

Abstract
Objectives
The study aimed to investigate the correlation between medial tibial slope (MTS) and lateral tibial slope (LTS) on magnetic resonance imaging (MRI), MTS measured by different imaging, and the intra- and interobserver reliability of measurements between reviewers with gaps of experience over 10 years.
Patients and methods
This retrospective study included 97 patients (93 males, 4 females; mean age: 30.8±8.3 years; range, 17 to 49 years) with anterior cruciate ligament (ACL) injuries who subsequently underwent double-bundle ACL reconstruction by a single surgeon between January 2005 and December 2014. The MTS was measured on lateral knee radiographs, and MTS and LTS were measured on MRIs. Three different reviewers, including a postgraduate year doctor, an orthopedic resident, and an attending orthopedic surgeon, performed the measurements. Each reviewer measured the slope of the same image three times. The correlations of MTS on radiographs and MTS/LTS on MRIs were calculated. Intra- and interobserver reliability were evaluated.
Results
The average MTS and LTS measured on MRI were not significantly different (6.4° and 6.9°, respectively; p=0.268) and exhibited a moderate positive correlation (r=0.544, p<0.001). The average MTS on radiographs was significantly greater than that on MRI (10.5° and 6.4°, respectively; p<0.001) with a low positive correlation (r=0.480, p<0.001). The intraobserver reliability of the postgraduate year doctor, the orthopedic resident, and the attending orthopedic surgeon were moderate to excellent. The interobserver reliability of MTS on radiographs was excellent (intraclass correlation coefficient [ICC]=0.925; p<0.001). The interobserver reliability of MTS on MRI as well as LTS on MRI was good (ICC=0.755 and 820, respectively; all p values <0.001).
Conclusion
Average MTS and LTS measured on MRI in patients with ACL injury exhibited a moderate positive correlation. The average MTS measured on radiographs was significantly greater than that on MRI with a low positive correlation.
Keywords: Anterior cruciate ligament injury, correlation, lateral tibial slope, magnetic resonance imaging, medial tibial slope.
Introduction
A steep tibial slope has been reported to be a potential risk factor for primary anterior cruciate ligament (ACL) injury and ACL reconstruction (ACLR) failure.[1-10] However, high variability in tibial slope values is noted in measurements obtained by different methods, and consensus regarding the best measurement method of true tibial slope on medical imaging has not been achieved to date. A variety of methods for tibial slope measurement have been applied in different studies. Imaging modality is one of the variables. Plain radiography, computed tomography (CT), and magnetic resonance imaging (MRI) have been proposed to be reliable measuring tools, and an increasing number of measurement methods have been proposed.[11-18] Furthermore, within one type of imaging modality, different methods can be applied for the measurement of tibial slope. For example, on knee lateral radiographs and MRI, there were several different methods to define the tibial axis.[12,13,19] A previous study demonstrated a high degree of variability and inaccuracy between imaging modalities and different measurement methods for tibial slope, but the measured degree of tibial slopes was reliable when a single measurement method was employed, and most of the intraclass correlation coefficients (ICCs) of these studies were >0.80.[20] Therefore, although different results of tibial slope degree were obtained using different measurement methods, the reliability was good and repeatable within a single study using the same method.
Tibial slopes can be further divided into two major components: the medial tibial slope (MTS) and the lateral tibial slope (LTS). It has been demonstrated that MTS and LTS are independent risk factors for ACLR failure.[2,5] However, another study showed that LTS was a significant predictor for ACLR failure, while MTS was not.[21] The different findings of these studies might partly result from the different degrees of tibial slopes measured by different measurement methods. Therefore, the correlation between MTS and LTS within a single study using the same method to measure tibial slope could be important. A previous study reported a significant positive correlation between MTS and LTS measured on CT scans.[22] Nevertheless, in patients with suspected ACL injury, knee radiographs and MRI were more commonly performed than CT scans, mainly due to the higher radiation exposure of CT scans and the advantage of MRI in soft tissue evaluation. Therefore, the correlation between LTS and MTS on MRI in patients with ACL injury is worth investigating.
In addition, a previous study reported that the intra- and interobserver results of tibial slope measurement via a single method were reliable on both radiographs and MRI, showing the reproducibility of each measurement for tibial slope and reliability between different reviewers when a single measurement method is applied.[23] However, patients with knee pain with radiographs and MRI on file were included in the study, whereas patients with ACL pathologies and surgical candidates for ACLR were not an area of focus. In addition, the three reviewers in the study were two orthopedic residents (ORs) and an orthopedic fellow. The interobserver reliability between reviewers with a larger clinical experience gap was not investigated.
The purpose of this study was to investigate the correlation between MTS and LTS measured on radiographs and MRI in patients with ACL injury who subsequently underwent ACLR. The hypothesis was that positive correlations exist between the tibial slope measured by radiographs and MRI and between MTS and LTS in patients with ACL injuries indicated for ACLR. Accordingly, whether the high MTS of a patient could predict the high LTS in the same modality was investigated. In addition, the reliability of the same measurement method between reviewers with a gap greater than 10 years in clinical experience was also investigated.
Patients and Methods
A total of 154 patients who underwent double-bundle ACLR at a single medical center by a single surgeon from January 2005 to December 2014 were reviewed in this study. All patients received complete image analysis, including knee lateral X-rays and MRI. Patients who underwent previous knee surgery and those with inadequate radiographs and MRI images on file were excluded. Adequate radiographs were defined using factors previously described by Jahn et al.,[23] including the posterior aspects of the femoral condyles being within 5 mm of distance, clear patellofemoral joint, and clear tibial femoral joint on the lateral radiograph. In addition, the MRI was considered to be adequate if both sagittal and axial tibia slices on file with sufficient length below tibial tuberosity.[23] Finally, a total of 97 patients (93 males, 4 females; mean age: 30.8±8.3 years; range, 17 to 49 years) were included, and their radiographs and MRI were reviewed to measure the tibial slopes. Bisicchia et al.[24] demonstrated that differences in posterior tibial slope exist between different ethnic groups. Therefore, all 97 patients were Asian in this study.
