

Key Points
-
•
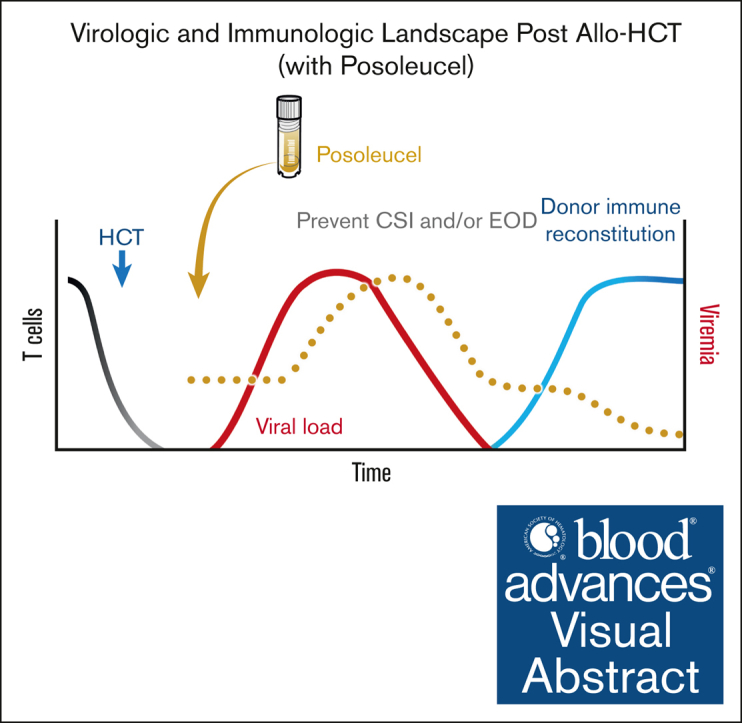
Allogeneic hematopoietic cell transplant recipients are at risk of clinically significant viral infections due to lack of T-cell immunity.
-
•
The multivirus-specific T-cell therapy posoleucel appeared to reduce the risk of clinically significant viral infections.
Visual Abstract
Abstract
Allogeneic hematopoietic cell transplantation (allo-HCT) recipients are susceptible to viral infections. We conducted a phase 2 trial evaluating the safety and rate of clinically significant infections (CSIs; viremia requiring treatment or end-organ disease) after infusion of posoleucel, a partially HLA-matched, allogeneic, off-the-shelf, multivirus-specific T-cell investigational product for preventing CSIs with adenovirus, BK virus, cytomegalovirus, Epstein-Barr virus, human herpesvirus-6, or JC virus. This open-label trial enrolled allo-HCT recipients at high risk based on receiving grafts from umbilical cord blood, haploidentical, mismatched, or matched unrelated donors; post-HCT lymphocytes of <180/mm3; or use of T-cell depletion. Posoleucel dosing was initiated within 15 to 49 days of allo-HCT and subsequently every 14 days for up to 7 doses. The primary end point was the number of CSIs due to the 6 target viruses by week 14. Of the 26 patients enrolled, only 3 (12%) had a CSI by week 14, each with a single target virus. In vivo expansion of functional virus-specific T cells detected via interferon-γ enzyme-linked immunosorbent spot assay was associated with viral control. Persistence of posoleucel-derived T-cell clones for up to 14 weeks after the last infusion was confirmed by T-cell–receptor deep sequencing. Five patients (19%) had acute graft-versus-host disease grade 2 to 4. No patient experienced cytokine release syndrome. All 6 deaths were due to relapse or disease progression. allo-HCT recipients at high risk who received posoleucel had low rates of CSIs from 6 targeted viruses. Repeat posoleucel dosing was generally safe and well tolerated and associated with functional immune reconstitution. This trial was registered at www.ClinicalTrials.gov as #NCT04693637.
Introduction
The past 2 decades have seen a steady rise in patients undergoing hematopoietic cell transplantation (HCT) from HLA-mismatched donors.1, 2, 3 This increase in high-risk allogeneic HCT (allo-HCT) has been largely driven by the availability of mismatched donors and improvements in graft-versus-host disease (GVHD) prevention.4 Newer T-cell ablative and posttransplant cyclophosphamide (PTCy)–based regimens, which are becoming standard of care for most mismatched and matched unrelated donor transplants, have led to significant reductions in the rates of GVHD and nonrelapse mortality (NRM).5 As a result, allo-HCT is increasingly available to patients who had previously not been eligible because of age, lack of matched donor, frailty, or disease status.6,7
However, the high level of immune suppression required to overcome the HLA barrier is known to increase the risk of potentially severe opportunistic infections from double-stranded DNA viruses, including adenovirus (AdV), BK virus (BKV), cytomegalovirus (CMV), Epstein-Barr virus (EBV), human herpesvirus-6 (HHV-6), and JC virus (JCV).8,9 In the first 100 days after allo-HCT, ∼90% of patients have reactivation of 1 of these viruses, and >60% have reactivations of >1 virus.10,11 A nearly 40% increase in NRM is observed for every log10 increase of viral burden during the first 100 days after allo-HCT.10 The use of antithymocyte globulin (ATG) has been linked to an increased risk of EBV and HHV-6 reactivation and disease, whereas PTCy is known to increase the risk of BKV and CMV reactivation and disease.12, 13, 14, 15, 16 Over 60% of these viral reactivations progress to clinically significant infections (CSIs; defined as viremia requiring antiviral treatment or end-organ disease [EOD]), resulting in substantial morbidity and mortality.10
The therapeutic armamentarium against these viruses is limited.17, 18, 19 There are no approved antivirals to treat AdV, BKV, EBV, JCV, and HHV-6, whereas the small-molecule antivirals used to treat or prevent CMV infection have suboptimal efficacy and carry the risk of severe toxicities and development of resistance.20,21 The limitations of existing treatments have encouraged research on preventive approaches. Some of the same broad-spectrum antivirals used in treatment have been used as prophylaxis but with the same shortcomings. The CMV DNA terminase–complex inhibitor letermovir, which was approved in 2017 for the prevention of CMV infection after allo-HCT, has an improved safety profile and greater potency at preventing CMV replication than other antivirals, but it has a relatively low barrier to resistance and targets only CMV.22 In the registrational phase 3 trial, letermovir had no statistically significant impact on all-cause mortality after allo-HCT,11 and late reactivations after the cessation of letermovir are common in patients at high risk.23 Moreover, letermovir, like other small-molecule antivirals, does not address the root cause of the heightened risk of viral infection, the absence of T-cell immunity.
