

Abstract
BACKGROUND:
The trajectories of late preterm development from infancy to kindergarten reading and math, and predictors of academic resilience and risk are unknown.
METHODS:
Sample included 1200 late preterm infants (LPIs) from the Early Childhood Longitudinal Study, Birth Cohort. Objective measurements of development at 9 and 24 months (Bayley-SFR) and reading and math academic achievement at preschool and kindergarten were standardized; trajectories of late preterm development from 9 months to kindergarten reading and math were identified using latent class growth analysis. Multinomial logistic regression [aOR, 95% CI] identified predictors of academic resilience and risk.
RESULTS:
Four trajectory groups were observed for reading and three for math. More optimal trajectories (in reading and math) and academic resilience were associated with experiencing sensitive parenting and preschool attendance. Suboptimal (at-risk) trajectories (in reading or math) and an increased odds of academic risk were associated with <high school education, twin/multiple gestation, prenatal smoking and male sex.
CONCLUSIONS:
LPI trajectories varied from infancy to kindergarten. More sensitive parenting and preschool attendance predicted academic resilience, and should be encouraged. Select risk factors (prenatal smoking, twin/multiple gestation, male sex, <high school education) predicted academic risk, and can help identify LPIs who might benefit from closer monitoring prior to school entry.
INTRODUCTION
Late preterm infants (LPIs: infants born between 340/7 and 366/7 weeks gestation) account for 75% of preterm births,1 translating to more than 400,000 late preterm births per year.2 While it is well documented that LPIs have developmental deficits compared to infants born full term,3–5 the magnitude of these deficits is relatively small compared to infants born at earlier gestational ages.4–7 At a population level, the majority of LPIs are performing at grade level without significant developmental delays.6 A significant gap in the literature relates to the patterns of developmental variability within the population of LPIs, including which LPIs will have more optimal trajectories, suggestive of academic resilience, and which are at risk for suboptimal trajectories, consistent with academic risk. Because children’s academic resilience is an important predictor of later school success and well-being,8 identifying the factors associated with better school performance is critical to helping LPIs thrive. Relatedly, the preschool years are a time when the developmental vulnerabilities of late preterm children emerge.3 Because LPIs are less likely to receive early intervention services compared to infants born very preterm,9 identifying the factors associated with academic risk may help target LPIs who may benefit from early intervention to prevent the emergence of school difficulties.5
Previous research, largely focused on very preterm infants, has examined the social and biological factors associated with developmental risk,10–13 with a relatively recent interest in the factors associated with resilience.14–19 Modifiable factors which have been associated with more optimal development in very preterm infants include a history of sensitive caregiving,16–18 and preschool attendance.20,21 While we hypothesize that these early experiences are similarly protective in LPIs, there is a paucity of research examining predictors of academic resilience in LPIs, which this study will address. Relatedly, factors associated with developmental risk in very preterm infants, have included a history of being born small for gestational age (SGA),22 socioeconomic adversity,11,12 and lower maternal education.13 Compared to full-term infants, socioeconomic risks23–25 have also been associated with poorer infant outcomes in children born moderate-late preterm; however, associations with early learning and kindergarten academic outcomes are relatively understudied. We were interested in identifying risk factors that could distinguish the most at-risk LPIs who could benefit from closer developmental monitoring and early intervention prior to school entry, and relatedly, we were interested in identifying factors that could foster more optimal academic outcomes. Because LPIs are not typically followed in neonatal follow-up clinics, identifying predictors associated with academic risk may help individualize the developmental care and anticipatory guidance provided to this population, which accounts for the majority of infants born preterm. To better understand the developmental heterogeneity among LPIs, and to identify predictors of risk and resilience, this study utilized data from a nationally representative, population-based US sample, and identified developmental trajectories of LPIs from infancy to kindergarten academic achievement. Drawing from prior research, we hypothesized that LPIs who experienced more sensitive early caregiving,16–18 and attended center-based preschool20,21 would manifest more optimal early learning trajectories consistent with academic resilience, and LPIs with a history of psychosocial or biological risk,11–13 would manifest suboptimal trajectories, suggestive of academic risk.
METHODS
Study design and sample
Data were drawn from the Early Childhood Longitudinal Study, Birth Cohort (ECLS-B), a nationally representative, population-based longitudinal study sponsored by the US Department of Education’s National Center for Education Statistics (NCES) in the Institute for Education Science. The ECLS-B is based on a nationally representative probability sample of children born in the United States in 2001 (inclusive), and data were collected from over 10,000 children and their parents at 9 months, with subsequent assessments at 24 months, preschool and kindergarten timepoints. In the United States, age of entry into preschool and kindergarten can vary, but typically ranges from 3 to 5 years of age (preschool) and 5 to 6½ years of age (kindergarten). In the ECLS-B, some children entered kindergarten for the first time in 2006, and others in 2007. For the kindergarten timepoint, we included first-time kindergarten enrollees from the 2006 and 2007 timepoints. Data collection consisted of home visits with parent interviews, and direct assessments of infant mental development at 9 and 24 months, and early academic skills in reading and math at preschool and kindergarten timepoints.26
Our study sample excluded children with congenital abnormalities, and included all children born late preterm (34–36 weeks inclusive) who had developmental outcomes at 9 months, and one additional timepoint (24 months, preschool, or kindergarten). A full-term group (gestational age 37–41 weeks) was also generated for comparison with the late preterm sample. Data were ascertained at birth, 9 months, 24 months, preschool and kindergarten. This study was considered exempt by the Institutional Review Board because it utilized a publicly available dataset with de-identified participants who could not be linked to the data.
Measures
Outcomes
Infant mental development: Mental development at 9 and 24 months was assessed with the Bayley Short Form-Research Edition (BSF-R) Mental Scores. The BSF-R, which was formulated from the Bayley Scales of Infant Development, Second Edition (BSID-II),27 assessed children’s problem-solving and language skills, and was administered at home by trained NCES staff. The BSF-R estimates the number of items a child would have passed correctly on the full BSID-II through the use of item response theory (IRT) modeling, and demonstrates a reliability coefficient of 0.80 compared with the full BSID-II.28 BSF-R scaled scores were used in these analyses.
Preschool and kindergarten reading and math academic skills: Children were assessed at preschool and kindergarten using specialized reading and math assessments developed for the ECLS-B. The reading assessment measured basic reading skills (letter and word recognition, phonological awareness, and understanding words in simple sentences). The IRT reliability coefficient of the early reading assessment was 0.84 at preschool, and 0.92 at kindergarten. The ECLS-B mathematics assessment measured basic math skills (number sense, counting, numerical operations, and pattern recognition). The IRT reliability coefficient for the early mathematics assessment was 0.89 at preschool and 0.92 at kindergarten.29 Scores provide ability estimates in particular domains with scaled scores used in these analyses.
