

Abstract
Introduction Wrist parameters measured on direct radiography are essential in diagnosing scaphoid-related pathologies and treatment. Although computed tomography has been used to establish normative for scaphoid measurement, no research has focused on Indian norms. This study aimed to determine the distribution and normal limits of parameters measured in our population's posteroanterior (PA) and direct lateral radiographs of the wrist.
Materials and Methods Two investigators conducted a prospective analysis of normal wrist radiographs in a single center. Radiology information system-picture archiving and communication system was used to collect standard digitized normal X-rays without significant osseous pathology over a year. The sample size was 600, distributed among age groups 18 to 30, 31 to 50, and 51 years and above. Scaphoid length, scaphoid width, scapholunate ratio, and scapholunate distance using both Cautilli and Gilula techniques were measured on a PA view, and scapholunate, radioscaphoid, and intrascaphoid angles were measured on a lateral view. As the lunate morphology is supposed to affect carpal kinematics with the scaphoid, the same was evaluated using the Viegas classification.
Results A total of eight measurements were documented. Scaphoid length, scaphoid width measurements, and lateral intrascaphoid angle were more in males than in females and were found to be statistically significant. No other parameters showed any significance in terms of age and relation to lunate morphology.
Conclusion The study offers a comprehensive analysis of measuring parameters specific to the Indian population. For the first time, the measurement of scapholunate distance was conducted utilizing two distinct methodologies. The normative intrascaphoid angle range and clinical implications were determined.
Keywords: normative, scaphoid, Indian, scapholunate, intrascaphoid
Introduction
Wrist biomechanics relies on the scaphoid, which links the proximal and distal carpal rows. Knowledge of the standard lengths and widths of the scaphoid at different levels may be beneficial for inventory management in the operating room during scaphoid fracture management, in instances where screw placement is required, and in nonunion. 1 2
Several measurements and indices, such as the scapholunate (SL) angle, the scaphoid lunate ratio, and the SL gap, have been used to quantify and diagnose carpal instability. 3 4 5 The radioscaphoid angle has been recognized as a quantifiable measure for assessing outcomes in intercarpal arthrodesis. 6 The lateral intrascaphoid is described to correlate with scaphoid malunion, which alters wrist biomechanics. 7 Type II lunate shape with its lunohamate articulation is described to reduce dorsal intercalated segmental instability (DISI) deformity as it is invariably connected to scaphoid. 8
The contralateral wrist cannot be used as a reference in bilateral conditions. Some conditions that appear to be unilateral have very modest asymptomatic involvement on the side considered normal. 9 Several studies on a normal database of posterior-anterior (PA) radiographic wrist measurements are not exclusive to scaphoid-related parameters. 10 11 There have only been a few studies on normative data for the scaphoid, which are mainly computed tomography (CT)-based. 12 There is no normal morphometric radiography database of the scaphoid in a representative sample of the Indian population. This study aimed to establish a precedent regarding the normality of scaphoid bone measurements among the Indian population, focusing on their clinical significance. This article aims to provide a standard normative database of PA and lateral radiographic measurements of the scaphoid and its relationship to lunate in an Indian population sample. The database would facilitate surgeons in achieving optimal corrections for scaphoid-related disorders in the Indian population.
Materials and Methods
After institutional board ethical clearance, we conducted a prospective analysis of normal PA and lateral wrist radiographs. Using the radiology information system-picture archiving and communication system (RIS-PACS), we collected standard digitized normal wrist X-rays and measured various linear and angular parameters over 1 year. Normal wrist X-rays were based on radiographs of patients presenting with contusion, laceration, and abrasions to the hand and wrist and radiographs of the wrist obtained from patients presenting with carpal tunnel syndrome, tenosynovitis, and benign swellings such as ganglion and lipoma. Contralateral radiographs of patients presenting with radius malunion, scaphoid nonunion, and Kienbock's disease, which were taken as controls, were also included in the study. Patients with a history of previous fracture or surgery, as well as those whose wrist radiographs indicated skeletal immaturity, were excluded from the study. The sample size for the study was calculated to be 600 X-rays, which was attempted to be evenly distributed among the age groups of 18 to 30, 31 to 50, and 51 years and above. We compared the carpal measurements in these age groups and also between males and females within those age groups. Only the true PA and lateral (Scaphoid, Pisiform and Capitate [SPC]) radiographs were included in the study, as any deviation from this would result in improper measurement of indices. 13
Standard radiographic measurements were taken on a PA view.
