

Abstract
Objective
Syringe irrigation, commonly used for delivering sodium hypochlorite (NaOCl) during root canal treatment, requires careful handling to prevent NaOCl extrusion into periapical tissues. This randomised controlled in vitro study aimed to quantify syringe plunger forces exerted by dental undergraduates and to assess the impact of an educational intervention on adherence to safe irrigant delivery parameters.
Methods
Fifty-two undergraduates performed syringe irrigation at three intervals: baseline (T1), after two weeks (T2), and after 12 weeks (T3). At T1, irrigation was conducted without prior educational intervention, while at T2, it was preceded by an intervention. The educational intervention involved a short video highlighting safe irrigation practices, including plunger force and time recommendations for syringe irrigation. At T3, the undergraduates were randomly allocated to two groups: One received a repeated intervention, while the other did not. Syringe irrigation was performed on a 3D-printed tooth using two side-vented cannulas: one of 25 Gauge (G) and another of 30 G. A syringe equipped with a force sensor recorded the plunger forces. Based on earlier research, plunger forces exceeding 10 Newtons (N) for the 25 G cannula and 40 N for the 30 G cannula were deemed critical. The data were subjected to descriptive statistical analyses.
Results
Overall, the mean of maximum values of plunger forces remained under 10 N for the 25 G and below 20 N for the 30 G cannulas, with only a few measurements exceeding 40 N. Instances of surpassing the critical plunger force threshold were more common with the 25 G side-vented cannula than with the 30 G variant. At T3, the group that received the repeated educational intervention exhibited lower average maximum plunger forces for both cannulas than the group that did not receive the intervention.
Conclusion
Integrating plunger force measurements with targeted educational interventions presents an effective approach for instructing undergraduates in the proper techniques of syringe irrigation. The findings suggest that, generally, undergraduates do not apply excessive plunger forces that could risk apical irrigant extrusion. Implementing repeated educational interventions decreased the plunger forces exerted by undergraduates, underscoring its effectiveness in fostering safe endodontic irrigation.
Keywords: Dental education, endodontic education, NaOCl, root canal treatment, sodium hypochlorite accident, undergraduate education
HIGHLIGHTS
A repeated educational intervention lowers the plunger and forces undergraduates to apply it during syringe irrigation.
Undergraduates rarely exert plunger forces that exceed critical levels.
The magnitude of the applied plunger forces varies depending on the type of cannula used.
INTRODUCTION
To achieve a favourable outcome in endodontic treatment, microbial load within the root canal system should be substantially reduced (1). Irrigation is key in disinfection and chemo-mechanical preparation during root canal treatment (2–4). Sodium hypochlorite (NaOCl) is the most widely used and most effective irrigant (5–8). Its capacity to dissolve vital and necrotic tissue and its efficiency in eliminating endodontic pathogens underscores its importance in endodontic therapy (7, 9, 10).
However, NaOCl also exhibits cytotoxic effects when in contact with healthy tissue (11). If NaOCl is extruded into the periapical area, it can adversely affect these tissues due to its oxidising properties (12). Such extrusions can lead to specific signs and symptoms, commonly referred to as NaOCl accidents (13, 14). Though these accidents are infrequent in clinical practice, they can have severe implications for the patients involved (15). Reported symptoms of NaOCl accidents in case studies include intense pain, bleeding from the root canal, facial swelling, ecchymosis, oedema, skin ulcers, a chlorine-like odour in the nose, throat irritation, anaesthesia, paraesthesia, and respiratory difficulties (13, 14). These signs and symptoms usually subside within a month. However, in cases where NaOCl accidents result in nerve damage, paraesthesia or a permanent loss of sensory function may persist (14). Therefore, irrigation with NaOCl should be meticulously controlled to ensure it remains confined to the root canal system and prevent any extrusion beyond the apical constriction.
Though the precise apical pressure threshold required for apical irrigant extrusion remains uncertain, the central venous pressure (mean: 5.88 mmHg ± standard deviation of 0.15 mmHg) is often cited as a critical benchmark (16–21). It is likely that the critical value for extrusion of sodium hypochlorite varies among individuals and may be influenced by several factors, including sex and the presence of periapical pathology (22, 23).
Syringe irrigation remains the predominant method for irrigant delivery in root canal therapy (6). The pressure generated during syringe irrigation is partially influenced by the dental practitioner (22). Factors such as the force applied to the syringe plunger, the depth of cannula insertion, wedging of the cannula in the root canal and the type and diameter of the cannula are determinants of the pressure generated in the apical region, influencing the risk of apical extrusion (18, 24–30).