The radiographs and MRI scans were viewed, and the slopes were measured using imaging software (the picture archiving and communicating system). The MTS on lateral knee radiographs and MRI scans and the LTS on MRI scans were measured by three reviewers, including a postgraduate year (PGY) doctor, an OR, and an attending orthopedic surgeon (visiting staff; VS). Each reviewer used radiographs and MRI to measure the MTS and LTS all three times. The methods of MTS and LTS measurement were mainly based on those described by Hashemi et al.[25] and Jahn et al.,[23] with some modifications.
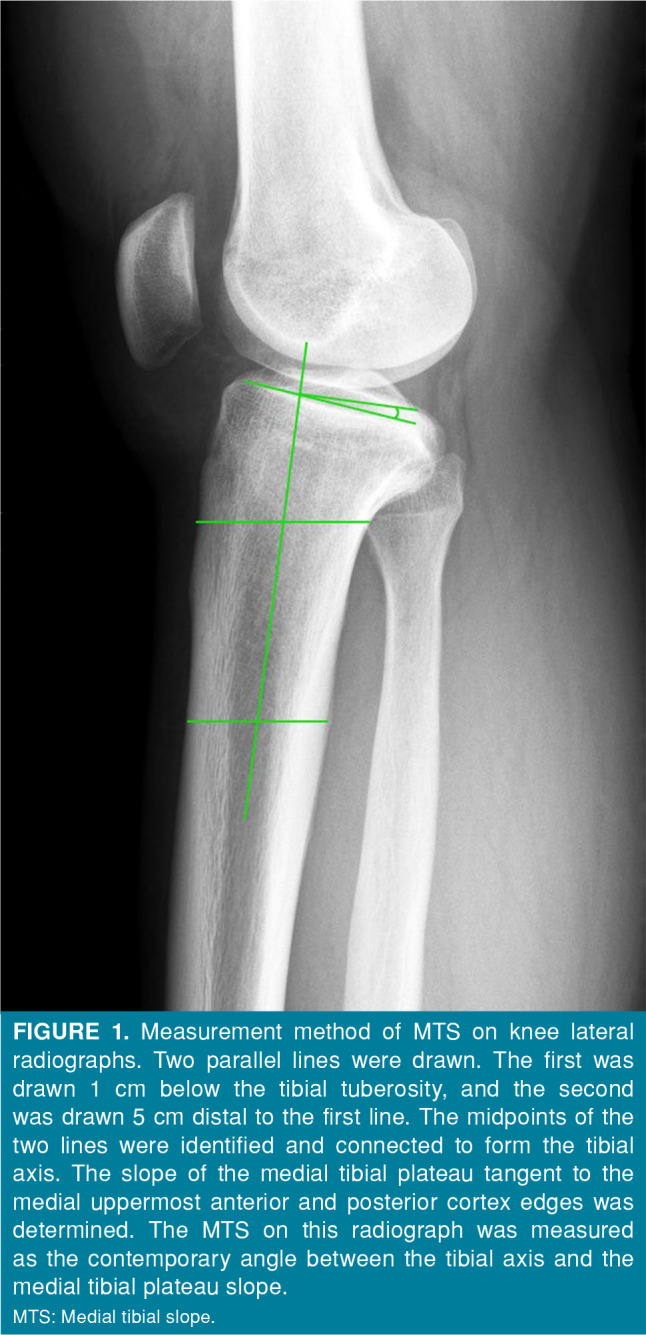
The measurement of the tibial slope involved the generation of a line on the tibial axis and another line tangent to the tibial plateau, and the tibial slope was defined as the contemporary angle of these two lines. On lateral knee radiographs, we measured MTS only because the lateral tibial plateau was relatively unclear with poorly defined borders on radiographs. The tibial axis was defined as a line connected by two points on radiographs. One point was the midpoint of the anterior and posterior cortex of the tibia at a level of 1 cm below the tibial tuberosity, and the other point was the midpoint of the anterior and posterior cortex of the tibia at a level of 5 cm distal to the first point. The line tangent to the medial tibial plateau connecting the uppermost anterior and posterior cortex edges was drawn. The MTS was defined as the contemporary angles of the angle between the tibial axis line and the line tangent to the medial tibial plateau (Figure 1).
Figure 1. Measurement method of MTS on knee lateral radiographs. Two parallel lines were drawn. The first was drawn 1 cm below the tibial tuberosity, and the second was drawn 5 cm distal to the first line. The midpoints of the two lines were identified and connected to form the tibial axis. The slope of the medial tibial plateau tangent to the medial uppermost anterior and posterior cortex edges was determined. The MTS on this radiograph was measured as the contemporary angle between the tibial axis and the medial tibial plateau slope.<br> MTS: Medial tibial slope.
