

Abstract
BACKGROUND:
Offspring born to mothers with pre-eclampsia (Pre-E) suffer higher risks of adult cardiovascular diseases, suggesting that exposure to an antiangiogenic environment in-utero has a lasting impact on the development of endothelial function. The goal of this study is to test the hypothesis that in-utero exposure to Pre-E results in alterations of angiogenic factors/cytokines that negatively impact vascular development during infancy.
METHODS:
Infants born from mothers with and without Pre-E were recruited and followed up at 6 months. Plasma cytokines, blood pressure, microvessel density, and vascular reactivity were assessed.
RESULTS:
6-month-old infants born to mothers with Pre-E had unchanged blood pressure (p = 0.86) and microvessel density (p = 0.57). Vascular reactivity was decreased in infants born to mothers with Pre-E compared to infants born to healthy mothers (p = 0.0345). Interleukin 8 (IL-8) (p = 0.03) and Angiopoeitin-2 (Ang-2) (p = 0.04) were increased in infants born to mothers with Pre-E. We observed that higher IL-8 was associated with lower vascular reactivity (rho = −0.14, p < 0.0001).
CONCLUSION:
At 6 months of age, infants born to mothers with Pre-E had impaired vascular reactivity and higher IL-8 and Ang-2, but similar blood pressure and microvessel density compared to infants born to non-Pre-E mothers.
INTRODUCTION
The incidence of pre-eclampsia (Pre-E) affects 6.5–11% of pregnancies in the US.1 The diagnosis of Pre-E is associated with significant long-term morbidity in both mothers and their children.2,3 Several studies found that women with Pre-E have an imbalance in circulating levels of angiogenic and antiangiogenic factors, such as PIGF and soluble FMS-like Tyrosine Kinase-1 (sFlt-1).4–7 These factors were thought to be a major contributor of vascular and endothelial dysfunction in women suffering from Pre-E.8 Likewise, several angiogenic and antiangiogenic factors were found to be altered in the cord blood of infants born to mothers with Pre-E.9–12 As an example, elevated sFlt1/VEGF (Vascular Endothelial Growth Factor) in infants born to mothers with Pre-E was associated with neonatal pulmonary hypertension,9 which is a disease of endothelial dysfunction where pulmonary vasculature fails to relax after birth. These findings suggest that in-utero exposure to an antiangiogenic environment may impede normal endothelial function in the offspring of mothers with Pre-E.
In offspring, smaller studies also showed that infants born to mothers with hypertensive disorders had lower capillary density,13 but did not show a definite association with vascular health in young children.14 In fact, large population studies from Sweden show that offspring born to mothers with Pre-E have an increased risk of ischemic heart disease at young adulthood, and this risk increases with the severity of Pre-E.3,15 Taken together, these observations highlight that the impact of exposure to Pre-E in-utero extends well beyond the neonatal period, where offspring born to mothers with Pre-E continue to exhibit subtle endothelial dysfunction during early childhood and suffer long-term risks of developing cardiovascular disease in young adulthood.
While several studies have reported the immediate impact of Pre-E exposure on angiogenic/anti-angiogenic factors in cord blood, it is unclear how these factors evolve over time during the first 6 months of life. Further, how these changes in angiogenic/anti-angiogenic affect their vascular development are also unclear. The goal of this study is to test the hypothesis that in-utero exposure to Pre-E results in alterations of angiogenic factors/cytokines that negatively impact vascular development of offspring (vascular reactivity, microvascular density, and blood pressure). The current study was performed using clinical data and samples collected from a prior single-center, prospective, observational cohort, where the primary outcome was to assess pulmonary function tests of offspring.16
METHODS
Study population and design
This single-center, prospective, observational cohort study was approved by the Indiana University Institutional Review Board and informed consent was obtained from all mothers of infants participating in the study. The study participants were recruited between 2/2016 to 11/2020 from three hospitals:. Two hospitals (Methodist Hospital and Sidney & Lois Eskenazi Hospital) are in downtown Indianapolis, IN, and include patients with diverse, urban socio-economic, racial, and cultural backgrounds. One hospital (IU North Hospital) is in a suburban area of Indianapolis, IN and has a higher proportion of privately-insured patients. Physicians from Indiana University provide patient care at these three hospitals. Inclusion and exclusion criteria were previously described (NCT02639676).16 Briefly, mothers with a clinical diagnosis of Pre-E (based on definition in the American College of Obstetrics and Gynecology Task Force on Hypertension in Pregnancy 2013 report) with anticipated delivery between 26 and 40-weeks gestational age (GA) determined by best obstetrical dating (last menstrual period or confirmed by ultrasound) were included. A cohort of infants born from normotensive pregnant women with anticipated delivery between 26 and 40-weeks GA were recruited during the same period. Exclusion criteria included multiple gestation pregnancy, prenatally identified fetal cardiopulmonary defects, known fetal chromosomal disorders, women with diabetes (type 1, type 2, or gestational diabetes), and women with chronic or gestational hypertension. The infant offspring returned at six months corrected gestational age for measurement of blood pressure, cutaneous vascular reactivity, and buccal mucosal microvessel density. Venous blood was drawn for cytokine analysis. (Fig. 1a)
Fig. 1. Study cohorts and assessed outcomes.
