

Abstract
BACKGROUND
This study implemented the Copenhagen Adductor Exercise (CAE) and Nordic Hamstring Exercise (NHE) to examine 1) whether CAE and NHE interventions are associated with adductor and hamstring strength gains in youth African male soccer players and 2) whether strength changes after a rest period and secondary intervention.
STUDY DESIGN
Pre-post intervention study.
METHODS
Forty-four African elite male academy players (age 14.7±1.5 [12-18] years) participated in twice weekly CAE and NHE interventions for 8- and 10-week periods separated by a 4-week rest. Long lever adductor squeeze strength and prone isometric hamstring strength were measured with mixed-effects linear regression models to observe strength changes over time.
RESULTS
Ninety-six and 95% of CAE and NHE sessions were completed in each intervention, with no adverse events related to the execution of the exercises. Adductor squeeze strength increased during the first intervention (baseline 3.23 [2.99-3.47] N/kg, post-intervention 3.53 [3.30-3.76] N/kg, p=0.911) and was maintained following the rest period (3.52 [3.27-3.76] N/kg, p=0.999) and second intervention (3.60 [3.35-3.84] N/kg, p=0.002). Hamstring strength improved during the first intervention (baseline 4.95 [4.42-5.49] N/kg, post-intervention 5.48 [4.95-6.02] N/kg, p<0.001), decreased to baseline during the rest period (4.98 [4.44-5.53] N/kg, p=0.996), and did not improve during the second intervention (5.01 [4.46-5.55] N/kg, p=0.978).
CONCLUSION
CAE and NHE interventions can be implemented at an elite African academy with high compliance. Adductor and hamstring strength improved in the first intervention, with no further improvements in the second intervention. Secondary interventions therefore should include higher exercise volume or load to improve longitudinal adductor and hamstring strength.
Level of Evidence
Level III (Cohort Study)
Keywords: Copenhagen Adductor, Nordic Hamstring, Football, Strength, Soccer
INTRODUCTION
In African soccer (football) players, general injury risk reduction strategies have been successful with interventions such as the FIFA 11+.1,2 Although general injury risk was reduced by 41% and 55-71% in these studies, a significant reduction to injuries in the thigh1 and thigh/groin2 were not observed. Despite lacking injury prevalence studies in African players, it is known from other regions that groin and hamstring injuries are common in soccer players.3,4
To target the groin and hamstrings more specifically, injury risk reduction strategies have been recommended in soccer players outside West Africa. The Copenhagen Adductor Exercise (CAE) and Nordic Hamstring Exercise (NHE) have been studied, with randomized controlled trials in European soccer players showing a significant reduction in groin and hamstring injuries, respectively.5,6 Adding the CAE to the FIFA 11+ improves adductor strength,7 and has also been promoted as an addition to the FIFA 11+ by Football Australia’s Perform+ initiative.8 One study in Japanese soccer players even suggests combining the CAE and NHE is more effective at reducing adductor injuries than implementing the CAE alone.9 The only African NHE intervention study shows a 70% reduction in hamstring injuries compared to the previous season in Egyptian players, showing promise for other interventions on the continent.10
Injury risk reduction using the CAE and NHE may be attributed to increases in adductor and hamstring strength, respectively.5,6 Following CAE intervention, under-19 soccer players improved eccentric hip adduction strength by 36%.11 In the adductors, every unit (Nm/kg) of increased long lever adductor squeeze strength reduced injury risk by 35% in Spanish soccer players.12 In amateur male soccer players, a ten-week in-season NHE intervention improved peak eccentric hamstring strength by 19%,13 and lower than 2.4 Nm/kg eccentric hamstring peak torque has been associated with higher injury risk.14
No studies have examined adductor and hamstring strength longitudinally in West African soccer players. First examining whether the CAE and NHE can elicit strength gains in this population is necessary before recommending the interventions for injury risk reduction in West African soccer players. Further, strength booster periods have been suggested to counteract potential strength decay during the season,15 but no studies have explored this yet. Therefore, the authors also examined what happens to adductor and hamstring strength following a rest period and second intervention period to see if the CAE and NHE may have further beneficial and longitudinal effects on strength.