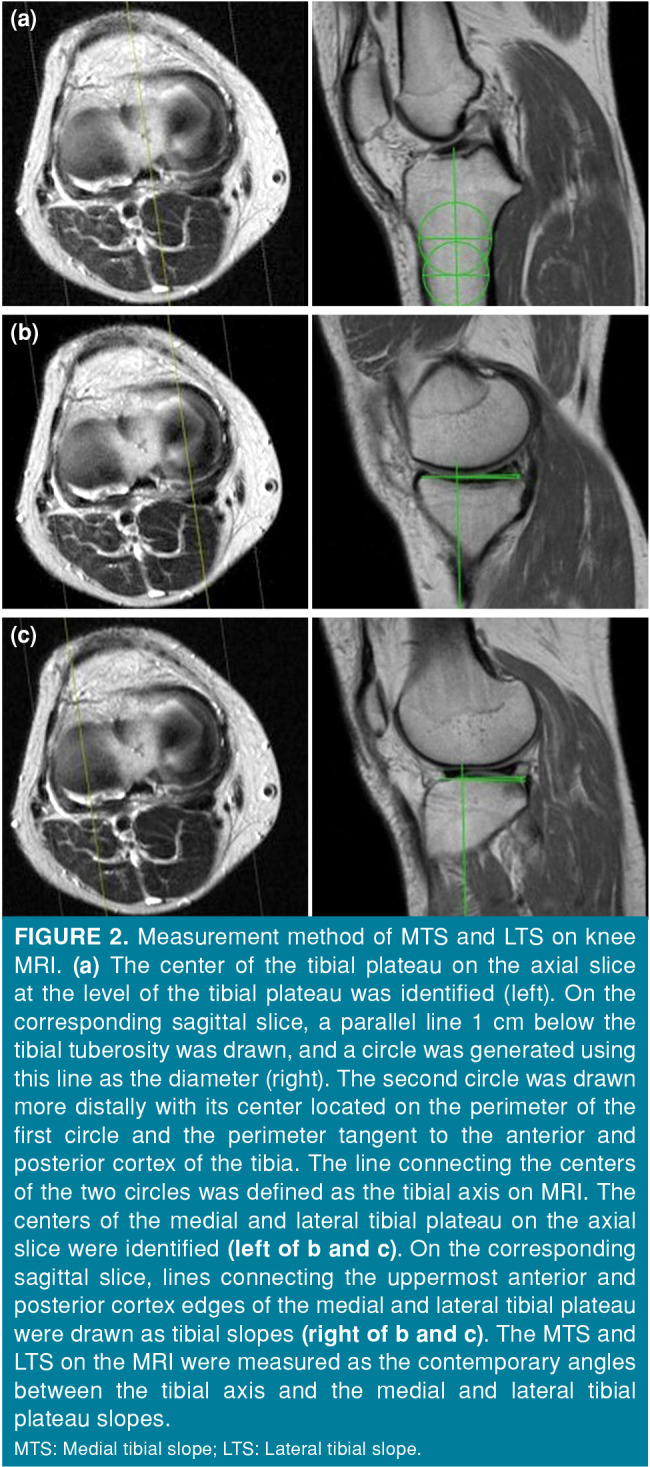
On MRI, both MTS and LTS were measured on proton density images. The method described by Hudek et al.[26] has been demonstrated to be the most repeatable method to measure sagittal tibial slopes on MRI and is independent of proximal tibial length.[12] Since most MRI scans of the knee presented the proximal tibia that was not long enough to place the second point at the level of 6 cm distal to the tibial tuberosity, a two-circle method modified by Hudek et al.[26] was applied to define the tibial axis on MRI in our study. The two-circle method in this study was modified to be similar to the method of measurement on radiographs adopted in our study. First, to define the tibial axis, an axial slice of the tibial plateau was referenced. After the reference line of the sagittal slice was placed on the center of the tibial plateau on the axial slice, that sagittal slice was used to determine the tibial axis. A circle was drawn with its perimeter tangent to the anterior and posterior tibial cortex with the center of the circle at the level of 1 cm below the tibial tuberosity. Afterward, the second circle, of which the perimeter was also tangent to the anterior and posterior tibial cortices, was drawn more distally with its center on the perimeter of the first circle. A line connected by these two centers of the circles was defined as the tibial axis on MRI. Next, we referred to the axial slice and scrolled the reference line of the sagittal slice to the middle of the medial and lateral plateau. Afterward, a line tangent to the articular surface of both the medial and lateral tibial plateau was created on the sagittal slice. The contemporary angles of the angles between the tibial axis and the line tangent to the medial and lateral tibial plateau were defined as the MTS and LTS on MRI scans (Figure 2).
Figure 2. Measurement method of MTS and LTS on knee MRI. (a) The center of the tibial plateau on the axial slice at the level of the tibial plateau was identified (left). On the corresponding sagittal slice, a parallel line 1 cm below the tibial tuberosity was drawn, and a circle was generated using this line as the diameter (right). The second circle was drawn more distally with its center located on the perimeter of the first circle and the perimeter tangent to the anterior and posterior cortex of the tibia. The line connecting the centers of the two circles was defined as the tibial axis on MRI. The centers of the medial and lateral tibial plateau on the axial slice were identified (left of b and c). On the corresponding sagittal slice, lines connecting the uppermost anterior and posterior cortex edges of the medial and lateral tibial plateau were drawn as tibial slopes (right of b and c). The MTS and LTS on the MRI were measured as the contemporary angles between the tibial axis and the medial and lateral tibial plateau slopes.<br> MTS: Medial tibial slope; LTS: Lateral tibial slope.
Statistical analysis
To plan the number of cases, we performed a power analysis by G*Power version 3.1.9.7 software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany), with an effect size of 0.59, according to a previous study by Meier et al.[22] A sample of at least 14 patients was required to reach a power over 80%.