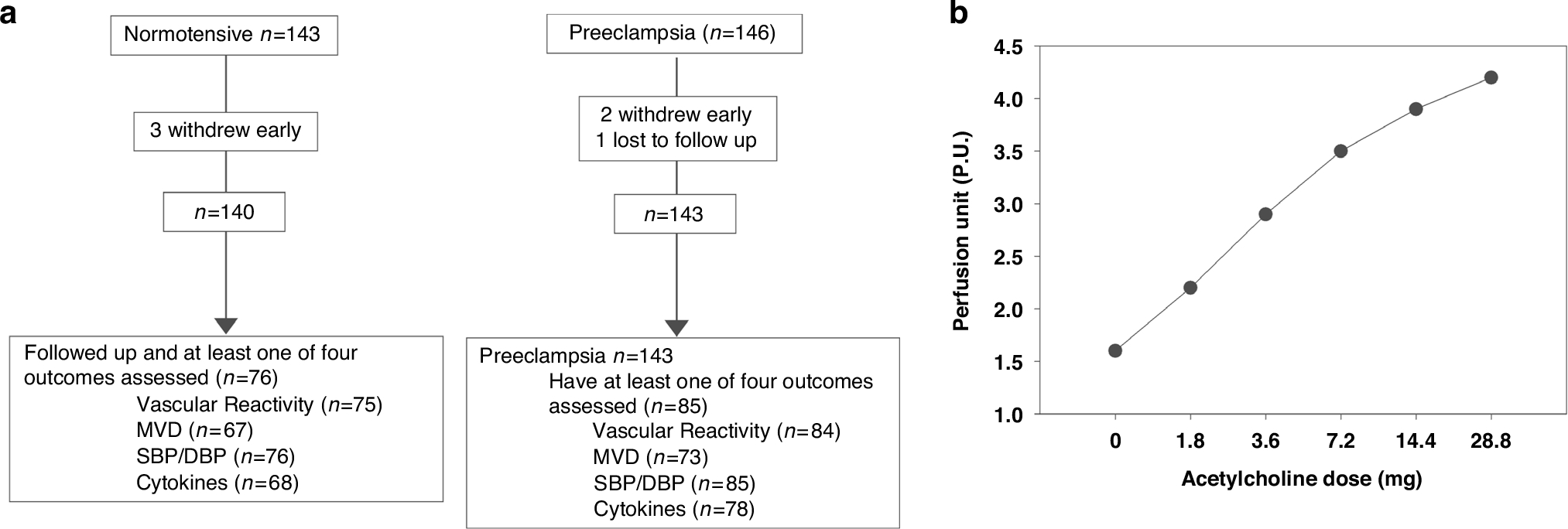
a Numbers of patients enrolled in the study and infants who had outcomes measured. b Representative graph of cutaneous perfusion measured using Periflux System 5000. Perfusion unit was assessed using laser doppler probe at time 0 (baseline), and then followed by Acetylcholine chloride solution delivered via iontophoresis at the rate of 1.8 mg over 10 s. Every 10 sec therefore represents an increment of 1.8 mg in Acetylcholine dose.
Clinical data
Maternal clinical information, such as maternal medications (e.g., antenatal steroids [ANS], magnesium sulfate, other antihypertensive therapies), tobacco use, and family history of asthma were obtained from the electronic medical record. Neonatal clinical information, including birth weight and length, GA at birth, sex, and race were recorded. Infants were categorized into small (SGA), appropriate (AGA), and large (LGA) for gestational age according to a reference published by Kramer et. al.17 Prematurity-related morbidities such as bronchopulmonary dysplasia (BPD), history of mechanical ventilation, and retinopathy of prematurity (ROP) were recorded.
Blood pressure measurement
Infants were held by a parent and received a mild oral sedative (chloral hydrate: 80–100 mg/kg) for pulmonary function testing, which was the primary outcome of the prior study.16 Infants were placed supine on the pulmonary function test table when they were sleeping, and systolic (SBP)/diastolic blood pressure (DBP) was measured in the left upper extremity using an appropriately sized cuff and automatic (oscillometric) equipment (GE Dinamap®, Pro100, Tampa, Florida).
Cutaneous vascular reactivity
Cutaneous perfusion was measured with a laser Doppler probe (Periflux System 5000, Perimed Instruments, Stockholm, Sweden) applied to the dorsal surface of the mid-forearm. Probe temperature was maintained at 32 °C as recommended by the manufacturer and basal cutaneous perfusion was recorded for at least 2 min. Next, Acetylcholine chloride solution 0.18 ml (Ach, 10 mg/ml; Sigma-Aldrich Solutions, Merck KgaA, Darmstadt, Germany) was delivered for 10 s by iontophoresis (Perilont PF 382b, Perimed Instruments). This sequence was repeated with increasing Ach doses, which was obtained by applying the same Ach concentration for longer periods (10, 20, 40, 80, and 160 s), which yielded Ach doses of (1.8, 3.6, 7.2, 14.4, and 28.8 mg), as described previously to assess endothelium-dependent vascular reactivity.18–21 A dose response curve was generated from the maximal perfusion units (PU) measured at 2-minutes following each ACh dose. (Fig. 1b)
Buccal mucosal microvessel density
The mucosal surface of the lower lip was video-imaged using Sidestream Dark Field (SDF) microscopy (Microscan, Microvision Medical©, Amsterdam, Netherlands) as published.22,23 Images were stored for automated analysis using AVA 5.0 (Microvision Medical©), which isolates the vessels by diameter (capillaries <10 micron; small vessels <20 micron; medium vessels >20 to <50 micron) using a beta version that categorized vessel size to <10 microns. A microvessel was defined as any vessel with diameter <20um. Microvessel density (MVD) was calculated by dividing the total length of perfused microvessels (mm) by the area of the analyzed image (mm2). Three separate sites within the lower lip were recorded for each infant and the MVD was expressed as the average of the three sites.
