

Abstract
We present a case of cardioembolic stroke in a patient with a history of mechanical aortic valve who was compliant with anticoagulation medication. Cardiac computed tomography was used as an alternative, noninvasive means of evaluation for the cardioembolic source of stroke and identified subvalvular mobile pannus of the mechanical aortic valve.
Key Words: cardiac computed tomography, cardioembolic stroke, mechanical valve
Graphical Abstract
History of Presentation
A 60-year-old man with a history of ischemic stroke 4 weeks before presentation, atrial flutter, and a modified Bentall procedure with a St Jude mechanical aortic valve replacement, on warfarin and aspirin, presented with a chief complaint of acute-onset left-sided numbness as well as dysarthria. Vital signs on presentation were within normal limits, and an electrocardiogram showed a normal sinus rhythm. The physical examination was notable for expressive aphasia, left upper and lower extremity sensory deficits, and mild dysdiadochokinesia. An initial laboratory investigation was notable for an international normalized ratio (INR) of 2.4, below the patient’s INR goal of 2.5 to 3.5. Computed tomography (CT) and CT angiogram of the head showed no acute intracranial abnormality. Subsequent magnetic resonance imaging of the brain revealed acute infarcts in multiple vascular territories concerning for a cardioembolic source of the stroke (Figure 1).
Learning Objectives
-
•
To understand the role of cardiac computed tomography as an alternative, noninvasive imaging modality in the evaluation of cardioembolic sources of stroke.
-
•
To recognize the advantages of cardiac computed tomography in the evaluation of cardioembolic sources of stroke in patients with mechanical valves as compared with echocardiography.
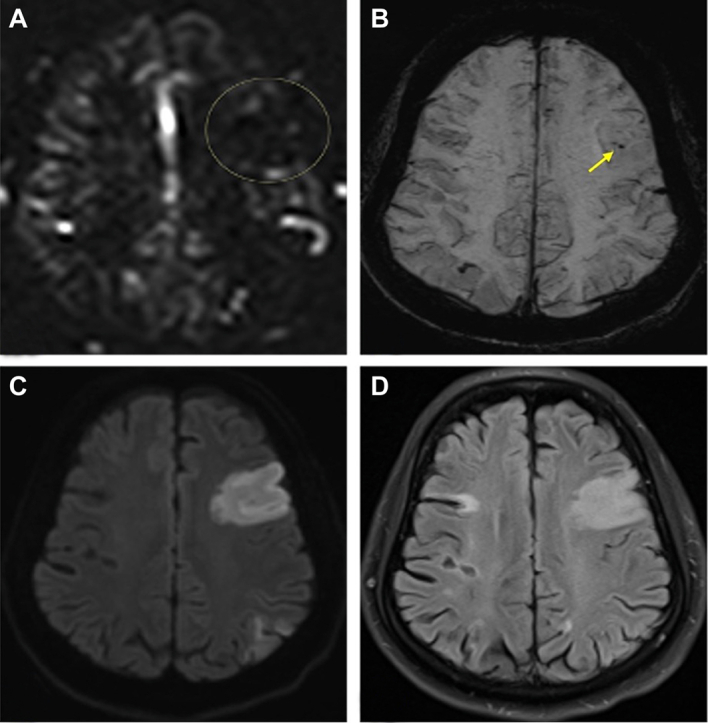
Figure 1.

Noncontrast Magnetic Resonance Imaging of the Head Showing Evidence of Acute Infarcts in Multiple Vascular Territories Concerning for Cardioembolic Etiology of Stroke
(A) Perfusion: an asymmetrically decreased area of cortical perfusion in the left frontal lobe (circle) that correlates with diffusion weighted imaging. (B) Susceptibility weighted image: within the frontal lobe infarct territory are areas of susceptibility blooming (arrow), suggesting the presence of thrombus or slow flow in the distal middle cerebral artery. (C) Diffusion weighted image: large area of diffusion restriction in the left frontal lobe and smaller patchy area seen in the parietal lobe indicating acute multifocal infarct. (D) Fluid-attenuated inversion recovery (FLAIR): Hyperintense signal in the left frontal lobes, correlating with the diffusion weighted images. The left parietal territory is not evident on this image.