Data were analyzed using Excel (Microsoft Corp., Redmond, WA, USA) and IBM SPSS version 22.0 software (IBM Corp., Armonk, NY, USA). The two-sample t-test was used to compare LTS and MTS on MRI. The paired t-test was used to compare measurements of MTS on radiographs and MRI. Pearson correlation coefficients were calculated to determine the relation between measurements on radiographs versus MRI scans, as well as the correlation between LTS and MTS measured by MRI. Intraclass correlation coefficients were used to evaluate the intra- and interobserver reliability of measurements within each imaging modality. A p-value <0.05 was defined as statistically significant. Based on the 95% confidence interval of the ICC estimate, ICC values <0.5, between 0.5-0.75, between 0.75-0.9, and >0.90 indicated poor, moderate, good, and excellent reliability, respectively.[27] Correlation was classified into six levels via the Pearson correlation coefficient: perfect (r=±1), very high (±0.9≤r<[DY3]±1), high (±0.7≤r<±0.9), moderate (±0.5≤r<±7), low (±0.3≤r<±0.5), or negligible (r<±0.3).[28]
Results
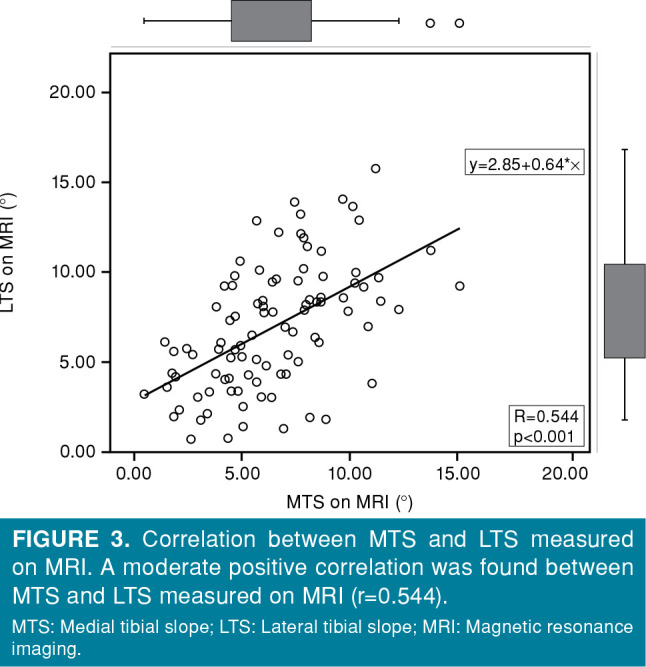
The demographic data are shown in Table I. The MTS (6.4°) and LTS (6.9°) measured on MRI were not different (p=0.268; Table II), and a moderate positive correlation was found (r=0.544, p<0.001; Figure 3).
Table 1. Demographic parameters (n=97).
| n | Mean±SD | |
| Age (year) | 30.8±8.3 | |
| Sex | ||
| Male | 93 | |
| Female | 4 | |
| Body mass index (kg/m2) | 26.6±4.35 | |
| SD: Standard deviation. | ||
Table 2. Comparison between average MTS and LTS measured on MRI.
| Mean±SD | p | |
| MTS on MRI (°) | 6.4±2.97 | 0.268 |
| LTS on MRI (°) | 6.9±3.47 | |
| MTS: Medial tibial slope; LTS: Lateral tibial slope; MRI: Magnetic resonance imaging; SD: Standard deviation. | ||
Figure 3. Correlation between MTS and LTS measured on MRI. A moderate positive correlation was found between MTS and LTS measured on MRI (r=0.544).<br> MTS: Medial tibial slope; LTS: Lateral tibial slope; MRI: Magnetic resonance imaging.
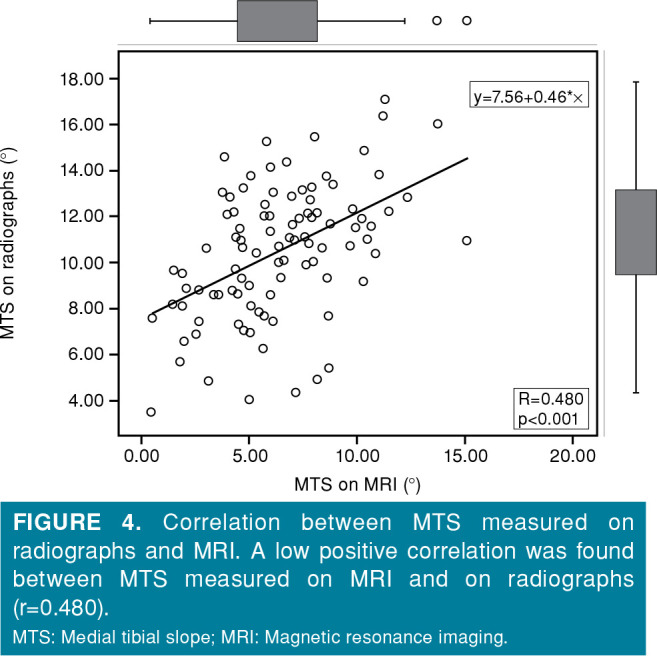
The MTS on radiographs (10.5°) was significantly larger than the MTS on MRI (6.4°) (p<0.001; Table III), with a low positive correlation (r=0.480, p<0.001; Figure 4).
Table 3. Comparison between average MTS measured on MRI and radiographs.
| Mean±SD | p | |
| MTS on MRI (°) | 6.4±2.97 | <0.001 |
| MTS on radiographs (°) | 10.5±2.85 | |
| MTS: Medial tibial slope; MRI: Magnetic resonance imaging; SD: Standard deviation. | ||
Figure 4. Correlation between MTS measured on radiographs and MRI. A low positive correlation was found between MTS measured on MRI and on radiographs (r=0.480).<br> MTS: Medial tibial slope; MRI: Magnetic resonance imaging.