Cytokine analysis
Venous blood plasma samples obtained during the study visit at six months corrected gestational age were analyzed with the Milliplex® MAP Human Angiogenesis Growth Factor Magnetic Bead Panel (HAGP1MAG-12K, Merck KGaA, Darmstadt, Germany) using Luminex software. The 17 analytes included: ET-1, Angiopoietin-2 (Ang-2), Bone morphogenic protein 9 (BMP-9), Endoglin (ENG), VEGF-A, VEGF-C, VEGF-D, Fibroblastic growth factor 1 (FGF-1), Fibroblastic growth factor 2 (FGF-2), Granulocyte colony-stimulating factor (G-CSF), Interleukin-8 (IL-8), Hepatocyte growth factor (HGF), Epidermal growth factor (EGF), Heparin-binding EGF-like growth factor (HB-EGF), Leptin, Placental growth factor (PLGF), and Follistatin. An additional angiogenic factor, VEGFR-1, not included in the panel, was analyzed using the SimpleStep ELISA® kit (Abcam plc ©, Cambridge, UK).
Statistical analysis
Categorical data were analyzed using Chi-Square or Fisher’s exact test. Continuous variables were analyzed using two-sample t-tests or Wilcoxon rank-sum test. For vasoreactivity, a dose-response curve of cutaneous vascular reactivity was analyzed using Generalized Estimating Equations, which models the repeated measures covariance structure and allows for the use of exponential family distributions to accurately model the PU distribution. MVD, SBP, DBP, and cytokines were analyzed utilizing Generalized Linear Models, which also allow for non-normal distributions. Cytokine levels below the level of detection were assigned a value by dividing the minimal detectable concentration of each cytokine by half. If initial modeling of these parameters were non-normal, logarithmic transformations were attempted. Amongst the 17 measured analytes, eight were either undetected in most of the samples or remained non-normally distributed after log-transformation and therefore these analytes were excluded from further analysis. Con and Pre-E comparisons were adjusted for in utero growth restriction, race, sex, and gestational age of patients. Statistical significance was defined as p-value < 0.05. Race was self-reported by the birth mother and dichotomized for analysis as Caucasian vs. non-Caucasian. Secondary analyses evaluating for a relationship between cytokine levels among all infants and either vascular reactivity, BP, or MVD were performed. All analytic assumptions were verified, and analyses were performed using SAS v9.4 (SAS Institute, Cary, NC). As this was a pilot study, we did not have pre-identified sample sizes to identify differences in vascular reactivity, MVD, and cytokine measurements between Con and Pre-E infants.
RESULTS
Demographics
A total of 161 infants (76 Con and 85 Pre-E) from the original cohort of 289 infants had SBP), DBP, MVD, vascular reactivity, or plasma cytokines measured at 6-months of corrected gestational age (Fig. 1a). Of the 85 Pre-E infants, 21 (25%) were born to mothers with mild Pre-E and 64 (75%) were born to mothers with severe Pre-E, categorized according to the criteria published by The American College of Obstetricians and Gynecologists.24 Infants born to mothers with Pre-E were born at a lower gestational age and had a higher rate of small for gestational age, had lower body weight and length at birth and were more affected by in-utero growth restriction (Table 1). There was no difference between Con and Pre-E in head circumference (OFC), sex, maternal race, and antenatal smoke exposure. Given the higher rate of prematurity, infants born to mothers with Pre-E had a higher rate of antenatal corticosteroid exposure and neonatal intensive care unit (NICU) admissions. However, there was no difference in bronchopulmonary dysplasia, retinopathy of prematurity or history of mechanical ventilation.
Table 1.
Clinical characteristics of infants.