A recent laboratory study comprehensively assessed apical pressures during syringe irrigation, highlighting the significance of plunger force (20). Based on these findings, recommendations were formulated for safe irrigant delivery using a 5 mL syringe combined with various cannula types (20). When employing a 30 G cannula, plunger forces under 40 Newtons (N) are deemed safe (20). Conversely, with 25 G cannulas, limiting the applied force to a maximum of 10 N is advisable to avoid the risk of NaOCl extrusion (20). These guidelines are instrumental in enhancing the safety and efficacy of syringe irrigation in endodontic treatment.
Given the crucial role of dental practitioners in ensuring safe irrigant delivery, it is imperative to educate dental undergraduates on avoiding NaOCl accidents by instructing them on safe irrigant delivery parameters. However, currently, there is a lack of evidence regarding dental education in syringe irrigation. Therefore, this randomised controlled in vitro study, conducted in an established laboratory setup, aims to collect data on the syringe plunger forces exerted by undergraduates. Additionally, this study aims to assess the impact of an educational intervention, specifically an instructional video, on adherence to the parameters necessary for safe irrigant delivery in endodontic patient care.
MATERIALS AND METHODS
Ethical Approval and Informed Consent
An approval of University of Basel research protocols by the Ethics Committee in accordance with international agreements (Declaration of Helsinki) was not required as the study did not involve patients or patients’ data. It was conducted following the regulatory requirements of the Swiss Human Research Act and Human Research Ordinance. Informed consent was obtained from all participating undergraduate dental students who joined the study voluntarily. They consented to using the data generated for research and educational purposes. This study, conducted without mandatory attendance, was integrated into the undergraduates’ regular endodontics course. Participation and performance in this study did not impact the students’ assessment or grading in the course.
Study Design and Cohort
The study cohort comprised 24 third-year and 28 fourth-year dental undergraduates. Before the study, the third-year undergraduates had not received any preclinical training in endodontics. The fourth-year undergraduates had undergone two months of preclinical endodontic training, which included eight 4-hour supervised sessions and seven 2.5-hour sessions without supervision dedicated to primary root canal treatment.
The participants were tasked with performing endodontic irrigation at three different time points: at baseline (T1), after a two-week interval (T2), and following a 12-week period (T3). The initial irrigation procedure at T1 was conducted without any prior educational intervention. At T2, all participants received an educational intervention before performing endodontic irrigation. To evaluate the impact of repeated educational intervention, the participants were randomly split into two groups of almost equal size at T3, using an online tool (randomizer.org). At T3, one group received the educational intervention again before their irrigation experiments, while the other group did not undergo a further intervention. This study design is illustrated in Figure 1.
Figure 1.
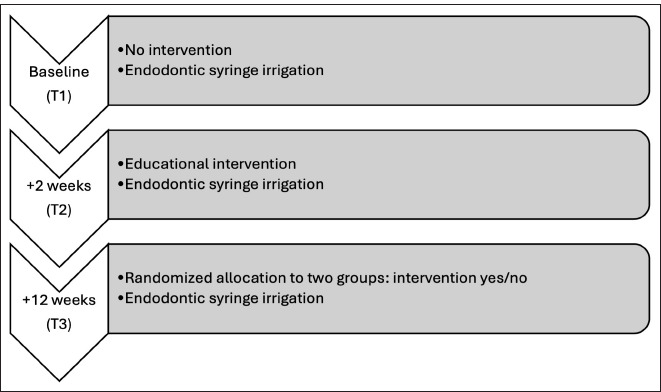
Study flow diagram
Syringe Irrigation without Educational Intervention (T1)
To assess the forces applied to the plunger of irrigation syringes, the undergraduates were tasked with performing syringe irrigation using 5 mL syringes (Omnifix Solo, B. Braun Medical AG, Sempach, Switzerland) coupled with two different types of cannulas, a 25 Gauge (G) side-vented cannula and a 30 G side-vented cannula (Dental Needle Tips, KerrHawe SA, Bioggio, Switzerland). The only guidance provided to the undergraduates regarding the cannula positioning at 1 mm short of the working length, with no advice on appropriate plunger force or recommended time for emptying the syringe. Additionally, no timekeeping devices, such as clocks or stopwatches, were accessible to the students during irrigation.