Past Medical History
The patient’s medical history was significant for severe aortic stenosis status after undergoing a modified Bentall procedure with placement of a St Jude Medical bileaflet mechanical aortic valve 18 years before. The patient was placed on warfarin for anticoagulation with an INR goal of 2.5 to 3.5. A review of the outpatient anticoagulation clinic records revealed that before the current presentation, the patient had remained on consistent dosing of warfarin with INRs in the desired range. Aspirin had been recently added for dual-antiplatelet equivalent therapy in the setting of the patient’s recent ischemic stroke. Other history included paroxysmal atrial flutter, controlled hypertension, nonobstructive coronary artery disease, insulin-dependent type 2 diabetes mellitus, and hyperlipidemia.
Differential Diagnosis
The differential diagnosis for cardioembolic stroke includes peripheral thrombus with intracardiac (right-to-left) shunt, intracardiac tumor, left atrial thrombus, left ventricular thrombus, perivalvular thrombus, infective endocarditis, seronegative endocarditis, papillary fibroelastoma, mechanical valve pannus formation, and aortic atheroma or thrombus.
Investigations
A transthoracic echocardiography (TTE) demonstrated normal mechanical aortic valve function (peak velocity of 2.78 m/s, Doppler velocity index of 0.45, and indexed prosthetic valve area of 1.04 cm2/m2) with no evidence of pathologic obstruction, normal contrasted images, and an early positive agitated saline study suggestive of an atrial-level shunt (Figure 2, Video 1). An evaluation for left atrial– and mechanical valve–associated sources of stroke was severely limited by a shadowing artifact from the mechanical valve. Cardiac CT (CCT) was selected as a noninvasive alternative to transesophageal echocardiography (TEE) to assess the aortic valve prosthesis and atrial-level shunt and to rule out intracardiac thrombus. CCT images revealed a small patent foramen ovale without a septal aneurysm and a well-seated bileaflet mechanical aortic valve with a subvalvular mass prolapsing between the leaflets with elevated Hounsfield units ranging between 179 and 220, which was consistent with a highly mobile pannus (Figure 3, Video 2). The left atrial appendage, left atrium, mitral valve, and left ventricle were all assessed by CCT without evidence of thrombus, vegetation, or other significant pathology.
Figure 2.

Key Measurements of the Prosthetic Valve Function Obtained Using Transthoracic Echocardiography
(Top) Velocity time integral (VTI) measurements obtained using transthoracic echocardiography with continuous-wave Doppler of both the left ventricular outflow tract and prosthetic aortic valve used to calculate the indexed prosthetic valve area. (Bottom) VTI measurements of the left ventricular outflow tract and prosthetic aortic valve obtained using continuous-wave Doppler with transthoracic echocardiography used to calculate the dimensionless index.
Figure 3.

Cardiac Computed Tomography Multiplanar Reconstruction of the Subvalvular Pannus
Multiple cardiac computed tomography images showing evidence of subvalvular pannus (crosshairs). Hounsfield units of the measured pannus (arrows) seen in bottom left of image. Please refer to the videos for further images and videos of the pannus. AO = aorta; CW = continuous-wave Doppler; EOA = effective orifice area; LA = left atrium; LVOT = left ventricular outflow tract; PW = pulsed-wave Doppler.
Management
The patient was referred to a local valve center of excellence for consideration of surgical management of the identified subvalvular pannus. Because pannus may serve as a nidus for thrombus formation, the therapeutic anticoagulation target INR was increased from 2.5 to 3.5 to 3.0 to 3.5 along with continued antiplatelet therapy with aspirin with a plan for interval imaging to re-evaluate the pannus.