| All (n = 289) | Control (n = 143) | Pre-eclampsia (n = 146) | p-value | |
|---|---|---|---|---|
| Gestational age at birth, week (SD) | 36.5 (3.5) | 37.1 (3.6) | 36.0 (3.4) | 0.0057 |
| Gestational age categories, n (%) | ||||
| Small | 45 (15.7) | 14 (9.9) | 31 (21.2) | 0.0188 |
| Normal | 230 (80.1) | 119 (84.4) | 111 (76.0) | |
| Large | 12 (4.2) | 8 (5.7) | 4 (2.7) | |
| Weight, kg (SD) | 2.7 (0.8) | 2.9 (0.7) | 2.5 (0.8) | 0.0003 |
| Length, cm (SD) | 47.0 (5.3) | 47.9 (5.2) | 46.1 (5.2) | 0.0048 |
| OFC, cm (SD) | 31.9 (3.8) | 32.1 (4.2) | 31.8 (3.3) | 0.3859 |
| In-Utero Growth restriction, n (%) | 48 (16.7) | 16 (11.4) | 32 (21.9) | 0.0164 |
| Prematurity, n (%) | 129 (44.8) | 55 (38.7) | 74 (50.7) | 0.0414 |
| Antenatal steroids, n (%) | 130 (45.3) | 55 (39.0) | 75 (51.4) | 0.0354 |
| NICU admission, n (%) | 136 (47.4) | 56 (39.7) | 80 (54.8) | 0.0105 |
| Sex, n (%) | ||||
| Female | 136 (47.2) | 61 (43.0) | 75 (51.4) | 0.1528 |
| Male | 152 (52.8) | 81 (57.0) | 71 (48.6) | |
| Race, n (%) | ||||
| Black | 141 (49.0) | 67 (47.2) | 74 (50.7) | 0.9080 |
| White | 130 (45.1) | 67 (47.2) | 63 (43.2) | |
| Multi | 15 (5.2) | 7 (4.9) | 8 (5.5) | |
| Unknown | 2 (0.7) | 1 (0.7) | 2 (0.7) | |
| Antenatal smoke exposure, n (%) | 66 (22.8) | 33 (23.1) | 33 (22.6) | 0.9235 |
| BPD, n (%) | 8 (2.8) | 2 (1.4) | 6 (4.1) | 0.2827 |
| ROP, n (%) | 9 (3.1) | 3 (2.1) | 6 (4.1) | 0.5014 |
| History of mechanical ventilation, n (%) | 20 (7.0) | 8 (5.7) | 12 (8.2) | 0.3972 |
Values are means (standard deviations) for continuous variables and frequencies (percentages) for categorical variables. P-values are from Student’s t-tests and Chi-Square tests (Fisher’s Exact when 25% of cells have a cell count <5), respectively. OFC Occipital Frontal Circumference, NICU Neonatal intensive Care Unit, BPD Bronchopulmonary Dysplasia, ROP Retinopathy of Prematurity.
Statistically significant p < 0.05 values are in bold.
Pre-E is associated with a modest decrease in vascular reactivity in 6-month-old offspring, but not microvessel density, SBP/DBP
Infants returned at the age of six months corrected gestational age for an assessment of vascular reactivity, microvessel density, and blood pressure measurement. After correcting for gestational age at birth, age at testing, in-utero growth restriction, race, and sex, we found that exposure to Pre-E was not associated with changes in microvessel density (Table 2) and SBP/DBP (Table 3) in offspring. Interestingly, we found that infants born to mothers with Pre-E had a modest decrease in Acetylcholine-induced vascular reactivity (Table 4). Additionally, we found that growth restriction, non-Hispanic White, female, and lower gestational age at birth are factors associated with higher vascular reactivity (Table 4).
Table 2.
Microvessel density.
| Group only | Adjusted Model | |
|---|---|---|
| VR | ||
| Group | ||
| Control | 8.90 (0.23) | 8.94 (0.28) |
| Preeclamptic | 8.69 (0.22) P =.5055 |
8.76 (0.27) P = 0.5557 |
| Growth Restriction | ||
| No | 8.89 (0.17) | |
| Yes | 8.81 (0.42) P = 0.8493 |
|
| Race | ||
| White | 9.04 (0.30) | |
| Non-white | 8.66 (0.25) P = 0.2487 |
|
| Sex | ||
| Female | 9.33 (0.28) | |
| Male | 8.37 (0.27) P = 0.0033 |
|
| Gestational Age | −0.01 (0.05) P = 0.8117 |
|
Values are mm vessel length/mm2 means (standard errors) for categorical variables and slope parameters (standard errors) for continuous variables, with p-values from ANCOVA/Generalized Linear Models.
Statistically significant p-values are in bold.
Table 3.
Blood pressure.
| Group only | Adjusted Model | |
|---|---|---|
| Systolic BP | ||
| Group | ||
| Control | 81.7 (1.1) | 80.3 (1.4) |
| Preeclamptic | 81.2 (1.1) P = 0.7338 |
80.0 (1.3) P = 0.8624 |
| Growth Restriction | ||
| No | 82.2 (0.9) | |
| Yes | 78.2 (2.1) P =.0805 |
|
| Race | ||
| White | 80.7 (1.5) | |
| Non-white | 79.6 (1.2) P =.5131 |
|
| Sex | ||
| Female | 80.5 (1.4) | |
| Male | 79.9 (1.3) P = 0.6986 |
|
| Gestational Age | -0.26 (0.24) P =.2837 |
|
| Diastolic BP | ||
| Group | ||
| Control | 44.6 (0.8) | 43.6 (1.0) |
| Preeclamptic | 45.4 (0.8) P = 0.4710 |
44.7 (0.9) P = 0.3171 |
| Growth Restriction | ||
| No | 45.7 (0.6) | |
| Yes | 42.6 (1.4) P = 0.0549 |
|
| Race | ||
| White | 45.3 (1.0) | |
| Non-white | 43.0 (0.9) P = 0.0493 |
|
| Sex | ||
| Female | 44.9 (1.0) | |
| Male | 43.4 (0.9) P = 0.1924 |
|
| Gestational Age | −0.22 (0.17) P = 0.1924 |
|
Values are mmHg means (standard errors) for categorical variables and slope parameters (standard errors) for continuous variables, with p-values from ANCOVA/Generalized Linear Models.
Statistically significant p-values are in bold.
Table 4.
