

ABSTRACT
Introduction:
Pain management in pediatric dentistry is crucial for ensuring positive treatment outcomes and reducing patient suffering. This study aimed to evaluate postoperative discomfort and analgesic usage among pediatric dental patients undergoing various procedures in India.
Methodology:
A cross-sectional study was conducted at a tertiary care dental hospital in India from June 2023 to December 2023. A total of 150 pediatric patients aged 2–18 years who underwent different dental procedures were included. Data on postoperative discomfort and analgesic usage were collected immediately following the procedure and during follow-up phone calls.
Results:
Significant differences were found in immediate postoperative discomfort following pulpotomy (P = 0.03). Patients receiving primary stainless steel crowns (SSCs) alone or in combination with pulpotomy were significantly more likely to report discomfort (P < 0.001 and P < 0.05, respectively). No significant associations were observed between discomfort and sealants, preventive resin restorations, 1- or 2-surface restorations, or extractions. Over-the-counter analgesic usage was prevalent, particularly following SSC placement.
Conclusion:
This study highlights the variability in postoperative discomfort among pediatric dental patients undergoing different procedures in India. Tailored pain management strategies based on specific procedures are essential to minimize discomfort and improve patient outcomes in pediatric dentistry.
KEYWORDS: Analgesic usage, dental procedures, India, pediatric dentistry, postoperative discomfort
INTRODUCTION
In India, pediatric dental care is essential yet often overlooked, leading to inadequate pain management in children undergoing dental procedures.[1] Despite the availability of validated pain measurement scales such as the Wong-Baker FACES pain rating scale, misconceptions persist regarding children’s ability to communicate pain.[2] This gap in understanding contributes to undertreatment and unnecessary suffering among pediatric dental patients. Furthermore, limited research in Indian pediatric dentistry exacerbates the challenge of predicting and managing pain effectively.
To address this issue, this study investigated discomfort and analgesic usage following routine pediatric dental procedures, aiming to enhance pain prediction and management strategies. By evaluating pain experiences and analgesic needs in Indian children undergoing dental treatment, this research provides valuable insights into optimizing pediatric dental care practices, ultimately improving patient outcomes and reducing pain-related suffering in the Indian context.
METHODOLOGY
This cross-sectional study was conducted at Vyas Dental College and Hospital in India. Participants included children aged 2–18 years who underwent restorative or surgical dental procedures or fissure sealant preventive procedures from June 2023 to December 2023. Informed consent was obtained from a parent or guardian for each participant, and written consent was obtained from children aged 8 years and older. Ethical approval for the study was obtained from the institutional ethics committee (VDCH/IEC/2023/058).
A structured form was developed to gather demographic information, type of dental procedure, use of local anesthetic and nitrous oxide, behavior during treatment (Frankl Scale Rating),[3] and pain assessment using the Wong-Baker FACES pain rating scale. A pediatric dentist attempted to contact each parent or guardian within 48 hours post procedure to gather information on any complaints made by the child, presence and severity of discomfort, pain medication usage, effects of local anesthesia, and other relevant details. Statistical analysis was performed using appropriate tests such as the Wilcoxon-Mann-Whitney test to determine differences in pain among procedures and the exact Pearson’s Chi-square test to evaluate associations between discomfort, analgesic usage, and other variables. Descriptive statistics were computed for all variables.
RESULTS
All patients who could be reached by telephone agreed to respond to the script (100% response rate) and were included in the study. In total, 77 males and 73 females, ranging from 2–18 years old (mean age: 8.3 years; median age: 7.0 years), participated in the study. Sixty patients received nitrous oxide, and 86 received local anesthetic (2% lidocaine with 1:100,000 epinephrine). The specific frequency of each procedure and the mean age of children for each procedure are shown in Table 1.
Table 1.
Pain reporting and analgesic usage following pediatric dental procedures
| Procedure | n | Average age (years) | No. (%) reporting pain per procedure (%) | No. (%) taking analgesics (%) |
|---|---|---|---|---|
| Sealant only | 4 | 7 | 0 (0) | 0 (0) |
| Preventive resin | 10 | 12.6 | 2 (20) | 2 (20) |
| Restorations | ||||
| 1-surface restoration | 33 | 8 | 11 (33.3) | 10 (30.3) |
| 2-surface restoration | 39 | 9 | 12 (30.7) | 8 (23) |
| Stainless steel crown | 51 | 6.1 | 25 (49.01) | 21 (41.1) |
| SSC | ||||
| SSC + pulpotomy | 14 | 7.2 | 9 (64.2) | 8 (57.1) |
| Extraction | 21 | 8.4 | 5 (23.8) | 5 (23.8) |
The table provides a comprehensive overview of pain reporting and analgesic usage among pediatric dental patients following different dental procedures conducted in India from June 2023 to December 2023. Notably, among the procedures examined, those involving more invasive treatments such as stainless steel crown (SSC) placement and SSC combined with pulpotomy showed higher rates of pain reporting, with approximately 49.01% and 64.2% of subjects experiencing pain, respectively. Moreover, a significant proportion of these subjects, 41.1% and 57.1% respectively, required analgesics to manage their discomfort. Conversely, procedures such as sealant application and preventive resin restorations (PRRs) exhibited lower rates of pain reporting, with all subjects in the sealant-only group reporting no pain and not requiring analgesics.