Adoptive virus-specific T-cell therapy, which has been studied for the treatment and prophylaxis of double-stranded DNA viral infections after allo-HCT, may offer an alternative approach to prevention without the disadvantages associated with small molecule antivirals.24, 25, 26, 27, 28, 29, 30 Posoleucel is an allogeneic, off-the-shelf, multivirus-specific T-cell therapy designed for administration as a partially HLA-matched product for the prevention or treatment of CSIs due to AdV, BKV, CMV, EBV, HHV-6, and JCV in patients who are immunocompromised. Posoleucel is polyclonal and polyfunctional with a low potential for alloreactivity (supplemental Appendix 'posoleucel manufacturing').31,32 In the phase 2 CHARMS treatment trial, 95% of allo-HCT recipients with refractory and resistant infections due to the targeted viruses who received posoleucel had a partial or complete clinical response with no safety or tolerability concerns.33,34 This successful outcome prompted the current phase 2 study designed to evaluate the safety of posoleucel and its potential to prevent viral reactivation or de novo infection from progressing to CSIs (with the 6 viruses as detailed above) in allo-HCT recipients.
Methods
Eligibility criteria and study design
This open-label, single-arm, phase 2 study enrolled patients who were within 15 and 49 days of allo-HCT and who were at high risk for CSIs, defined as an AdV, BKV, CMV, EBV, HHV-6, or JCV viral infection requiring treatment. High-risk patients were defined as those who had received a graft from a haploidentical, mismatched unrelated, matched unrelated donor, or from umbilical cord blood , had lymphocytes <180/mm3 at the time at which a partially HLA matched posoleucel cell line was identified (ie, time of randomization) or patients who had received T-cell depletion by ex vivo graft manipulation, ATG, or alemtuzumab. To be eligible, patients were required to have engrafted, based on an absolute neutrophil count of >500 per μL. Those with grade ≥3 GVHD and those requiring high-dose steroids (>0.5 mg/kg per day prednisone equivalent) at enrollment were not eligible. All other immunosuppressive agents for GVHD prophylaxis were allowed. Viremia at screening was not exclusionary, but nonprophylactic receipt of antiviral therapy for a targeted virus or signs and symptoms of EOD from 1 of the targeted viruses in the prior 6 months were exclusionary. Standard-of-care antiviral prophylaxis was allowed, including letermovir. See supplemental Appendix for full eligibility criteria. Investigators obtained informed consent from each participant or each participant's guardian. The study protocol, amendments, and informed consent forms were approved by the independent ethics committee or institutional review board at participating centers. All authors had access to primary clinical trial data. The study was conducted in accordance with the Declaration of Helsinki.
Posoleucel cell lines were selected for each patient based on a partial HLA match of at least 2 shared alleles between the transplant donor, recipient, and posoleucel cell line (see supplemental Appendix for information on the manufacture of posoleucel, and HLA alleles considered during the matching process). Each patient received infusions from the same cell line, which was generated from a single donor.
Patients received posoleucel once every 14 days (±3 days) for up to a total of 7 infusions, which were administered either in the hospital or in the infusion center. Cells were administered at a dose of 2 × 107 cells in 2 mL for patients with a body mass of <40 kg or 4 × 107 cells in 4 mL for patients with a body mass of ≥40 kg. For patients on ATG, alemtuzumab, or other immunosuppressive T-cell–targeted monoclonal antibodies, posoleucel dosing was delayed by at least 28 days from the last dose of anti–T-cell antibody.
AdV, BKV, CMV, EBV, HHV-6, and JCV viral loads were assessed by quantitative polymerase chain reaction at a central laboratory during screening, weekly from the initiation of dosing through week 14, and then monthly through week 26. Viremia was defined as viral load above the lower level of quantitation. Patients were contacted by telephone or email ∼52 weeks after their first treatment to assess 1-year mortality if unknown from record review.
End points
The primary end point of the study was the number of CSIs or EOD per patient due to AdV, BKV, CMV, EBV, HHV-6, or JCV through week 14. A CMV CSI was defined as a viral load of >910 IU/mL plus the initiation of antiviral therapy.35 The definitions of CSIs of EBV or AdV were viral loads of >10 000 copies per mL (or 2 consecutive results of >1000 copies per mL, with the second being higher than the first and drawn at least 48 hours after the first) plus the initiation of antiviral therapy. HHV-6, BKV, and JCV CSIs were not defined by viral load threshold but by the development of associated EOD. EOD was defined as signature signs or symptoms of organ damage from AdV, BKV, CMV, EBV, HHV-6, or JCV. In the instance of end organ dysfunction in which biopsy was not performed, assignment of cause was made by the study principal investigator. The key secondary end point was the number of CSIs per patient through week 26.
Safety end points included the severity and incidence of acute and chronic GVHD, cytokine release syndrome (CRS), and secondary graft failure. Clinical laboratory values, adverse events (AEs), and serious AEs were assessed at 2-week intervals through week 26. Safety events were graded by the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.