Scaphoid central axis : The scaphoid axis is defined as the line that passes through the tip of the proximal pole and the midpoint of the tangential line traced to the distal articular surface at the distal pole.
1. Scaphoid length ( Fig. 1A ): The length of the scaphoid bone is determined by measuring along the scaphoid axis, which is represented by a line from the tip of the proximal pole to the midpoint of a line drawn tangent to the distal articular surface of the scaphoid at the distal pole. 5 14
2. Scaphoid width ( Fig. 1B ): The term superior width refers to the measurement of width at the distal pole, taken at a right angle to the scaphoid axis. The measurement of middle width is taken at the midpoint of the scaphoid axis, perpendicular to it. On the other hand, inferior width is the measurement taken at the proximal pole, perpendicular to the scaphoid axis. 5
-
3. SL distance/gap ( Fig. 1C ): We quantified the SL gap via two methodologies:
(i) The SL gap is determined by measuring the distance from the proximal ulnar corner of the scaphoid to the proximal radial corner of the lunate as described by Cautilli and Wehbé. 4
(ii) The SL gap is assessed at the central point of the flat ulnar facet of the scaphoid and the radial facet of the lunate, as described by Gilula and Weeks. 15
4. SL ratio ( Fig. 1D ): The SL ratio is determined by dividing the scaphoid length by the lunate length. Lunate length is measured along its axis, that is, the line perpendicular to the line joining the medial and lateral corners of the anterior horn. 5
Fig. 1.

Determination of key landmarks and linear and angular measurements.
On the lateral radiograph, we measured:
5. SL angle ( Fig. 1E ): The angle formed by the longitudinal axis of the scaphoid and lunate. The scaphoid axis on a lateral radiograph can be determined by drawing a line that passes between the proximal and distal volar convexities of the scaphoid bone. The lunate axis is at a right angle to a line connecting the distal poles of the lunate. 3
6. Radioscaphoid angle ( Fig. 1F ): The angle formed between the longitudinal axis of the scaphoid and the radius on a lateral radiograph. 6
7. Intrascaphoid angle ( Fig. 1G ): The angle formed between the perpendicular lines on the scaphoid's distal and proximal articular surfaces (tangential drawn to the articular surfaces). 7
8. Lunate morphology ( Fig. 2 )
Fig. 2.
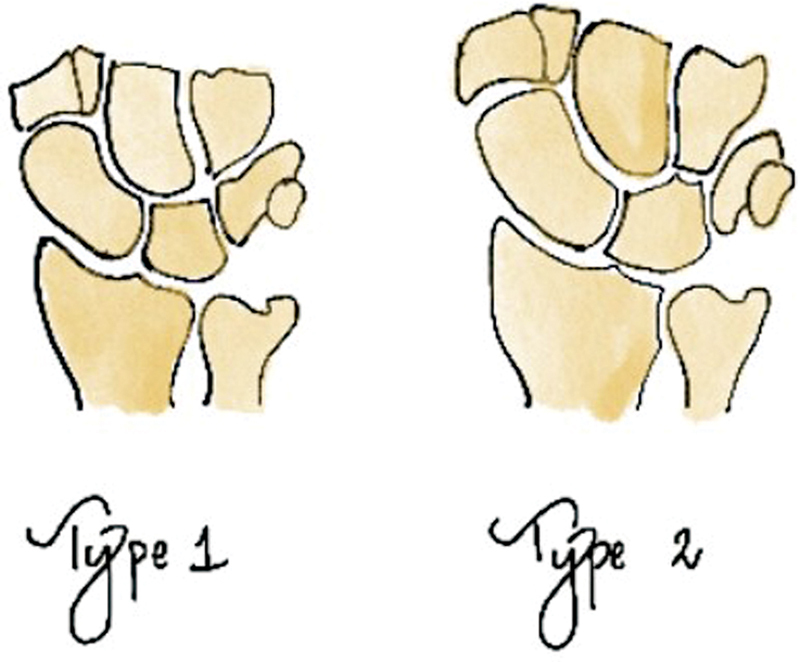
Lunate morphology as per Viegas classification.
