

Abstract
Purpose
Using swept-source optical coherence tomography (SS-OCT) to explore the effect of high myopia on superficial retina vascular density (SVD) of the peripheral region and the area of radial peripapillary capillaries (RPCs).
Methods
In this cross-sectional study, a total of 91 volunteers (34 male subjects and 57 female subjects) were recruited and 34 individuals in the high myopic group (group A) and 57 individuals in the low myopic group (group B). Using the wide-field OCT-angiography (OCTA; 24 × 20 mm, 120 degrees angular field) compared the peripheral SVD and the area of RPC between the two groups and investigated its correlation with ocular axial length and diopter.
Results
Peripheral SVD of group B around the supratemporal (SVD1), supranasal (SVD2), infratemporal (SVD3), and infranasal (SVD4) directions were significantly higher than those of group A (all P < 0.05). The RPC area of group B around the supranasal (RPC2) and infranasal (RPC4) were significantly larger than that of group A (all P < 0.01). Ocular axial length and diopter were significantly correlated with SVD2 and SVD4 (all P < 0.05), and they also have a significant correlation with the supratemporal (RPC1), RPC2, and RPC4 (all P < 0.05).
Conclusions
Peripheral SVD was decreased and the RPC area was mainly reduced on the nasal side in the high myopic group. Peripheral SVD and area of RPC are significantly correlated with ocular axial length and diopter.
Translational Relevance
The wide-field OCTA can be used for new detection of myopia’s impact on the retinal peripheral SVD and area of peripapillary RPC, offering new insights into the progression of myopia.
Keywords: swept-source optical coherence tomography (SS-OCT), wide-field optical coherence tomography angiography (OCTA), high myopia, peripheral retina, superficial vascular density (SVD), radial peripapillary capillaries (RPCs)
Introduction
Recently, myopia is becoming a global public health problem, especially in East and Southeast Asian countries.1 As it was reported in this area, the incidence of myopia in young adults was about 80%, accompanying approximately 10% of patients with high myopia among them.1 It is worse that almost half of the global population might get myopia by the end of 2050, which included 10% high myopia.2 With the progress of myopia, there would be many serious complications, especially in pathological myopia, such as retinal detachment, retinal neovascularization, glaucoma, and so on, which can lead to uncorrectable vision loss or even blindness and reduce the quality of life sharply.3 Therefore, for patients with myopia, it might be a vital public health priority to prevent or delay the appearance of pathology myopia by discovering early differences in the retina’s structure and vessels.
Swept-source optical coherence tomography angiography (SS-OCTA) is a high-resolution, rapid, noninvasive, noncontact fundus angiography technology which is widely applied to the examination of retinopathy.4 Wide-field OCTA can scan the maximum image with 24 mm in the horizontal direction, 20 mm in the vertical direction, and 6 mm in depth, which allowed us to observe the retina’s structure and capillaries on a larger scale.
Recently, several studies explored the effects of myopia on retinal thickness, vascular density (VD), and radial peripapillary capillary (RPC) VD using wide-field OCTA.5–7 It was found that the thickness of the inner retina in most peripheral regions and outer retina in the superior and supranasal peripheral regions significant decreased as the severity of myopia increased.5 Another study has shown that macular area VD were significantly decreased in patients with high myopia.7 In addition, it has also found an association between reduced RPC VD and high myopia.6 RPC is crucial for the nutrition and blood supply of the retinal nerve fiber layer (RNFL) surrounding the optic nerve, which might lead to RNFL atrophy in patients with myopia.6,8
Although there were several studies on myopia and retinal VD, they have not specifically examined peripheral SVD and the area of RPC by using the wide-field OCTA, and analyzed the relationship among ocular axial length, diopter, and them. In this study, it focused on the changes of peripheral SVD and the area of RPC of different regions in high myopia and explored the correlation among ocular axial length, diopter, peripheral SVD, and area of RPC. It was hoped that new detection of changes in peripheral SVD and the area of RPC in high myopia would have exploratory implications for myopia progression.
Methods
This study was approved by the institutional review board of Wuhan University and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from each volunteer before wide-field OCTA imaging.
Subjects
A total of 91 volunteers were recruited for this study at the Eye Center, Renmin Hospital of Wuhan University, between September 2021 and December 2021. The age of the volunteers ranged from 16 to 36 years. One eye per volunteer was selected randomly and recruited only with an image quality over 7/10. Each volunteer underwent a slit-lamp fundus examination, intraocular pressure (IOP) measurement, and collection of basic clinic data. All participants were divided into two groups: group A (high myopia, 34 eyes, diopter <−6), and group B (low myopia, 57 eyes, diopter ≥−6).