Immunoassays
Interferon gamma (IFN-γ) enzyme-linked immunosorbent spot (ELISpot) analysis was used to determine the frequency (spot-forming cells) of IFN-γ+–producing T cells specific for target viruses.36 Posoleucel is a non–gene-modified T-cell product. Hence, to track the presence and persistence of posoleucel clones, T-cell receptor vβ (TCRvβ) sequencing (Adaptive Biotechnologies, Seattle, WA) was performed on the infused lines and serial patient peripheral blood samples collected before and after infusion.37 T-cell clones identified within posoleucel were compared with patient samples from before and after infusion. Those clones that were shared between posoleucel and the preinfusion blood were nondiscriminatory and not used for tracking, whereas those clones that were detected only in the postinfusion blood samples were defined as posoleucel-derived and used to assess persistence. However, it is impossible to definitively discriminate between TCRs of endogenous vs posoleucel origin, because the latter is not genetically modified. Thus, the tracking approach (by TCRvβ deep sequencing and comparison with preinfusion samples) may overestimate or underestimate the number of posoleucel-derived clones. TCR sequencing and ELISpot are complementary, TCRvβ sequencing tracks unique posoleucel-derived TCR sequences and IFN-γ ELISpot detects functional, virus-specific T cells that are both endogenous and of posoleucel origin.
Statistical analysis
CSIs were considered as a failure of prevention; thus, in a given patient, each virus was counted once, even if there were multiple episodes of viremia for a given virus. For the purposes of the primary analysis, only new-onset CSIs with 1 of the 6 target viruses that occurred after the patient’s first dose of posoleucel were considered in the count of CSIs or episodes of EOD per patient.
The protocol, protocol amendments, informed consent form, investigator brochure, and other relevant documents were submitted to an institutional review board/institutional ethics committee by the investigator and reviewed and approved by the institutional review board/institutional ethics committee before the study was initiated.
Results
Patient enrollment and disposition
Of the 37 patients screened for enrollment, 10 did not meet eligibility criteria. A matching posoleucel cell line was found for 36 of 37 patients (97%) screened for enrollment. Table 1 shows the demographics and baseline disease characteristics for the 26 patients enrolled and dosed. Most patients had received HCT grafts from haploidentical (n = 12, 46%) or mismatched unrelated donors (n = 9, 35%). Four patients (15%) had ATG, and 20 (77%) received PTCy. At baseline, 12 patients (46%) had detectable viremia, and 16 (62%) patients received letermovir. Of the 11 patients screened but not dosed, 6 had baseline viral testing; 3 patients (50%) had detectable viremia, 1 each with BKV, EBV, and JCV.
Table 1.
Demographic and disease characteristics
| Characteristic | N = 26 |
|---|---|
| Sex, n (%) | |
| Male | 14 (54) |
| Female | 12 (46) |
| Median age, y (range) | 59.5 (14-76) |
| Race, n (%) | |
| Caucasian | 18 (69) |
| Black or African American | 3 (12) |
| Multiracial | 1 (4) |
| Native Hawaiian or other Pacific Islander | 1 (4) |
| Unknown or unspecified | 3 (12) |
| Ethnicity, n (%) | |
| Not Hispanic or Latino | 19 (73) |
| Hispanic or Latino | 7 (27) |
| Diagnosis, (%) | |
| Acute myeloid leukemia | 8 (31) |
| Acute lymphoblastic leukemia | 5 (19) |
| Chronic myeloid leukemia | 2 (8) |
| Chronic lymphocytic leukemia | 1 (4) |
| Myelodysplasia/myeloproliferative | 3 (12) |
| Sickle cell anemia | 2 (8) |
| Multiple myeloma | 1 (4) |
| Other∗ | 4 (15) |
| Transplant type, n (%) | |
| Haploidentical | 12 (46) |
| Mismatched unrelated | 9 (35) |
| Matched unrelated with T-cell depletion | 4 (15) |
| Umbilical cord blood | 1 (4) |
| Preconditioning type, n (%) | |
| Myeloablative | 12 (46) |
| Reduced intensity/nonmyeloablative | 14 (54) |
| CMV donor (D)/recipient (R) serostatus, n (%) | |
| D−/R+ | 7 (27) |
| D+R+ | 9 (35) |
| D+/R− | 3 (12) |
| D−/R−† | 7 (27) |
| Receiving letermovir at baseline, n (%) | 16 (62) |
| GVHD prophylaxis, n (%) | |
| ATG | 4 (15) |
| PTCy | 21 (81) |
| Viremia at study day 1, n (%)‡ | |
| BKV | 8 (31) |
| HHV-6 | 5 (19) |
| EBV | 2 (8) |
| AdV | 1 (4) |
| None | 14 (54) |
Adrenoleukodystrophy, cutaneous γ-δ T-cell lymphoma, diffuse large B-cell lymphoma, T-cell prolymphocytic leukemia.
One patient was reported as CMV D−/R− but had CMV viremia. Upon investigation by the site, the patient was previously reported as R+ but was presumed to have lost their CMV antibody positivity in a prior chimeric antigen receptor T-cell process.
Eight patients had viremia with a single virus (BKV, n = 4; HHV-6, n = 3; and EBV, n = 1), and 4 had viremia with 2 viruses (BKV + HHV-6, n = 2; AdV + BKV, n = 1; and BKV + EBV, n = 1).
Dosing of the 26 patients began at a median of 42 days (range, 23-52 days) after allo-HCT. The median number of posoleucel doses received was 7 (interquartile range, 5-7). Of the 26 patients dosed, 16 completed treatment, and 10 discontinued dosing (supplemental Figure 1). Four (15%) patients discontinued posoleucel because of ≥1 treatment-emergent AEs (see “Safety”).
Seventeen patients (65%) received systemic corticosteroids at doses >0.5 mg/kg per day (prednisone equivalent) at some point during the study, mostly in short courses to manage GVHD symptoms. Sixteen patients were on letermovir prophylaxis on day 1; see CMV serologies in Table 1.