Intraobserver measurement of MTS on radiographs showed good to excellent agreement for the three reviewers (ICC=0.914 for PGY, 0.915 for OR, 0.855 for VS; all p values <0.001). Intraobserver measurement of MTS on MRI showed moderate, good, and excellent agreement for the three reviewers (ICC=0.864 for PGY, 0.712 for OR, 0.926 for VS; all p values <0.001). Intraobserver measurement of LTS on MRI showed good to excellent agreement among the three reviewers (ICC=0.866 for PGY, 0.915 for OR, 0.858 for VS; all p values <0.001; Table IV).
Table 4. Intraobserver reliability of tibial slope measurements made by the three reviewers.
| Intraobserver reliability of tibial slope measurements made by a postgraduate year doctor | |||
| ICC | 95% CI | p | |
| MTS on radiographs | 0.914 | 0.883-0.939 | <0.001 |
| MTS on MRI | 0.864 | 0.817-0.903 | <0.001 |
| LTS on MRI | 0.866 | 0.819-0.904 | <0.001 |
| Intraobserver reliability of tibial slope measurements made by an orthopedic resident | |||
| ICC | 95% CI | p | |
| MTS on radiographs | 0.915 | 0.776-0.916 | <0.001 |
| MTS on MRI | 0.712 | 0.399-0.908 | <0.001 |
| LTS on MRI | 0.915 | 0.782-0.976 | <0.001 |
| Intraobserver reliability of tibial slope measurements made by an attending orthopedic surgeon | |||
| ICC | 95% CI | p | |
| MTS on radiographs | 0.855 | 0.623-0.962 | <0.001 |
| MTS on MRI | 0.926 | 0.808-0.979 | <0.001 |
| LTS on MRI | 0.858 | 0.647-0.959 | <0.001 |
| ICC: Intraclass correlation coefficients; CI: Confidence interval; MTS: Medial tibial slope; MRI: Magnetic resonance imaging; LTS: Lateral tibial slope. | |||
Interobserver measurement of MTS on radiographs showed excellent agreement among the three reviewers (ICC=0.925, p<0.001; Table V). Interobserver measurement of MTS on MRI showed good agreement among the three reviewers (ICC=0.755, p=0.002). Interobserver measurement of LTS on MRI showed good agreement among the three reviewers (ICC=0.820, p<0.001).
Table 5. Interobserver reliability of tibial slope measurements made by the three reviewers.
| Interobserver reliability of tibial slope measurements made by the three reviewers | |||
| ICC | 95% CI | p | |
| MTS on radiographs | 0.925 | 0.788-0.980 | <0.001 |
| MTS on MRI | 0.755 | 0.335-0.932 | 0.002 |
| LTS on MRI | 0.820 | 0.491-0.951 | <0.001 |
| ICC: Intraclass correlation coefficients; CI: Confidence interval; MTS: Medial tibial slope; MRI: Magnetic resonance imaging; LTS: Lateral tibial slope. | |||
Discussion
Our study suggested a moderate positive correlation between MTS and LTS measured on MRI in 97 patients with ACL injury. The average MTS and LTS did not significantly differ from each other. Second, the average MTS measured on radiographs was significantly greater than that measured on MRI scans, with a low positive correlation. In addition, the intra- and interobserver reliability was mostly good to excellent between reviewers with over 10 years of clinical experience gaps.
Our study demonstrated a significant positive correlation between MTS and LTS measured on MRI scans. The average LTS was slightly larger than the MTS on MRI, but the difference was not significant in our study. Meier et al.[22] demonstrated a significant positive correlation between MTS and LTS measured by CT scans using three-dimensional computer-aided design models, and the Pearson’s correlation coefficient (r) between MTS and LTS was 0.59, with a p value <0.0001. The tibial slope measurement method described in Meier et al.’s[22] study was somewhat different from our study with the mechanical tibial axis defined by using the ankle center. Although different tibial axis definitions and imaging modalities were adopted in the study mentioned above and our study, the results showed a similar correlation coefficient between MTS and LTS, with ours being 0.544. It may be concluded that regardless of the measurement method or imaging modality adopted, the correlation between MTS and LTS was moderately positive with statistical significance. Regarding the correlation between different imaging modalities using a similar definition of tibial slope measurement, Jahn et al.[23] showed a low to negligible correlation between radiographic and MRI measurements for both MTS and LTS (r=0.30 and 0.37, respectively), whereas the p-value was not reported in the study. Our study also showed a low correlation of MTS measured by radiographs and MRI with significance (r=0.480, p<0.001). The main difference in the measurement method was that we used the two-circle method to define the tibial axis on MRI, whereas Jahn et al.[23] used a connected line of two middle points between the anterior and posterior tibial cortex 1 cm and 6 cm distal to the tibial tuberosity, separately. Although both studies showed a low correlation between radiographs and MRI, the correlation coefficient was higher in our study, suggesting that the different measurement methods adopted may influence the tibial slope correlation between different imaging modalities. Further comparison of the correlation between other different measurement methods on MRI and a single method of measurement on radiographs could be investigated to determine the method with the best correlation.