Exclusion criteria were as follows: (1) IOP > 21 mm Hg; (2) best corrected visual acuity < 1.0; (3) obvious media opacity; (4) history of the ophthalmological disease, and existing uveitis, glaucoma, retinal diseases, and/or choroidal diseases; (5) history of cerebral disease; (6) history of respiratory disease; (7) history of cardiac disease; (8) history of hypertension; and (9) history of diabetes mellitus.
OCTA Imaging
The wide-field OCTA (TowardPi BM-400K) has an A-scan repetition rate of 400,000 Hz and uses a laser centered at 1060 nm. It utilizes a swept-source vertical cavity surface emitting laser (VCSEL) with a wavelength of 1060 nm and a scanning rate of 400,000 A-scans per second, providing a transverse resolution of 10 um and an in-depth resolution (optical) of 3.8 um. This instrument has an A-scan depth of 6.0 mm in tissue (2560 pixels). The OCTA scan is centered on the macula as default; a single scan presents the OCTA image in a range of 24 × 20 mm, corresponding to a 120 degrees angular field of view. The typical acquisition time is about 15 seconds for each 24 mm width OCTA scan.
The quantification of SVD was automatically calculated using the built-in algorithm, based on the scan of 24 × 20 mm OCTA images in the peripheral superficial retina. The SVD is defined as the region between the internal limiting membrane and 9 µM above the inner plexiform layer. The macular as the center, and the X-axis is the line of the macular center to the optic disc; the Y-axis crosses the center of the macula and is perpendicular to the X-axis. Along the four-angle bisector on the XY axes at 9 mm from the macula in the supratemporal (SVD1), supranasal (SVD2), infratemporal (SVD3), and inferonasal (SVD4) directions, the built-in system automatically generated and calculated SVD of the 6 × 6 mm circles. The inside semicircular density was obtained from the four selected areas (Fig. 1).
Figure 1.

The four points were selected from the superficial retina vascular density of peripheral regions.
The RPCs are the linear vessels radiated from the optic disc that supplies the RNFL around the optic disc. The optic disc is the center, and the X-axis is the line of the optic disc to the macular center; the Y-axis crosses the center of the optic disc and is perpendicular to the X-axis. The area of RPC was divided into four parts. In the wide-field OCTA images, the long and straight capillaries can be observed. At the ends of RPCs, the capillaries bifurcate to form capillary arcs or disappear, which can be used to mark the boundary of the RPC region (Fig. 2). It was manually traced in the linear vessels and we performed the localization of four RPC areas in the supratemporal (RPC1), supranasal (RPC2), infratemporal (RPC3), and inferonasal (RPC4 ) directions. Two 5-year experienced ophthalmologists of fundus diseases utilized the characteristics of RPC to analyze and calculate the area of RPC using Image J software. No statistical difference was found between the data obtained by the two ophthalmologists (Fig. 3).
Figure 2.
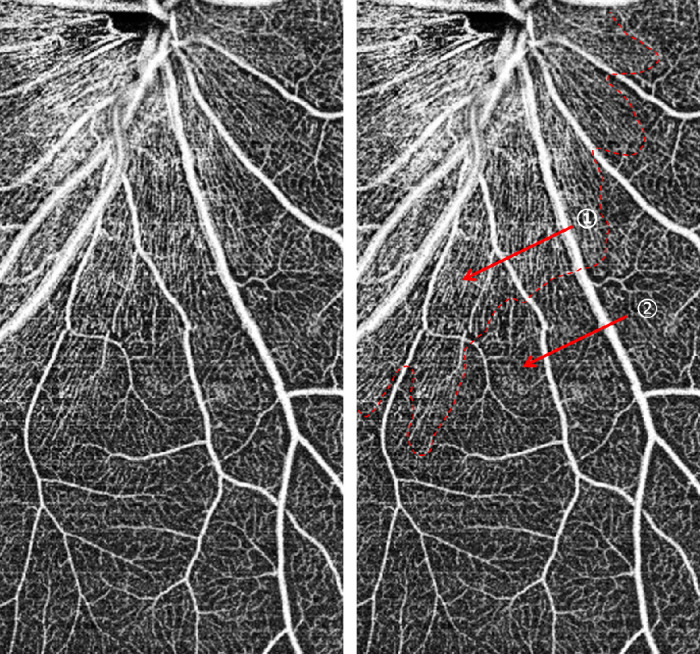
① Radial peripapillary capillaries: long and straight linear vessels. ② Capillaries: capillary arcs or disappear.
