. Arch Phys Med Rehabil. 2014;95(11):2006–12. [DOI] [PubMed] [Google Scholar]
- 38.Tong RK, Ng MF, Li LS. Effectiveness of gait training using an electromechanical gait trainer, with and without functional electric stimulation, in subacute stroke: a randomized controlled trial. Arch Phys Med Rehabil. 2006;87(10):1298–304. [DOI] [PubMed] [Google Scholar]
- 39.Hu C, Wang X, Pan T. Effect of acupuncture combined with lower limb gait rehabilitation robot on improving walking function in stroke patients with hemiplegia. NeuroRehabilitation. 2024;54(2):309–17. [DOI] [PubMed] [Google Scholar]
- 40.Tian H, Yang Y, Zhang H, Zhao W, Zhou J, Tian J, et al. Efficacy of Daoyin combined with lower limb robot as a comprehensive rehabilitation intervention for stroke patients: a randomized controlled trial. J Tradit Chin Med. 2024;44(3):530–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lee J, Kim DY, Lee SH, Kim JH, Kim DY, Lim K-B, et al. End-effector lower limb robot-assisted gait training effects in subacute stroke patients: a randomized controlled pilot trial. Medicine. 2023;102:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kóra S, Bíró A, Prontvai N, Androsics M, Drotár I, Prukner P, et al. Investigation of the effectiveness of the robotic restore soft exoskeleton in the development of early mobilization, walking, and coordination of stroke patients: a randomized clinical trial. Robotics. 2024;13:3. [Google Scholar]
- 43.Castelli L, Iacovelli C, Loreti C, Malizia AM, Barone Ricciardelli I, Tomaino A, et al. Robotic-assisted rehabilitation for balance in stroke patients (ROAR-S): effects of cognitive, motor and functional outcomes. Eur Rev Med Pharmacol Sci. 2023;27(17):8198–211. [DOI] [PubMed] [Google Scholar]
- 44.Roelofs JMB, Zandvliet SB, Schut IM, Huisinga ACM, Schouten AC, Hendricks HT, et al. Mild stroke, serious problems: limitations in balance and gait capacity and the impact on fall rate, and physical activity. Neurorehabil Neural Repair. 2023;37(11–12):786–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Goncalves S, Le Bourvellec M, Mandigout S, Duclos NC. Impact of active physiotherapy on physical activity level in stroke survivors: a systematic review and meta-analysis. Stroke. 2023;54(12):3097–106. [DOI] [PubMed] [Google Scholar]
- 46.O’Dell MW, Jaywant A, Frantz M, Patel R, Kwong E, Wen K, et al. Changes in the activity measure for post-acute care domains in persons with stroke during the first year after discharge from inpatient rehabilitation. Arch Phys Med Rehabil. 2021;102(4):645–55. [DOI] [PubMed] [Google Scholar]
- 47.Esquenazi A, Packel A. Robotic-assisted gait training and restoration. Am J Phys Med Rehabil. 2012;91:11. [DOI] [PubMed] [Google Scholar]
- 48.Teasell R, Salbach NM, Foley N, Mountain A, Cameron JI, Jong A, et al. Canadian stroke best practice recommendations: rehabilitation, recovery, and community participation following stroke part one rehabilitation and recovery following stroke. Int J Stroke. 2020;15(7):763–88. [DOI] [PubMed] [Google Scholar]
- 49.Gunduz ME, Bucak B, Keser Z. Advances in stroke neurorehabilitation. J Clin Med. 2023;12:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Nedergard H, Arumugam A, Sandlund M, Brandal A, Hager CK. Effect of robotic-assisted gait training on objective biomechanical measures of gait in persons post-stroke: a systematic review and meta-analysis. J Neuroeng Rehabil. 2021;18(1):64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Tedla JS, Dixit S, Gular K, Abohashrh M. Robotic-assisted gait training effect on function and gait speed in subacute and chronic stroke population: a systematic review and meta-analysis of randomized controlled trials. Eur Neurol. 2019;81(3–4):103–11. [DOI] [PubMed] [Google Scholar]
- 52.Schröder J, Saeys W, Embrechts E, Hallemans A, Yperzeele L, Truijen S, et al. Recovery of quiet standing balance and lower limb motor impairment early poststroke: how are they related? Neurorehabil Neural Repair. 2023;37(8):530–44. [DOI] [PubMed] [Google Scholar]
