

Pancreatic metastasis from a renal cell carcinoma (PRCC) is rare, and diagnosis difficult. Recently, EUS-related procedures, including elastography, contrast-enhanced harmonic EUS (CE-EUS), and fine-needle aspiration (FNA), have been used as diagnostic tools for pancreatic tumor cases. Reported here are findings obtained with EUS-related procedures for PRCC diagnosis.
A 59-year-old woman underwent a computed tomography examination, which indicated multiple pancreatic tumors [Figure 1]. EUS findings revealed round tumors, in the head, body, and tail of the pancreas, with diameters of 15, 15, and 39 mm, respectively [Figure 2]. Furthermore, elastography results showed homogeneous blue patterns in the head and body tumors and a heterogeneous blue-predominant pattern in the tail tumor [Figure 3]. CE-EUS revealed hyperenhancement in the early phase in all 3 [Figure 4, Video 1]. Similar time-intensity curve (TIC) and calculated values were noted for all tumors regardless of size or location [Figure 5, Table 1]. A final diagnosis was successfully determined based on FNA results [Figure 6, Video 2].
Figure 1.

Computed tomography images. Hyperenhancement of tumors in the head, body, and tail of the pancreas in the arterial phase was noted. (A) Tumor in head. (B) Tumor in body. (C) Tumor in tail.
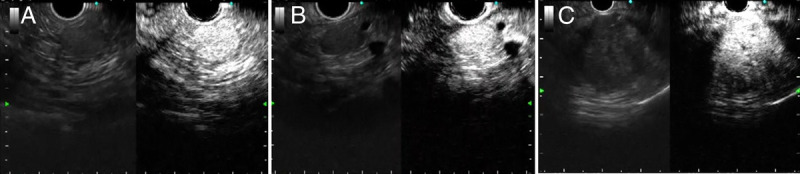
Figure 2.
EUS images. Conventional EUS revealed round isoechoic tumors, in the head, body, and tail of the pancreas. (A) Tumor in head. (B) Tumor in body. (C) Tumor in tail.
Figure 3.
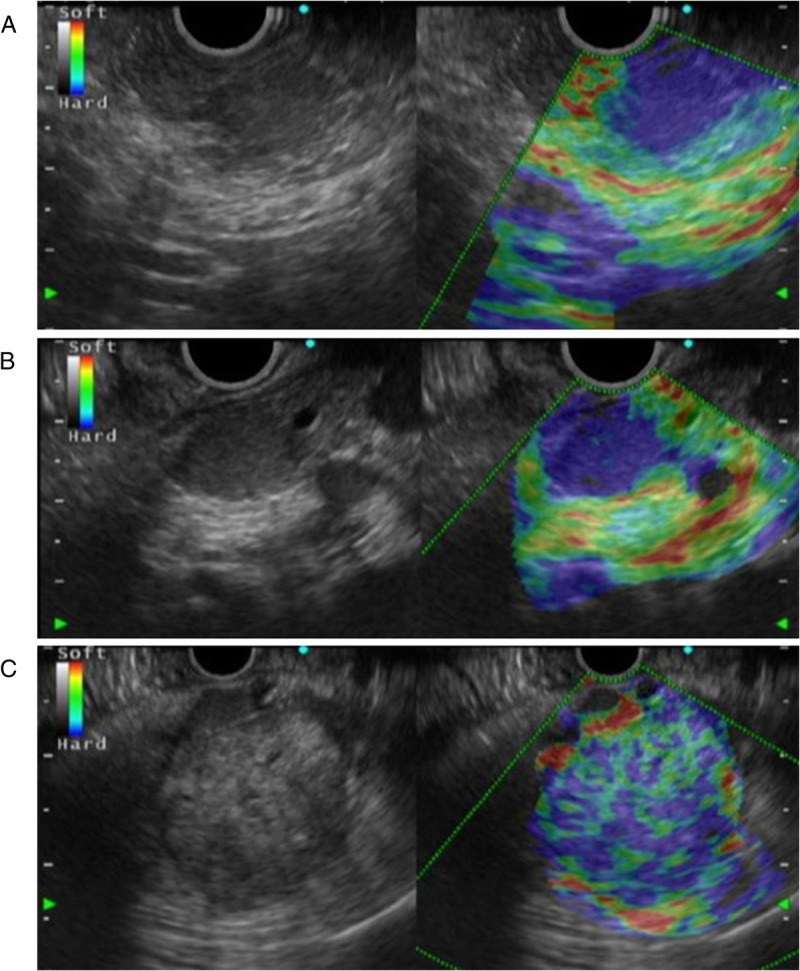
EUS elastography images. (A) Tumor in head. Homogeneous blue pattern suggesting malignant tumor. (B) Tumor in body. Homogeneous blue pattern suggesting malignant tumor. (C) Tumor in tail. Heterogeneous blue-predominant pattern suggesting malignant tumor with necrosis.