Figure 3.

The area of radial peripapillary capillaries in high myopia (a, b) and low myopia (c, d).
Statistics
All data were analyzed using SPSS software (version 23.0; SPSS, Inc., Chicago, IL, USA). All continuous data were examined by the D'Agostino and Pearson omnibus normality test, after which they were examined by the Levene test to determine the homogeneity of variance. All data are presented as means ± standard deviations. The statistical method was the t-test. A multivariable regression analysis was used to examine the relationship between age, axial length, diopter, SVD, and the area of RPC. All P values were 2-sided, and the P values < 0.05 were considered statistically significant. Localization of the area of RPC and calculation of their coverage area was done using ImageJ.
Results
Demographic Information
A total of 91 volunteers and 91 eyes were recruited for this study at the Eye Center. The volunteers were divided into two groups, the high myopic group and the low myopic group. The maximum refractive error of the volunteers was −11 diopters (D), and the maximum ocular axial length was 30.5 mm. There was no statistical difference in age or gender in the two groups (all P > 0.05). The high myopia group had longer axial lengths and higher degrees of myopia (all P < 0.0001; Table 1).
Table 1.
Demographic Information
| Group | Low Myopiaa | High Myopiaa | P Value |
|---|---|---|---|
| Age, y | 25.19 ± 5.642 | 23.21 ± 4.333 | 0.081 |
| Sex, male/female | 22/35 | 12/22 | 0.753 |
| Spherical equivalent, diopter | −3.25 ± 2.01 | −8.10 ± 1.20 | <0.0001 |
| Axial length, mm | 25.38 ± 1.40 | 28.55 ± 1.09 | <0.0001 |
Mean ± SD. The statistical method was the t-test and all P values were 2-sided, and P values < 0.05 were considered statistically significant.
Comparison of Peripheral SVD Between High and Low Myopic Groups
The peripheral SVD of group B around the four directions were higher than that of group A, and all the differences were significant (SVD1 = 29.94 ± 6.41 vs. 33.37 ± 5.17, SVD2 = 34.46 ± 5.43 vs. 37.73 ± 5.49, SVD3 = 27.05 ± 6.96 vs. 30.32 ± 7.33, and SVD4 = 25.01 ± 5.73 vs. 27.98 ± 6.48; all P < 0.05; Fig. 4).
Figure 4.
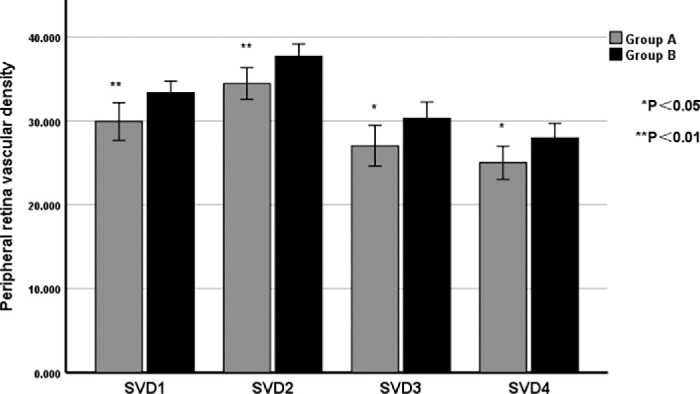
Comparison of supratemporal (SVD1), supranasal (SVD2), infratemporal (SVD3), and infranasal (SVD4) peripheral superficial vascular density between high and low myopic groups. The statistical method was the t-test and all P values were 2-sided, and P values < 0.05 were considered statistically significant.
The Area of RPC in Low and High Myopic Groups
The whole area of RPC of group B was significantly larger than that of group A (RPC = 31.48 mm2 ± 6.20 vs. 39.49 mm2 vs. 8.98; P < 0.01). The area of RPC of group B around RPC2 and RPC4 were larger than that of group A, and all the differences were significant (RPC2 = 4.68 mm2 ± 1.75 vs. 7.31 mm2 ± 2.26, and RPC4 = 2.80 mm2 ± 1.40 vs. 5.08 mm2 ± 2.35; all P < 0.01). There was no significant differences of the area of RPC1 and RPC3 (RPC1 = 11.53 mm2 ± 3.47 vs. 13.11 mm2 ± 4.05, and RPC3 = 12.47 mm2 ± 3.46 vs. 13.98 mm2 ± 3.98; all P > 0.05; Fig. 5).