Predictors
Maternal and psychosocial characteristics: Maternal characteristics associated with developmental risk in preterms were chosen a priori after a review of the literature. The following was gathered from the restricted ECLS-B birth certificate data: maternal age, race/ethnicity, marital status (married/unmarried), history of prenatal smoking (yes/no), plurality (singleton; twin/multiple gestation), and ever breastfed (yes/no). We also included measures of maternal education (<high school; ≥high school) and poverty (<185% federal poverty line; ≥185% federal poverty line).
Parent–child interactions: Because more sensitive parenting interactions have been associated with more favorable development in preterm infants,14–18 we included a measure of parental sensitivity at 24 months. Parental sensitivity, characterized as responsive and child-centered parenting behavior, was coded from interactions using the Two-Bags Task, a 10-min semi-structured parent–child activity. Behaviors were coded on a 7-point scale with higher scores indicating more sensitive parenting behaviors.28
Child characteristics and neonatal health risks: We examined biological risks previously associated with development risk in preterms,11–13 as predictors in our multivariate model: birthweight, SGA (birthweight <10%); and 5-min Apgar scores (dichotomized as >7 versus ≤7). We also included gestational age (obtained from birth certificate data, categorized as 34, 35 or 36 weeks), child sex, and center-based preschool attendance (yes/ no) as predictors.
Statistical analyses
Maternal and child characteristics were examined using descriptive statistics. Following ECLS-B Codebook recommendations to use scale scores for longitudinal analyses,28 we standardized (z-scored) BSF-R mental scale scores and reading and math scale scores for all infants at each timepoint. From these standardized scores, we generated developmental trajectories of LPIs (gestational age 34–36 weeks), and compared the mean scores of each LPI trajectory to the mean scores of full-term infants (gestational age 37–41 weeks) at each timepoint. Distinct trajectories of late preterm development from 9 months to kindergarten were identified for reading and math using latent class growth analysis (LCGA). LCGA is a probabilistic analysis that identifies subgroups of individuals who share similar profiles of developmental pathways.30 Models are fit in steps, beginning with an unconditional model, with a subsequent increase in the number of classes until an optimal number of latent classes is determined. Model comparisons were conducted using a set of model fit indices, including the Bayesian Information Criterion (BIC), with less negative scores representing better fitting models.31 In addition to goodness-of-fit indices (i.e., least negative BIC), the optimal models were chosen based on a combination of factors, including posterior probability indices >75%,32 parsimony, theoretical justification, and interpretability (Appendix A).
Trajectories were identified by modeling developmental outcomes as a function of age in months using the PROC TRAJ procedure in SAS.31 The trajectory chosen as the reference group manifested z-scores closest to zero (i.e., mean) across timepoints; trajectories above the reference group indicated academic resilience, and trajectories below the reference group indicated academic risk. We also included the mean standardized scores of infants born full term (GA 37–41 weeks) on our trajectory plots (Fig. 1) to allow for comparison of mean scores between late preterm and full-term groups at each timepoint. PROC GLM in SAS was used to compare the mean standardized developmental scores for each LPI trajectory group in reading and math, with the full-term mean score at each timepoint (9 months, 24 months, preschool- kindergarten), with p < 0.05 indicating significant pairwise differences between mean LPI scores and full-term means at each timepoint (Appendix B).
Fig. 1. Developmental trajectories of late preterm infants from infancy to kindergarten academic achievement.
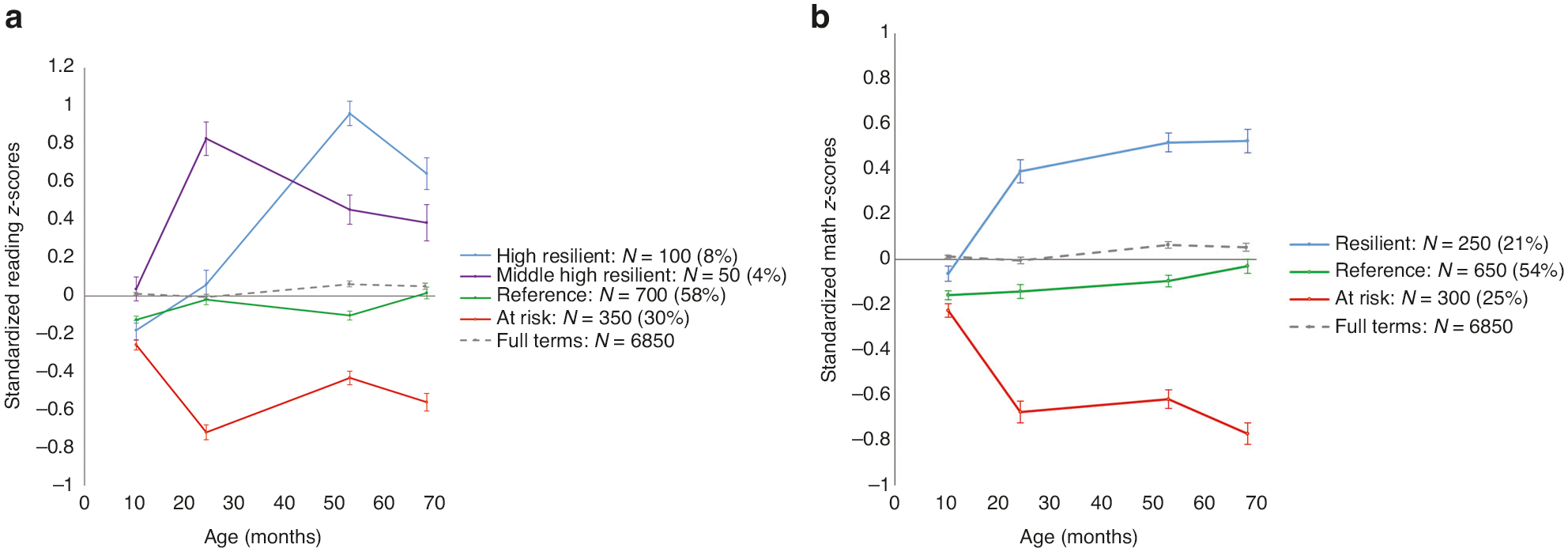
a Late preterm reading trajectories. b Late preterm math trajectories.