Haase et al 8 and Rhee et al 16 were the first investigators to discover the significant influence of lunate type (morphology) on carpal misalignment in persons with scaphoid nonunions and complete SL ligament tears, respectively. In 1990, Viegas defined the lunate morphology based on the existence of a medial facet. 17 The lunate with a single facet that articulates with the capitate bone is classed as type I, while the lunate with an extra facet that articulates with the hamate bone is classified as type II.
Statistics
The coefficient of variation (CoV) was computed for all the measurements documented in the literature. The CoV is calculated by multiplying the standard deviation (SD) by 100 and dividing the result by the mean. The sample size was determined using the formula, Z 2 σ 2 / D 2 , where Z represents the critical value (1.96), σ represents the SD, and D represents the margin of error. The study's sample size was determined to be 600 X-rays, with an attempt to evenly distribute them among each group. The data was analyzed via the most recent version of SPSS and presented as the sample mean and SD. A p -value below 0.05 was deemed to have statistical significance. An intraclass correlation test was used to compare the measurements between two observers. Additionally, the lead investigator took measurements 1 month apart to compare within their own observations for the pilot study.
Results
Six hundred radiographs were analyzed, including 316 males and 284 females in three different age groups (18–30, 31–50, and more than 50 years). We analyzed 200 X-rays from each age group. Measurements to study the gender variability showed that the scaphoid length, superior, middle, and inferior width measurements, and lateral intrascaphoid angle were more in males than in females; this difference was statistically significant ( p < 0.05) with the Mann–Whitney U test ( Table 1 ).
Table 1. Descriptive statistical data for the measured parameters with sex distribution.
| Parameters | Male, mean (SD) (316) |
Female, mean (SD) (214) |
p -Value (Mann–Whitney U test) |
|---|---|---|---|
| Scaphoid length (mm) | 21.8 (1.7) | 21.4 (1.6) | 0.0.005 |
| Scaphoid width (mm) (superior) |
13.1 (1.6) | 12.3 (1.5) | < 0.0001 |
| Scaphoid width (mm) (middle) |
8.7 (1.2) | 7.8 (1) | < 0.0001 |
| Scaphoid width (mm) (inferior) |
5.8 (0.9) | 5.2 (0.8) | < 0.0001 |
| SL ratio | 1.9 (0.2) | 1.9 (0.3) | 0.9 |
| SL distance, proximal (mm) | 3.4 (0.7) | 3.3 (0.7) | 0.14 |
| SL distance, middle (mm) | 1.5 (0.5) | 1.6 (0.5) | 0.05 |
| Radio scaphoid angle (degrees) | 42.4 (5.1) | 43 (4.9) | 0.097 |
| Lateral intrascaphoid angle (degrees) | 24.2 (2.6) | 23.7 (2.5) | 0.007 |
| Lateral scapholunate angle (degree) | 48.3 (6.7) | 48.1 (7.1) | 1 |
Abbreviations: SD, standard deviation; SL, scapholunate.
Measurements to study the variability in age showed that none of the parameters exhibited any significant variation with age on the Kruskal–Wallis test ( Table 2 ).