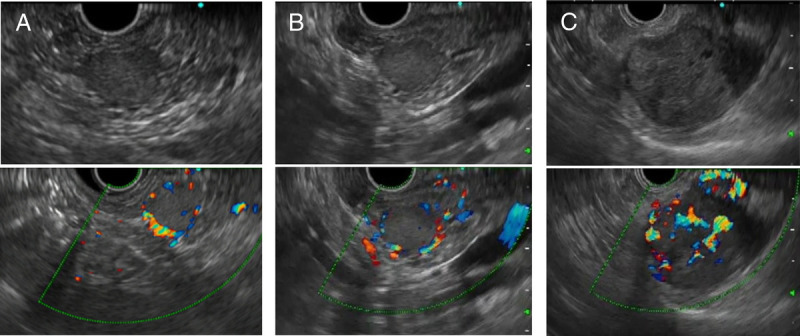
Figure 4.
Contrast-enhanced US images at peak. Images were obtained using contrast-enhanced harmonic EUS (EU-ME2 PREMIER PLUS; Olympus, Tokyo, Japan) at peak intensity after injection of perflubutane (Sonazoid; GE Healthcare Pharma, Tokyo, Japan). (A) Tumor in head. (B) Tumor in body. (C) Tumor in tail.
Figure 5.
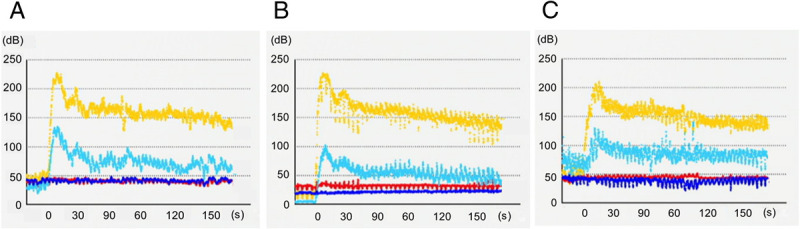
Time-intensity curve analysis results. Characteristic visual findings showing hyperenhancement and slow washout in 3 tumors were objectively obtained. Yellow line shows contrast intensity of pancreatic tumor. Light blue line shows contrast intensity of surrounding pancreatic parenchyma. Red line shows base echo intensity of pancreatic tumor before injection of the contrast agent. Blue line shows base echo intensity of surrounding pancreatic parenchyma before injection of the contrast agent. (A) Tumor in head. (B) Tumor in body. (C) Tumor in tail.
Table 1.
Calculated results from time-intensity curve analysis.
| Igain of tumor (dB) | Igain of pancreas parenchyma (dB) | ER | RR120 | |
|---|---|---|---|---|
| Head | 183.32 | 91.66 | 2.00 | 0.30 |
| Body | 213.90 | 100.00 | 2.14 | 0.34 |
| Tail | 161.20 | 72.20 | 2.23 | 0.35 |
ER: elevation rate [ER is (Igain of tumor)/(Igain of pancreatic parenchyma)]; Igain: peak intensity-base intensity; Igain of tumor/Igain of pancreatic parenchyma; RR120: reduction rate at 120 s; peak intensity-intensity at 120 s/peak intensity.