A 3D-printed tooth, modelled from micro-computed tomography imaging data of an immature tooth #21, was mounted in the oral cavity of a dental training manikin (P-6, Frasaco, Tettnang, Germany). This tooth, measuring 17 mm long, featured an ideal access cavity and an empty root canal. The undergraduates performed syringe irrigation by positioning the cannula 1 mm short of the working length, i.e., at 16 mm. They performed the task twice for each cannula type. The supervisor stopped the undergraduates after performing irrigation for at least 10 s. Tap water served as the irrigant.
For these experiments, the syringe plunger was equipped with a force sensor (KM25, Transmetra, Flurlingen, Switzerland). This sensor, capable of recording forces ranging from 0 N to 100 N, was connected to a measurement amplifier (GM40, Lorenz Messtechnik, Alfdorf, Germany) via a data cable. The amplifier relayed the signals of the force sensor to an analogue-digital converter (12 bit, RedLab 1208FS USB Mini-Messlabor, Meilhaus Electronic, Alling, Germany), which then transmitted the digitized data to a personal computer. The data were processed using laboratory software (LabVIEW, International Instruments, Austin, TX, USA) equipped with a customized program. The force range for each experiment was recorded. The screen displaying these measurements remained concealed from the participants throughout the experimental procedures.
Syringe Irrigation with Prior Educational Intervention (T2)
The participants were shown an educational video two weeks after the initial measurements. The video is accessible in an open repository (31). This video emphasized the fundamentals of safe irrigation practices, incorporating evidence-based guidelines on appropriate plunger forces and the required time for safe irrigant delivery. The undergraduates watched this instructional video, which lasted 4 min and 54 s, back-to-back. The specific content of the educational video is detailed in Tables 1 and 2.
TABLE 1.
Educational video content on safe syringe irrigation: General guidelines and safety practices (18, 22, 25, 34)
|
TABLE 2.
Educational video content on safe syringe irrigation: Recommended parameters for conventional irrigation with a 5 mL syringe (20)
| Recommended parameters for irrigation with a 5 mL syringe (20) | |||
|---|---|---|---|
| Cannula | Type | Plunger force (N) | Irrigant delivery gauge duration (s) |
| 25 G | Side-vented | 10 | ≥21 |
| 25 G | Open-vented | 10–20 | ≥18 |
| 30 G | Side-vented | 10–40 | ≥38 |
| 30 G | Open-vented | 10–40 | ≥30 |
N: Newton, G: Gauge
Immediately after watching the video, the undergraduates repeated the same irrigation experiments as in the first round. The experimental setup remained the same, except that the participants now had access to a clock and a stopwatch at their workstation, enabling them to monitor the time spent on each irrigation procedure. This addition aimed to assist the undergraduates in adhering more closely to the recommended irrigation parameters, per the instructions in the educational video.
Syringe Irrigation with and without Prior Repetition of the Educational Intervention (T3)
Twelve weeks after the initial round of measurements, the participants were randomly divided into two groups. One-half of the undergraduates were again shown the instructional video before conducting the irrigation experiments. The remaining half performed the irrigation experiments without re-watching the video.
The experimental setup for the syringe irrigation tasks remained consistent with the previous rounds. All undergraduates had access to a clock and stopwatch at their workstations, allowing them to time their irrigation procedures. The investigator responsible for recording the measurements was blinded to the group allocations to avoid observer bias.
Statistical Analysis
Descriptive statistical analyses were conducted using the higher of the two plunger force measurements obtained in each trial. The mean of the maximum values, the 95% confidence intervals and the percentage exceeding the critical plunger forces were subjected to the analysis. Critical forces were defined as exceeding 10 Newtons (N) for 25 G side-vented cannulas and 40 N for 30 G side-vented cannulas, with forces beyond these limits potentially leading to NaOCl extrusion. An unblinded investigator performed all statistical analyses using SPSS (version 28.0, IBM, Armonk, NY, USA). The data collected and processed during this study are accessible in an open repository (31).
RESULTS
Overall, most of the maximum plunger forces were below 20 N at each time point (T1-T3) across both groups, whether they had an additional educational intervention or not (Figs. 2, 3). A few instances of forces exceeding 40 N were recorded (Figs. 2, 3). In terms of year-specific differences, fourth-year undergraduates showed similar plunger forces over time (T1-T3), whereas third-year undergraduates exhibited more variability in their applied forces from T1 to T3 (Fig. 2).
Figure 2.