Primary and key secondary end points
In the first 14 weeks of posoleucel dosing (primary end point period), 23 of 26 patients (88%) remained free of CSIs from any of the target viruses, with none developing hemorrhagic cystitis. Of the 26 patients, 22 (85%) had viremia with ≥1 target viruses, and 13 (50%) had ≥2 viral reactivations (Figure 1). Only 3 patients (12%) progressed to CSIs; 2 received preemptive valganciclovir for asymptomatic CMV viremia; both had been on letermovir previously; and 1 patient developed EBV posttransplant lymphoproliferative disease 6 days after receiving a single dose of intravenous hydrocortisone (75 mg) to treat a sensitivity reaction and in the setting of ongoing methylprednisolone treatment for acute GVHD (aGVHD). All 3 patients with CSIs experienced rapid and full recovery (supplemental Table 1 for details). No pattern was observed in outcome based on the number of HLA matches, or HLA match by class. All 3 CSIs through week 14 occurred in patients who matched at both HLA Class I and Class II loci to posoleucel.
Figure 1.

Viremia and CSIs up to week 14. For each numbered patient in the study (N = 26), there are 6 rows, 1 per target virus. Bars represent the duration of measured viremia (viral load > lower limit of quantification [LLOQ]) per virus. The first panel shows all viremia including viremia that was categorized as CS or causing EOD, the second panel shows duration of viremia categorized as CS (2 patients with CMV), the third panel shows duration of viremia categorized as causing EOD (1 patient with EBV). Nine of 22 patients with viremia had detection of 1 target virus, 5 with 2 viruses, 6 with 3 viruses, and 2 with 4 viruses. Fifteen of 26 patients (58%) had detectable BKV by week 14, making it the most frequently detected virus, followed by EBV (13 of 26 patients, 50%), HHV-6 (6 of 26 patients, 23%), CMV (5 of 26 patients, 19%), AdV (3 of 26 patients, 12%), and JCV (3 of 26 patients, 12%). Notably, there were no CSls from BKV, HHV-6, or JCV, and a single EBV-associated CSI leading to EOD. CS, clinically significant.
From the initiation of posoleucel dosing until the end of week 26 (secondary end point period), a total of 19 patients (73%) remained free of CSIs from any of the target viruses. With respect to the 4 additional patients who developed CSIs between weeks 15 and 26, 3 were cases of asymptomatic CMV viremia in patients who were antibody seropositive, who had previously received letermovir prophylaxis, and who required preemptive antiviral treatment (supplemental Table 2). Of these 3 patients, 1 was receiving dasatinib, which is known to be associated with CMV reactivation,38,39 and another occurred 6 weeks after the last posoleucel infusion, which had ceased when the patient was identified as having relapsed disease (multiple myeloma) that was treated with ixazomib. The fourth CSI in this period was AdV viremia in a patient with diarrhea but not diagnosed with target organ disease. This patient was treated with cidofovir and intravenous immune globulin, and the viremia cleared 5 weeks later. None of the late CSIs progressed to EOD, per treating physician.
T-cell function and persistence
To determine whether posoleucel dosing and the presence or absence of detectable viremia influenced the circulating frequency of virus-reactive T cells (endogenous and posoleucel derived), cellular immune responses to 5 of the target viruses (AdV, BKV, CMV, EBV, and HHV-6) during viremic events were evaluated by IFN-γ ELISpot within the primary end point period. Before posoleucel dosing, most patients lacked detectable T-cell activity against any of the target viruses. In the absence of viremia, the frequency of virus-specific T cells remained relatively static. In contrast, viral reactivation was associated with an increase in the frequency of functional virus-specific T cells (Figure 2A). To determine whether changes in the frequency of functional virus-specific responses were associated with antiviral benefit, preinfusion and postinfusion T-cell responses were evaluated in correspondence to peak and week 14 viral loads in patients who were viremic for a target virus up to week 14. Of 39 viremia events across 5 viruses that did not result in a CSI (AdV, n = 3; BKV, n = 15; CMV, n = 3; EBV, n = 12; and HHV-6, n = 6), there was a reduction in viral titers in 29 of 39 (74%) cases, with a corresponding increase in the circulating frequency of virus-specific T cells for the reactivating virus in 28 of 39 (72%) cases (Figure 2B).
Figure 2.

Viral load (VL), functional virus-specific immune reconstitution, and posoleucel persistence functional immune reconstitution evaluated by ELISpot assay. The frequency of virus- specific IFN-γ+–producing cells (posoleucel and endogenous derived) was evaluated after stimulation of patient peripheral blood mononuclear cells (PBMCs) with AdV, BKV, CMV, EBV, or HHV-6 antigens (spot-forming cells [SFCs] per 5 × 105 PBMCs). (A) ELISpot responses are plotted for all patients (and target viruses) with evaluable data before infusion (Pre; N = 53; mean = 14 SFCs), who were aviremic for a target virus through week 14 (aviremic; n = 51; mean = 28 SFCs), and who were viremic for a target virus through week 14 (viremic, n = 39 of a total of 45 viremic events; mean = 171 SFCs). Box plots show the median with all values plotted. (B) ELISpot responses are plotted for all patients with evaluable data who were viremic for ≥1 viruses during the primary end point. Data shown represent the circulating frequency of IFN-γ+ T cells before posoleucel infusion (Pre) and the peak response through week 14 (Post). VLs are also shown per virus by plotting the peak VL through week 14 (peak VL) and at week 14/last time point available (week 14 VL). VLs from 3 patients with CSIs are excluded (CMV, n = 2; and EBV, n = 1). (C) TCRβ sequencing was used to track presence of TCRβ sequences unique to posoleucel during the infusion period and after (postinfusion). The percentage of patients with detectable posoleucel T cells during each indicated study period are shown.