Figure 5.
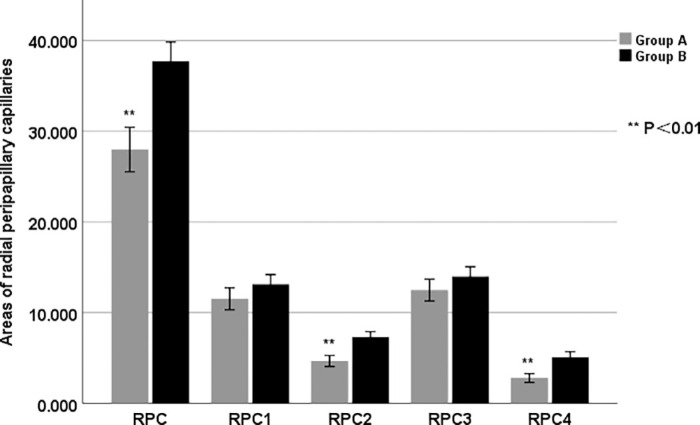
Comparison of the whole, supratemporal (RPC1), supranasal (RPC2), infratemporal (RPC3), and infranasal (RPC4) areas of radial peripapillary capillaries between high and low myopic groups. The statistical method was the t-test and all P values were 2-sided, and P values < 0.05 were considered statistically significant.
Univariate Regression Analysis of Peripheral SVD and the Area of RPC With Axial Length, Diopter, Age, and Sex
Axial length was negatively correlated with peripheral SVD in SVD2, SVD3, and SVD4 (all P < 0.05). Diopter was positively correlated with peripheral SVD in SVD2, SVD3, and SVD4 (all P < 0.05). Axial length was negatively correlated with the area of RPC in RPC1, RPC2, and RPC4 (all P < 0.05). Diopter was positively correlated with the area of RPC in RPC1, RPC2, and RPC4 (all P < 0.05). There was no statistical difference in age, sex, peripheral SVD, and area of RPC (Table 2).
Table 2.
Univariate Regression Analysis to Identify Factors Associated with Peripheral SVD and Area of RPC
| AL | SE | Age | Sex | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | R2 | P Value | B | R2 | P Value | B | R2 | P Value | B | R2 | P Value | |
| SVD1 | −0.544 | 0.035 | 0.076 | 0.403 | 0.041 | 0.055 | 0.066 | 0.004 | 0.541 | −0.776 | 0.004 | 0.545 |
| SVD2 | −0.744 | 0.070 | 0.010a | 0.521 | 0.073 | 0.009a | −0.155 | 0.025 | 0.132 | 1.099 | 0.009 | 0.374 |
| SVD3 | −0.795 | 0.048 | 0.037a | 0.628 | 0.064 | 0.016a | 0.28 | 0.056 | 0.084 | −0.548 | 0.001 | 0.732 |
| SVD4 | −0.911 | 0.084 | 0.005a | 0.565 | 0.069 | 0.012a | 0.098 | 0.008 | 0.397 | −0.238 | 0.001 | 0.863 |
| RPC1 | −0.484 | 0.063 | 0.017a | 0.361 | 0.075 | 0.009a | 0.006 | 0.001 | 0.928 | −1.623 | 0.041 | 0.054 |
| RPC2 | −0.602 | 0.248 | 0.001a | 0.433 | 0.273 | 0.001a | 0.048 | 0.013 | 0.286 | 0.069 | 0.001 | 0.896 |
| RPC3 | −0.229 | 0.014 | 0.258 | 0.179 | 0.019 | 0.195 | 0.060 | 0.008 | 0.391 | −1.175 | 0.022 | 0.160 |
| RPC4 | −0.491 | 0.182 | 0.001a | 0.375 | 0.227 | 0.001a | 0.071 | 0.032 | 0.090 | −0.255 | 0.003 | 0.614 |
P values < 0.05 were considered statistically significant.
R2, correlation coefficient; B, regression coefficient.