Multinomial logistic regression using the SURVEYLOGISTIC procedure in SAS identified maternal, child and psychosocial factors associated with LPI class membership. Mean values and percentages of the predictors within each trajectory group were examined. From the multivariate models, post-hoc pairwise comparisons identified significant group differences associated with predictors among the LPI trajectory groups for reading and math.
We were also interested in identifying predictors of “combined resilience” (academic resilience in 1 or 2 areas) and “combined risk” (academic risk in 1 or 2 areas) by examining patterns of overlap between reading and math trajectory groups. We identified a combined resilience group, characterized by individuals who demonstrated above-average trajectories (>reference) in 1 or both categories (reading or math) and a combined risk group, characterized by individuals who demonstrated below-average trajectories (<reference) in 1 or both categories. Multinomial logistic regression identified predictors associated with membership in the combined resilience or combined risk groups, compared with individuals who were in the combined reference group (reference group for reading and math).
All analyses were conducted using SAS 9.4.33 Because of the complex sample design, sample weights and the Jackknife method were utilized to account for stratification, clustering and unit non-response, thereby allowing the weighted results to generalize to the population of US children born in 2001. According to the NCES requirements for ECLS-B data usage, reported numbers were rounded to the nearest 50.
RESULTS
Sample characteristics
There were 1200 LPIs with developmental assessments at two or more timepoints, including 9 months, who served as the sample for our LCGA. Of these 1200 children, 850 had all covariates and a corresponding weight in our final model. Children included in our final multivariate model (n = 850) did not differ from children excluded due to missing data (n = 350) on most demographic characteristics, however, included children were more likely to be singletons, and had higher kindergarten math scores than excluded children. Maternal and infant sample characteristics of the weighted LPI sample are shown in Table 1, with an additional column indicating the demographic characteristics of the full-term infants included for comparison.
Table 1.
Sample characteristics of late preterm infants, and demographic characteristics of the full-term comparison group.
| Mean (SD) or weighted% (LPI sample: N = 1200) | Mean (SD) or weighted % (FT comparison: N = 6850) | |
|---|---|---|
| Maternal characteristics | ||
| Age (years) | 27.4 (9.2) | 27.4 (3.6) |
| Race/ethnicity | ||
| White/Non-Hispanic | 51.2% | 58.9% |
| Black/Non-Hispanic | 19.7% | 12.8% |
| Hispanic | 22.5% | 22.4% |
| Asian | 3.6% | 3.5% |
| Other | 3.1% | 2.4% |
| Marital status | ||
| Married | 63.0% | 69.0% |
| Unmarried | 37.0% | 31.0% |
| History of prenatal smoking | ||
| No | 87.4% | 89.3% |
| Yes | 12.6% | 10.7% |
| Ever breastfed | ||
| Yes | 61.4% | 70.8% |
| No | 38.6% | 29.2% |
| Plurality | ||
| Singleton | 86.7% | 98.4% |
| Twin or multiple gestation | 13.3% | 1.6% |
| Socioeconomic indicators calculated from measures of education and income at 9 months | ||
| Maternal education | ||
| Less than high school | 22.4% | 18.4% |
| High school degree or greater | 77.6% | 81.6% |
| Income | ||
| <185% federal poverty line | 52.7% | 46.2% |
| ≥185% federal poverty line | 47.3% | 53.7% |
| Child characteristics | ||
| Child sex | ||
| Male | 53.2% | 51.2% |
| Female | 46.8% | 48.8% |
| Birthweight (g) | 2880.1 (831.8) | 3404.2 (358.6) |
| Gestational age (weeks) | 35.3 (0.9) | 39.1 (1.5) |
| 34 | 17.6% | |
| 35 | 30.7% | |
| 36 | 51.8% | |
| % Growth restricted (<10% SGA) | 9.6% | 10.5% |
| Apgar >7 | 92.2% | 98.2% |
| Enrollment in any center-based program at preschool timepoint | ||
| No | 51.3% | 44.0% |
| Yes | 48.7% | 56.0% |
| Mean age at Time 1 (months) | 10.2 (2.6) | 10.3 (4.1) |
| Mean age at Time 2 (months) | 24.2 (1.9) | 24.3 (2.2) |
| Mean age at preschool timepoint (months) | 52.6 (5.5) | 52.5 (5.6) |
| Mean age at kindergarten timepoint (months) | 68.2 (6.7) | 68.1 (7.0) |
Source: US Department of Education, National Center for Education Statistics, Early Childhood Longitudinal Study, Birth Cohort. Selected years 2001–2007.
Developmental trajectories of LPIs from infancy to kindergarten reading and math academic achievement, and comparison with full-term mean scores
Developmental trajectories of LPIs varied across the infancy to kindergarten transition. The LCGA indicated that a 4-class model fit for reading and a 3-class model for math was optimal, as evidenced by less negative BICs, posterior probability indices ≥75%, and parsimonious group size (Appendix A).
Trajectories of LPI reading achievement.
Four trajectories of late preterm reading were labeled: High Resilient: highest developmental scores at kindergarten (n = 100); Middle-high Resilient: next highest developmental scores at kindergarten (n = 50); Reference (z-scores closest to zero) (n = 700); and At-risk: lowest developmental scores at all timepoints (n = 350). At the 9-month timepoint, the mean developmental scores of LPI infants differed from the developmental scores of the full-term group in the High (p < 0.001), Reference (p < 0.001), and At-risk reading trajectories (p < 0.001). At 24 months, the mean developmental scores of LPI infants differed from the developmental scores of the full-term group in Middle-high (p < 0.001), and At-risk trajectories (p < 0.001). At the preschool timepoint, the mean developmental score of LPI infants differed from the developmental scores of the full-term group across all trajectories (p < 0.001). At the kindergarten timepoint, the mean developmental score of LPIs differed from the developmental scores of the full-term group across the High, Middle-high and At-risk trajectories (p < 0.001). Of note, the mean developmental scores of late preterms in the At-risk reading trajectory fell below the mean scores of full-term infants at all timepoints. In contrast, while the mean scores in the reading Reference group diverged at times from the mean full-term scores, at the kindergarten timepoint, the mean scores of the reference group did not differ from the full-term group (p = 0.10). (Fig. 1a and Appendix B).
Trajectories of LPI math achievement.
Regarding trajectories of math academic achievement, the three trajectories of late preterm math were labeled Resilient: (n = 250); Reference (n = 650); and At-risk (n = 300). The mean developmental scores of LPI infants across all trajectories differed from the mean scores of the full-term group at all timepoints (p < 0.001). The mean developmental/academic scores of late preterms in the Resilient math trajectory were higher than those of the full-term group at the 24 months, preschool and kindergarten timepoints, while the developmental/academic scores of late preterms in the At-risk math trajectory were lower than those of the full-term group at all timepoints. In contrast to the late preterm reading trajectory, mean scores in the math Reference group were lower than mean scores for the full-term group at all timepoints (Fig. 1b and Appendix B).