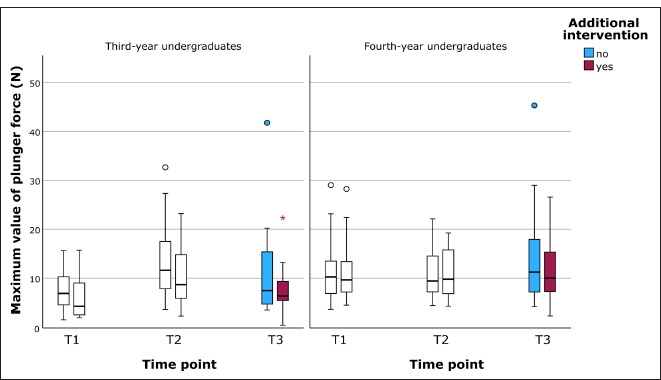
Distribution of the maximum values of the plunger forces in the third and fourth study years across different time points (T1-T3) and groups (additional intervention: yes/no)
N: Newton
Figure 3.
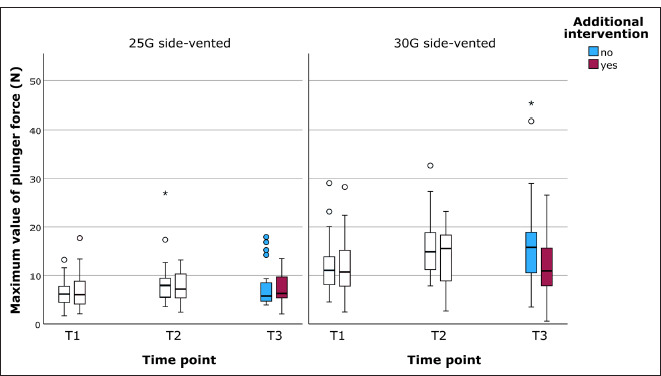
Distribution of the maximum values of the plunger forces for both cannulas across different time points (T1-T3) and groups (additional intervention: yes/no)
The applied plunger force was found to be dependent on the type of cannula used. The 25 G side-vented cannula showed lower applied force compared with the 30 G side-vented cannula (Fig. 3).
Overall, the 25 G side-vented cannula led more frequently to an exceedance of the critical plunger force compared with the 30 G side-vented cannula (Table 3). The mean of the maximum plunger force was lower in the group with the intervention compared with the group with no intervention at T3 for both cannulas (Table 3). The critical plunger pressure using the 30 G side-vented cannula was only exceeded in two measurements (both third-year undergraduates, T3 without intervention) (Table 3).
TABLE 3.
Descriptive analysis of plunger forces per study year, time point and group (repeated intervention)
| Group | RI | n | Cannula type | |||||
|---|---|---|---|---|---|---|---|---|
| 30 G side-vented cannula | 25 G side-vented cannula | |||||||
| Mean (N) | 95% CI (N) | n > 40 N (%) | Mean (N) | 95% CI (N) | n >10 N (%) | |||
| 3rd | N/A | 72 | 12.0 | 10.3–13.7 | 2 (2.8%) | 6.6 | 5.7–7.6 | 11 (15.3%) |
| 4th | N/A | 84 | 15.3 | 13.9–16.7 | 0 (0%) | 7.9 | 7.2–8.5 | 16 (19.1%) |
| T1 | N/A | 52 | 11.9 | 10.3–13.6 | 0 (0%) | 6.5 | 5.6–7.4 | 7 (13.5%) |
| T2 | N/A | 52 | 14.8 | 13.1–16.4 | 0 (0%) | 8.1 | 7.0–9.2 | 12 (23.1%) |
| T3 | Yes | 25 | 12.4 | 9.7–15.0 | 0 (0%) | 7.1 | 5.9–8.3 | 4 (16.0%) |
| No | 27 | 16.6 | 12.8–20.4 | 2 (7.4%) | 7.5 | 5.9–9.1 | 4 (14.8%) | |
Data are presented as the mean of the maximum plunger forces, the corresponding 95% CI, and the number of undergraduates producing forces above the critical threshold of 10 N for the side-vented 25 G cannula and 40 N for the side-vented 30 G cannula. CI: Confidence interval, N: Newton, G: Gauge, RI: Repeated intervention, n: Number, T: Time point, N/A: Not applicable
Using the 25 G side-vented cannula, the fourth-year undergraduates produced more critical pressures than the third-year undergraduates. At T2, almost a quarter of all undergraduates produced plunger forces exceeding the critical value. At T1 and T3, the measured forces exceeded the critical value in fewer cases than in T2.