AL, axial length, mm; SE, spherical equivalent, Diopter; age, years, and sex, male/female.
Peripheral superficial vascular density of supratemporal (SVD1), supranasal (SVD2), infratemporal (SVD3), and infranasal (SVD4).
Areas of radial peripapillary capillaries of supratemporal (RPC1), supranasal (RPC2), infratemporal (RPC3), and infranasal (RPC4).
Multivariable Regression Analysis of Peripheral SVD and the Area of RPC with Axial Length and Diopter After Adjusting for Age and Sex
After adjusting for the effects of age and sex, a multivariable regression analysis was performed. Axial length was negatively correlated with peripheral SVD in SVD2 and SVD4 (all P < 0.05). Diopter was positively correlated with peripheral SVD in SVD2 and SVD4 (all P < 0.05). Axial length was negatively correlated with the area of RPC in RPC1, RPC2, and RPC4 (all P < 0.05). Diopter was positively correlated with the area of RPC in RPC1, RPC2, and RPC4 (all P < 0.05; Table 3).
Table 3.
Multivariable Regression Analysis to Identify Factors Associated with Peripheral SVD and Area of RPC
| AL | SE | |||||
|---|---|---|---|---|---|---|
| B | R2 | P Value | B | R2 | P Value | |
| SVD1 | −0.509 | 0.036 | 0.129 | 0.379 | 0.042 | 0.093 |
| SVD2 | −1.020 | 0.128 | 0.001a | 0.681 | 0.126 | 0.001a |
| SVD3 | −0.578 | 0.072 | 0.158 | 0.509 | 0.088 | 0.064 |
| SVD4 | −0.944 | 0.053 | 0.008a | 0.569 | 0.070 | 0.019a |
| RPC1 | −0.488 | 0.096 | 0.025a | 0.354 | 0.104 | 0.015a |
| RPC2 | −0.655 | 0.262 | 0.001a | 0.462 | 0.286 | 0.001a |
| RPC3 | −0.145 | 0.035 | 0.507 | 0.126 | 0.038 | 0.391 |
| RPC4 | −0.481 | 0.184 | 0.001a | 0.370 | 0.229 | 0.001a |
P values < 0.05 were considered statistically significant.
R2, correlation coefficient; B, regression coefficient.
AL, axial length, mm; SE, spherical equivalent, Diopter.
Areas of radial peripapillary capillaries of supratemporal (RPC1), supranasal (RPC2), infratemporal (RPC3), and infranasal (RPC4).
Peripheral superficial vascular density of supratemporal (SVD1), supranasal (SVD2), infratemporal (SVD3), and infranasal (SVD4).
Discussion
High myopia is often associated with a variety of complications that greatly increase the likelihood of retinal vascular and neurological lesions in the fundus and can even lead to blindness.9–11 Recently, several studies explored the effects of myopia on retinal thickness, VD, and RPC VD,5,6,12 and discovered that high myopia can lead to alterations in the peripheral thickness of the retinal layer and RPC VD. However, few studies have explored the relationship among myopia, peripheral SVD, and the area of RPC. Therefore, the new detection of changes in peripheral SVD and the area of RPC may provide valuable insights into the effects of myopia progression. The wide-field OCTA can provide clear OCTA images of the fundus within a range of 24 × 20 mm, enabling the detection of changes in peripheral retinal capillaries. In this study, it was found that the high myopic group has lower peripheral SVD and a smaller area of RPC. Furthermore, ocular axial length and diopter had significant correlations with peripheral SVD and the area of RPC.