Multivariate predictors associated with reading and math trajectory groups
Reading academic trajectory.
Class membership in trajectory groups for late preterm reading academic achievement varied by maternal, infant and psychosocial characteristics, with significant pairwise comparisons among trajectory groups indicated by superscripts which differ from one another (Table 2a). Late preterms were more likely to be in the High Resilient reading group (compared with the Reference group) if they experienced more sensitive parenting (mean sensitivity scores 5.3 vs. 4.6 (reference)) or if they attended preschool (85.9% vs. 50.2% (reference)). Late preterms were also more likely to be in the Middle-high Resilient reading group (compared with the Reference group) if they experienced more sensitive parenting (mean scores 5.2 vs. 4.6 (reference)). Membership in the High reading trajectory group also varied by select race/ethnicity groups. Compared to the Reference group, there was a higher percentage of Asian race in the High reading trajectory, (16.0% vs. 3.3% (reference)). Predictors associated with membership in the At-risk reading trajectory (compared with the Reference group) included experiencing less sensitive parenting (mean scores 4.1 vs. 4.6 (reference)); being the product of a twin or multiple gestation (15.0% versus 11.7% (reference)); being male (68.1% versus 52.6% (reference)) and maternal education <high school (40% vs. 19.8% (reference)).
Table 2.
a Multivariate predictors and pairwise comparisons: adjusted associations with reading trajectory groups. b Multivariate predictors and pairwise comparisons: adjusted associations with math trajectory groups.
| a | |||||
|---|---|---|---|---|---|
| Predictors (mean, SD, or weighted %) | High N = 100 | Mid-high N = 50 | Reference N = 700 | Low/at risk N = 350 | |
| Education | <HS graduate | 5.5%ab | 7.6%ab | 20.0%a | 39.9%b |
| Race | White | 56.8%ab | 71.4%a | 53.1%a | 31.0%b |
| Black | 20.7%a | 16.4%a | 18.8%a | 25.8%a | |
| Hispanic | – | 9.4 %b | 21.5%b | 38.7%b | |
| Asian | 16.0%a | – | 3.3%b | 2.0%b | |
| Other | – | – | 3.3%a | 2.5%a | |
| Sex (male) | 49.1%ac | 18.6%b | 52.6%a | 68.1%c | |
| Plurality (twin or multiple gestation) | 21.3%ab | 11.9%a | 11.7%a | 15.0%b | |
| SGA (<10%) | 12.3%a | 2.7%a | 8.5%a | 13.3%a | |
| Prenatal smoking (yes) | 3.4%b | – | 13.4%ab | 14.8%a | |
| Attended preschool (yes) | 86.0%a | 71.5%ab | 50.2%b | 39.8%ab | |
| Maternal age (years) | 29.8a | 28.2a | 27.2a | 26.6a | |
| Sensitivity 24 months | 5.3a | 5.2a | 4.6b | 4.1c | |
| b | ||||
|---|---|---|---|---|
| Predictors (mean, SD, or weighted %) | High N = 250 | Reference N = 650 | Low/at risk N = 300 | |
| Education | <HS graduate | 6.4%a | 23.2%a | 41.2%b |
| Race | White | 68.6%a | 48.5%a | 29.3%b |
| Black | 12.0%a | 22.0%a | 25.4%a | |
| Hispanic | 10.2%a | 23.6%a | 38.6%a | |
| Asian | 6.3%a | 3.3%b | 1.5%b | |
| Other | 3.0%ab | 2.5%a | 5.1%b | |
| Sex (male) | 40.9%a | 55.0%ab | 65.1%b | |
| Plurality (twin or multiple gestation) | 11.6%a | 12.4%b | 16.7%c | |
| Small for gestational age (BW <10%) | 6.2%a | 8.8%ab | 15.2%b | |
| Prenatal smoking (yes) | 9.7%ab | 11.6%a | 18.5%b | |
| Attended preschool (yes) | 73.0%a | 47.3%b | 38.5%ab | |
| Mother’s age | 29.3ab | 26.4b | 27.6a | |
| Sensitivity 24 months | 5.1a | 4.5b | 4.1c | |
Source: US Department of Education, National Center for Education Statistics, Early Childhood Longitudinal Study, Birth Cohort. Selected years 2001–2007. The pairwise comparisons for each predictor are adjusted for all the other predictors in the model. Multivariate predictors include: maternal sensitivity, maternal age, maternal education, male sex, preschool attendance, small for gestational age, plurality, prenatal smoking, race/ethnicity.
Panel a: superscript letters a, b and c that differ from one another denote significant differences (p < 0.05) between high, middle-high, reference and at-risk trajectory groups; – indicate values suppressed per IES data sharing requirements. N = unweighted sample sizes for each trajectory group.
Panel b: superscript letters a, b and c that differ from one another denote significant differences (p < 0.05) between high, reference and at-risk trajectory groups. N = unweighted sample sizes for each trajectory group.
Math academic trajectory.
Similar to reading trajectories, class membership in late preterm math trajectory groups also varied by maternal, infant and psychosocial characteristics. Late preterms were more likely to be in the High Resilient math group (compared with the Reference group) if they experienced more sensitive parenting (mean sensitivity scores 5.1 vs. 4.5 (reference)) or if they attended preschool (73.0% vs. 47.3% (reference)). Predictors associated with membership in the At-risk math trajectory (compared with the Reference group) included experiencing less sensitive parenting (mean scores 4.1 vs. 4.5 (reference)); maternal education <high school (41.2% vs. 23.2% (reference)), and biological risks including history of prenatal tobacco exposure (18.5% vs. 11.6% (reference)); and history of twin or multiple gestation (16.7% versus 12.4% (reference)) (Table 2b). Membership in the math trajectory groups also varied by select race/ethnicity groups. Compared to the Reference group, there was a higher percentage of Asian race in the High math trajectory (6.3% vs. 3.3% (reference)); there was a lower percentage of White race/ethnicity in the At-risk math trajectory (29.3% vs. 48.5% (reference)), and there was a higher percentage of “Other” race/ethnicity in the At-risk math trajectory (5.1% vs. 2.5% (reference)).