This study aims to implement the Copenhagen Adductor Exercise (CAE) and Nordic Hamstring Exercise (NHE) to examine 1) whether CAE and NHE interventions are associated with adductor and hamstring strength gains in youth West African male soccer players and 2) whether strength changes after a rest period and second intervention.
METHODS
All male players from the U14, U16, and U18 squads from one elite West African soccer academy were included. Players were excluded if a time-loss injury was present during a testing date. Data were collected in the summer and fall of 2021 on-site at the academy. This study was approved by the University of Ghana College of Health Sciences Ethical and Protocol Review Committee and all participants had a parent/guardian sign consent. The study was conducted in accordance with the ethical standards in the Declaration of Helsinki. This population was chosen to further broaden the scope of sport and exercise medicine research in understudied geographical regions.
Intervention Periods
The primary intervention period was eight weeks, followed by a four-week rest period, and a secondary ten-week intervention period. The rest period included no formal strength program or soccer training. The intervention periods included twice weekly exposures of the CAE and NHE in addition to normal soccer participation. A linear periodization program was followed with increasing weekly volume every two weeks: CAE (2x6, 2x8, 2x10, 2x12) and NHE (2x6, 3x5, 3x6, 3x8) (Figure 1). Harøy et al.7 demonstrated 470 repetitions over eight weeks leads to injury risk reduction and approximately 10% adductor strength gain. The present study employed a similar dosage in the first intervention, with 576 CAE repetitions over eight weeks. The CAE was performed with a concentric:eccentric ratio of 1:1, with each phase of the exercise spanning 2-3 seconds. The NHE was performed as slowly as possible while maintaining forward movement. The work: rest ratio was approximately 1:1, as the players rested while assisting their partner in the exercise.
Figure 1. Participant flow (n=44).
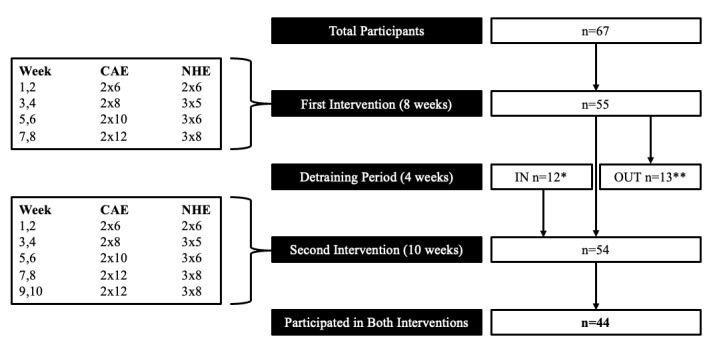
Two intervention sessions per week (sets x repetitions). NHE, Nordic hamstring exercise. CAE, Copenhagen adductor exercise. Total per first intervention period: CAE 288 repetitions each side, NHE 276 repetitions. Total per second intervention period: CAE 384 repetitions each side, NHE 372 repetitions. *Players who entered the second intervention period after being promoted to the U14 squad. **Players who exited after the first intervention period (graduated from academy n=12, unrelated injury n=1).
The CAE was performed as previously described.5 Players partnered with a teammate of similar body mass to stabilize the static limb, and repetitions were counted aloud by the group. The NHE intervention was also performed as previously described, with the resting partner holding the ankles of the exercising player.6,16 For all intervention sessions, at least one physiotherapist was present (MDD, MNH, PW) who instructed the exercise and tracked adherence. All interventions occurred prior to training, either in association with the warmup on the pitch or in a gym session. Adverse events were defined as time-loss injury related to the adductor and/or hamstring during the study period.
Soccer Exposure
Soccer exposures were tracked for each team during the intervention periods. The U14 squad trained four days per week, and the U16 and U18 squads trained five days per week. The first two weeks of each intervention period were “preseason” with a gradually increasing volume of soccer participation (three sessions in week one, four sessions in week two). A training deload week occurred in week six, with all squads participating in three training sessions and no matches. All other training weeks included training sessions and one match.