DISCUSSION
This randomised controlled study aimed to quantitatively assess the syringe plunger forces applied in conventional root canal irrigation and to examine the impact of an educational intervention on these forces among dental undergraduates. The findings demonstrate that irrespective of educational intervention, dental undergraduates rarely exert syringe plunger forces exceeding 40 N. Notably, an educational intervention conducted two weeks following the initial measurements led to increased plunger forces, in contrast to the baseline forces observed without intervention. A subsequent educational intervention with one group after 12 weeks reduced syringe plunger forces compared to the group that did not receive a second intervention. This indicates a nuanced effect of educational interventions on the application of plunger force in syringe irrigation, suggesting the potential for adjustments in educational approaches to optimise clinical techniques among undergraduates.
The educational intervention in this study was designed to instruct undergraduates on safety measures in syringe irrigation and to raise awareness about the potential consequences of imprudent irrigant application. A key focus was the prevention of NaOCl accidents, which are not only a significant inconvenience for the practitioner but, more importantly, can have severe implications for the patient (14). This study primarily examined the application of plunger forces in syringe irrigation, as research has consistently demonstrated a correlation between applied plunger pressure and resulting periapical pressure (24). Elevated plunger forces generate higher periapical pressures, increasing the likelihood of a NaOCl accident (18).
However, the literature lacks consensus regarding the specific pressure level at which irrigants may exceed the periapical region, potentially leading to an accident. A frequently cited critical value is the central venous pressure (mean: 5.88 mmHg ± 0.15 mmHg) (19). The hypothesis underpinning this threshold suggests that exceeding the central venous pressure during root canal irrigation can cause NaOCl to infiltrate the facial venous system, potentially resulting in characteristic, distinct haemorrhages along the venous blood vessels (21). Various other critical values have been proposed in dental literature (16, 32), but the definitive critical threshold remains undetermined.
A recent in vitro study evaluated which plunger forces result in critical apical pressures in immature teeth with an open apex (20). This study utilised the same cannulas as those employed in the present investigation. According to its findings, when using a 25 G side-vented cannula, it is advised that plunger forces should not exceed 10 N (20). For the side-vented 30 G cannula, plunger forces of up to 40 N can be safely applied to teeth without surpassing the central venous pressure threshold (20).
The force values documented in the present investigation showed higher values in the 30 G cannula compared with the 25 G cannula. Furthermore, the mean of the maximum values for each cannula type did not surpass the recommended plunger forces delineated in a laboratory study (20). However, it is critical to acknowledge that, despite the overall adherence to these recommended force limits, there were instances where some undergraduates applied forces exceeding 40 N. These outliers highlight the variability in force application among individuals and underscore the importance of comprehensive training and education in ensuring the safe and effective use of syringe irrigation in endodontic treatments.
A key observation from this study was the overall increase in plunger forces from T1, the baseline measurements taken without any intervention, to T2, following the educational intervention. This uptick was particularly noticeable among the third-year undergraduates. One possible explanation for this phenomenon could be the inherent caution typically exercised by students when performing a practical exercise for the first time. As they gain familiarity and confidence with the procedure, their application of force may naturally increase, as observed in this study. Therefore, a single educational intervention may not influence the maximum force application as intended. The observed reduction in median plunger forces from T2 to T3, following a subsequent intervention, emphasised the critical role of repeated interventions.
In contrast, when analysing the data from fourth-year undergraduates, a more consistent pattern was evident in comparing results from T1 to T3. The fourth-year students consistently applied similar plunger forces across these time points. This consistency is likely attributable to their prior experience with syringe irrigation, which suggests they had already developed a certain level of familiarity and proficiency with the technique.
The differences observed between the third and fourth-year undergraduates underscore the importance of early and effective education in dental practices, particularly in techniques like syringe irrigation. Introducing such practices at an earlier stage in dental education could ensure that students develop appropriate and safe habits from the outset. This approach could prevent the formation of less effective or potentially hazardous practices that might become in-grained over time. Therefore, the study advocates for early educational interventions to guide students toward establishing safe and efficient syringe irrigation techniques from the beginning of their training.