Figure 6.
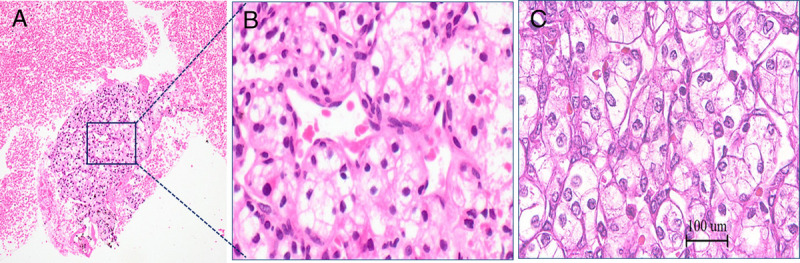
Histopathological findings. Referral to previous nephrectomy specimen findings confirmed metastasis from RCC. (A) FNA specimen from tumor in head. (B) High-power view of FNA specimen. (C) High-power view of nephrectomy specimen. FNA: fine-needle aspiration.
Video 1 Contrast-enhanced harmonic EUS findings, which included hyperenhancement and slow washout, were used for analysis of pancreatic metastasis from a renal cell carcinoma.
The video is only available at the official website of the journal (http://www.eusjournal.com).
Video 2 Fine-needle aspiration from tumor in the head. An EZ Shot 3 Plus, 22G (Olympus, Tokyo, Japan) was used.
Video is only available at the official website of the journal (http://www.eusjournal.com).
Although FNA can provide definitive results, those are not always accurate[1]; thus, an alternative method is needed when an adequate sample cannot be obtained. Diagnosis of PRCC requires differentiation from other pancreatic tumors, especially pancreatic neuroendocrine neoplasm (PNEN). Elastography findings showing a blue-predominant pattern indicate possible malignancy,[2] although additional evaluation is required for differentiation from PNEN. Takada et al reported precise CE-EUS values for TIC analyses of PNEN,[3] including enhancement ratio (ER) values of 1.51 for G1/G2 and 0.77 for G3/neuroendocrine carcinoma (NEC), whereas the reduction rate at 120 s (RR120) for each was 0.37 and 0.82, respectively. Precise TIC value for PRCC has not been reported. The ER of the present PRCCs was 2 units, beyond the value for PNEN, whereas the RR120 value was 0.3 units, equivalent to G1/G2 and lower than G3/NEC. Our results indicate that a high ER value suggests PRCC possibility. Furthermore, the low RR120 values were useful for differentiation from G3/NEC.
CE-EUS findings with TIC analysis are considered to be effective for PRCC diagnosis, whereas accumulation of quantified data will lead to a definitive diagnosis strategy.
Declaration of Informed Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Author Contributions
The authors provided care for the patient and also contributed to writing and editing the manuscript.
Source of Funding
None.
Contributor Information
Asumi Saima, Email: lunekuumn@gmail.com.
Hiroaki Tsunoda, Email: tsuno@me.com.
Koji Onishi, Email: kouji-onisi-mf@healthcarenet.jp.
Kousaku Kawashima, Email: kk461223@med.shimane-u.ac.jp.
Conflicts of Interest
The authors declare that they have no financial conflict of interest with regard to the content of this report.
References
- 1.Bechade D Palazzo L Fabre M, et al. EUS-guided FNA of pancreatic metastasis from renal cell carcinoma. Gastrointest Endosc 2003;58:784–788. [DOI] [PubMed] [Google Scholar]
- 2.Igresias-Garcia J Larino-Noia J Abdulkader I, et al. EUS elastography for the characterization of solid pancreatic messes. Gastrointest Endosc 2009;70:1101–1108. [DOI] [PubMed] [Google Scholar]
- 3.Takada S Kato H Saragai Y, et al. Contrast-enhanced harmonic endoscopic ultrasound using time-intensity curve analysis predicts pathological grade of pancreatic neuroendocrine neoplasm. J Med Ultrason 2019;46:449–458. [DOI] [PubMed] [Google Scholar]