Multivariate predictors associated with combined resilience and combined risk trajectory groups
In the unweighted sample of 1200, 250 (20.8%) were in the combined resilience group (characterized by above-average trajectories (>reference) in 1 or both categories (reading or math)); 400 (33.3%) were in the combined risk group (characterized by below-average trajectories (<reference) in 1 or both categories (reading or math)); and 550 individuals (45.8%) were in the combined reference group. In adjusted analyses, predictors associated with membership in the combined resilience group included experiencing more sensitive parenting (aOR = 1.62, 95% CI [1.2, 2.3]) and preschool attendance (aOR = 1.97, 95% CI [1.05, 3.7]).
Factors associated with membership in the combined risk group included maternal education <high school (aOR = 2.3, 95% CI [1.1, 4.5]); history of prenatal smoking (aOR = 1.8, 95% CI [1.03, 3.3]); male sex (aOR = 1.8, 95% CI [1.1, 2.8]); and being a product of a twin/multiple gestation (aOR = 2.0, 95% CI [1.2, 3.3]). Experiencing more sensitive parenting was associated with a lower odds of being in the combined risk group (aOR = 0.6, 95% CI [0.5, 0.8]). In multivariate analyses, membership in the combined risk group also varied by select race/ethnicity groups. Hispanic ethnicity was associated with a higher odds of being in the combined risk group (aOR = 1.9, 95% CI [1.01, 3.7]), whereas White race was associated with a lower odds of being in the combined risk group (aOR = 0.5, 95% CI [0.3, 0.9]) (Fig. 2).
Fig. 2. Adjusted odds (aOR) and Multivarite Predictors of Combined Reading and Math Academic Achievement at Kindergarten.
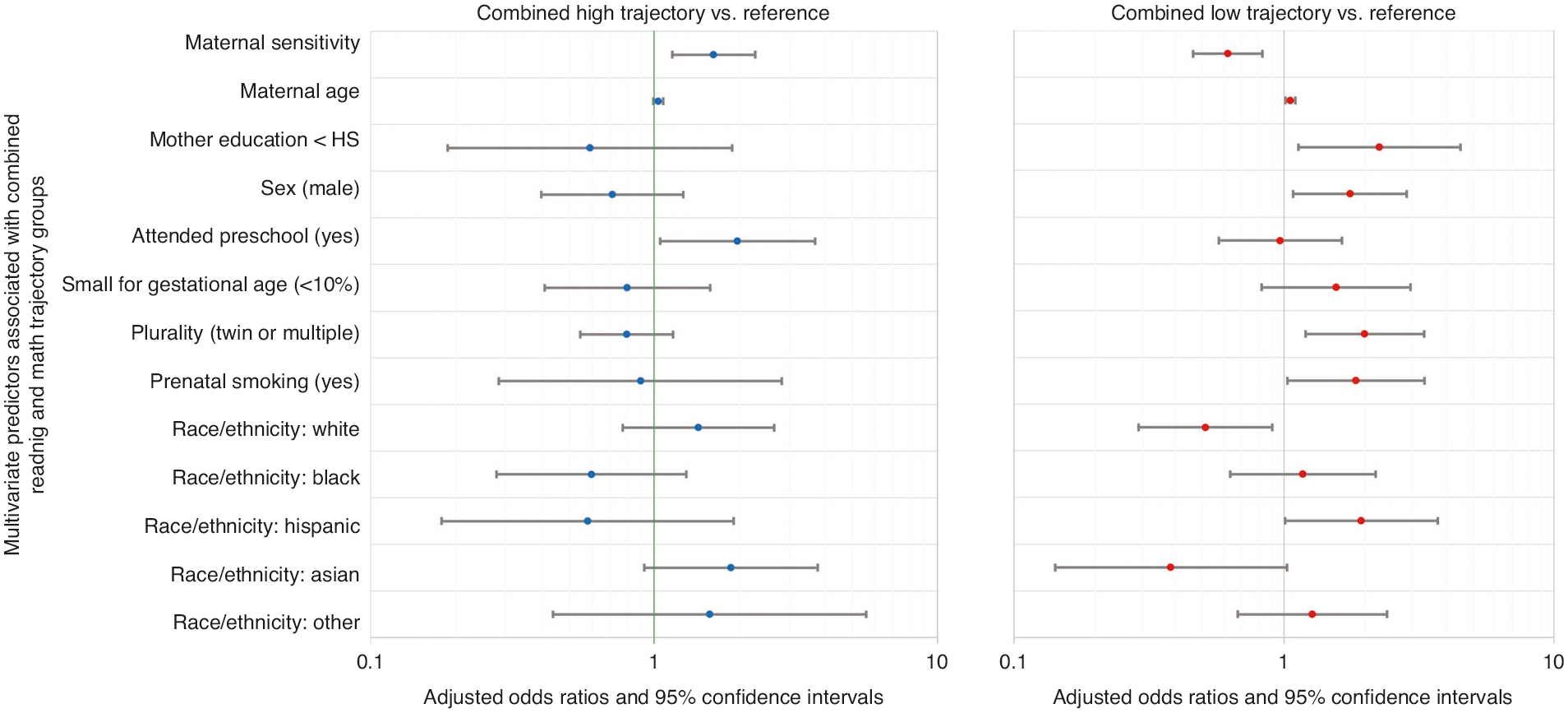
Multivariate Predictors Associated with Combined Academic Resilience (Blue) and Combined Academic Risk (Red).
DISCUSSION
This is the first study to examine trajectories of late preterm development from infancy to kindergarten, and associated predictors of academic resilience and risk. We identified different patterns and predictors for the emergence of reading and math skills, which can help inform pediatric anticipatory guidance given to LPIs. Regarding early reading trajectories, compared with full-term infants, most LPIs (70%) demonstrated early reading skills that were at or above the full-term population mean, with mean LPI scores either equivalent to, or exceeding mean full-term reading scores at the kindergarten timepoint. This is an optimistic view of LPI early reading skills which can be communicated to families. Regarding early math trajectories, a different picture emerges. Across the infancy to kindergarten transition, compared with full-term infants, most LPIs (79%) demonstrated lower mean math scores at all time points, with the greatest gaps in early math skills in the at-risk math trajectory at the kindergarten timepoint. It is not clear why most LPIs manifest early vulnerabilities in math (but not reading). One possible explanation is that the deficits in early numeracy are related to unique characteristics of late preterm brain development including structural changes in the neural pathways related to visuo-constructive skills34,35 or neurodevelopmental immaturity35,36 in neurocognitive domains associated with math processing. Though the mechanisms underlying academic risk in LPIs is an area in need of future research, our findings suggest that as a population, late preterms have vulnerabilities in early math skills, and may merit closer follow-up in the period prior to school entry to identify and remediate deficits in early numeracy.