Testing Procedures
Outcome measures were performed prior to and after each intervention period (four total). To minimize post-soccer fatigue, all testing sessions were performed in lieu of soccer training on that day. The day prior to testing was always an off-day to mitigate the effects of fatigue from soccer participation, although the end-of-intervention testing dates occurred on a matchday plus two. All players had previous exposure to the CAE and NHE prior to the study period. Long lever adductor squeeze strength and prone isometric hamstring strength were captured using the microFET2 digital handheld dynamometer (Hoggan Scientific LLC, Salt Lake City, Utah, USA). The long lever adductor squeeze strength test has good reliability (intra-class coefficient 0.95 [0.87-0.98], standard error of measurement 3.2% [1.9-5.1%], minimal detectable change 6.6%.17 Long lever adductor squeeze strength was measured as an iteration of the five-second squeeze test by adding a handheld dynamometer component.18,19 The squeeze width was the tester’s forearm (MDD) plus the handheld dynamometer placed in the tester’s palm. Each player was instructed to squeeze isometrically for five seconds with maximal effort using the verbal cue “ready-go-1-2-3-4-5-and relax”. Three five-second isometric repetitions were collected with sixty seconds of rest between each. The highest squeeze score was used for data analysis.
Prone isometric hamstring strength was measured isometrically with a rigid, external belt attached to the handheld dynamometer, using the protocol established by Ishøi et al.13 The testing leg was placed in approximately 15 degrees knee flexion, with the dynamometer placed on the posterior shank 5 cm proximal to the lateral malleolus. The standardized verbal cue used was “ready-3-2-1-go-push-push-push-and relax”. Each player performed three trials with 60 seconds of rest between repetitions, and the highest output from the three trials was used for data analysis. Hamstring strength was collected one limb at a time, and an average of the maximal efforts from the left and right limbs were used for analysis.
Statistical Analyses
Isometric hamstring strength and adductor squeeze strength were used as two separate outcome variables. All statistical analyses were performed using R.20 Two mixed-effects linear regression models (one for hamstring, one for adductor) were developed with time and mass as fixed factors and player and team as random factors (random intercepts). Time was included in the models at four points: start of first intervention, end of first intervention, start of second intervention, and end of second intervention. The lm4e package was used:
lmer (Strength Measure ~ time + mass + (1|participant) + (1|team), data = data)
Assumptions were checked for each model using the performance package with the check_model function. None of the models violated any assumptions.
RESULTS
Sixty-seven players participated in at least one intervention period. Twelve players were not eligible for the first intervention because they had not yet been promoted to the U14 squad. Thirteen players missed the second intervention period due to graduation from the academy (n=12) or injury unrelated to the adductors or hamstrings (n=1). In total, 44 players (age 14.7±1.5 [12-18] years) completed the two intervention periods and were included in the present study (Table 1). Age, height, and body mass increased in the group over the course of the entire 22-week study period. The players’ countries of origin were Ghana (n=28) and Ivory Coast (n=16).
Table 1. Participant descriptive data (n=44).
| Start – Intervention 1 | End – Intervention 1 | Start – Intervention 2 | End – Intervention 2 | p (Start to End) | |
|---|---|---|---|---|---|
| Age (years) | 14.7±1.5 [12-18] |
14.8±1.4 [12-18] |
14.9±1.3 [12-18] |
15.0±1.4 [12-18] |
<0.001 |
| Height (cm) | 168.2±9.1 [145-186] | 168.9±8.8 [146.5-187] | 169.4±8.6 [147-187] | 170.6±8.3 [149-187] | <0.001 |
| Body Mass (kg) | 56.9±9.7 [40.3-75.4] | 59.5±9.9 [39.7-79.5] | 59.1±9.3 [41.1-77.1] | 60.1±9.3 [41.5-77] | <0.001 |
Players were consistently compliant with performing the interventions under the direct supervision of a physiotherapist. Ninety-six percent of all sessions were completed in the first intervention, and 95% in the second intervention period. No adverse events related to the execution of the interventions occurred, but eight groin injuries with minimal time-loss (1-3 days) and two with moderate time-loss (8-28 days) occurred during the study period. There were no hamstring injuries recorded during the intervention period.