Additionally, it is worth noting that MTS measured by radiographs and MRI scans were significantly different. Although a significant positive correlation was observed, the correlation was not high (r=0.480). The study by Jahn et al.[23] also reported a similar finding, demonstrating that the tibial slope was different when measured by radiographs and MRI scans in patients with knee pain. In Jahn et al.’s study,[23] patients suffering from knee pain with complete images on file were included; thus, the 81 patients included in that study might include those with and without ACL injury that was indicated for ACLR. Our study further focused on the patient group with ACL pathologies who subsequently underwent double-bundle ACLR by a single surgeon. The average MTS on radiographs was 8.7° vs. 10.5° in their study and our study, respectively. The MTS on MRI was 4.4° and 6.4°, respectively, and the average LTS on MRI was 6.2° and 6.9°, respectively. Considering the similar methods of measurement in the two studies, it appears that although these values cannot be compared statistically, the tibial slopes measured either by radiographs or MRI in our study were generally larger than those in the study by Jahn et al.[23] This finding was consistent with previous studies suggesting a correlation between a steeper tibial slope and ACL injury.[1,2] Furthermore, a previous study demonstrated that a steeper LTS may result in inferior long-term subjective outcomes in patients undergoing double-bundle ACLR. Therefore, the study on tibial slope measurement focusing on patients with ACL injury is of great importance.[29]
It remains unclear which imaging modality is most correlated with ACL injury or ACLR failure. A previous study in which the tibial axis was defined as two connected points that represented the midpoints of the anteroposterior width of the tibia made approximately 4 to 5 cm apart and as distally in the sagittal image as possible on MRI showed that the MTS cutoff for increased ACL injury risk was 4.5° in male and 4.3° in female patients.[30] Another study also used MRI with a different tibial axis definition as the midpoint of the anteroposterior width of the tibia at two points located 4 to 5 cm from the joint line and as distal as possible, reporting a cutoff LTS of 4° as a predictor of increased risk of pediatric ACL tears.[31] The LTS cutoff for high-grade rotatory laxity after ACL injury was 9° based on another measurement method on MRI with two cranial and caudal circles fitted to the head of the tibia and a connected line of the center of the two circles defined as the tibia longitudinal axis.[32] Regarding ACLR failure, some previous studies demonstrated that when the patient’s tibial slope measured on radiographs using the tibial axis defined as a line connecting the midcortical diameters of the tibia at points 5 and 15 cm distal to the knee joint was greater than 12°, the risk of ACLR failure increased.[6,8,9,33] Another study using the posterior tibial cortex as the tibial axis on radiographs showed that the tibial slope was significantly greater in patients undergoing primary ACLR than in patients with a healthy knee with tibial slopes of 6.79° and 5.31°, respectively, and these values were markedly less than those reported in studies using 12° as the cutoff.[13] Grassi et al.[21] used two midpoints between the anterior and posterior tibial cortex, including 5- and 15-cm distances below the tibial tuberosity, connected as the tibial axis on MRI, demonstrating that an LTS cutoff of 7.4° was a predictor of ACLR failure. Two studies using the method with two circles fitted to the proximal tibia on MRI showed that the risks of anterior tibial translation ≥5 mm and lower ACLR survivorship would be greater if MTS >5.6° and LTS >3.8°.[34,35] Another study used the intermediate vertical line on the sagittal image as the tibial axis on MRI, reporting an average MTS of 4.47° and LTS of 2.66° in the ACL-deficient group.[2] However, none of these studies compared tibial slopes measured by radiographs and MRI scans and investigated the imaging modality that was most correlated with poor outcomes after ACLR. The precise definition of tibial slope and standard measurement methods remain variable and debatable. Future studies should focus on investigating the different imaging modalities of tibial slope measurement, including radiographs, CT, and MRI, and the different measurement methods of each imaging modality that are most correlated with ACL injury, ACLR failure, or poor functional outcomes after ACLR.
In addition, Jahn et al.[23] demonstrated a good reproducibility and reliability of tibial slope measurement on both radiographs and MRI. Compared to Jahn et al.’s study that included three reviewers who were two ORs and an orthopedic fellow, our study demonstrated the intra- and interobserver reliability of measurements among three reviewers with considerably different levels of knowledge, familiarity, and experience in orthopedics and ACL surgery. The three reviewers in our study included a PGY doctor, an OR, and an attending orthopedic surgeon. Our findings indicate that when the reviewers are well-educated and the methods of tibial slope measurement reach consensus, the tibial slopes measured by different reviewers with differences in years of experience are reliable.
Some limitations in our study should be noted. First, due to unclear and poorly defined borders of the lateral tibial plateau, LTS was not measured on radiographs. A precise definition of LTS on radiographs should be made to investigate the correlation between MTS and LTS on radiographs, and further investigation of the correlation of LTS measured by radiographs and MRI could be performed. In addition, the correlation between MTS and LTS on radiographs should be assessed. In addition, a modified method of tibial slope measurement on MRI was proposed in this study with good to excellent intra- and interobserver reliability. The correlation between tibial slope measured by this method and ACL injury or clinical outcomes after ACLR could be investigated in future studies. In addition, the sex of the patients included in our study was predominantly male (male-tofemale ratio of 93:4). Therefore, future studies should investigate the effect of sex on the correlation of MTS and LTS as well as the tibial slopes on different imaging modalities.
In conclusion, the average MTS and LTS measured on MRI in patients with ACL injury did not significantly differ, but a moderate positive correlation was observed. The average MTS measured on radiographs was significantly greater than that on MRI, with a low positive correlation. Therefore, a high MTS on MRI could predict a high LTS in the same patient with ACL injury and vice versa. In addition, the results of tibial slopes measured by different reviewers with gaps in years of experience could be reliable.
Footnotes
Ethics Committee Approval: The study protocol was approved by the Chang Gung Medical Foundation Institutional Review Board (date: 12.09.2022, no: 202201347B0). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Patient Consent for Publication: A written informed consent was obtained from each patient.
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Author Contributions: Study conception and design, data collection, performing analysis; and writing the paper: K.Y.L.; Study conception and design data, collection: C.P.Y.; Data collection: S.Y.Y., Y.C.H., S.F.H., Y,J,C.; Study conception and design: C.H.C., C.S.H., Y.S.C.