Table 2. Descriptive statistical data for the measured parameters with age distribution.
| Parameters (mean, SD) | 18–30 y (225) |
31–50 y (225) |
> 50 y (150) |
p
-Value
(Kruskal–Wallis test) |
|---|---|---|---|---|
| Scaphoid length (mm) | 21.8 (1.5) | 21.9 (1.5) | 22.1 (1.6) | 0.08 |
| Scaphoid width (mm) (superior) |
12.5 (1.4) | 12.8 (1.6) | 12.9 (1.8) | 0.2 |
| Scaphoid width (mm) (middle) |
8.4 (1.2) | 8.2 (1.2) | 8.3 (1.2) | 0.7 |
| Scaphoid width (mm) (inferior) |
5.5 (0.9) | 5.5 (0.9) | 5.5 (0.9) | 0.9 |
| SL ratio | 1.9 (0.2) | 1.9 (0.2) | 1.9 (0.3) | 0.09 |
| SL distance, proximal (mm) | 3.4 (0.6) | 3.2 (0.7) | 3.4 (0.7) | 0.08 |
| SL distance, middle (mm) | 1.6 (0.5) | 1.6 (0.5) | 1.5 (0.5) | 0.5 |
| Radio scaphoid angle (degrees) | 42.8 (4.8) | 42.6 (5.4) | 42.7 (4.7) | 0.6 |
| Lateral intrascaphoid angle (degrees) | 24 (2.4) | 24 (2.6) | 23.9 (2.6) | 0.7 |
| Lateral scapholunate angle (degrees) | 48.8 (6.4) | 48.6 (6.9) | 47.1 (7.1) | 0.07 |
Abbreviations: SD, standard deviation; SL, scapholunate.
Interclass and intraclass correlations for all the measurements showed excellent agreement between the observers ( Table 3 ).
Table 3. Descriptive statistical data for the measured parameters with inter- and intraclass correlation.
| Parameters | Interclass correlation | %95 CI | Intraclass correlation | %95 CI |
|---|---|---|---|---|
| Scaphoid length (mm) | 0.994 | 0.994 (0.986–1.003) | 0.994 | 0.994 (0.993–0.995) |
| Scaphoid width (superior) (mm) | 0.999 | 0.999 (0.995–1.003) | 0.999 | 0.999 (0.998–0.999) |
| Scaphoid width (middle) (mm) | 0.998 | 0.998 (0.994–1.003) | 0.998 | 0.998 (0.998–0.999) |
| Scaphoid width (inferior) (mm) | 0.998 | 0.998 (0.993–1.004.) | 0.997 | 0.997 (0.997–0.998) |
| Lunate length (mm) | 0.996 | 0.996 (0.991–1.003) | 0.997 | 0.997 (0.995–0.998) |
| SL distance, proximal (mm) | 0.991 | 0.991 (0.981–1.002) | 0.991 | 0.991 (0.989–0.993) |
| SL distance, middle (mm) | 0.998 | 0.998 (0.994–1.003) | 0.988 | 0.988 (0.986–0.990) |
| Scapholunate ratio | 0.998 | 0.998 (0.994–1.003) | 0.998 | 0.998 (0.998–0.999) |
| Radio scaphoid angle (degrees) | 0.989 | 0.989 (0.977–1.001) | 0.988 | 0.988 (0.986–0.990) |
| Lateral intrascaphoid angle (degrees) | 0.955 | 0.955 (0.931–0.979) | 0.954 | 0.954 (0.946–0.9610 |
| Lateral scapholunate angle (degrees) | 0.994 | 0.994 (0.985–1.003) | 0.994 | 0.994 (0.992–0.995) |
Abbreviations: CI, confidence interval; SL, scapholunate.
Lunate morphology did not influence the linear and angular measurements in association with scaphoid articulation ( Table 4 ).