Regarding predictors of academic resilience in LPIs, more optimal trajectories were associated with well-established promotive factors including experiencing early sensitive caregiving, and preschool attendance. Experiencing more sensitive parenting and preschool attendance were significantly associated with membership in the High-resilience trajectory for both reading and math, and with greater odds of being in the combined-high group, compared with the reference groups. Our findings align with current pediatric recommendations highlighting the importance of responsive relationships and early educational experiences to foster resilience and mitigate biological risk.37
Regarding predictors of academic risk in LPIs, suboptimal academic trajectories were associated with well-described psychosocial, and biological risk factors. Psychosocial risk (e.g., <high school maternal education) was associated with a higher likelihood of being in the at-risk reading and at-risk math trajectories, and a greater odds of being in the combined risk group, compared with the reference groups. Biological risks including a history of a twin or multiple gestation38 was associated with membership in the at-risk reading and at-risk math trajectories, and increased odds of being in the combined-low group. Other biological factors (i.e., history of prenatal tobacco exposure39) predicted academic risk in math and an increased odds of being in the combined-low group. In addition, male sex predicted academic risk in reading and increased odds of being in the combined-low group, compared to the reference group, which is consistent with previous research identifying sex differences, and lower academic achievement in males.40 The mechanism leading to increased academic risk in LPI males is not clear. These differences may be related to functional differences in neural connectivity between males and females which contribute to differences in learning,41 or may be due to sex-related differences in self-regulation, contributing to differences in academic achievement.40 Taken together, these data suggest that LPIs with these aforementioned risk factors (male sex, twin/multiple gestation, prenatal smoking) may merit closer monitoring for the emergence of deficits in early academic skills in the period prior to school entry.
We also observed some racial/ethnic differences regarding predictors of academic risk and resilience. Compared to the reference group, Asian race was associated with a greater likelihood of being in the high-resilient trajectory for reading and math. Compared to the reference group, “Other” race was associated with a greater likelihood of being in the at-risk trajectory for math and Hispanic ethnicity was associated with a higher odds of being in the combined-low group. Although the mechanism of these associations is not clear, and is an area in need of future research, one potential explanation may be related to English language proficiency in families, which may differ across racial/ethnic groups. In previous research, higher English proficiency among Asian families has been associated with higher academic achievement,42 while lower English proficiency in Latino families has been associated with lower academic achievement.43 Taken together, this highlights the need to identify factors associated with racial/ethnic differences in academic achievement in LPIs, in hopes of determining potential intervention targets to mitigate gaps in academic achievement.
In addition to identifying predictors associated with suboptimal academic trajectories, our study also identified potential opportunities to promote resilience (promotive factors) and mitigate risk (protective factors) in LPIs. Because parental sensitivity was associated with higher academic resilience, and lower academic risk in LPIs, evidence-based interventions to promote parental sensitivity in early childhood (e.g., VIP44) may be beneficial, especially for mothers with educational disadvantage.45 Relatedly, there is a growing awareness of the benefits of promoting early relational health (and positive parenting strategies) as a secondary prevention strategy for individuals with a heightened “biological sensitivity to context” to toxic stress.46 Preterm birth can be considered a “biologically sensitive context” in which infant outcomes are differentially susceptible to the effects of the caregiving environment,47 with more positive outcomes associated with more sensitive parenting.48 Taken together, this highlights a potential opportunity foster early academic outcomes of LPIs through targeted secondary prevention strategies focused on early relational health promotion in parents of late preterms. Because LPIs are not routinely followed in specialized neonatal follow-up programs in the US, population-level strategies to promote early relational health in LPIs should focus on opportunities to foster sensitive parenting in the context of primary care, or through expanded eligibility for parenting supports through early intervention.9
While preschool enrollment was also associated with more optimal trajectories, and greater odds of being in the combined-high group, less than half of our late preterm sample was enrolled in preschool at the preschool timepoint. This suggests that anticipatory guidance regarding the benefits of preschool attendance may be especially relevant for LPI parents. Our study also identified biological factors associated with academic risk (e.g., prenatal smoking, multiple gestation, male sex), which may help identify LPIs in need of closer developmental monitoring and early intervention. By individualizing developmental supports to LPIs in the period prior to school entry, we can potentially remediate early academic delays, which can have significant effects at a population level.49 Of note, our study did not include data beyond the kindergarten timepoint. Because neurodevelopmental impairments in late preterms can emerge throughout the lifespan (e.g., ADHD, learning disabilities, and mental health concerns),50–52 LPIs (especially those identified as “at risk”) could benefit from ongoing monitoring in the school-age years.
Our study had several strengths and limitations. Strengths include a large, nationally representative sample, whose results are generalizable to the population, and longitudinal observational assessments of parenting and child development, thus minimizing biases that can be associated with parent-report measures. Our study also had some limitations. The ECLS-B contained limited information on pregnancy history and neonatal risks including the maternal medical conditions which led to the preterm delivery, which may be an important predictor for late preterm outcomes. Relatedly, although the ECLS-B had data on plurality (i.e., singleton vs. twin/multiple gestation), data were not available regarding whether the gestation was mono-chorionic versus di-chorionic, which is another predictor of preterm outcomes.53 In addition, no data on maternal intelligence or history of learning difficulties were available, which are additional potential confounders. Despite these limitations, data from our study can help inform pediatric providers about the early academic outcomes of LPIs, and provide guidance regarding which LPIs may benefit from closer developmental monitoring prior to school entry.
CONCLUSION
Our study identified distinct profiles of academic resilience and academic risk in late preterms from infancy to kindergarten. Our findings affirm that pediatric anticipatory guidance provided in pediatric care to foster school readiness in all children (e.g., encouraging sensitive parenting and preschool enrollment)54,55 is also promotive of academic resilience in children born late preterm. Considering the beneficial role of early relational health as a secondary prevention strategy for infants at risk,46 expanding opportunities to foster early relational health in LPI infants should be considered to help promote academic resilience and mitigate the academic risks associated with late preterm birth. In addition, our findings suggest that late preterms with select risks (e.g., history of prenatal smoking, and history of multiple gestation, male sex, maternal education <high school) are at risk for deficits in early academic achievement by kindergarten. LPIs with these risk factors, might benefit from closer developmental surveillance and targeted interventions prior to school entry (and beyond) to mitigate academic risk and optimize later outcomes.
Supplementary Material
IMPACT:
Late preterm infants (LPIs) have developmental risks compared to full terms. LPI trajectories of early reading and math varied from infancy to kindergarten. We identified predictors of academic resilience and risk, which can help inform anticipatory guidance provided to LPIs prior to kindergarten.