Vascular reactivity.
| Group only | Adjusted Model | |
|---|---|---|
| VR | ||
| Group | ||
| Control | 3.10 (0.04) | 3.20 (0.04) |
| Preeclamptic | 3.01 (0.03) P = 0.0698 |
3.09 (0.04) P = 0.0345 |
| Dose | 0.53 (0.01) P < 0.0001 |
0.53 (0.01) P < 0.0001 |
| Growth Restriction | ||
| No | 3.05 (0.03) | |
| Yes | 3.24 (0.06) P = 0.0067 |
|
| Race | ||
| White | 3.31 (0.04) | |
| Non-white | 3.00 (0.04) P < 0.0001 |
|
| Sex | ||
| Female | 3.20 (0.04) | |
| Male | 3.08 (0.04) P = 0.0159 |
|
| Gestational Age | −0.02 (0.01) P = 0.0007 |
|
Values are means (standard errors) for categorical variables and slope parameters (standard errors) for continuous variables, with p-values from ANCOVA/Generalized Estimating Equations models.
Statistically significant p-values are in bold.
Pre-E exposure is associated with modest increase in IL-8 and Angiopoietin-2
We next determine the impact of maternal Pre-E exposure on angiogenic factors/cytokines in offspring at 6 months old. Of the 17 measured analytes, 9 cytokines were detectable across all samples and had normal distributions with or without log transformation. We found that infants born to mothers with Pre-E had a modest increase in IL-8 and Angiopoietin-2 in both unadjusted (Fig. 2a, b) and adjusted model (Table 5) (adjusted p-value < 0.05). Finally, VEGFR-1 trended higher in infants born to mothers with Pre-E (P = 0.0678).
Fig. 2. Plasma cytokine levels of infants at 6 months follow up.

Bar graph showing mean ± SEM of a IL-8 and b Angiopoeitin-2 of infants born to control (Con) mothers and mothers with Pre-eclampsia (Pre-E). Each dot represents cytokine level of a patient, *p < 0.05 by regular t-test.
Table 5.
Cytokine Concentrations.
| Con | Pre-E | p-value | |
|---|---|---|---|
| BMP-9 | 0.53 (0.04) | 0.59 (0.03) | P = 0.1417 |
| VEGF-D | 0.19 (0.02) | 0.21 (0.01) | 0.2384 |
| Angiopoietin-2 (log) | 1.36 (0.05) | 1.48 (0.05) | 0.0422 |
| Endoglin (log) | 0.84 (0.05) | 0.93 (0.05) | 0.1793 |
| VEGFR-1 (log) | −2.16 (0.34) | −1.45 (0.31) | 0.0678 |
| VEGF-c (log) | 0.06 (0.06) | −0.02 (0.07) | 0.3862 |
| IL-8 (log) | −5.40 (0.11) | −5.12 (0.10) | 0.0298 |
| Follistatin (log) | 0.23 (0.10) | 0.16 (0.09) | 0.7995 |
| HB-EGF (log) | −3.67 (0.08) | −3.68 (0.07) | 0.9262 |
Values are means of concentration (ug/mL) (standard errors), with p-values from ANCOVA/Generalized Estimating Equations models, adjusted for growth restriction, race, sex, and gestational age.
Statistically significant p-values are in bold.
IL-8 was negatively associated with offspring vascular reactivity
In secondary analyses assessing cytokine levels and vascular reactivity, we sought to determine the correlation between the levels of IL-8, Ang-2, and VEGFR-1, as well as whether these cytokines correlate with vascular reactivity. We performed Spearman Correlation analysis to evaluate for a relationship between these three cytokines (Fig. 3a–c). No correlation between VEGFR-1 with IL-8 (rho = 0.1096, p = 0.1880) or Ang-2 (rho = 0.0800, p = 0.3369) was identified. A significant, but weak association was found between IL-8 and Ang-2 (rho = 0.2601, p = 0.0015), suggesting that these cytokines may be mechanistically associated. Upon comparing these cytokines with vascular reactivity, we found that only IL-8 had a significant negative association with vascular reactivity (−0.14, P < 0.0001). There were no associations between Ang-2 (−0.04, p = 0.5665) or VEGFR-1 (−0.001, p = 0.9024) with vascular reactivity.
Fig. 3. Spearman Correlation demonstrating association between different cytokines.

a Correlation between IL-8 with VEGFR-1 (rho = 0.1096, p = 0.1880). b Correlation between VEGFR-1 with Ang-2 (rho = 0.0800, p = 0.3369). c Correlation between IL-8 with Ang-2 (rho = 0.2601, p = 0.0015). black circles represent data from Con infants, open circles represent data from Pre-E infants.