To evaluate the presence and persistence of posoleucel, we performed tracking studies using TCR deep sequencing with specific focus on detecting sequences unique to the infused posoleucel cell lines. All patients evaluated by TCR sequencing (n = 25 of 25) had detectable posoleucel T-cell clones (albeit at low levels, ranging from 0.0005%-0.2%) at ≥1 time points during the dosing period of the study (week 1 to week 14) with persistence for up to 14 weeks after the dosing period in 21 of 21 evaluable patients (Figure 2C). Figure 3 shows representative posoleucel persistence and ELISpot data for 3 patients with viremia from multiple viruses not requiring treatments (BKV, EBV, and HHV-6 [Figure 3A-B]; BKV and EBV [Figure 3C-D]; or BKV, CMV, EBV, and JCV [Figure 3E-F]). Supplemental Figure 2 shows 3 patients with CSIs (EBV posttransplant lymphoproliferative disease [panels A-B]; CMV CSI and BK and JCV viremia [panels C-D]; and CMV CSI and BKV viremia [panels E-F]). In patients with viremia that did (n = 3; supplemental Figure 2) or did not progress to CSI (n = 3; Figure 3), viral control was coincident with detection of posoleucel clones and expansion of functional T cells against the replicating virus(es).
Figure 3.

Detection of functional immune reconstitution and posoleucel clones over time coincident with viremia reduction. Patient examples of viral load plotted with unique posoleucel clones detected by TCRβ sequencing (left panels) and functional IFN-γ+ virus-specific T-cell responses detected by ELISpot (posoleucel and endogenous derived; right panels) through week 26 of the study for patients with viremia of ≥1 target virus(es). Three patients with viremia that did not progress to CSI are shown: patient 1: BKV, EBV, and HHV-6 viremia (A-B; received all 7 doses of posoleucel); patient 2: BKV and EBV viremia (C-D; received all 7 doses of posoleucel); and patient 3: BKV, CMV, EBV, and JCV viremia (E-F; received all 7 doses of posoleucel). TCRβ clones unique to posoleucel are shown as the log2 fold change of the sum frequency of clones relative to first time point detected. Virus-specific IFN-γ+–producing cells were measured by ELISpot after stimulation of patient PBMCs with AdV, BKV, CMV, EBV, or HHV-6 antigens (SFCs per 5 × 105 PBMCs). All detectable viremia (viremia > LLOQ) is shown in the left panels with TCRβ sequencing data. In right panels with ELISpot data, only viremia for which there was corresponding ELISpot data is shown.
Safety
All 26 (100%) patients had at least 1 AE during the study (Table 2). The most common AEs were diarrhea (in 62% of patients) and acute skin GVHD (38%). Abdominal pain, dyspnea, pain in extremity, tremor, or decreased weight each occurred in 23% of patients. Nineteen patients (73%) had at least 1 serious AE, of which 3 (12%) were considered treatment related by the investigator. Four (15%) patients had an AE that led to discontinuation of study treatment, whereas none had an AE that led to discontinuation of the study. No renal toxicity or myelosuppression was observed.
Table 2.
AEs
| Event | N = 26, n (%) |
|---|---|
| Patients with any treatment-emergent AE | 26 (100) |
| Any treatment-related AE | 12 (46) |
| Patients with most common treatment-emergent AEs (>20%) | |
| Diarrhea | 16 (62) |
| aGVHD in the skin | 10 (38) |
| Abdominal pain | 6 (23) |
| Dyspnea | 6 (23) |
| Pain in extremity | 6 (23) |
| Tremor | 6 (23) |
| Weight decreased | 6 (23) |
| Any serious AE | 19 (73) |
| Any treatment-related serious AE | 3 (12) |
| aGVHD in the skin | 1 (4) |
| Chronic GVHD in the lung | 1 (4) |
| Hypersensitivity | 1 (4) |
| Any grade ≥3 AE | 19 (73) |
| Any treatment-related grade ≥3 AE | 4 (15) |
| Any AE leading to discontinuation of study treatment | 4 (15) |
| Pancreatitis | 1 (4) |
| aGVHD in the skin | 1 (4) |
| GVHD in the gastrointestinal tract | 1 (4) |
| Dyspnea | 1 (4) |
| Any deaths related to treatment | 0 |
Five patients (19%) had Mount Sinai Acute GVHD International Consortitium grade 2 to 4 treatment-emergent aGVHD: 3 with grade 2, and 1 each with grades 3 and 4 (supplemental Table 3). In this small sample, no trend was observed between the incidence or severity of GVHD and the number of matched HLA alleles (representing the number of shared alleles between the HCT donor, recipient, and posoleucel cell line received). Of 26 patients, 21 (81%) received PTCy, and among this cohort 2 of 21 (10%) developed grade 2 to 4 aGVHD, 0 of 21 (0%) developed grade 3/4 aGVHD, and 3 of 21 (14%) developed moderate to severe chronic GVHD. No patient experienced CRS.
At 1 year on study, NRM after allo-HCT was 0% (Figure 4). Six patients died, all as a result of primary disease relapse. None of the deaths were considered by the investigator to be related to treatment, and none were attributed to GVHD or infection with 1 of the target viruses.
Figure 4.

Overall survival (OS) through week 52.
Discussion
In this study, designed to evaluate posoleucel’s safety and ability to prevent CSIs from 6 targeted double-stranded DNA viruses in a high-risk cohort of allo-HCT recipients, only 12% of patients had CSIs in the first 14 weeks after the initiation of posoleucel. Moreover, the rate of NRM we observed after 1 year on study was 0%. These results support the safety and tolerability of posoleucel. The efficacy of posoleucel is being investigated in a placebo-controlled phase 3 trial for the prevention of CSIs from the 6 targeted viruses, for decreasing the use of myelotoxic and nephrotoxic antivirals, and for potentially contributing to broadly favorable immune protection after allo-HCT. Because managing CSIs in transplant recipients often requires prolonged hospitalization and complex interventions, posoleucel has the potential to reduce health resource use, with attendant clinical and economic benefits.40,41
As a frequent cause of CSIs in allo-HCT recipients, CMV has received much attention from researchers, which has led to the development of new options for CMV prevention and treatment. Although AdV, BKV, EBV, and HHV-6 viremias are monitored less consistently, CSIs caused by these viruses are nonetheless important causes of posttransplant morbidity and adverse outcomes, and account for substantial health care resource use.42,43 Importantly, patients frequently experience sequential or simultaneous viral reactivations/infections with corresponding increases in morbidity and mortality.10 In this study, there were no CSIs involving HHV-6, BKV, or JCV for the duration of the study (>6 months), and the incidence of CSIs involving AdV and EBV was only 4% although 13 patients (50%) were viremic with >1 virus and were therefore at higher risk of CSIs. However, definitive efficacy results will require assessment in the context of a randomized, placebo-controlled phase 3 clinical trial. Most patients who were viremic for ≥2 viruses demonstrated evidence of functional immune reconstitution for multiple viruses during posoleucel dosing. Together, these data highlight the clinical utility of a multivirus-targeted therapy to bridge the lymphopenic period after allo-HCT and support the mode of action of posoleucel to expand in response to viremia and ultimately control infection, preventing progression to clinically significant disease.