The retinal capillaries ensured all cells in the entire retina receive sufficient oxygen and nutrients, which were essential for the health and function of the visual system.13 Recent studies have explored the relationship between myopia and the macular area VD and found that retinal thickness and macular area VD were significantly decreased in high myopia.7,14 Similar with previous results, it was found that group A had significantly lower peripheral SVD in all four directions in our study. This may be attributed to the elongation of the eyeball associated with the increasing degree of myopia. Because of the eyeball continuously stretching, the retina was progressively thinned, leading to a gradual reduction in VD.14 In addition, the traction on blood vessels can affect the blood flow supply to the retina, leading to retina ischemia, which created a vicious cycle that further reduced retinal VD, especially in the peripheral area.15 In addition, because of peripheral retinal vessels being sparse and had smaller diameters, they may be more sensitive to ocular axis elongation or retinal ischemia and hypoxia in the early stages.16 Therefore, patients in group A exhibited lower peripheral SVD. A latest study reported that the deep layer VD in the dark without pressure zones was reduced compared to the corresponding regions in the opposite eye, whereas the superficial layers of VD showed no significant differences.17 White and dark without pressure usually occurred in the peripheral retina in high myopic individuals, which belonged to peripheral fundus lesions.17 Our study revealed that in high myopic individuals without peripheral retinal lesions, the peripheral SVD is lower compared to that in low myopic individuals. It was also reported that the deep layer VD did not show any significant difference in patients with high myopia without peripheral retinal lesions in the peripheral regions of the retina.6 These findings might suggest that changes in the peripheral SVD may occur earlier than in the deep layers VD during the development of high myopia. Therefore, changes in the peripheral SVD may also be involved in the development of dark without pressure zones in myopia. Early detecting the vasculature and structure of the peripheral retina may be beneficial in identifying some early differences in high myopia, and further researches are needed to explore such high myopia changes.
Group A exhibited a significantly smaller distribution area of RPC compared with group B. The decrease in the area of RPC might be due to RPCs’ characteristic of small, straight, and long vessels with fewer shunts from the surrounding vessels, which was more susceptible to the elongation of the ocular axis in patients with high myopia.18,19 Moreover, the area of RPC was significantly smaller on the nasal side in group A, and there were no significant differences on the temporal side. Previous studies also found that the VD of RPC was mainly lower on the nasal side in the high and mild myopic groups because of the temporal tilt of the optic disc,20,21 which matched the region of decrease in the area of RPC in our results. Currently, the relationship between RPC and RNFL has been one of the focus issues in the progress of myopia. Previous studies supposed that a decrease in the RNFL thickness led to the VD of RPC being reduced in highly myopic eyes.22,23 Whereas recent research proved that the VD of RPC changes may precede a decrease in RNFL thickness and relate to visual function.24 The area of RPC, a new biomarker, was proposed in this study that might be used for exploring the relationship between changes in RPC and RNFL and monitoring structural and functional defects in the progress of myopia. Meanwhile, it was observed that RPCs were replaced by capillary arcs or disappeared, and the specific underlying mechanism for this phenomenon remains unclear, which needs further investigation. Multiple common features were observed in patients with glaucoma and patients with myopia, which brings diagnostic challenges.25 The changes of RPC were also observed in glaucoma,26 thus the exploration of the area of RPC may help us to identify the impact of high myopia and glaucoma on the optic nerve.
Ocular axial length and diopter were significantly correlated with SVD2 and SVD4 in the peripheral retina. Previous studies have shown that an increase in myopia is often accompanied by elongation of the eyeball.27 It was suggested that the elongated eyeball might exert traction on the retina, leading to retinal thinning and a reduction in the caliber of peripheral retinal vessels, ultimately resulting in decreased VD.14,28 In addition, it was found that there was no significant correlation among axial length, diopter, and SVD1. It was also reported that no significant differences were found in the peripheral SVD1 region between different degrees of myopia.5 It has shown that the temporal region of the retina tends to exhibit a thicker retinal thickness and higher perfusion indices of SVD in OCTA images, indicating stronger compensatory ability in the temporal region.29 Moreover, in our study, the maximum refractive error and ocular axial length of the volunteers were −11 D and 30.5 mm, probably not yet breaking the limit of SVD1 compensation.
It was found that the area of RPC1, RPC2, and RPC4 had significant correlation with ocular axial length and diopter, whereas the area of RPC3 did not. In patients with myopia, the elongation of the ocular axial length occurs with an increase in diopters.30 As the diopter deepened, the vascular structure around the optic disc was affected, which might lead to a correlation with the area of RPC. Moreover, because the optic nerve originates from the nasal superior region of the orbit, there is a reduced probability of temporal inferior displacement of the peripapillary region during the progression of myopia.31 Therefore, the impact on RPC3 is relatively smaller. The blood supply provided by the RPC was particularly important for the nutrition and function of RNFL. Therefore, the identification of the relationship among ocular axial length, diopter, and area of RPC helps us to detect the impact of myopia at an early stage and intervene as soon as possible.
