

Abstract
Introduction and importance
Meckel's diverticulum is The most common congenital anomaly of the gastrointestinal tract, Meckel's diverticulum, affects around 2 % of the general population. Meckel's diverticulum symptoms in the newborn stage are quite uncommon.
Case presentation
A male newborn, aged 6 days, was brought to our hospital due to recurrent episodes of vomiting during nursing and fever. There was bilious vomiting along with distention of the abdomen. Following a physical assessment and radiological analysis, the patient had an exploratory laparotomy with a bowel perforation impression. The abdominal cavity contained bowel content and a diagnosis of perforated MD was made. Following a thorough abdominal wash with warm normal saline, wedge resection and anastomosis were performed. Released three days following eight days of hospitalization and attaining full feeding. Six-month follow-up showed good recovery and ideal growth and development.
Clinical discussion
Meckel's diverticulum (MD), the most prevalent congenital gastrointestinal tract malformation, results from partial obliteration of the proximal portion of the omphalomesenteric duct during the seventh week of pregnancy. We report in this study an MD case with a range of complex spectra, such as severe distention and vomiting in the neonatal period. Meckel's diverticulum perforation is a deadly complication that typically results from gangrene, diverticulitis, or peptic ulceration brought on by an ectopic stomach mucosa.
Conclusion
The two most common clinical manifestations of symptomatic MD in newborns are partial bowel obstruction and pneumoperitoneum. Surgery is the only accurate method for both diagnostic and therapeutic purposes with a successful outcome.
Keywords: Neonate, Meckel's diverticulum, Perforation
Highlights
-
•
Meckel's diverticulum (MD), the most prevalent congenital gastrointestinal tract malformation,
-
•
affects around 2% of the general population, MD symptoms in the newborn stage are quite uncommon,
-
•
Surgery is the only accurate method for both diagnostic and therapeutic purposes.
1. İntroduction
The most common congenital anomaly of the gastrointestinal tract (GI), Meckel's diverticulum (MD), affects around 2 % of the general population [1]. MD symptoms in the newborn stage are quite uncommon. Nearly 4 % of cases are complicated [2]. Pneumoperitoneum is a severe disorder in newborns that needs to be treated surgically right away. In this age range, necrotizing enterocolitis and intestinal atresia, which include a variety of idiopathic illnesses, are the most frequent causes. A perforated Meckel's diverticulum (MD) is an uncommon cause; to date, only a small number of cases have been published [3]. Here we present 6 days-old neonate patient who presented distention and bilious vomiting with pneumoperitoneum on an erect abdominal x-ray.
2. Case presentation
A male newborn, aged 6 days, was brought to our hospital due to recurrent episodes of vomiting during feeding and fever. There was bilious vomiting along with distention of the abdomen. With an APGAR score of 9 at minute 1 and 10 at minute 5, the neonate weighed 3200 g at birth and was delivered vaginally by a 26-year-old mother who was gravid 3. The patient was transferred from the hospital where he was born. Upon arrival, the newborn had a sluggish state and underwent a thorough physical examination that showed tachycardia, fever, and considerable abdominal distention. Assessment in the laboratory was completed on the first day of admission. 13.36 g/dL of white blood cells were counted. It had 8.4 g/dL of hemoglobin. There were 123,000 platelets (Fig. 1). Urea nitrogen in the blood was 35 mg/d, creatine 0.17 mg/dL, CRP 18, and albumin 2.5 (Fig. 2). Thoraco-abdominal radiography was performed as a result of bilious vomiting, which showed peumoperitoneum (Fig. 3). Following a physical assessment and radiological analysis, the patient had an exploratory laparotomy with a bowel perforation impression. The abdominal cavity contained bowel content, and free air burst out as soon as it entered and relieved distension. and a perforated MD diagnosis was made (Fig. 4). Following a thorough abdominal wash with warm normal saline, wedge resection and anastomosis were performed. After which the abdomen was closed and a drain was put in place. The pathological report verified the diagnosis of MD in the absence of heterotopic gastric mucosa. Five days following the procedure, the nasogastric tube was taken out, and oral feeding was initiated with 5 % dextrose and then formula, which was then gradually increased without any complications. Released three days following eight days of hospitalization and attaining full feeding. Six-month follow-up showed good recovery and ideal growth and development.
Fig. 1.
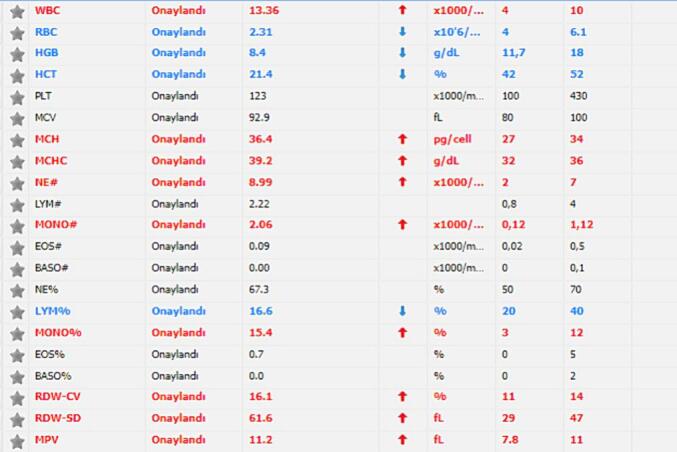
Hemogram results.