Posoleucel is designed not to prevent the occurrence of viremia but to prevent reactivated or new infections from progressing to CSIs. Thus, the mostly subclinical viremia observed in this study, at rates roughly comparable to those seen in historical studies, was not unexpected. Importantly, low-level antigen exposure can activate and stimulate the expansion of the infused posoleucel cells. As seen in studies of CMV prevention using conventional antivirals, restricting CMV replication appears to delay CMV-specific immune reconstitution by eliminating antigens necessary for supporting functional immune reconstitution. In a study of CMV-specific T-cell reconstitution in patients receiving letermovir, the subpopulation of patients with subclinical CMV reactivation during prophylaxis had superior CMV-specific CD8+ and CD4+ T-cell responses at the end of prophylaxis than patients with complete suppression of reactivation.44
Viremia in our patient population resulted in a selective expansion of T cells reactive against the replicating virus(es), with consequent reduction of viremia. To determine whether posoleucel could have contributed to this immune reconstitution, TCR sequencing was used to track unique posoleucel clones during the study. This analysis confirmed the presence and persistence of posoleucel throughout dosing and follow-up, and serial sampling within patients highlighted changes in sum frequencies of posoleucel clones during viral reactivation.
The results of this trial add to the considerable body of evidence that virus-specific T-cell therapy is a safe and well-tolerated approach.45 Despite receiving multiple infusions of posoleucel, no patient experienced CRS, and the rate of aGVHD was in line with rates seen in previous studies in allo-HCT recipients at high risk. In addition, the rates of aGVHD grade 2 to 4 (10%) and aGVHD grade 3/4 (0%) for patients receiving PTCy were in line with recently reported cohorts (53.8% and 6.3%, respectively). Because posoleucel consists of virus-specific CD4+ and CD8+ memory T cells, its potential for alloreactivity is low. No renal toxicity or myelosuppression was observed.
Interpretation of the results of this trial is necessarily limited given the relatively small sample size, lack of a comparison group, and relatively late initiation of posoleucel dosing (a median of 42 days after allo-HCT). Dosing sooner after allo-HCT may benefit patients in potentially preventing CSIs that occur earlier in these patients who are severely immunosuppressed and has been implemented within 25 (+5) days after HCT in the phase 3 study.
In this open label phase 2 study, posoleucel appeared safe and well tolerated in this diverse group of patients. A phase 3 randomized, placebo-controlled study of posoleucel for the prevention of infection or disease due to AdV, BKV, CMV, EBV, HHV-6, or JCV in adult and pediatric patients at high risk after allo-HCT is currently ongoing (ClinicalTrials.gov identifier: NCT05305040).
Conflict-of-interest disclosure: S.S.D. has served on an advisory board for Merck; has served as a speaker for Takeda, Merck, and Astellas; has received research funding from AlloVir, Karius, Ansun Biopharma, Merck, and Amplyx/Pfizer; and has stock options with Aseptiscope, Inc. G.D.M. has served on an advisory board and speakers bureau for Novartis; has consulted for Eliana; and has received research funding from AlloVir. M.M., J.M., S.A., S.A.G., and D.M. are employees of, and hold stock in, AlloVir. S.V. and A.M.L. are consultants for, and hold stock in, AlloVir. J.A.H. has served as a consultant for Amplyx. The remaining authors declare no competing financial interests.
Acknowledgments
The authors extend their gratitude to the patients and their families, and to Manik Kuvalekar, Ayumi Watanabe, and Yovana Velazquez for their work on the ELISpot analyses.
The study was funded by AlloVir.
Authorship
Contributions: M.M. and A.M.L. designed the study; S.S.D., R.B., M.W.S., J.A.Y., G.D.M., J.A.H., and J.-A.H.Y. provided study materials or recruited patients; S.S.D., R.B., M.W.S., J.A.Y., G.D.M., J.A.H., J.-A.H.Y., J.M., M.M., S.A., S.A.G., S.V., and A.M.L. collected and assembled data; S.S.D., M.M., S.A., S.A.G., S.V., J.M., and A.M.L. analyzed and interpreted the data; M.M., D.M., S.A.G., and A.M.L. drafted the manuscript; and all authors approved the manuscript and agree to be accountable for all aspects of the work.
Footnotes
J.A.H. and J.-A.H.Y. are joint senior authors.
Qualified researchers may request from AlloVir data supporting the clinical findings of this study by contacting info@allovir.com; individual patient data will not be shared.
The full-text version of this article contains a data supplement.