Table 4. Descriptive statistical data for the measurements between the two lunate morphology as described by Viegas.
| Parameters | Type I (343) | Type II (257) | p -Value |
| SL distance proximal | 3.3 (0.7) | 3.3 (0.7) | 0.5 |
| SL distance middle | 1.5 (0.5) | 1.6 (0.5) | 0.1 |
| Radio scaphoid angle | 42.6 (5.1) | 42.9 (4.8) | 0.3 |
| Lateral intrascaphoid angle | 23.9 (2.6) | 23.9 (2.5) | 0.9 |
| Lateral scapholunate angle | 47.9 (6.9) | 48.7 (6.7) | 0.2 |
Abbreviation: SL, scapholunate.
Discussion
In routine clinical practice, two-dimensional plain X-rays in both the PA and lateral planes are the fundamental approach to imaging the wrist. Diagnosing pathological conditions should be primarily based on the analysis of X-rays, followed by additional investigations as deemed necessary. 5 X-ray is the commonly performed index investigation for assessment of injuries related to scaphoid. When assessing the congruity of the carpus, lateral radiographs are essential as the intercarpal bony congruence is diagnostic for many wrist conditions. 3 The literature on radiographic studies on carpal measurements is not exclusive to scaphoid measurements and is part of carpal and wrist measurements. 9 Most recent scaphoid normative studies are CT-based, with the sample size ranging from 80 to 120. 12 There is no published normal morphometric radiographic database of the scaphoid in the Indian population. Hence, this study was undertaken.
The scaphoid bone dimensions must be considered when choosing implants for internal fixation. Measurements determine the screw length and the number of screws needed to compress and reduce by various levels. Our storage inventory includes headless compression screws in 2.4- and 3-mm diameters ranging from 16 to 40 mm. It is crucial to find the best screw sizes for surgical outcomes, especially in patients with scaphoid nonunion, where we use a radiograph of the normal side to evaluate screw length. 1 2 In surgical cases, the inserted guidewire measures scaphoid screw length, although knowing the average length in men and women is helpful. Our data showed that male scaphoid length averaged 21.8 (1.8) mm and females 21.4 (1.6) mm. It was statistically significant ( p = 0.005). Belgian research by Feipel et al 5 found an average length of 22 mm. Iranian researchers 10 analyzed Mashhad residents' radiological indices. The study found a mean scaphoid length of 23.1 (3.6) mm, with males at 25.5 mm and females 20.5 mm. These findings differ slightly from our study. The mean superior, middle, and inferior widths were 12.5 (1.4), 8.3 (1.2), and 5.5 (0.9) mm. These measurements were slightly lower than Feipel et al. 5 We found that males had longer scaphoid length, superior, middle, and inferior widths, and a larger lateral intrascaphoid angle. This difference was significant ( p < 0.05) using the Mann–Whitney U test. Angular measurements can vary with ageing due to degenerative changes. 14 We found no significant difference between linear and angular measurements with age.
The main characteristics of SL dissociation are scaphoid flexion and lunate extension, leading to DISI. Changes in the PA projections of these two bones would reduce the SL ratio. The average PA SL ratio in our population was 1.94 (SD 0.23), slightly more than that described by Feipel et al, which was 1.4. 5 However, there was no significant difference among the various age groups and genders. The PA SL ratio below 1.00 would be considered abnormal, suspecting dissociation leading to carpal instability.
A SL distance greater than 5 mm is considered pathological and is a measure of SL dissociation leading to instability. If there is no foreshortened scaphoid or “cortical ring sign” with the wrist in the neutral position, a SL distance of up to 5 mm should be regarded as within normal limits. Due to the considerable heterogeneity observed in the criteria employed for diagnosing SL dissociation, it was deemed imperative to establish a standard reference measurement for SL distance in asymptomatic wrists of individuals lacking any history of trauma. None of the studies done to date measures SL gap by two separate methods (Cautilli and Wehbé and Gilula and Weeks method), which helps in the assessment of carpal instability. The article by Cautilli and Wehbé 4 examined radiographs of 100 asymptomatic individuals. Mean values of 3.7 (0.6) mm were obtained, with females having 3.6 (0.5) mm and males having 4 (0.5) mm compared to our study, where females had 3.3(0.7) mm and males had 3.4 (0.7) mm.