DISCUSSION
This is the first study to our knowledge that evaluated the association between angiogenic factors/cytokines and vascular health (vascular reactivity, MVD, SBP/DBP) in offspring at the age of 6 months. The demographic data indicate that infants born to mothers with Pre-E are more likely preterm with lower birthweight and have experienced intrauterine growth restriction, which is consistent with previous studies.25–29 Many of these factors were colinear (e.g. prematurity status with gestational age, birthweight, NICU admission etc), therefore, we selected factors with the highest significance and impact as covariates for adjustment. After correcting for important covariates, we detected a modest decrease in vascular reactivity, while MVD and blood pressure were not statistically different between Pre-E and Con offspring. This is an important finding that indicates that these apparently healthy infants, with normal blood pressure, begin exhibiting changes in vascular vasodilatation in response to acetylcholine within the first year of life. A lower acetylcholine-induced vascular reactivity has been associated with prehypertension30 and may result in hypertension.31 These findings are also consistent with numerous metanalyses reporting the higher risks of developing vascular/cardiovascular diseases in offspring born to mothers with Pre-E during late childhood or young adulthood.3,15
Our initial hypothesis was that exposure to Pre-E results in alterations of angiogenic factors/cytokines that negatively impact the vascular development of offspring. We discovered that IL-8 and angiopoetin-2 were elevated in infants born to mothers with Pre-E.7,32,33 IL-8 is a pro-inflammatory cytokine that acts as a chemoattractant and induces mitosis of vascular smooth muscle cells as well as promotes angiogenesis.34,35 In a large case-control study with over 2300 patients, IL-8 was associated with increased risks of developing fatal and non-fatal coronary artery disease in otherwise healthy men and women.36 IL-8 was also found to be three times higher in pregnant mothers with Pre-E compared to healthy control pregnant mothers.37 These studies demonstrate the potential role of IL-8 as a biomarker for cardiovascular health in adults and in pregnant mothers. In preterm infants, elevated IL-8 has been associated with bronchopulmonary dysplasia or death.38 Angiopoetin-2 is a growth factor that is known to regulate angiogenesis.39 In adults, elevated Angiopoetin-2 levels are capable of predicting arterial stiffness, diastolic heart failure, and cardiovascular risks in patients with hypertension.40,41 Likewise, the role of Angiopoetin-2 in offspring of mothers with Pre-E has not been studied, but elevated levels in tracheal aspirates from preterm infants is also associated with the development of bronchopulmonary dysplasia.42 Taken together, increased IL-8 and Angiopoetin-2 levels along with decreased acetylcholine-induced vasodilation in young infants exposed to Pre-E in utero suggest an elevated risk for development of future vascular diseases. Such findings warrant close follow up of infants’ blood pressure as well as the need for studies to understand mechanisms contributing to endothelial dysfunction in these offspring.
This study has several strengths and limitations. A strength of our study is that infants were assessed at 6 months corrected gestational age, allowing us to evaluate whether vascular impairment is present past the newborn period, increasing the potential to persist into adulthood. Another strength is that we evaluated vascular development and function using multiple non-invasive modalities in addition to blood pressure to identify earlier evidence of reduced vascular health. Additionally, we evaluated for relationships between vasoreactivity and angiogenic factors, which may provide preliminary data for future mechanistic and biomarker studies. A limitation of our study is no differences in BP were detected, which is the gold standard measurement for hypertension diagnosis and a clinically actionable outcome. However, the absence of a difference may reflect the very young age which the subjects were evaluated and the low prevalence of systemic hypertension in this age group.43,44 The lack of differences in MVD is potentially methodologic. While the technology used for buccal MVD assessment had good interobserver reproducibility,45 newer generation of dark field microscopy equipment can visualize approximately 20% more vessels in preterm infants.46 In addition, we were limited to the assessment of baseline MVD of buccal mucosa, in contrast to the evaluation of older cooperative subjects that can use the re-perfusion technique to obtain maximal MVD. Lastly, the number of infants evaluated at 6 months corrected gestational age limits the power to assess and detect associations of subgroups, such impact of mild- versus severe Pre-E.
CONCLUSION
In summary, Pre-E is associated with a modest decrease in infant vascular reactivity, increased levels of IL-8 and Angiopoetin-2, and an association between vasoreactivity and these cytokines at 6 months corrected gestational age. Our study suggests that vascular reactivity may be an early pathophysiologic indicator associated with Pre-E exposure, however, the underlying mechanisms regulating this altered vascular reactivity remain unknown. Future studies should aim to delineate the relationship between elevated IL-8 and Angiopoietin-2 during early infancy and the impairments in vascular reactivity. In addition, further studies are required to determine if vascular diseases, such as hypertension, at an older age are related to reduced vascular reactivity early in life. Additional assays specifically designed for biomarker discovery could also inform novel circulating molecules that may serve as disease biomarkers and targets for intervention.
IMPACT STATEMENT:
Changes in cord blood antiangiogenic factors are documented in infants of mothers with pre-eclampsia and may contribute to offspring risks of adult cardiovascular disease. How these factors evolve during early infancy and their correlation with offspring vascular development have not been studied.
This study found that 6-month-old infants born to mothers with pre-eclampsia had decreased vascular reactivity, which was correlated with higher IL-8.
These findings underscore the lasting impact of maternal pre-eclampsia on offspring vascular development and highlight the need for long-term follow-up in children born to mothers with pre-eclampsia.
ACKNOWLEDGEMENTS
The authors thank the Multiplex Analysis Core at the Indiana University Melvin and Bren Simon Comprehensive Cancer Center for providing support in analyzing samples and interpretation of data.
FUNDING
This study is supported by R01HL122215 (R.S.T, L.S.H), K08HD109636 (K.L.K), March of Dimes Basil O’Connor Award (K.L.K).
Footnotes
COMPETING INTERESTS
The authors declare no competing interests.
Reprints and permission information is available at http://www.nature.com/reprints
Consent statement Patient consent was obtained prior to enrollment as described in methods section.