Supplementary Material
References
- 1.Auletta JJ, Kou J, Chen M, Shaw BE. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR US summary slides. CIBMTR. 2021. https://cibmtr.org/CIBMTR/Resources/Summary-Slides-Reports
- 2.Niederwieser D, Baldomero H, Bazuaye N, et al. One and a half million hematopoietic stem cell transplants: continuous and differential improvement in worldwide access with the use of non-identical family donors. Haematologica. 2022;107(5):1045–1053. doi: 10.3324/haematol.2021.279189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gratwohl A, Pasquini MC, Aljurf M, et al. One million haemopoietic stem-cell transplants: a retrospective observational study. Lancet Haematol. 2015;2(3):e91–e100. doi: 10.1016/S2352-3026(15)00028-9. [DOI] [PubMed] [Google Scholar]
- 4.McDonald GB, Sandmaier BM, Mielcarek M, et al. Survival, non-relapse mortality, and relapse-related mortality after allogeneic hematopoietic cell transplantation: comparing 2003-2007 vs. 2013-2017 cohorts. Ann Intern Med. 2020;172(4):229–239. doi: 10.7326/M19-2936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Penack O, Peczynski C, Mohty M, et al. How much has allogeneic stem cell transplant–related mortality improved since the 1980s? A retrospective analysis from the EBMT. Blood Adv. 2020;4(24):6283–6290. doi: 10.1182/bloodadvances.2020003418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.D’Souza A, Fretham C, Lee SJ, et al. Current use of and trends in hematopoietic cell transplantation in the United States. Biol Blood Marrow Transplant. 2020;26(8):e177–e182. doi: 10.1016/j.bbmt.2020.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bryant AR, Perales MA. Advances in ex vivo T cell depletion – where do we stand? Adv Cell Gene Ther. 2019;2(1) doi: 10.1002/acg2.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stanojevic M, Bertaina A, Bonfim C, et al. Viral infection in hematopoietic stem cell transplantation: an International Society for Cell & Gene Therapy Stem Cell Engineering Committee review on the role of cellular therapy in prevention and treatment. Cytotherapy. 2022;24(9):884–891. doi: 10.1016/j.jcyt.2022.05.010. [DOI] [PubMed] [Google Scholar]
- 9.Young JAH, Logan BR, Wu J, et al. Infections after transplantation of bone marrow or peripheral blood stem cells from unrelated donors. Biol Blood Marrow Transplant. 2016;22(2):359–370. doi: 10.1016/j.bbmt.2015.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hill JA, Mayer BT, Xie H, et al. The cumulative burden of double-stranded DNA virus detection after allogeneic HCT is associated with increased mortality. Blood. 2017;129(16):2316–2325. doi: 10.1182/blood-2016-10-748426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Marty F, Ljungman P, Chemaly RF, et al. Letermovir prophylaxis for cytomegalovirus in hematopoietic-cell transplantation. N Engl J Med. 2017;377(25):2433–2444. doi: 10.1056/NEJMoa1706640. [DOI] [PubMed] [Google Scholar]
- 12.Perchetti GA, Biernacki MA, Xie H, et al. Cytomegalovirus breakthrough and resistance during letermovir prophylaxis. Bone Marrow Transplant. 2023;58(4):430–436. doi: 10.1038/s41409-023-01920-w. [DOI] [PubMed] [Google Scholar]
- 13.Singh A, Dandoy CE, Chen M, et al. Post-transplantation cyclophosphamide is associated with an increase in non-cytomegalovirus herpesvirus infections in patients with acute leukemia and myelodysplastic syndrome. Transplant Cell Ther. 2022;28(1):48.e1–48.e10. doi: 10.1016/j.jtct.2021.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Figgins B, Hammerstrom A, Ariza-Heredia E, Oran B, Milton DR, Yeh J. Characterization of viral infections after antithymocyte globulin-based conditioning in adults undergoing allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2019;25(9):1837–1843. doi: 10.1016/j.bbmt.2019.05.020. [DOI] [PubMed] [Google Scholar]
- 15.Slade M, Goldsmith S, Romee R, et al. Epidemiology of infections following haploidentical peripheral blood hematopoietic cell transplantation. Transpl Infect Dis. 2017;19(1) doi: 10.1111/tid.12629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Esquirol A, Pascual MJ, Kwon M, et al. Severe infections and infection-related mortality in a large series of haploidentical hematopoietic stem cell transplantation with post-transplant cyclophosphamide. Bone Marrow Transplant. 2021;56(10):2432–2444. doi: 10.1038/s41409-021-01328-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lin R, Liu Q. Diagnosis and treatment of viral diseases in recipients of allogeneic hematopoietic stem cell transplantation. J Hematol Oncol. 2013;6:94. doi: 10.1186/1756-8722-6-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Otto WR, Green A. Antiviral therapeutics in pediatric transplant recipients. Infect Dis Clin North Am. 2022;36(1):125–146. doi: 10.1016/j.idc.2021.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chemaly RF, Hill JA, Voigt S, Peggs KS. In vitro comparison of currently available and investigational antiviral agents against pathogenic human double-stranded DNA viruses: a systematic literature review. Antiviral Res. 2019;163:50–58. doi: 10.1016/j.antiviral.2019.01.008. [DOI] [PubMed] [Google Scholar]
- 20.Chou S. Advances in the genotypic diagnosis of cytomegalovirus antiviral drug resistance. Antiviral Res. 2020;176 doi: 10.1016/j.antiviral.2020.104711. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chou S, Song K, Wu J, Bo T, Crumpacker C. Drug resistance mutations and associated phenotypes detected in clinical trials of maribavir for treatment of cytomegalovirus infection. J Infect Dis. 2022;226(4):576–584. doi: 10.1093/infdis/jiaa462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hofmann E, Sidler D, Dahdal S, et al. Emergence of letermovir resistance in solid organ transplant recipients with ganciclovir resistant cytomegalovirus infection: a case series and review of the literature. Transpl Infect Dis. 2021;23(3) doi: 10.1111/tid.13515. [DOI] [PubMed] [Google Scholar]