Gilula and Weeks 15 state that SL dissociation can be identified when the distance exceeds 2 mm, and a diagnosis is confirmed when the measurement is 4 mm or above. According to our study, the average scapholunate distance (SLD), measured using the Gilula and Weeks method, was 1.6 (0.5) mm in females and 1.5 (0.5) mm in males. In our study, the average SLD was 1.6 (0.5) mm for individuals aged 18 to 30 years, 1.6 (0.5) mm for individuals aged 31 to 50 years, and 1.5 (0.5) mm for individuals above 50 years of age. There was no statistically significant disparity in the scores among the gender and age categories. The study conducted by Katayama et al 18 in 2015 included 134 healthy individuals. The findings revealed that the average measurements for men and women using the Gilula and Weeks technique were 1.2 (0.2) mm for both genders. Hence, our SL distance values obtained from both methods are similar to those reported in the existing scientific literature.
A cadaveric investigation by Bain et al 19 examined lunate morphology's effect on carpus three-dimensional kinematics. Compared to type II wrists, type I wrists (Viegas) had a statistically significant increase in radiocarpal joint mobility which was attributed to lunatohamate articulation by Haase et al. 8 Further lunatohamate articulation may protect against SL instability after a scaphoid fracture. Our study on two-dimensional normal radiographs found no significant changes in lunate morphology and SL distance.
In normal wrists, the SL angle averages 46 degrees and ranges between 30 and 60 degrees, according to Linscheid and colleagues. 14 In 1989, Nakamura et al 20 examined 84 wrist radiographs from healthy individuals and found an average angle of 56 degrees. In 2003, Thienpont et al 21 examined 126 wrist radiographs from healthy individuals and found an average angle of 53.5 degrees. A recent survey in a representative Turkish population found that mean Scapholunate angle (SLA) value was 56.2 (12.2) degrees. Females had a mean scpholunate angle (SLA) value of 56.9 (12.6) degrees and males 55.04 (11.5) degrees. In the age group of 18 to 30 years it was 55.7 (11.7) and 55.9 (11.7) degrees in the age group of 31 to 50 years, and the age group over 50 years had 57.2 (13.7) degrees. However, there were no statistically significant differences between gender and age groups. Our study found that males had an average SL angle of 48.3 (6.7) degrees and females 48.1 (7.06) degrees. No age or gender difference was statistically significant. Compared to the normal range, the values are low. Additionally, lunate morphology did not differ in angular measures.
Intrascaphoid malunion substantially alters wrist biomechanics. Because of an increased lateral intrascaphoid angle, truncated volar cortex generates a “humpback” deformity. SL angle and carpal bone links change with scaphoid anatomy. This produces DISI. The lateral intrascaphoid angle best delineated positive and negative clinical outcomes, according to Amadio et al. 7 The study determined satisfactory and unsatisfactory results using a 35-degree lateral intrascaphoid angle criterion. No studies have determined intrascaphoid angle norms. Our study demonstrated a statistically significant mean intrascaphoid angle of 24.2 (2.6) degrees in males and 23.7 (2.5) degrees in females ( p = 0.007). Additionally, lunate morphology did not affect angular measurements.
A shift in scaphoid bone orientation (vertical or horizontal) during intercarpal arthrodesis operations like scaphotrapeziotrapezoid (STT) or scaphocapitate (SC) fusion affects wrist range of motion. Minamikawa et al's cadaveric investigation recommends radioscaphoid angle of 41 to 60 degrees for STT fusion and 30 to 57 degrees for SC fusion for optimal and acceptable motion in all four planes. 6 In the present scenario, understanding the normative radioscaphoid angle is critical. Radioscaphoid angles averaged 42.4 (5.1) in men and 43 (4.9) in women in our study. There were no significant angle changes with age.