Citation: Lin KY, Yang CP, Yao SY, Hung YC, Hung SF, Chen YJ, et al. Correlation of medial tibial slope and lateral tibial slope measured on radiographs and magnetic resonance imaging in patients with anterior cruciate ligament injury. Jt Dis Relat Surg 2024;35(3):504-512. doi: 10.52312/jdrs.2024.1558.
Financial Disclosure
The authors received no financial support for the research and/or authorship of this article.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1.Korthaus A, Krause M, Pagenstert G, Warncke M, Brembach F, Frosch KH, et al. Tibial slope in the posterolateral quadrant with and without ACL injury. Arch Orthop Trauma Surg. 2022;142:3917–3925. doi: 10.1007/s00402-021-04298-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hohmann E, Tetsworth K, Glatt V, Ngcelwane M, Keough N. Medial and lateral posterior tibial slope are independent risk factors for noncontact ACL injury in both men and women. Orthop J Sports Med. 2021;9:23259671211015940–23259671211015940. doi: 10.1177/23259671211015940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lin LJ, Akpinar B, Meislin RJ. Tibial slope and anterior cruciate ligament reconstruction outcomes. e0184JBJS Rev. 2020;8 doi: 10.2106/JBJS.RVW.19.00184. [DOI] [PubMed] [Google Scholar]
- 4.Christensen JJ, Krych AJ, Engasser WM, Vanhees MK, Collins MS, Dahm DL. Lateral tibial posterior slope is increased in patients with early graft failure after anterior cruciate ligament reconstruction. Am J Sports Med. 2015;43:2510–2514. doi: 10.1177/0363546515597664. [DOI] [PubMed] [Google Scholar]
- 5.Jaecker V, Drouven S, Naendrup JH, Kanakamedala AC, Pfeiffer T, Shafizadeh S. Increased medial and lateral tibial posterior slopes are independent risk factors for graft failure following ACL reconstruction. Arch Orthop Trauma Surg. 2018;138:1423–1431. doi: 10.1007/s00402-018-2968-z. [DOI] [PubMed] [Google Scholar]
- 6.Lee CC, Youm YS, Cho SD, Jung SH, Bae MH, Park SJ, et al. Does posterior tibial slope affect graft rupture following anterior cruciate ligament reconstruction. Arthroscopy. 2018;34:2152–2155. doi: 10.1016/j.arthro.2018.01.058. [DOI] [PubMed] [Google Scholar]
- 7.Li Y, Hong L, Feng H, Wang Q, Zhang H, Song G. Are failures of anterior cruciate ligament reconstruction associated with steep posterior tibial slopes. A case control study. Chin Med J (Engl) 2014;127:2649–2653. [PubMed] [Google Scholar]
- 8.Salmon LJ, Heath E, Akrawi H, Roe JP, Linklater J, Pinczewski LA. 20-year outcomes of anterior cruciate ligament reconstruction with hamstring tendon autograft: The catastrophic effect of age and posterior tibial slope. Am J Sports Med. 2018;46:531–543. doi: 10.1177/0363546517741497. [DOI] [PubMed] [Google Scholar]
- 9.Webb JM, Salmon LJ, Leclerc E, Pinczewski LA, Roe JP. Posterior tibial slope and further anterior cruciate ligament injuries in the anterior cruciate ligamentreconstructed patient. Am J Sports Med. 2013;41:2800–2804. doi: 10.1177/0363546513503288. [DOI] [PubMed] [Google Scholar]
- 10.Gültekin MZ, Dinçel YM, Keskin Z, Arslan S, Yıldırım A. Morphometric risk factors effects on anterior cruciate ligament injury. Jt Dis Relat Surg. 2023;34:130–137. doi: 10.52312/jdrs.2023.910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ho JPY, Merican AM, Hashim MS, Abbas AA, Chan CK, Mohamad JA. Three-dimensional computed tomography analysis of the posterior tibial slope in 100 knees. J Arthroplasty. 2017;32:3176–3183. doi: 10.1016/j.arth.2017.04.060. [DOI] [PubMed] [Google Scholar]
- 12.Lipps DB, Wilson AM, Ashton-Miller JA, Wojtys EM. Evaluation of different methods for measuring lateral tibial slope using magnetic resonance imaging. Am J Sports Med. 2012;40:2731–2736. doi: 10.1177/0363546512461749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gaj E, Monaco E, De Carli A, Wolf MR, Massafra C, Redler A, et al. Measurement technique for posterior tibial slope on radiographs can affect its relationship to the risk of anterior cruciate ligament rupture. Int Orthop. 2021;45:1469–1475. doi: 10.1007/s00264-020-04865-7. [DOI] [PubMed] [Google Scholar]
- 14.Faschingbauer M, Sgroi M, Juchems M, Reichel H, Kappe T. Can the tibial slope be measured on lateral knee radiographs. Knee Surg Sports Traumatol Arthrosc. 2014;22:3163–3167. doi: 10.1007/s00167-014-2864-1. [DOI] [PubMed] [Google Scholar]
- 15.Amerinatanzi A, Summers RK, Ahmadi K, Goel VK, Hewett TE, Nyman E. Automated measurement of patientspecific tibial slopes from MRI. Bioengineering (Basel) 2017;4:69–69. doi: 10.3390/bioengineering4030069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Utzschneider S, Goettinger M, Weber P, Horng A, Glaser C, Jansson V, et al. Development and validation of a new method for the radiologic measurement of the tibial slope. Knee Surg Sports Traumatol Arthrosc. 2011;19:1643–1648. doi: 10.1007/s00167-011-1414-3. [DOI] [PubMed] [Google Scholar]