Promotive factors (sensitive parenting and preschool enrollment) predicted academic resilience. Select maternal and neonatal characteristics (<high school education, male sex, prenatal smoking, and multiple gestation) predicted academic risk at kindergarten.
LPIs account for the majority of preterm infants. Encouraging preschool enrollment and fostering sensitive parenting may promote early academic achievement in LPIs, which has population-level impacts.
FUNDING
University of Michigan, NICHD (K08HD078506).
Footnotes
COMPETING INTERESTS
The authors declare no competing interests.
CONSENT TO PARTICIPATE
None required. This study utilized a publicly available dataset with de-identified participants who could not be linked to the data.
Supplementary information The online version contains supplementary material available at https://doi.org/10.1038/s41390-023-02756-2.
DATA AVAILABILITY
Data for this study were obtained from the Early Childhood Longitudinal Study-Birth Cohort, restricted-use dataset. Data can be accessed after entering into a data use agreement with the Institute of Educational Statistics, National Center for Educational Statistics.
REFERENCES
- 1.Davidoff M et al. Changes in the gestational age distribution among US singleton births: Impact on rates of late preterm birth, 1992 to 2002. Semin. Perinatol 30, 8–15 (2006). [DOI] [PubMed] [Google Scholar]
- 2.Raju TNK, Higgins RD, Stark AR & Leveno KJ Optimizing care and outcome for late-preterm (near-term) infants: a summary of the workshop sponsored by the National Institute of Child Health and Human Development. Pediatrics 118, 1207–1214 (2006). [DOI] [PubMed] [Google Scholar]
- 3.Shah P, Kaciroti N, Richards B, Oh W & Lumeng JC Developmental outcomes of late preterm infants from infancy to kindergarten. Pediatrics 138, e20153496. 10.1542/peds.2015-3496 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Williams BL et al. Perinatal origins of first-grade academic failure: role of prematurity and maternal factors. Pediatrics 131, 693 (2013). [DOI] [PubMed] [Google Scholar]
- 5.Chan E & Quigley MA School performance at age 7 years in late preterm and early term birth: a cohort study. Arch. Dis. Child. Fetal Neonatal Ed 99, F451–F457 (2014). [DOI] [PubMed] [Google Scholar]
- 6.Shah PE, Kaciroti N, Richards B & Lumeng JC Gestational age and kindergarten school readiness in a national sample of preterm infants. J. Pediatr 178, 61–67 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Garfield CF et al. Educational performance of children born prematurely. JAMA Pediatr 171, 764–770 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dollar JM, Perry NB, Calkins SD, Keane SP & Shanahan L Temperamental anger and positive reactivity and the development of social skills: implications for academic competence during preadolescence. Early Educ. Dev 29, 747–761 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kalia JL, Visintainer P, Brumberg HL, Pici M & Kase J Comparison of enrollment in interventional therapies between late-preterm and very preterm infants at 12 months’ corrected age. Pediatrics 123, 804–809 (2009). [DOI] [PubMed] [Google Scholar]
- 10.Woodward LJ, Clark CA, Bora S & Inder TE Neonatal white matter abnormalities an important predictor of neurocognitive outcome for very preterm children. PLoS One 7, e51879 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mangin KS, Horwood LJ & Woodward LJ Cognitive development trajectories of very preterm and typically developing children. Child Dev 88, 282–298 (2017). [DOI] [PubMed] [Google Scholar]
- 12.Erdei C, Austin NC, Cherkerzian S, Morris AR & Woodward LJ Predicting school-aged cognitive impairment in children born very preterm. Pediatrics 145, e20191982. 10.1542/peds.2019-1982 (2020). [DOI] [PubMed] [Google Scholar]
- 13.Linsell L, Malouf R, Morris J, Kurinczuk JJ & Marlow N Prognostic factors for poor cognitive development in children born very preterm or with very low birth weight: a systematic review. JAMA Pediatr 169, 1162–1172 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Poehlmann-Tynan J et al. Risk and resilience in preterm children at age 6. Dev. Psychopathol 27, 843–858 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Faure N et al. Maternal sensitivity: a resilience factor against internalizing symptoms in early adolescents born very preterm? J. Abnorm. Child Psychol 45, 671–680 (2017). [DOI] [PubMed] [Google Scholar]
- 16.Wolke D, Jaekel J, Hall J & Baumann N Effects of sensitive parenting on the academic resilience of very preterm and very low birth weight adolescents. J. Adolesc. Health 53, 642–647 (2013). [DOI] [PubMed] [Google Scholar]
- 17.Treyvaud K et al. Parenting behavior at 2 years predicts school-age performance at 7 years in very preterm children. J. Child Psychol. Psychiatry 57, 814–821 (2016). [DOI] [PubMed] [Google Scholar]
- 18.Nguyen TN et al. Language skills in children born preterm (<30 wks’ gestation) throughout childhood: associations with biological and socioenvironmental factors. J. Dev. Behav. Pediatr 40, 735–742 (2019). [DOI] [PubMed] [Google Scholar]
- 19.ElHassan NO et al. The impact of prematurity and maternal socioeconomic status and education level on achievement-test scores up to 8th grade. PLoS One 13, e0198083 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chen JH, Claessens A & Msall ME Prematurity and school readiness in a nationally representative sample of Australian children: does typically occurring preschool moderate the relationship. Early Hum. Dev 90, 73–79 (2014). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Reid LD & Strobino DM A population-based study of school readiness determinants in a large urban public school district. Matern Child Health J 23, 325–334 (2019). [DOI] [PubMed] [Google Scholar]
- 22.Girsen AI, Do SC, El-Sayed YY, Hintz SR & Blumenfeld YJ Association between small-for-gestational age and neurocognitive impairment at two years of corrected age among infants born at preterm gestational ages: a cohort study. J. Perinatol 37, 958–962 (2017). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Potijk MR, Kerstjens JM, Bos AF, Reijneveld SA & de Winter AF Developmental delay in moderately preterm-born children with low socioeconomic status: risks multiply. J. Pediatr 163, 1289–1295 (2013). [DOI] [PubMed] [Google Scholar]
- 24.Brown HK, Speechley KN, Macnab J, Natale R & Campbell MK Mild prematurity, proximal social processes, and development. Pediatrics 134, e814–e824 (2014). [DOI] [PubMed] [Google Scholar]