In contrast to previous studies conducted on a comparable topic, 22 23 the sample size of the cohort under investigation in our study is substantial with a prospective design; nonetheless, further efforts are required to ensure adequate representation of diverse ethnic backgrounds. The study group lacks acceptable homogeneity regarding age and gender distribution, and the body mass index has not been computed. Two authors utilized the PACS system to conduct all necessary procedures electronically, and subsequently, the reliability of both interobserver and intraobserver was assessed.
To conclude, our study evaluated eight scaphoid-specific variables across age and gender. Males had larger scaphoid length, superior, middle, and inferior widths, and lateral intrascaphoid angles than females. with a statistical significance ( p < 0.05). This study was one of the first to quantify SL distance using two methods. Our research has established this clinically essential information for scaphoid malunion by providing normal intrascaphoid angles in different age groups and genders. A comprehensive collection of normal X-ray readings helps investigate pathologies. The data may predict long-term functional outcomes in scaphoid fracture, wrist instability, and wrist arthritis patients.
Acknowledgments
We extend our sincerest gratitude to Dr. Mukund Thatte for his visionary guidance and unwavering support in embarking on the normative data of the Indian hand. His foresight and encouragement have been instrumental in steering our research endeavors toward a deeper understanding of Indian demographics and contributing significantly to advancing our scientific knowledge.
Funding Statement
Funding None.
Conflict of Interest None declared.
Ethical Approval
Approval Letter Number: KHIEC/876/221.
Authors' Contributions
A.K.B. was responsible for the concept, data measurement analysis, statistics, and manuscript editing. M.P.G. acted as the principal investigator, handling measurement and analysis, as well as manuscript writing. A.S. contributed to data collection, measurements, and analysis.
References
- 1.Patel S, Giugale J, Tiedeken N, Debski R E, Fowler J R. Impact of screw length on proximal scaphoid fracture biomechanics. J Wrist Surg. 2019;8(05):360–365. doi: 10.1055/s-0039-1685514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Yildirim B, Deal D N, Chhabra A B. Two-screw fixation of scaphoid waist fractures. J Hand Surg Am. 2020;45(08):7830–7.83E6. doi: 10.1016/j.jhsa.2020.03.013. [DOI] [PubMed] [Google Scholar]
- 3.Larsen C F, Mathiesen F K, Lindequist S. Measurements of carpal bone angles on lateral wrist radiographs. J Hand Surg Am. 1991;16(05):888–893. doi: 10.1016/s0363-5023(10)80156-x. [DOI] [PubMed] [Google Scholar]
- 4.Cautilli G P, Wehbé M A. Scapho-lunate distance and cortical ring sign. J Hand Surg Am. 1991;16(03):501–503. doi: 10.1016/0363-5023(91)90022-4. [DOI] [PubMed] [Google Scholar]
- 5.Feipel V, Rinnen D, Rooze M. Postero-anterior radiography of the wrist. Normal database of carpal measurements. Surg Radiol Anat. 1998;20(03):221–226. [PubMed] [Google Scholar]
- 6.Minamikawa Y, Peimer C A, Yamaguchi T, Medige J, Sherwin F S. Ideal scaphoid angle for intercarpal arthrodesis. J Hand Surg Am. 1992;17(02):370–375. doi: 10.1016/0363-5023(92)90421-k. [DOI] [PubMed] [Google Scholar]
- 7.Amadio P C, Berquist T H, Smith D K, Ilstrup D M, Cooney W P, III, Linscheid R L. Scaphoid malunion. J Hand Surg Am. 1989;14(04):679–687. doi: 10.1016/0363-5023(89)90191-3. [DOI] [PubMed] [Google Scholar]