DATA AVAILABILITY
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
REFERENCES
- 1.Boakye E et al. Nativity-related disparities in preeclampsia and cardiovascular disease risk among a racially diverse cohort of US Women. JAMA Netw. Open 4, e2139564 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Irgens HU, Reisæter L, Irgens LM & Lie RT Long term mortality of mothers and fathers after pre-eclampsia: population based cohort study. BMJ 323, 1213–1217 (2001). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang L et al. Maternal hypertensive disorders during pregnancy and the risk of offspring diabetes mellitus in childhood, adolescence, and early adulthood: a nationwide population-based cohort study. BMC Med. 21, 59 (2023). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hecht JL et al. The pathology of eclampsia: An autopsy series. Hypertens. Pregnancy 36, 259–268 (2017). [DOI] [PubMed] [Google Scholar]
- 5.Weel IC et al. Association between placental lesions, cytokines and angiogenic factors in pregnant women with Preeclampsia. PLoS ONE 11, e0157584 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Clark DE et al. A vascular endothelial growth factor antagonist is produced by the human placenta and released into the maternal circulation. Biol. Reprod. 59, 1540–1548 (1998). [DOI] [PubMed] [Google Scholar]
- 7.Tangerås LH et al. Distinct first trimester cytokine profiles for gestational hypertension and preeclampsia. Arterioscler. Thromb. Vasc. Biol. 35, 2478–2485 (2015). [DOI] [PubMed] [Google Scholar]
- 8.Tomimatsu T et al. Preeclampsia: Maternal systemic vascular disorder caused by generalized endothelial dysfunction due to placental antiangiogenic factors. Int. J. Mol. Sci. 20, 4246 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Heath-Freudenthal A et al. Vascular disorders of pregnancy increase susceptibility to neonatal pulmonary hypertension in high-altitude populations. Hypertens. Dallas Tex. 1979 79, 1286–1296 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vinayagam V, Bobby Z, Habeebullah S, Chaturvedula L & Bharadwaj SK Maternal and cord blood plasma sEng and TGF-β1 in patients with hypertensive disorders of pregnancy: a pilot study in a South. Indian Popul. J. Clin. Diagn. Res. JCDR 11, QC32–QC34 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kim D-H, Shin SH, Kim E-K & Kim H-S Association of increased cord blood soluble endoglin with the development of bronchopulmonary dysplasia in preterm infants with maternal preeclampsia. Pregnancy Hypertens. 13, 148–153 (2018). [DOI] [PubMed] [Google Scholar]
- 12.Sezer SD et al. Comparison of angiogenic and anti-angiogenic factors in maternal and umbilical cord blood in early- and late-onset pre-eclampsia. Gynecol. Endocrinol. J. Int. Soc. Gynecol. Endocrinol. 28, 628–632 (2012). [DOI] [PubMed] [Google Scholar]
- 13.Antonios TFT et al. Capillary remodeling in infants born to hypertensive pregnancy: pilot study. Am. J. Hypertens. 25, 848–853 (2012). [DOI] [PubMed] [Google Scholar]
- 14.Varley BJ et al. Intrauterine exposure to preeclampsia does not impair vascular health in children. Front. Public Health 10, 1071304 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nahum Sacks K et al. Prenatal exposure to preeclampsia as an independent risk factor for long-term cardiovascular morbidity of the offspring. Pregnancy Hypertens. 13, 181–186 (2018). [DOI] [PubMed] [Google Scholar]
- 16.Ren CL et al. Forced expiratory flows and diffusion capacity in infants born from mothers with pre-eclampsia. Pediatr. Pulmonol. 57, 2481–2490 (2022). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kramer MS et al. A new and improved population-based Canadian reference for birth weight for gestational age. Pediatrics 108, E35 (2001). [DOI] [PubMed] [Google Scholar]
- 18.Acosta JC et al. Gestational diabetes mellitus alters maternal and neonatal circulating endothelial progenitor cell subsets. Am. J. Obstet. Gynecol. 204, 254.e8–254.e15 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.DiMeglio LA et al. Endothelial abnormalities in adolescents with type 1 diabetes: a biomarker for vascular sequelae? J. Pediatr. 157, 540–546 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Martin H, Gazelius B & Norman M Impaired acetylcholine-induced vascular relaxation in low birth weight infants: implications for adult hypertension? Pediatr. Res. 47, 457–462 (2000). [DOI] [PubMed] [Google Scholar]
- 21.Krispinsky LT et al. Endothelial-dependent vasomotor dysfunction in infants after cardiopulmonary bypass. Pediatr. Crit. Care Med. J. Soc. Crit. Care Med. World Fed. Pediatr. Intensive Crit. Care Soc. 21, 42–49 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hubble SMA, Kyte HL, Gooding K & Shore AC Variability in sublingual microvessel density and flow measurements in healthy volunteers. Microcirculation 16, 183–191 (2009). [DOI] [PubMed] [Google Scholar]