- 23.Hill JA, Zamora D, Xie H, et al. Delayed-onset cytomegalovirus infection is frequent after discontinuing letermovir in cord blood transplant recipients. Blood Adv. 2021;5(16):3113–3119. doi: 10.1182/bloodadvances.2021004362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Basso S, Compagno F, Zelini P, et al. Harnessing T cells to control infections after allogeneic hematopoietic stem cell transplantation. Front Immunol. 2020;11 doi: 10.3389/fimmu.2020.567531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ottaviano G, Chiesa R, Feuchtinger T, et al. Adoptive T cell therapy strategies for viral infections in patients receiving haematopoietic stem cell transplantation. Cells. 2019;8(1):47. doi: 10.3390/cells8010047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gottlieb DJ, Clancy LE, Withers B, et al. Prophylactic antigen-specific T-cells targeting seven viral and fungal pathogens after allogeneic haemopoietic stem cell transplant. Clin Transl Immunology. 2021;10(3) doi: 10.1002/cti2.1249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rubinstein JD, Lutzko C, Leemhuis T, et al. Scheduled administration of virus-specific T cells for viral prophylaxis after pediatric allogeneic stem cell transplant. Blood Adv. 2022;6(9):2897–2907. doi: 10.1182/bloodadvances.2021006309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kinoshita H, Mandava M, Jensen-Wachspress M, et al. Outcomes following posttransplant virus-specific T-cell therapy in patients with sickle cell disease. Blood Adv. 2023;7(10):2105–2116. doi: 10.1182/bloodadvances.2022008219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gerbitz A, Gary R, Aigner M, et al. Prevention of CMV/EBV reactivation by double-specific T cells in patients after allogeneic stem cell transplantation: results from the randomized phase I/IIa MULTIVIR-01 study. Front Immunol. 2023;14 doi: 10.3389/fimmu.2023.1251593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Comoli P, Labirio M, Basso S, et al. Infusion of autologous Epstein-Barr virus (EBV)-specific cytotoxic T cells for prevention of EBV-related lymphoproliferative disorder in solid organ transplant recipients with evidence of active virus replication. Blood. 2002;99(7):2592–2598. doi: 10.1182/blood.v99.7.2592. [DOI] [PubMed] [Google Scholar]
- 31.Gerdemann U, Keirnan JM, Katari UL, et al. Rapidly generated multivirus-specific cytotoxic T lymphocytes for the prophylaxis and treatment of viral infections. Mol Ther. 2012;20(8):1622–1632. doi: 10.1038/mt.2012.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Papadopoulou A, Gerdemann U, Katari UL, et al. Activity of broad-spectrum T cells as treatment for AdV, EBV, CMV, BKV, and HHV-6 infections after HSCT. Sci Transl Med. 2014;6(242):242ra83. doi: 10.1126/scitranslmed.3008825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Tzannou I, Papadopoulou A, Naik S, et al. Off-the-shelf virus-specific T cells to treat BK virus, human herpesvirus 6, cytomegalovirus, Epstein-Barr virus, and adenovirus infections after allogeneic hematopoietic stem-cell transplantation. J Clin Oncol. 2017;35(31):3547–3557. doi: 10.1200/JCO.2017.73.0655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Pfeiffer T, Tzannou I, Wu M, et al. Posoleucel, an allogeneic, off-the-shelf multi-virus specific T cell therapy, for the treatment of refractory viral infections in the post-HCT setting. Clin Cancer Res. 2023;29(2):324–330. doi: 10.1158/1078-0432.CCR-22-2415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lodding IP, Mocroft A, da Cunha Bang C, et al. Impact of CMV PCR blips in recipients of solid organ and hematopoietic stem cell transplantation. Transplant Direct. 2018;4(6) doi: 10.1097/TXD.0000000000000787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lulla PD, Tzannou I, Vasileiou S, et al. The safety and clinical effects of administering a multiantigen-targeted T cell therapy to patients with multiple myeloma. Sci Transl Med. 2020;12(554) doi: 10.1126/scitranslmed.aaz3339. [DOI] [PubMed] [Google Scholar]
- 37.Wolf K, Hether T, Gilchuk P, et al. Identifying and tracking low-frequency virus-specific TCR clonotypes using high-throughput sequencing. Cell Rep. 2018;25(9):2369–2378.e4. doi: 10.1016/j.celrep.2018.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Prestes DP, Arbona E, Nevett-Fernandez A, et al. Dasatinib use and risk of cytomegalovirus reactivation after allogeneic hematopoietic-cell transplantation. Clin Infect Dis. 2017;65(3):510–513. doi: 10.1093/cid/cix325. [DOI] [PubMed] [Google Scholar]
- 39.Choi JK, Cho SY, Choi SM, et al. Cytomegalovirus colitis during dasatinib treatment for patients with hematologic malignancy: case series and literature review. Infect Chemother. 2018;50(2):153–159. doi: 10.3947/ic.2018.50.2.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.McGuirk J, Divine C, Moon SH, Chandak A, Zhang Z, Papanicolaou GA. Economic and clinical burden of virus-associated hemorrhagic cystitis in patients following allogeneic hematopoietic stem cell transplantation in the United States. Transplant Cell Ther. 2021;27(6):505.e1–505.e9. doi: 10.1016/j.jtct.2021.02.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hill JA, Moon SH, Chandak A, Zhang Z, Boeckh M, Maziarz RT. Clinical and economic burden of multiple double-stranded DNA viral infections after allogeneic hematopoietic cell transplantation. Transplant Cell Ther. 2022;28(9):619.e1–619.e8. doi: 10.1016/j.jtct.2022.06.016. [DOI] [PubMed] [Google Scholar]
- 42.Wang X, Patel SA, Haddadin M, Cerny J. Post-allogeneic hematopoietic stem cell transplantation viral reactivations and viremias: a focused review on human herpesvirus-6, BK virus and adenovirus. Ther Adv Infect Dis. 2021;8(9) doi: 10.1177/20499361211018027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Lee YJ, Su Y, Cho C, et al. Human herpesvirus 6 DNAemia is associated with worse survival after ex vivo T-cell-depleted hematopoietic cell transplant. J Infect Dis. 2022;225(3):453–464. doi: 10.1093/infdis/jiab412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Zamora D, Duke ER, Xie H, et al. Cytomegalovirus-specific T-cell reconstitution following letermovir prophylaxis after hematopoietic cell transplantation. Blood. 2021;138(1):34–43. doi: 10.1182/blood.2020009396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Simmons HZ, Bazzell AF, Dains JE. Adverse effects of virus-specific T-cell therapy: an integrative review. J Adv Pract Oncol. 2019;10(2):120–131. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.