Adductor Squeeze Strength
Mean and 95% confidence intervals at each timepoint are provided in Table 2, including comparisons between each timepoint. Adductor squeeze strength increased during the first intervention period (mean difference: 0.30 N/kg; p=0.011) and was maintained during the four-week break period (mean difference compared to end of first intervention: -0.01; p=0.999). At the start of the second intervention period, adductor squeeze strength was higher than at the start of the first intervention period (mean difference: 0.29 N/kg; p=0.022). Adductor squeeze strength did not increase during the second intervention period (mean difference 0.08 N/kg; p=0.818). From the start of the first intervention to the end of the second intervention, adductor squeeze strength improved (mean difference: 0.37 N/kg; p=0.002). The increase in adductor squeeze strength during the first intervention period (8.9%) and from the start of the first intervention to the end of the second intervention (10.8%) exceed the minimal detectable change for long lever adductor squeeze strength.
Table 2. Changes in adductor squeeze strength and hamstring strength between timepoints statistically significant at p<0.05 in bold; data presented as mean [95% confidence interval].
| Adductor squeeze strength | |||||
|---|---|---|---|---|---|
| Timepoints | Mean Difference | Significance | Percent Change | ||
| First Intervention | Start I | End I | 0.302 | 0.01 | 9.29% |
| 3.23 [2.99-3.47] | 3.53 [3.30-3.76] | ||||
| Rest Period | End I | Start II | -0.014 | 0.999 | -0.28% |
| 3.53 [3.30-3.76] | 3.52 [3.27-3.76] | ||||
| Second Intervention | Start II | End II | 0.081 | 0.818 | 2.27% |
| 3.52 [3.27-3.76] | 3.60 [3.35-3.84] | ||||
| Total Study Period | Start I | End II | 0.369 | 0.002 | 11.46% |
| 3.23 [2.99-3.47] | 3.60 [3.35-3.84] | ||||
| Hamstring strength | |||||
| Timepoints | Mean Difference | Significance | Percent Change | ||
| First Intervention | Start I | End I | 0.528 | <0.001 | 10.71% |
| 4.95 [4.42-5.49] | 5.48 [4.95-6.02] | ||||
| Rest Period | End I | Start II | -0.501 | <0.001 | -9.12% |
| 5.48 [4.95-6.02] | 4.98 [4.44-5.53] | ||||
| Second Intervention | Start II | End II | 0.023 | 0.997 | 0.60% |
| 4.98 [4.44-5.53] | 5.01 [4.46-5.55] | ||||
| Total Study Period | Start I | End II | 0.051 | 0.978 | 1.21% |
| 4.95 [4.42-5.49] | 5.01 [4.46-5.55] | ||||
Figure 2. Adductor squeeze strength (N/kg) throughout the study period. Individual players represented by black lines and group average indicated by the red line.

A significant increase occurred from Start of Term 1 to End of Term 1 (p=0.01, 9.3% increase).
Isometric Hamstring Strength
Mean and 95% confidence intervals are included in Table 2, including comparisons between each timepoint. Hamstring strength improved during the first intervention period (mean difference 0.528 N/kg; p<0.001) and decreased during the four-week break period (mean difference -0.501 N/kg; p=0.001). At the start of the second intervention period, there was no difference from the start of the first intervention period (mean difference -0.028 N/kg; p=0.996). Hamstring strength did not improve during the second intervention period (mean difference 0.023 N/kg; p=0.997). From the start of the first intervention to the end of the second intervention, no significant improvement in strength was observed (mean difference 0.051 N/kg; p=0.978).
Figure 3. Isometric hamstring strength (N/kg) throughout the study period.

Individual players represented by black lines and group average indicated by the red line. Significant increase from Start of Term 1 to End of Term 1 (p<0.001, 10.7%), and decrease from End of Term 1 to Start of Term 2 (p<0.001, -9.2%).
DISCUSSION
This study examined the implementation of the CAE and NHE in a West African soccer academy and looked upon whether CAE and NHE interventions are associated with adductor and hamstring strength gains in youth West African male soccer players during the season. Under supervision, players were compliant (96% and 95% in each intervention period), and no adverse events related to the execution of the exercises occurred. Overall, adductor squeeze strength improved in the first intervention period, was maintained during the rest period, and was unchanged in the second intervention, whereas hamstring strength increased in the first intervention, decreased to baseline during the rest period, and was unchanged in the second intervention.