The study was carried out utilising a well-established laboratory setup specifically designed for the precise collection of data on syringe plunger forces (19, 20). Consistent with previous research, irrigation was conducted in a 3D-printed central maxillary incisor with an open apex. The selection of an immature tooth for this study was strategic, given the paramount importance of NaOCl irrigation and the necessity of minimizing mechanical preparation to preserve the integrity of thin dentin walls during root canal treatment (33). Additionally, an open apex is a critical factor that increases the likelihood of NaOCl accidents (23). Therefore, the educational video contained guidelines for irrigation in teeth with open apices to teach the undergraduates the safest parameters for root canal irrigation. Unlike previous research (20), the present study exclusively used side-vented cannulas. The decision to forego open-ended cannulas was informed by research indicating that they generate higher pressures compared with side-vented cannulas (26). This evidence supports the recommendation to exclude open-ended cannulas from undergraduate endodontic training programs to mitigate the risk of NaOCl extrusion.
The educational video offered undergraduates comprehensive, evidence-based, safe root canal irrigation guidelines. In addition to specifying parameters for irrigant delivery, the video also addressed other critical safety practices. These included adhering to the predetermined working length and avoiding the wedging of the cannula in the canal, both of which are crucial for preventing the undesirable extrusion of the irrigant (25, 29). These practices represent practitioner-dependent factors that have been identified in various studies as significant in mitigating the risk of irrigant extrusion (22). Furthermore, the content of the educational video extended beyond these technical aspects to include precautions against other potential mishaps that could occur during endodontic irrigation. These included scenarios such as the patient’s inadvertent swallowing of the irrigant and the accidental spillage of the irrigant on clothing (13). By covering a comprehensive range of scenarios and safety practices, the educational video aimed to equip undergraduates with a broad understanding of the various facets of safe syringe irrigation.
A limitation of this study was the small number of repetitions each undergraduate performed with each cannula type. This constraint in the number of repetitions was a deliberate decision to ensure that the study did not overly burden the undergraduates or detract significantly from their regular curriculum.
CONCLUSION
The novel approach for teaching undergraduates about safe parameters for syringe irrigation proves to be well-suited for endodontic education. The occurrence of high plunger pressures, which might result in the extrusion of the irrigant, was notably rare among undergraduates. Moreover, the study revealed that a repeated educational intervention focusing on safe root canal irrigation practices reduces the plunger forces applied by undergraduates. This finding is particularly significant, considering that the application of excessive plunger pressures can result in the unwanted extrusion of the irrigant into the periapical region. Thus, incorporating training on safety measures in syringe irrigation within the endodontic curriculum for dental students appears to be highly advantageous. By doing so, students are better equipped to apply these critical practices in a clinical setting, enhancing the overall safety and effectiveness of the endodontic treatments they administer.
Footnotes
Please cite this article as: Magni E, Scianna A, Connert T, Leontiev W, Weiger R, Eggmann F. A Novel Educational Approach For Safe Endodontic Syringe Irrigation: A Randomised Controlled In Vitro Study. Eur Endod J 2024; 9: 279-86
Disclosures
Authorship Contributions
Concept – F.E.; Design – F.E., R.W.; Supervision – F.E., T.C., R.W., E.M.; Funding – F.E.; Data collection and/or processing – A.S.; Data analysis and/or interpretation – F.E., T.C., W.L., A.S., E.M.; Literature search – E.M.; Writing – F.E., W.L., R.W., E.M.; Critical review – F.E., T.C., R.W., W.L., A.S., E.M.
Conflict of Interest
All authors declared no conflict of interest.
Use of AI for Writing Assistance
Assisted technologies and plagiarism: The authors deny any use of artificial intelligence assisted technologies in the production of the submitted work.
Financial Disclosure
Florin Eggmann reports scholarships from the Gottfried and Julia Bangerter-Rhyner Foundation and the Freiwillige Akademische Gesellschaft Basel (FAG) during the conduct of the study.