This study exhibits some limitations. First, the measurements were confined to peripheral SVD, excluding superficial thickness. Second, it mainly focused on the measurement and analysis of the area of RPC without calculating VD of the RPC. Moreover, four directions were selected to analyze the peripheral SVD with a high risk of retinal degeneration area,32,33 but this did not comprehensively represent the peripheral SVD. Fourth, a long-term follow-up of the volunteers was not conducted to assess the interplay and variations among ocular axial length, diopter, and peripheral SVD. Therefore, with the progress of OCTA technology, the condition of peripheral SVD will be comprehensively measured, and its relationship with myopia-related parameters would be analyzed by long-term follow-up studies in the future. Finally, high myopia often accompanies posterior staphyloma, and it did not eliminate the deviation caused by posterior staphyloma, which warrants further investigation in our future studies.
In conclusion, the study revealed a significant decrease in peripheral SVD and the area of RPC in the high myopic group. Additionally, it was found that ocular axial length and diopter have a significant correlation with peripheral SVD2 and SVD4 and the areas of RPC1, RPC2, and RPC4. These findings indicated that high myopia can lead to compromised blood supply in the peripheral SVD and the area of RPC. Therefore, wide-field OCTA can be used for new detection of myopia’s impact on the retinal capillaries, which can provide new insights of the progression in myopia.
Acknowledgments
The authors thank all study participants for their support of the current work.
Supported by the National Natural Science Foundation of China (NO. 42201457).
Disclosure: J. Gu, None; Y. Xu, None; D. Xiao, None; Y. Wang, None; W. Lei, None; Z. Chen, None; D. Hua, None
References
- 1. Morgan IG, French AN, Ashby RS, et al.. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. 2018; 62: 134–149. [DOI] [PubMed] [Google Scholar]
- 2. Bruce A. Re: Holden et al.: global prevalence of myopia and high myopia and temporal trends from 2000 through 2050 (Ophthalmology 2016;123:1036-1042). Ophthalmology. 2017; 124(3): e24–e25. [DOI] [PubMed] [Google Scholar]
- 3. Ikuno Y. Overview of the complications of high myopia. Retina. 2017; 37(12): 2347–2351. [DOI] [PubMed] [Google Scholar]
- 4. Lains I, Wang JC, Cui Y, et al.. Retinal applications of swept source optical coherence tomography (OCT) and optical coherence tomography angiography (OCTA). Prog Retin Eye Res. 2021; 84: 100951. [DOI] [PubMed] [Google Scholar]
- 5. Zhang W, Li C, Gong Y, et al.. Advanced ultrawide-field optical coherence tomography angiography identifies previously undetectable changes in biomechanics-related parameters in nonpathological myopic fundus. Front Bioeng Biotechnol. 2022; 10: 920197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Cheng D, Ruan K, Wu M, et al.. Characteristics of the optic nerve head in myopic eyes using swept-source optical coherence tomography. Invest Ophthalmol Vis Sci. 2022; 63(6): 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lin F, Zhao Z, Li F, et al.. Longitudinal macular retinal and choroidal microvasculature changes in high myopia. Invest Ophthalmol Vis Sci. 2021; 62(15): 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Sung MS, Heo H, Piao H, Guo Y, Park SW.. Parapapillary atrophy and changes in the optic nerve head and posterior pole in high myopia. Sci Rep. 2020; 10(1): 4607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Jonas JB, Ang M, Cho P, et al.. IMI prevention of myopia and its progression. Invest Ophthalmol Vis Sci. 2021; 62(5): 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Medina A. The cause of myopia development and progression: theory, evidence, and treatment. Surv Ophthalmol. 2022; 67(2): 488–509. [DOI] [PubMed] [Google Scholar]
- 11. Ruiz-Medrano J, Montero JA, Flores-Moreno I, Arias L, Garcia-Layana A, Ruiz-Moreno JM.. Myopic maculopathy: current status and proposal for a new classification and grading system (ATN). Prog Retin Eye Res. 2019; 69: 80–115. [DOI] [PubMed] [Google Scholar]