- 17.Balta O, Erpala F, Astan S, Uçar C, Altınayak H, Aytekin K. The prevalence of fabella and its relationship with the lateral posterior condylar offset and lateral posterior tibial slope values. Jt Dis Relat Surg. 2022;33:588–598. doi: 10.52312/jdrs.2022.723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Amerinatanzi A, Summers R, Ahmadi K, Goel VK, Hewett TE, Nyman E Jr. A novel 3D approach for determination of frontal and coronal plane tibial slopes from MR imaging. Knee. 2017;24:207–216. doi: 10.1016/j.knee.2016.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yoo JH, Chang CB, Shin KS, Seong SC, Kim TK. Anatomical references to assess the posterior tibial slope in total knee arthroplasty: A comparison of 5 anatomical axes. J Arthroplasty. 2008;23:586–592. doi: 10.1016/j.arth.2007.05.006. [DOI] [PubMed] [Google Scholar]
- 20.Naendrup JH, Drouven SF, Shaikh HS, Jaecker V, Offerhaus C, Shafizadeh ST, et al. High variability of tibial slope measurement methods in daily clinical practice: Comparisons between measurements on lateral radiograph, magnetic resonance imaging, and computed tomography. Knee. 2020;27:923–929. doi: 10.1016/j.knee.2020.01.013. [DOI] [PubMed] [Google Scholar]
- 21.Grassi A, Signorelli C, Urrizola F, Macchiarola L, Raggi F, Mosca M, et al. Patients with failed anterior cruciate ligament reconstruction have an increased posterior lateral tibial plateau slope: A case-controlled study. Arthroscopy. 2019;35:1172–1182. doi: 10.1016/j.arthro.2018.11.049. [DOI] [PubMed] [Google Scholar]
- 22.Meier M, Janssen D, Koeck FX, Thienpont E, Beckmann J, Best R. Variations in medial and lateral slope and medial proximal tibial angle. Knee Surg Sports Traumatol Arthrosc. 2021;29:939–946. doi: 10.1007/s00167-020-06052-y. [DOI] [PubMed] [Google Scholar]
- 23.Jahn R, Cooper JD, Juhan T, Kang HP, Bolia IK, Gamradt SC, et al. Reliability of plain radiographs versus magnetic resonance imaging to measure tibial slope in sports medicine patients: Can they be used interchangeably. Orthop J Sports Med. 2021;9:23259671211033882–23259671211033882. doi: 10.1177/23259671211033882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bisicchia S, Scordo GM, Prins J, Tudisco C. Do ethnicity and gender influence posterior tibial slope. J Orthop Traumatol. 2017;18:319–324. doi: 10.1007/s10195-017-0443-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hashemi J, Chandrashekar N, Gill B, Beynnon BD, Slauterbeck JR, Schutt RC Jr, et al. The geometry of the tibial plateau and its influence on the biomechanics of the tibiofemoral joint. J Bone Joint Surg [Am] 2008;90:2724–2734. doi: 10.2106/JBJS.G.01358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hudek R, Schmutz S, Regenfelder F, Fuchs B, Koch PP. Novel measurement technique of the tibial slope on conventional MRI. Clin Orthop Relat Res. 2009;467:2066–2072. doi: 10.1007/s11999-009-0711-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15:155–163. doi: 10.1016/j.jcm.2016.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Mukaka MM. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med J. 2012;24:69–71. [PMC free article] [PubMed] [Google Scholar]
- 29.Yang CP, Hung SF, Lin KY, Hung YC, Chen YJ, Yao SY, et al. The increased lateral tibial slope may result in inferior long-term clinical outcome after DB-ACL reconstruction. Arch Orthop Trauma Surg. 2024;144:619–626. doi: 10.1007/s00402-023-05114-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kızılgöz V, Sivrioğlu AK, Ulusoy GR, Aydın H, Karayol SS, Menderes U. Analysis of the risk factors for anterior cruciate ligament injury: An investigation of structural tendencies. Clin Imaging. 2018;50:20–30. doi: 10.1016/j.clinimag.2017.12.004. [DOI] [PubMed] [Google Scholar]
- 31.Dare DM, Fabricant PD, McCarthy MM, Rebolledo BJ, Green DW, Cordasco FA, et al. Increased lateral tibial slope is a risk factor for pediatric anterior cruciate ligament injury: An MRI-based case-control study of 152 patients. Am J Sports Med. 2015;43:1632–1639. doi: 10.1177/0363546515579182. [DOI] [PubMed] [Google Scholar]
- 32.Rahnemai-Azar AA, Abebe ES, Johnson P, Labrum J, Fu FH, Irrgang JJ, et al. Increased lateral tibial slope predicts high-grade rotatory knee laxity pre-operatively in ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2017;25:1170–1176. doi: 10.1007/s00167-016-4157-3. [DOI] [PubMed] [Google Scholar]
- 33.Schillhammer C. Editorial commentary: Managing excessive posterior slope in anterior cruciate ligament reconstruction: Where do we draw the line. Arthroscopy. 2018;34:2156–2157. doi: 10.1016/j.arthro.2018.04.005. [DOI] [PubMed] [Google Scholar]
- 34.Li Y, Hong L, Feng H, Wang Q, Zhang J, Song G, et al. Posterior tibial slope influences static anterior tibial translation in anterior cruciate ligament reconstruction: A minimum 2-year follow-up study. Am J Sports Med. 2014;42:927–933. doi: 10.1177/0363546514521770. [DOI] [PubMed] [Google Scholar]
- 35.Yoon KH, Park SY, Park JY, Kim EJ, Kim SJ, Kwon YB, et al. Influence of posterior tibial slope on clinical outcomes and survivorship after anterior cruciate ligament reconstruction using hamstring autografts: A minimum of 10-year follow-up. Arthroscopy. 2020;36:2718–2727. doi: 10.1016/j.arthro.2020.06.011. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.