Peer-review
Externally peer-reviewed
References
- 1.Siqueira JF, Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008;34(11):1291–301. doi: 10.1016/j.joen.2008.07.028. [DOI] [PubMed] [Google Scholar]
- 2.Gulabivala K, Patel B, Evans G, Ng Y-L. Effects of mechanical and chemical procedures on root canal surfaces. Endod Topics. 2005;10(1):103–22. [Google Scholar]
- 3.Haapasalo M, Endal U, Zandi H, Coil JM. Eradication of endodontic infection by instrumentation and irrigation solutions. Endod Topics. 2005;10(1):77–102. [Google Scholar]
- 4.Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30(8):559–67. doi: 10.1097/01.don.0000129039.59003.9d. [DOI] [PubMed] [Google Scholar]
- 5.Savani GM, Sabbah W, Sedgley CM, Whitten B. Current trends in endodontic treatment by general dental practitioners: report of a United States national survey. J Endod. 2014;40(5):618–24. doi: 10.1016/j.joen.2014.01.029. [DOI] [PubMed] [Google Scholar]
- 6.Zaugg LK, Savic A, Amato M, Amato J, Weiger R, Connert T. Endodontic treatment in Switzerland. A National Survey. Swiss Dent J. 2019;130(1):18–29. doi: 10.61872/sdj-2020-01-02. [DOI] [PubMed] [Google Scholar]
- 7.Zehnder M. Root canal irrigants. J Endod. 2006;32(5):389–98. doi: 10.1016/j.joen.2005.09.014. [DOI] [PubMed] [Google Scholar]
- 8.Dutner J, Mines P, Anderson A. Irrigation trends among American Association of Endodontists members: a web-based survey. J Endod. 2012;38(1):37–40. doi: 10.1016/j.joen.2011.08.013. [DOI] [PubMed] [Google Scholar]
- 9.Mohammadi Z. Sodium hypochlorite in endodontics: an update review. Int Dent J. 2008;58(6):329–41. doi: 10.1111/j.1875-595x.2008.tb00354.x. [DOI] [PubMed] [Google Scholar]
- 10.Boutsioukis C, Arias-Moliz MT. Present status and future directions-Irrigants and irrigation methods. Int Endod J. 2022;55:588–612. doi: 10.1111/iej.13739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pashley EL, Birdsong NL, Bowman K, Pashley DH. Cytotoxic effects of Na-OCl on vital tissue. J Endod. 1985;11(12):525–8. doi: 10.1016/S0099-2399(85)80197-7. [DOI] [PubMed] [Google Scholar]
- 12.Slaughter RJ, Watts M, Vale JA, Grieve JR, Schep LJ. The clinical toxicology of sodium hypochlorite. Clin Toxicol (Phila) 2019;57(5):303–11. doi: 10.1080/15563650.2018.1543889. [DOI] [PubMed] [Google Scholar]
- 13.Hülsmann M, Hahn W. Complications during root canal irrigation--literature review and case reports. Int Endod J. 2000;33(3):186–93. doi: 10.1046/j.1365-2591.2000.00303.x. [DOI] [PubMed] [Google Scholar]
- 14.Guivarc’h M, Ordioni U, Ahmed HM, Cohen S, Catherine JH, Bukiet F. Sodium hypochlorite accident: a systematic review. J Endod. 2017;43(1):16–24. doi: 10.1016/j.joen.2016.09.023. [DOI] [PubMed] [Google Scholar]
- 15.Spencer HR, Ike V, Brennan PA. Review: the use of sodium hypochlorite in endodontics--potential complications and their management. Br Dent J. 2007;202(9):555–9. doi: 10.1038/bdj.2007.374. [DOI] [PubMed] [Google Scholar]
- 16.Charara K, Friedman S, Sherman A, Kishen A, Malkhassian G, Khakpour M, et al. Assessment of apical extrusion during root canal irrigation with the novel GentleWave system in a simulated apical environment. J Endod. 2016;42(1):135–9. doi: 10.1016/j.joen.2015.04.009. [DOI] [PubMed] [Google Scholar]
- 17.Goode N, Khan S, Eid AA, Niu LN, Gosier J, Susin LF, et al. Wall shear stress effects of different endodontic irrigation techniques and systems. J Dent. 2013;41(7):636–41. doi: 10.1016/j.jdent.2013.04.007. [DOI] [PubMed] [Google Scholar]
- 18.Khan S, Niu LN, Eid AA, Looney SW, Didato A, Roberts S, et al. Periapical pressures developed by nonbinding irrigation needles at various irrigation delivery rates. J Endod. 2013;39(4):529–33. doi: 10.1016/j.joen.2013.01.001. [DOI] [PubMed] [Google Scholar]