- 25.Johnson S et al. Differentiating the preterm phenotype: distinct profiles of cognitive and behavioral development following late and moderately preterm birth. J. Pediatr 193, 85–92.e81 (2018). [DOI] [PubMed] [Google Scholar]
- 26.Nord C, Edwards B, Andreassen C, Green JL, Wallner-Allen K Early Childhood Longitudinal Study, Birth Cohort (ECLS-B), User’s Manual for the ECLS-B Longitudinal 9-Month: 2-Year Data File and Electronic Codebook (NCES 2006–046) (US Department of Education, National Center for Education Statistics, 2006). [Google Scholar]
- 27.Bayley N Bayley Scales of Infant and Toddler Development 2nd edn (Harcourt Assessment, 1993). [Google Scholar]
- 28.Snow K, et al. Early Childhood Longitudinal Study, Birth Cohort (ECLS-B) 9-Month—Preschool Restricted-Use Data File and Electronic Codebook In: U.S. Department of Education NCES, ed. Washington, DC: U.S. Department of Education; 2007. [Google Scholar]
- 29.Snow K et al. Early Childhood Longitudinal Study, Birth Cohort (ECLS-B) Kindergarten 2006 and 2007 Data File User’s Manual (2010–010) In: Statistics NCES, editor. Washington, D.C.: Institute of Educational Sciences, U.S. Department of Education; 2009. [Google Scholar]
- 30.Magidson J & Vermunt JK in The Sage Handbook of Quantitative Methodology for the Social Sciences 175–198; Sage Publications, (2004). [Google Scholar]
- 31.Jones BL, Nagin DS & Roeder K A SAS procedure based on mixture models for estimating developmental trajectories. Sociol. Methods Res 29, 374–393 (2001). [Google Scholar]
- 32.Nagin DS & Nagin D Group-Based Modeling of Sevelopment (Harvard University Press, 2005). [Google Scholar]
- 33.Base SAS(R) 9.4 Procedures Guide: Statistical Procedures (Cary, NC: 2014). [Google Scholar]
- 34.Munoz-Moreno E et al. Structural brain network reorganization and social cognition related to adverse perinatal condition from infancy to early adolescence. Front. Neurosci 10, 560 (2016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Oros D et al. Pathways of neuronal and cognitive development in children born small-for-gestational age or late preterm. Ultrasound Obstet. Gynecol 43, 41–47 (2014). [DOI] [PubMed] [Google Scholar]
- 36.Walsh JM, Doyle LW, Anderson PJ, Lee KJ & Cheong JLY Moderate and late preterm birth: effect on brain size and maturation at term-equivalent age. Radiology 273, 232–240. 10.1148/radiol.14132410 (2014). [DOI] [PubMed] [Google Scholar]
- 37.Shonkoff JP, Boyce WT, Levitt P, Martinez FD & McEwen B Leveraging the biology of adversity and resilience to transform pediatric practice. Pediatrics 147, e20193845 (2021). [DOI] [PubMed] [Google Scholar]
- 38.Bodeau-Livinec F et al. Do very preterm twins and singletons differ in their neurodevelopment at 5 years of age? Arch. Dis. Child. Fetal Neonatal Ed 98, F480–F487 (2013). [DOI] [PubMed] [Google Scholar]
- 39.Kristjansson AL et al. Maternal smoking during pregnancy and academic achievement of offspring over time: a registry data-based cohort study. Prev. Med 113, 74–79 (2018). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Weis M, Heikamp T & Trommsdorff G Gender differences in school achievement: the role of self-regulation. Front. Psychol 4, 442 (2013). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Spets DS, Jeye BM & Slotnick SD Different patterns of cortical activity in females and males during spatial long-term memory. Neuroimage 199, 626–634 (2019). [DOI] [PubMed] [Google Scholar]
- 42.Liu LL, Benner AD, Lau AS & Kim SY Mother-adolescent language proficiency and adolescent academic and emotional adjustment among Chinese American families. J. Youth Adolesc 38, 572–586 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Han WJ Bilingualism and academic achievement. Child Dev 83, 300–321 (2012). [DOI] [PubMed] [Google Scholar]
- 44.Juffer F, Struis E, Werner C & Bakermans-Kranenburg MJ Effective preventive interventions to support parents of young children: illustrations from the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD). J. Prev. Interv. Community 45, 202–214 (2017). [DOI] [PubMed] [Google Scholar]
- 45.Mendelsohn AL et al. Use of videotaped interactions during pediatric well-child care: impact at 33 months on parenting and on child development. J. Dev. Behav. Pediatr 28, 206 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Garner A & Yogman M Preventing childhood toxic stress: partnering with families and communities to promote relational health. Pediatrics 148, e2021052582. 10.1542/peds.2021-052582 (2021). [DOI] [PubMed] [Google Scholar]
- 47.Gueron-Sela N, Atzaba-Poria N, Meiri G & Marks K The caregiving environment and developmental outcomes of preterm infants: diathesis stress or differential susceptibility effects. Child Dev 86, 1014–1030 (2015). [DOI] [PubMed] [Google Scholar]
- 48.Poehlmann J et al. Preterm infants who are prone to distress: differential effects of parenting on 36-month behavioral and cognitive outcomes. J. Child Psychol. Psychiatry 53, 1018–1025 (2012). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Jaekel J & Wolke D Preterm birth and dyscalculia. J. Pediatr 164, 1327–1332 (2014). [DOI] [PubMed] [Google Scholar]
- 50.Labayru G et al. Small for gestational age moderate to late preterm children: a neuropsychological follow-up. Dev. Neuropsychol 46, 277–287 (2021). [DOI] [PubMed] [Google Scholar]
- 51.Suikkanen J et al. Reaction times, learning, and executive functioning in adults born preterm. Pediatr. Res 89, 198–204 (2021). [DOI] [PubMed] [Google Scholar]
- 52.Martínez-Nadal S & Bosch L Cognitive and learning outcomes in late preterm infants at school age: a systematic review. Int. J. Environ. Res. Public Health 18, 74 (2021). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hack KE et al. Long-term neurodevelopmental outcome of monochorionic and matched dichorionic twins. PLoS One 4, e6815 (2009). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Williams PG & Lerner MA School readiness. Pediatrics 144, e20191766 (2019). [DOI] [PubMed] [Google Scholar]
- 55.Council on Early Childhood. The pediatrician’s role in optimizing school readiness. Pediatrics 138, e20162293. 10.1542/peds.2016-2293 (2016). [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data for this study were obtained from the Early Childhood Longitudinal Study-Birth Cohort, restricted-use dataset. Data can be accessed after entering into a data use agreement with the Institute of Educational Statistics, National Center for Educational Statistics.