- 23.Bezemer R et al. Rapid automatic assessment of microvascular density in sidestream dark field images. Med. Biol. Eng. Comput. 49, 1269–1278 (2011). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hypertension in Pregnancy: Executive Summary. Obstet. Gynecol. 122, 1122 (2013). [DOI] [PubMed] [Google Scholar]
- 25.Källén B, Finnström O, Nygren K-G & Olausson PO Association between preterm birth and intrauterine growth retardation and child asthma. Eur. Respir. J. 41, 671–676 (2013). [DOI] [PubMed] [Google Scholar]
- 26.Nakimuli A et al. Relative impact of pre-eclampsia on birth weight in a low resource setting: A prospective cohort study. Pregnancy Hypertens. 21, 1–6 (2020). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Xiong X, Demianczuk NN, Saunders LD, Wang F-L & Fraser WD Impact of preeclampsia and gestational hypertension on birth weight by gestational age. Am. J. Epidemiol. 155, 203–209 (2002). [DOI] [PubMed] [Google Scholar]
- 28.Liu Y et al. Impact of gestational hypertension and preeclampsia on low birthweight and small-for-gestational-age infants in China: A large prospective cohort study. J. Clin. Hypertens. 23, 835–842 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yang Y et al. Preeclampsia prevalence, risk factors, and pregnancy outcomes in Sweden and China. JAMA Netw. Open 4, e218401 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Weil BR, Stauffer BL, Greiner JJ & DeSouza CA Prehypertension is associated with impaired nitric oxide-mediated endothelium-dependent vasodilation in sedentary adults. Am. J. Hypertens. 24, 976–981 (2011). [DOI] [PubMed] [Google Scholar]
- 31.Stockelman KA et al. Negative influence of insufficient sleep on endothelial vasodilator and fibrinolytic function in hypertensive adults. Hypertension 78, 1829–1840 (2021). [DOI] [PubMed] [Google Scholar]
- 32.Cemgil Arikan D, Aral M, Coskun A & Ozer A Plasma IL-4, IL-8, IL-12, interferon-γ and CRP levels in pregnant women with preeclampsia, and their relation with severity of disease and fetal birth weight. J. Matern. -Fetal Neonatal Med. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 25, 1569–1573 (2012). [DOI] [PubMed] [Google Scholar]
- 33.Han SY, Jun JK, Lee C-H, Park JS & Syn HC Angiopoietin-2: a promising indicator for the occurrence of severe preeclampsia. Hypertens. Pregnancy 31, 189–199 (2012). [DOI] [PubMed] [Google Scholar]
- 34.Yue TL et al. Interleukin-8. A mitogen and chemoattractant for vascular smooth muscle cells. Circ. Res. 75, 1–7 (1994). [DOI] [PubMed] [Google Scholar]
- 35.Li A, Dubey S, Varney ML, Dave BJ & Singh RK IL-8 directly enhanced endothelial cell survival, proliferation, and matrix metalloproteinases production and regulated Angiogenesis1. J. Immunol. 170, 3369–3376 (2003). [DOI] [PubMed] [Google Scholar]
- 36.Boekholdt SM et al. IL-8 plasma concentrations and the risk of future coronary artery disease in apparently healthy men and women. Arterioscler. Thromb. Vasc. Biol. 24, 1503–1508 (2004). [DOI] [PubMed] [Google Scholar]
- 37.Szarka A, Rigó J, Lázár L, Bekő G & Molvarec A Circulating cytokines, chemokines and adhesion molecules in normal pregnancy and preeclampsia determined by multiplex suspension array. BMC Immunol. 11, 1–9 (2010). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ambalavanan N et al. Cytokines associated with bronchopulmonary dysplasia or death in extremely low birth weight infants. Pediatrics 123, 1132–1141 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Akwii RG, Sajib MS, Zahra FT & Mikelis CM Role of Angiopoietin-2 in vascular physiology and pathophysiology. Cells 8, 471 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Patel JV, Lim HS, Varughese GI, Hughes EA & Lip GYH Angiopoietin-2 levels as a biomarker of cardiovascular risk in patients with hypertension. Ann. Med. 40, 215–222 (2008). [DOI] [PubMed] [Google Scholar]
- 41.Medvedeva TA & Kushnarenko NN Angiopoietin-2 is a new predictor of arterial stiffness and diastolic heart failure in gouty patients with arterial hypertension. Atherosclerosis 331, e229 (2021). [Google Scholar]
- 42.Aghai ZH et al. Angiopoietin 2 concentrations in infants developing bronchopulmonary dysplasia: attenuation by dexamethasone. J. Perinatol. J. Calif. Perinat. Assoc. 28, 149–155 (2008). [DOI] [PubMed] [Google Scholar]
- 43.Dionne JM, Abitbol CL & Flynn JT Hypertension in infancy: diagnosis, management and outcome. Pediatr. Nephrol. Berl. Ger. 27, 17–32 (2012). [DOI] [PubMed] [Google Scholar]
- 44.Flynn JT et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140, e20171904 (2017). [DOI] [PubMed] [Google Scholar]
- 45.van den Berg VJ et al. Reproducibility of microvascular vessel density analysis in Sidestream dark-field-derived images of healthy term newborns. Microcirc. N. Y. N. 1994 22, 37–43 (2015). [DOI] [PubMed] [Google Scholar]
- 46.van Elteren HA, Ince C, Tibboel D, Reiss IKM & de Jonge RCJ Cutaneous microcirculation in preterm neonates: comparison between sidestream dark field (SDF) and incident dark field (IDF) imaging. J. Clin. Monit. Comput. 29, 543–548 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.