- 8.Haase S C, Berger R A, Shin A Y. Association between lunate morphology and carpal collapse patterns in scaphoid nonunions. J Hand Surg Am. 2007;32(07):1009–1012. doi: 10.1016/j.jhsa.2007.06.005. [DOI] [PubMed] [Google Scholar]
- 9.Schuind F, Alemzadeh S, Stallenberg B, Burny F. Does the normal contralateral wrist provide the best reference for X-ray film measurements of the pathologic wrist? J Hand Surg Am. 1996;21(01):24–30. doi: 10.1016/s0363-5023(96)80150-x. [DOI] [PubMed] [Google Scholar]
- 10.Vaezi T, Hassankhani G G, Ebrahimzadeh M H, Moradi A. Evaluation of normal ranges of wrist radiologic indexes in Mashhad population. Arch Bone Jt Surg. 2017;5(06):451–458. [PMC free article] [PubMed] [Google Scholar]
- 11.Yalçın A, Polat A. Evaluation of radiographic measurements of the wrist in the Turkish population. J Surg Med [Internet] 2022;6(01):36–42. [Google Scholar]
- 12.Guldbrandsen C W, Radev D I, Gvozdenovic R. Normal ranges for measurements of the scaphoid bone from sagittal computed tomography images. J Hand Surg Eur Vol. 2021;46(06):594–599. doi: 10.1177/1753193420987522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bhat A K, Kumar B, Acharya A. Radiographic imaging of the wrist. Indian J Plast Surg. 2011;44(02):186–196. doi: 10.4103/0970-0358.85339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Schuind F A, Linscheid R L, An K N, Chao E Y. A normal data base of posteroanterior roentgenographic measurements of the wrist. J Bone Joint Surg Am. 1992;74(09):1418–1429. [PubMed] [Google Scholar]
- 15.Gilula L A, Weeks P M. Post-traumatic ligamentous instabilities of the wrist. Radiology. 1978;129(03):641–651. doi: 10.1148/129.3.641. [DOI] [PubMed] [Google Scholar]
- 16.Rhee P C, Moran S L, Shin A Y. Association between lunate morphology and carpal collapse in cases of scapholunate dissociation. J Hand Surg Am. 2009;34(09):1633–1639. doi: 10.1016/j.jhsa.2009.06.017. [DOI] [PubMed] [Google Scholar]
- 17.Viegas S F, Wagner K, Patterson R, Peterson P. Medial (hamate) facet of the lunate. J Hand Surg Am. 1990;15(04):564–571. doi: 10.1016/s0363-5023(09)90016-8. [DOI] [PubMed] [Google Scholar]
- 18.Katayama T, Ono H, Furuta K, Akahane M, Omokawa S. Clinical radiographic features of the wrist without osteoarthritis and its relations to age and sex in Japanese. Hand Surg. 2015;20(01):59–65. doi: 10.1142/S0218810415500082. [DOI] [PubMed] [Google Scholar]
- 19.Bain G I, Clitherow H D, Millar S et al. The effect of lunate morphology on the 3-dimensional kinematics of the carpus. J Hand Surg Am. 2015;40(01):81–90. doi: 10.1016/j.jhsa.2014.09.019. [DOI] [PubMed] [Google Scholar]
- 20.Nakamura R, Hori M, Imamura T, Horii E, Miura T.Method for measurement and evaluation of carpal bone angles J Hand Surg Am 198914(2 Pt 2):412–416. [DOI] [PubMed] [Google Scholar]
- 21.Thienpont E, Mulier T, De Smet L. Radiographic analysis of anatomic risk factors for scapholunate dissociation. Acta Orthop Belg. 2003;69(03):246–251. [PubMed] [Google Scholar]
- 22.Jafari D, Taheri H, Shariatzade H, Mazhar F N, Jalili A, Ghahramani M. Radiographic indices in one hundred fifty normal Iranian wrists. Med J Islam Repub Iran. 2012;26(03):132–139. [PMC free article] [PubMed] [Google Scholar]
- 23.Omadachi S E, Gwunireama I U, Aigbogun E O., Jr Radiologic assessment of angular wrist parameters of asymptomatic Nigerians. Acad Anatomica Int. 2017;3(02):52–57. [Google Scholar]