Following the procedure, a notable discrepancy was observed specifically in the immediate postoperative period, particularly in the case of pulpotomy, which exhibited a significant increase in postoperative discomfort as evidenced by the Wong-Baker FACES pain rating scale (P = 0.03). However, no other statistically significant differences were detected immediately post procedure. During the follow-up phone call, it was noted that 42% of the children reported experiencing discomfort. Notably, patients who underwent procedures involving primary SSCs alone or in combination with pulpotomy were significantly more likely to report discomfort (P < 0.001 and P < 0.05, respectively) compared to those undergoing other procedures. Conversely, no significant association was observed between the presence of discomfort and procedures such as sealants, PRRs, 1- or 2-surface restorations, and extractions. The most commonly reported issues associated with anesthesia were numbness and lower lip-biting. Furthermore, 36% of the children received over-the-counter analgesics from their parents, either as a preventive measure or in response to the child’s complaint of discomfort [Figure 1].
Figure 1.
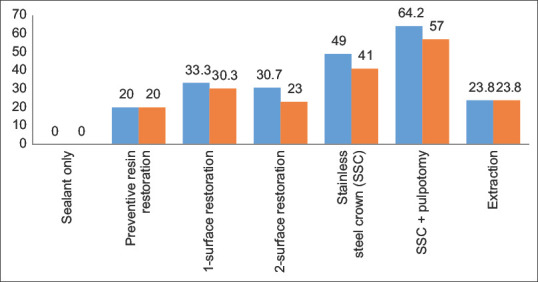
Postoperative pain and analgesic use
DISCUSSION
The findings of this study shed light on the prevalence of postoperative discomfort and analgesic usage among pediatric dental patients undergoing various dental procedures in India. The significant difference observed in immediate postoperative discomfort following pulpotomy highlights the importance of considering the specific nature of procedures in managing postoperative pain. This result aligns with previous research indicating that pulpotomy can lead to increased discomfort in pediatric patients due to its invasive nature and potential for pulp inflammation.[4]
Furthermore, the significant association between discomfort and procedures involving primary SSCs, both alone and in combination with pulpotomy, underscores the need for tailored pain management strategies for such cases. These findings are consistent with previous studies highlighting the potential for discomfort following SSC placement, attributed to factors such as tissue irritation, pressure on adjacent tissues, and difficulties in adjusting to the foreign object in the mouth.[5]
Conversely, the absence of significant discomfort reported in patients undergoing sealant-only procedures emphasizes the relatively low discomfort associated with noninvasive preventive treatments. This reaffirms the importance of early preventive dental care in reducing the likelihood of postoperative discomfort and the need for analgesic intervention.[6]
The observed gender difference in reporting numbness postoperatively, with a higher proportion of males experiencing this sensation compared to females, warrants further investigation. While the underlying reasons for this gender disparity remain unclear, it may reflect variations in pain perception and reporting between genders, highlighting the importance of considering gender-specific factors in pain management approaches.[7]
The high prevalence of over-the-counter analgesic usage among pediatric patients, particularly following SSC placement, underscores the need for effective pain management protocols in pediatric dentistry. This aligns with previous research emphasizing the importance of providing adequate pain relief measures to minimize postoperative discomfort and improve patient outcomes.[8]
CONCLUSION
In conclusion, this study provides valuable insights into the prevalence of postoperative discomfort and analgesic usage among pediatric dental patients in India. The findings underscore the importance of tailored pain management strategies based on the specific nature of dental procedures and highlight the need for further research to optimize pain management protocols in pediatric dentistry.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Jackson SL, Vann WF, Jr, Kotch JB, Pahel BT. Impact of poor oral health on children's school attendance and performance. Am J Public Health. 2011;101:1900–6. doi: 10.2105/AJPH.2010.200915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Garra G, Singer AJ, Taira BR, Chohan J, Cardoz H, Chisena E, et al. Validation of the wong-baker FACES pain rating scale in pediatric emergency department patients. Acad Emerg Med. 2010;17:50–4. doi: 10.1111/j.1553-2712.2009.00620.x. [DOI] [PubMed] [Google Scholar]
- 3.Mathur J, Diwanji A, Sarvaiya B, Sharma D. Identifying dental anxiety in children's drawings and correlating it with Frankl's behavior rating scale. Int J Clin Pediatr Dent. 2017;10:24–8. doi: 10.5005/jp-journals-10005-1401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Teeth IP. Guideline on Pulp Therapy for Primary-and Immature Permanent Teeth – Pulp Therapy Subcommittee. Guideline on Pulp Therapy for Primary and Immature Permanent Teeth. Council on Clinical Affairs, 1991 Revised 1998, 2001, 2004, 2009. [Google Scholar]
- 5.Fuks AB. Pulp therapy for the primary and young permanent dentitions. Dent Clin North Am. 2000;44:571–96. [PubMed] [Google Scholar]
- 6.Griffin SO, Barker LK, Wei L, Li CH, Albuquerque MS, Gooch BF Centers for Disease Control and Prevention (CDC) Use of dental care and effective preventive services in preventing tooth decay among U. S. Children and adolescents--Medical Expenditure Panel Survey, United States, 2003-2009 and National Health and Nutrition Examination Survey, United States, 2005-2010. MMWR Suppl. 2014;63:54–60. [PubMed] [Google Scholar]
- 7.Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL., 3rd Sex, gender, and pain: A review of recent clinical and experimental findings. J Pain. 2009;10:447–85. doi: 10.1016/j.jpain.2008.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.A FS, Ponraj S, Ramar K, A VS, S R, J G. Non-pharmacological behavior management techniques in pediatric dentistry: A bibliometric analysis. Cureus. 2023;15:e41329. doi: 10.7759/cureus.41329. [DOI] [PMC free article] [PubMed] [Google Scholar]