Fig. 2.
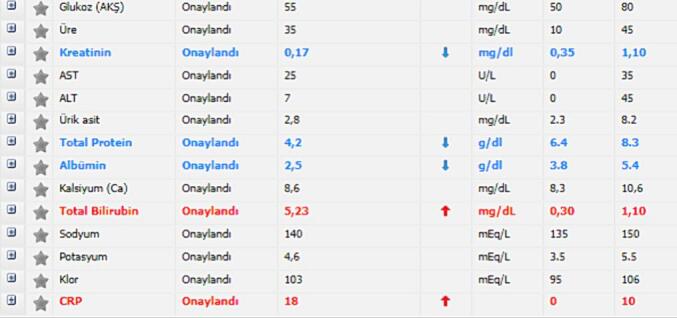
Biochemistry results.
Fig. 3.

Thoracoabdominal x-ray with large peumoperitoneum appearing football sign.
Fig. 4.

Perforated Meckel's diverticulum.
3. Discussion
Meckel's diverticulum (MD), the most prevalent congenital gastrointestinal tract malformation, results from partial obliteration of the proximal portion of the omphalomesenteric duct during the seventh week of pregnancy [4]. We report in this study an MD case with a range of complex nonspecific clinical symptoms, such as severe distention and vomiting in the neonatal period. Patients with MD rarely exhibit a clinical feature, but they can experience a range of symptoms, such as severe anemia from gross or occult gastrointestinal bleeding, small-bowel obstruction, or peritonitis [5]. Anemia and nonspecific clinical manifestations were present in the study's case report. Meckel's diverticula contain up to 55 % ectopic tissue [6]. This case ectopic tissue was not present. Meckel's diverticulum perforation is a deadly complication that typically results from gangrene, diverticulitis, or peptic ulceration brought on by an ectopic stomach mucosa. Littre's hernia and tumors such as leiomyosarcoma, lymphatic sarcoma, and poorly differentiated stromal tumors are among the other various pathologies that can result in perforation [7]. According to reports, perforation results from acute inflammation of MD, however the precise proportion of this pathology has not been disclosed [8]. Current case pathology of the specimen revealed presence of inflammation which is consistent. Bertozzi etel [9] reported case of two site perforation of Meckel's diverticulum with histopathology revealing neither inflammation of the MD nor heterotopic tissue, which is contrary to our case in which pathology revealed Meckel's diverticulum inflammation. Clinicians frequently lack the time to pursue different diagnostic measures when dealing with acute abdomen conditions, and conventional radiographs are not very useful in detecting perforated MD [10]. Duplication or mesenteric, ovarian, or choledochal cysts are among the differential diagnoses. Planning for delivery and managing the newborn are aided by prenatal evaluation. Following delivery, plain abdominal radiography, US, CT, and laparotomy may be required to confirm the diagnosis [11].our case erect abdominal x-ray was only image modality used. Treatment choice of symptomatic MD is surgery. The type of resection is determined by the shape of the diverticulum and the surgeon's experience and preference [12]. The type of resection is determined by the shape of the diverticulum and the surgeon's experience and preference [12]. The current case wedge resection and anastomosis were done as the base of the diverticulum was narrow. If the diverticulum has broad base resection, anastomosis is the best choice. BR Alvares et al. reported case of perforated MD and managed surgically with segmental resection anastomosis [13]. We emphasize that neonates with acute abdominal Meckel's diverticulum should have a first-line differential diagnosis, and exploratory laparotomy is the only approach that can be an accurate diagnosis.
This study was reported in accordance with the SCARE 2020 guidelines [14].
4. Conclusion
The two most common clinical manifestations of symptomatic MD in newborns are partial bowel obstruction and pneumoperitoneum. We emphasize that neonates with acute abdomen and Meckel's diverticulum should have a first-line differential diagnosis, and exploratory laparotomy is the only approach to reaching an accurate diagnosis. Wedge resection with anastomosis is the surgical method for narrow-base Meckel's diverticulum with a successful outcome.
Abbreviations
- MD
Meckel's diverticulum
- US
ultrasonography
- CT
computed tomography
Consent
Written informed consent was obtained from the patient's parents/legal guardian for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval was waived by the ethical committee of Mogadishu Somali Turkey, Recep Tayyip Erdogan Training and Research Hospital. No need ethical approval for case report study in our Hospital.
Funding
No funding was received.