- 53.Stramel DM, Winterbottom L, Stein J, Agrawal SK. Overground robotic gait trainer mTPAD improves gait symmetry and weight bearing in stroke survivors. Bioengineering. 2023;10:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Chu CL, Lee TH, Chen YP, Ro LS, Hsu JL, Chu YC, et al. Recovery of walking ability in stroke patients through postacute care rehabilitation. Biomed J. 2023;46(4): 100550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Saraiva J, Rosa G, Fernandes S, Fernandes JB. Current trends in balance rehabilitation for stroke survivors: a scoping review of experimental studies. Int J Environ Res Public Health. 2023;20:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Baronchelli F, Zucchella C, Serrao M, Intiso D, Bartolo M. The effect of robotic assisted gait training with lokomat® on balance control after stroke: systematic review and meta-analysis. Front Neurol. 2021;12: 661815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Gath CF, Gianella MG, Bonamico L, Russo MJ. Association between balance recovery during inpatient rehabilitation and gait without physical assistance in severe subacute post-stroke patients. Physiother Res Int. 2023;28(4):e2029. [DOI] [PubMed] [Google Scholar]
- 58.Kim DH, Cho ES, Park YS, Chang HJ, Park JG, Kim JY, et al. Changes in lower extremity muscle quantity and quality in patients with subacute stroke. Ann Rehabil Med. 2023;47:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Wu J, Liu Y, Zhao J, Jia Z. Research on a new rehabilitation robot for balance disorders. IEEE Trans Neural Syst Rehabil Eng. 2023;31:3927–36. [DOI] [PubMed] [Google Scholar]
- 60.Yang J, Gong Y, Yu L, Peng L, Cui Y, Huang H. Effect of exoskeleton robot-assisted training on gait function in chronic stroke survivors: a systematic review of randomised controlled trials. BMJ Open. 2023;13(9): e074481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Postol N, Marquez J, Spartalis S, Bivard A, Spratt NJ. Do powered over-ground lower limb robotic exoskeletons affect outcomes in the rehabilitation of people with acquired brain injury? Disabil Rehabil Assist Technol. 2019;14(8):764–75. [DOI] [PubMed] [Google Scholar]
- 62.Yu CS, Nam YG, Kwon BS. Comparison of high-intensive and low-intensive electromechanical-assisted gait training by Exowalk® in patients over 3-month post-stroke. BMC Sports Sci Med Rehabil. 2022;14(1):126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Tilson JK, Sullivan KJ, Cen SY, Rose DK, Koradia CH, Azen SP, et al. Meaningful gait speed improvement during the first 60 days poststroke: minimal clinically important difference. Phys Ther. 2010;90(2):196–208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Bohannon RW, Andrews AW, Glenney SS. Minimal clinically important difference for comfortable speed as a measure of gait performance in patients undergoing inpatient rehabilitation after stroke. J Phys Ther Sci. 2013;25(10):1223–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Xie R, Zhang Y, Jin H, Yang F, Feng Y, Pan Y. Effects of soft robotic exoskeleton for gait training on clinical and biomechanical gait outcomes in patients with sub-acute stroke: a randomized controlled pilot study. Front Neurol. 2023;14:1296102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hsu TH, Tsai CL, Chi JY, Hsu CY, Lin YN. Effect of wearable exoskeleton on post-stroke gait: a systematic review and meta-analysis. Ann Phys Rehabil Med. 2023;66(1): 101674. [DOI] [PubMed] [Google Scholar]
- 67.Sloot LH, Baker LM, Bae J, Porciuncula F, Clément BF, Siviy C, et al. Effects of a soft robotic exosuit on the quality and speed of overground walking depends on walking ability after stroke. J Neuroeng Rehabil. 2023;20(1):113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Li YA, Chen ZJ, He C, Wei XP, Xia N, Gu MH, et al. Exoskeleton-assisted sit-to-stand training improves lower-limb function through modifications of muscle synergies in subacute stroke survivors. IEEE Trans Neural Syst Rehabil Eng. 2023;31:3095–105. [DOI] [PubMed] [Google Scholar]
- 69.Çalıkuşu İ, Uzunhisarcıklı E, Fidan U, Çetinkaya MB. Analysing the effect of robotic gait on lower extremity muscles and classification by using deep learning. Comput Methods Biomech Biomed Engin. 2022;25(12):1350–69. [DOI] [PubMed] [Google Scholar]
- 70.Talaty M, Esquenazi A. Feasibility and outcomes of supplemental gait training by robotic and conventional means in acute stroke rehabilitation. J Neuroeng Rehabil. 2023;20(1):134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Zhang B, Wong KP, Kang R, Fu S, Qin J, Xiao Q. Efficacy of robot-assisted and virtual reality interventions on balance, gait, and daily function in patients with stroke: a systematic review and network meta-analysis. Arch Phys Med Rehabil. 2023;104(10):1711–9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.