- 19.Magni E, Jäggi M, Eggmann F, Weiger R, Connert T. Apical pressures generated by several canal irrigation methods: A laboratory study in a maxillary central incisor with an open apex. Int Endod J. 2021;54(10):1937–47. doi: 10.1111/iej.13575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jäggi M, Magni E, Eggmann F, ElAyouti A, Connert T, Weiger R. Apical pressure generated using conventional syringe irrigation in immature teeth-an in vitro study. Materials (Basel) 2021;14(10):2580. doi: 10.3390/ma14102580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Zhu WC, Gyamfi J, Niu LN, Schoeffel GJ, Liu SY, Santarcangelo F, et al. Anatomy of sodium hypochlorite accidents involving facial ecchymosis-a review. J Dent. 2013;41(11):935–48. doi: 10.1016/j.jdent.2013.08.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Boutsioukis C, Psimma Z, van der Sluis LW. Factors affecting irrigant extrusion during root canal irrigation: a systematic review. Int Endod J. 2013;46(7):599–618. doi: 10.1111/iej.12038. [DOI] [PubMed] [Google Scholar]
- 23.Kleier DJ, Averbach RE, Mehdipour O. The sodium hypochlorite accident: experience of diplomates of the American Board of Endodontics. J Endod. 2008;34(11):1346–50. doi: 10.1016/j.joen.2008.07.021. [DOI] [PubMed] [Google Scholar]
- 24.Boutsioukis C, Psimma Z, Kastrinakis E. The effect of flow rate and agitation technique on irrigant extrusion ex vivo. Int Endod J. 2014;47(5):487–96. doi: 10.1111/iej.12176. [DOI] [PubMed] [Google Scholar]
- 25.Boutsioukis C, Lambrianidis T, Verhaagen B, Versluis M, Kastrinakis E, Wesselink PR, et al. The effect of needle-insertion depth on the irrigant flow in the root canal: evaluation using an unsteady computational fluid dynamics model. J Endod. 2010;36(10):1664–8. doi: 10.1016/j.joen.2010.06.023. [DOI] [PubMed] [Google Scholar]
- 26.Boutsioukis C, Verhaagen B, Versluis M, Kastrinakis E, Wesselink PR, van der Sluis LW. Evaluation of irrigant flow in the root canal using different needle types by an unsteady computational fluid dynamics model. J Endod. 2010;36(5):875–9. doi: 10.1016/j.joen.2009.12.026. [DOI] [PubMed] [Google Scholar]
- 27.Shen Y, Gao Y, Qian W, Ruse ND, Zhou X, Wu H, et al. Three-dimensional numeric simulation of root canal irrigant flow with different irrigation needles. J Endod. 2010;36(5):884–9. doi: 10.1016/j.joen.2009.12.010. [DOI] [PubMed] [Google Scholar]
- 28.Boutsioukis C, Lambrianidis T, Kastrinakis E, Bekiaroglou P. Measurement of pressure and flow rates during irrigation of a root canal ex vivo with three endodontic needles. Int Endod J. 2007;40(7):504–13. doi: 10.1111/j.1365-2591.2007.01244.x. [DOI] [PubMed] [Google Scholar]
- 29.Psimma Z, Boutsioukis C, Kastrinakis E, Vasiliadis L. Effect of needle insertion depth and root canal curvature on irrigant extrusion ex vivo. J Endod. 2013;39(4):521–4. doi: 10.1016/j.joen.2012.12.018. [DOI] [PubMed] [Google Scholar]
- 30.Boutsioukis C, Gogos C, Verhaagen B, Versluis M, Kastrinakis E, Van der Sluis LW. The effect of root canal taper on the irrigant flow: evaluation using an unsteady computational fluid dynamics model. Int Endod J. 2010;43(10):909–16. doi: 10.1111/j.1365-2591.2010.01767.x. [DOI] [PubMed] [Google Scholar]
- 31.Magni E, Scianna A, Connert T, Leontiev W, Weiger R, Eggmann F. A novel educational approach for safe endodontic syringe irrigation: a randomized controlled study (Version 1) 2024 doi: 10.5281/zenodo.10822262. [Online ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lorono G, Zaldivar JR, Arias A, Cisneros R, Dorado S, Jimenez-Octavio JR. Positive and negative pressure irrigation in oval root canals with apical ramifications: a computational fluid dynamics evaluation in micro-CT scanned real teeth. Int Endod J. 2020;53(5):671–9. doi: 10.1111/iej.13260. [DOI] [PubMed] [Google Scholar]
- 33.Harlamb S. Management of figincompletely developed teeth requiring root canal treatment. Aust Dent J. 2016;61:95–106. doi: 10.1111/adj.12401. [DOI] [PubMed] [Google Scholar]
- 34.Mehdipour O, Kleier DJ, Averbach RE. Anatomy of sodium hypochlo-rite accidents. Compend Contin Educ Dent. 2007;28(10):544–6. 548, 550. [PubMed] [Google Scholar]