Author contribution
Abdishakur Mohamed Abdi: wrote the manuscript and corrected the manuscript for its scientific basis.
Abdullah Yusuf Ali: collected the data for the study.
Abdisalam Abdullahi Yusuf: head of pediatric neonatal ICU and was taking care of the patient after operation.
Ibrahim Mohamed Hirsi: pediatric emergency resident doctor received and stabilized the patient.
Ismail Gedi Ibrahim: radiology specialist reported abdominal x-ray.
All authors have read and approved the final manuscript.
Guarantor
Dr. Abdishakur Mohamed Abdi.
Research registration number
None.
Declaration of competing interest
This manuscript has not been submitted to, nor is it under review at, another journal or other publishing venue.
The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript.
References
- 1.Khoury V., Taishori N., Abdo A., Omran A. Idiopathic Meckel’s diverticulum perforation presenting at birth. J Pediatr Surg Case Rep. 2021 Nov 1;74:102022. [Google Scholar]
- 2.Frooghi M., Bahador A., Golchini A., Haghighat M., Ataollahi M., Javaherizadeh H. Perforated Meckel’s diverticulum in a 3-day-old neonate; a case report. Middle East Journal of Digestive Diseases. 2016 Oct;8(4):323. doi: 10.15171/mejdd.2016.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liaqat N., Mahomed A., Nayyar S.I., Akhtar N., Ali S., Haider N. Perforated Meckel’s diverticulum in neonates: a report of six cases and systematic review of the literature. Ann. Pediatr. Surg. 2022 Dec;18(1):1–9. doi: 10.1186/s43159-021-00154-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Tenreiro N., Moreira H., Silva S., Madureira L., Gaspar J., Oliveira A. Unusual presentation of a Meckel’s diverticulum: a case report. Int. J. Surg. Case Rep. 2015 Jan 1;16:48–51. doi: 10.1016/j.ijscr.2015.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gunadi Damayanti W., Saputra R.P., Ramadhita Ibrohim I.S., Lestiono A., Melati D., Permatahati W.I., Widowati T., Makhmudi A. Case report: complicated meckel diverticulum spectrum in children. Front. Surg. 2021 May 25;8:674382. doi: 10.3389/fsurg.2021.674382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.de Caso D.D. Meckel’s diverticulum. A case report. Int. J. Morphol. 2007;25(3):519–522. [Google Scholar]
- 7.Nishikawa T., Takei Y., Tsuno N.H., Maeda M. Perforation of Meckel’s diverticulum with enteroliths. Clin. J. Gastroenterol. 2012 Aug;5:298–301. doi: 10.1007/s12328-012-0313-6. [DOI] [PubMed] [Google Scholar]
- 8.Abizeid G.A., Aref H. Case report: preoperatively diagnosed perforated Meckel’s diverticulum containing gastric and pancreatic-type mucosa. BMC Surg. 2017 Dec;17:1–4. doi: 10.1186/s12893-017-0236-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bertozzi M., Melissa B., Radicioni M., Magrini E., Appignani A. Symptomatic Meckel’s diverticulum in newborn: two interesting additional cases and review of literature. Pediatr. Emerg. Care. 2013 Sep 1;29(9):1002–1005. doi: 10.1097/PEC.0b013e3182a315e5. [DOI] [PubMed] [Google Scholar]
- 10.Wang Y.J., Wang T., Xia S.L., Zhang Y.C., Chen W.B., Li B. Perforation of Meckel’s diverticulum in a very low birth weight neonate with severe pneumoperitoneum and review of literature. Turk. J. Pediatr. 2019 May 1;61(3):460–465. doi: 10.24953/turkjped.2019.03.025. [DOI] [PubMed] [Google Scholar]
- 11.Crankson S., Kadhi A., Al Tawil K., Ahmed I.A. Meckel’s diverticulum: a rare cause of intestinal perforation in a preterm newborn. Ann. Pediatr. Surg. 2013;9(4):147–149. [Google Scholar]
- 12.Huang C.C., Lai M.W., Hwang F.M., Yeh Y.C., Chen S.Y., Kong M.S., Lai J.Y., Chen J.C., Ming Y.C. Diverse presentations in pediatric Meckel’s diverticulum: a review of 100 cases. Pediatrics & Neonatology. 2014 Oct 1;55(5):369–375. doi: 10.1016/j.pedneo.2013.12.005. [DOI] [PubMed] [Google Scholar]
- 13.Alvares B.R., Yumioka A.S., Santos I.G. Uncommon presentation of perforated Meckel’s diverticulum in preterm newborn. Radiol. Bras. 2015 Jul;48:265–266. doi: 10.1590/0100-3984.2014.0134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sohrabi C., Mathew G., Maria N., Kerwan A., Franchi T., Agha R.A. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg Lond Engl. 2023;109(5):1136. doi: 10.1097/JS9.0000000000000373. [DOI] [PMC free article] [PubMed] [Google Scholar]