Discussion
Echocardiography, both TTE and TEE, is generally considered the criterion standard and preferred imaging modality in the evaluation of cardioembolic etiology of stroke.1,2 The initial TTE in this case revealed a small atrial-level shunt and no evidence of prosthetic valve dysfunction. Despite evidence of an atrial shunt and no evidence on TTE of valvular dysfunction, a high suspicion of a potential valvular pathology remained, such as adherent thrombus of pannus as the causative etiology of the patient’s stroke. The 2020 American College of Cardiology/American Heart Association guidelines for the management of valvular heart disease recommend (Class 1, Level of Evidence: C-LD) that in patients with clinical symptoms concerning for potential valvular dysfunction, further imaging with either TEE, gated CCT, or fluoroscopy is performed even in the absence of TTE findings.3 Because of the relatively high levels of acoustic impedance in hard substances such as stainless steel and molybdenum alloys found in mechanical valves, echocardiographic imaging modalities are subject to severe limitations when evaluating mechanical prosthetic valves because of acoustic shadowing, and TEE is often less effective in the evaluation of the anterior aspect of the aortic valve.4
CCT has been shown to perform well in the evaluation of both mechanical valves and of cardioembolic source of stroke, providing similar sensitivity, specificity, and negative predictive value to echocardiography.5, 6, 7, 8 In addition to the 2020 American College of Cardiology/American Heart Association guidelines, the 2024 guidelines for the evaluation of prosthetic valve function with imaging from the American Society of Echocardiography also recognizes the role of CT in the evaluation of prosthetic valves, citing the ability of CT to evaluate valve morphology, structural abnormalities, stenotic orifices, regurgitant orifices, sewing ring complications, and perivalvular complications.9 Additionally, a meta-analysis comparing the evaluation of prosthetic valve endocarditis between CCT and TEE showed both imaging modalities had good diagnostic accuracy; however, CCT was more specific than TEE and had improved periannular diagnostics, further supporting the use of CCT in the evaluation of mechanical valve complications.10 Given the superiority of CCT in these domains and the noninvasive nature of the test, CCT was chosen as the alternative imaging modality to assess for prosthetic valve dysfunction in this patient.
Mechanical aortic valve pannus formation is a rare but potentially deleterious complication of mechanical aortic valve replacement.11 The cumulative incidence of pannus formation increases with the age of the mechanical valve, rising from 0.5% in the first 10 years to 9.9% at 25 years.11 The exact cause of pannus formation has not yet been elucidated. However, it is believed to be a result of chronic inflammatory changes resulting from valve implantation and is histologically distinct from thrombus.12 This distinction can been observed on CT, with pannus demonstrating high attenuation exceeding 145 HU, whereas both acute and chronic thrombus have lower attenuation.12,13 The ability to better characterize mechanical valve pathology makes CCT an ideal imaging modality for the evaluation of mechanical valve pannus or thrombus and represents a diagnostic advantage when compared with traditional echocardiographic imaging.
Follow-Up
The patient was discharged from the hospital with plans to follow-up with the local valve center of excellence at an outside hospital for consideration of surgical management of subvalvular pannus. After diagnosis, the therapeutic INR goal was increased to 3.0 along with continued antiplatelet therapy and a plan for repeat imaging until definitive management with surgery was obtained. Unfortunately, the patient was lost to follow-up and died from unknown circumstances at an outside facility months afterward.
Conclusions
In this case, CCT identified a subvalvular mobile pannus as the cardioembolic source of acute ischemic stroke, hidden by shadowing artifacts from the mechanical aortic valve on TTE. CCT is a useful noninvasive adjunctive imaging modality in the evaluation of cardioembolic source of stroke, particularly for those with mechanical aortic valves in whom echocardiography has limited sensitivity to detect prosthetic abnormalities such as thrombus or pannus.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
Appendix
For supplemental videos, please see the online version of this paper.
Appendix
TTE cines of aortic valve, key measurements, and bubble study.
Cardiac CT angiogram cines of mobile pannus, left atrial appendage, and left ventricle.