- 12. Zhu Q, Chen C, Yao J. Vessel density and retinal thickness from optical coherence tomography angiography as new indexes in adolescent myopia. J Ophthalmol. 2021; 2021: 6069833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Kur J, Newman EA, Chan-Ling T.. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog Retin Eye Res. 2012; 31(5): 377–406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Liu M, Wang P, Hu X, Zhu C, Yuan Y, Ke B.. Myopia-related stepwise and quadrant retinal microvascular alteration and its correlation with axial length. Eye (Lond). 2021; 35(8): 2196–2205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Zhou M, Lu B, Zhang P, Zhao J, Wang Q, Sun X. Determination of topographic variations in inner retinal blood flow areas in young Chinese subjects using optical coherence tomography angiography. Curr Eye Res. 2017; 42(11): 1491–1496. [DOI] [PubMed] [Google Scholar]
- 16. Singer M, Sagong M, van Hemert J, Kuehlewein L, Bell D, Sadda SR.. Ultra-widefield imaging of the peripheral retinal vasculature in normal subjects. Ophthalmology. 2016; 123(5): 1053–1059. [DOI] [PubMed] [Google Scholar]
- 17. Yu H, Luo H, Zhang X, Sun J, Zhong Z, Sun X.. Analysis of white and dark without pressure in a young myopic group based on ultra-wide swept-source optical coherence tomography angiography. J Clin Med. 2022; 11(16): 4830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ye J, Lin J, Shen M, et al.. Reduced radial peripapillary capillary in pathological myopia is correlated with visual acuity. Front Neurosci. 2022; 16: 818530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Wang X, Kong X, Jiang C, Li M, Yu J, Sun X. Is the peripapillary retinal perfusion related to myopia in healthy eyes? A prospective comparative study. BMJ Open. 2016; 6(3): e010791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hwang YH, Yoo C, Kim YY.. Myopic optic disc tilt and the characteristics of peripapillary retinal nerve fiber layer thickness measured by spectral-domain optical coherence tomography. J Glaucoma. 2012; 21: 260–265. [DOI] [PubMed] [Google Scholar]
- 21. Wang T, Li H, Zhang R, Yu Y, Xiao X, Wu C. Evaluation of retinal vascular density and related factors in youth myopia without maculopathy using OCTA . Sci Rep. 2021; 11(1): 15361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Tan NYQ, Sng CCA, Ang M.. Myopic optic disc changes and its role in glaucoma. Curr Opin Ophthalmol. 2019; 30(2): 89–96. [DOI] [PubMed] [Google Scholar]
- 23. Lee SH, Lee EJ, Kim TW.. Comparison of vascular–function and structure–function correlations in glaucomatous eyes with high myopia. Br J Ophthalmol. 2019; 104(6): 807–812. [DOI] [PubMed] [Google Scholar]
- 24. Zhong H, Dong Q, Cun Q, et al.. Peripapillary vessel density correlates with visual field mean sensitivity in highly myopic eyes. J Transl Med. 2022; 20(1): 119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Dervisevic E, Pavljasevic S, Sanja A, et al.. Challenges in early glaucoma detection. Med Arch (Sarajevo, Bosnia and Herzegovina). 2016; 70(3): 203–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Mammo Z, Heisler M, Balaratnasingam C, et al.. Quantitative optical coherence tomography angiography of radial peripapillary capillaries in glaucoma, glaucoma suspect, and normal eyes. Am J Ophthalmol. 2016; 170: 41–49. [DOI] [PubMed] [Google Scholar]
- 27. Tideman JW, Snabel MC, Tedja MS, et al.. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016; 134(12): 1355–1363. [DOI] [PubMed] [Google Scholar]
- 28. Du R, Xie S, Igarashi-Yokoi T, et al.. Continued increase of axial length and its risk factors in adults with high myopia. JAMA Ophthalmol. 2021; 139(10): 1096–1103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Terada N, Murakami T, Ishihara K, et al.. Clinical relevance of parafoveal intercapillary spaces and foveal avascular zone in diabetic retinopathy without macular edema. Invest Ophthalmol Vis Sci. 2022; 63(12): 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Fan Q, Wang H, Jiang Z.. Axial length and its relationship to refractive error in Chinese university students. Cont Lens Anterior Eye. 2022; 45(2): 101470. [DOI] [PubMed] [Google Scholar]
- 31. Pan T, Su Y, Yuan ST, Lu HC, Hu ZZ, Liu QH.. Optic disc and peripapillary changes by optic coherence tomography in high myopia. Int J Ophthalmol. 2018; 11(5): 874–880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Aurora A, Aurora A. Commentary: clinical profile and distribution of peripheral retinal changes in myopic population in a hospital-based study in North India. Indian J Ophthalmol. 2022; 70(4): 1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Chen DZ, Koh V, Tan M, et al.. Peripheral retinal changes in highly myopic young Asian eyes. Acta Ophthalmologica. 2018; 96(7): e846–e851. [DOI] [PubMed] [Google Scholar]