References
- 1.de Bruijn S.F.T.M., Agema W.R.P., Lammers G.J., et al. Transesophageal echocardiography is superior to transthoracic echocardiography in management of patients of any age with transient ischemic attack or stroke. Stroke. 2006;37(10):2531–2534. doi: 10.1161/01.STR.0000241064.46659.69. [DOI] [PubMed] [Google Scholar]
- 2.Easton J.D., Saver J.L., Albers G.W., et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. Stroke. 2009;40(6):2276–2293. doi: 10.1161/STROKEAHA.108.192218. [DOI] [PubMed] [Google Scholar]
- 3.Otto C.M., Nishimura R.A., Bonow R.O., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J Am Coll Cardiol. 2021;77(4):e25–e197. doi: 10.1016/j.jacc.2020.11.018. [DOI] [PubMed] [Google Scholar]
- 4.Bouzas-Mosquera A., Álvarez-García N. Orientation of bileaflet mechanical aortic valve prostheses for optimal evaluation by transthoracic echocardiography. J Thorac Cardiovasc Surg. 2015;150(2):428–430. doi: 10.1016/j.jtcvs.2015.03.028. [DOI] [PubMed] [Google Scholar]
- 5.Apfaltrer G., Lavra F., De Cecco C.N., et al. Predictive value of cardiac CTA, cardiac MRI, and transthoracic echocardiography for cardioembolic stroke recurrence. AJR Am J Roentgenol. 2021;217(2):336–346. doi: 10.2214/AJR.20.23903. [DOI] [PubMed] [Google Scholar]
- 6.Austein F., Eden M., Engel J., et al. Practicability and diagnostic yield of one-stop stroke CT with delayed-phase cardiac CT in detecting major cardioembolic sources of acute ischemic stroke : a proof of concept study. Clin Neuroradiol. 2021;31(4):911–920. doi: 10.1007/s00062-021-01003-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Suh Y.J., Lee S., Im D.J., et al. Added value of cardiac computed tomography for evaluation of mechanical aortic valve: emphasis on evaluation of pannus with surgical findings as standard reference. Int J Cardiol. 2016;214:454–460. doi: 10.1016/j.ijcard.2016.04.011. [DOI] [PubMed] [Google Scholar]
- 8.Sandhu G.S., Velangi P.S., Kharoud H., et al. Prognostic impact of identifying etiology of prosthetic valve dysfunction with CT. J Cardiovasc Comput Tomogr. 2022;16(2):174–181. doi: 10.1016/j.jcct.2021.10.008. [DOI] [PubMed] [Google Scholar]
- 9.Zoghbi W.A., Jone P.-N., Chamsi-Pasha M.A., et al. Guidelines for the evaluation of prosthetic valve function with cardiovascular imaging: A report from the American Society of Echocardiography developed in collaboration with the Society for Cardiovascular Magnetic Resonance and the Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2024;37(1):2–63. doi: 10.1016/j.echo.2023.10.004. [DOI] [PubMed] [Google Scholar]
- 10.Jain V., Wang T.K.M., Bansal A., et al. Diagnostic performance of cardiac computed tomography versus transesophageal echocardiography in infective endocarditis: a contemporary comparative meta-analysis. J Cardiovasc Comput Tomogr. 2021;15(4):313–321. doi: 10.1016/j.jcct.2020.11.008. [DOI] [PubMed] [Google Scholar]
- 11.Choi J.W., Hwang H.Y., Lee Y., et al. Incidence and risk factors of pannus after mechanical aortic valve replacement. Thorac Cardiovasc Surg. 2022;70(3):182–188. doi: 10.1055/s-0041-1727152. [DOI] [PubMed] [Google Scholar]
- 12.Aladmawi M.A., Pragliola C., Vriz O., Galzerano D. Use of multidetector-row computed tomography scan to detect pannus formation in prosthetic mechanical aortic valves. J Thorac Dis. 2017;9(Suppl 4):S343–S348. doi: 10.21037/jtd.2017.04.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gündüz S., Özkan M., Kalçik M., et al. Sixty-four-section cardiac computed tomography in mechanical prosthetic heart valve dysfunction: thrombus or pannus. Circ Cardiovasc Imaging. 2015;8(12):1–11. doi: 10.1161/CIRCIMAGING.115.003246. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
TTE cines of aortic valve, key measurements, and bubble study.
Cardiac CT angiogram cines of mobile pannus, left atrial appendage, and left ventricle.