Adductor squeeze strength improved 10.8% from baseline to the end of the study period. Isometric hamstring strength increased in the first intervention, decreased to baseline during the rest period, and was unchanged in the second intervention (+1.2% change from start to end of study period). Although studies have considered injury risk reduction in African soccer players,1,2,10 no studies have observed possible strength changes following CAE and NHE interventions. During the first intervention period, adductor squeeze strength and isometric prone hamstring strength each improved. This aligns with studies of the CAE and NHE in other regions, where strength improvements have also been observed.5,11 Improving strength in the adductors and hamstrings may benefit soccer performance and also be an underlying mechanism for injury risk reduction in the adductors and hamstrings.12,14 Therefore, primary interventions of the CAE and NHE to improve adductor and hamstring strength in West African soccer players may be beneficial.
During four weeks of rest from soccer and strength interventions, adductor squeeze strength was maintained but hamstring strength reduced to baseline. Strength reductions with detraining can be expected. With the NHE, decreases in strength following detraining have been reported,21 even with a detraining period of one week.22 With the CAE, detraining periods have reduced adductor longus muscle thickness in sub-elite soccer players and other recreational athletes.23 However, the present study did not demonstrate strength declines during the detraining period for the adductors. Previous studies found that adductor strength was weakest at start of preseason and after a mid-season break,24,25 suggesting adductor strength may improve with soccer exposure. Therefore, it is unclear why the adductor strength in the present study did not decrease during a detraining period without soccer participation or the CAE intervention. Perhaps the high training load of the players (5-6 days per week) coupled with CAE elicited an overloading of the adductors. Adductor strength can be decreased for up to 72 hours following a match,26 and a period of match congestion led to nearly three-quarters of Australian youth players demonstrating reduced adductor squeeze strength.27 If the players in the present study were overloaded during the first intervention period, it is possible that the rest during the detraining period was advantageous for strength.
During the second intervention, neither adductor squeeze strength nor isometric hamstring strength improved. The secondary intervention may have lacked novelty to induce neuroplastic changes and/or sufficient progressive overload to induce hypertrophic changes. The linear periodization from the first intervention was repeated in the second intervention, and it is possible that this repeated stimulus was not novel enough to elicit strength gains. It is also possible that adductor strength had plateaued at this stage, and the interventions provided maintenance of strength. Strength maintenance may be beneficial during a competitive season when the physical demand is high. For hamstring strength, however, no improvements from baseline to the end of the second intervention period may indicate an insufficient longitudinal stimulus of the NHE. In one NHE study where high-volume and low-volume interventions were compared, no strength gains are observed from mid-intervention to post-intervention; however, this study has only two weeks rest between intervention periods and no stoppage in soccer participation.28 To overcome a plateau in strength, adjusting the periodization in a secondary intervention may provide a boost.15
Compliance is often a barrier to effective interventions. In one survey study, more than 80% of UEFA Champions League and Norwegian Tippeligaen teams failed to adopt the NHE as an injury risk reduction tool.29 Despite 85% of Dutch amateur male soccer players having knowledge of the NHE and 93% of the club medical staffs believing the NHE is effective, 69% of players reported never performing the exercise.30 The present study, supported by supervision of all intervention sessions, shows that high adherence can be achieved in youth soccer players. In the long-term, placing emphasis and promoting adherence to these exercise programs may aid future first team players and staff to understand their importance. Staff who invest in CAE and NHE interventions should supervise sessions to improve compliance.
When a new intervention is introduced to a population, it is important to consider whether any adverse events may occur. In this study no adverse events related to the execution of the intervention occurred. During the intervention period eight minimal time-loss (1-3 days) and two moderate time-loss (8-28 days) adductor injuries occurred which is lower or within what is to be expected at this level. It was very positive that there were no cases of long-standing or severe time-loss adductor cases, and no hamstring injuries, as these injuries both may pose a high burden on young soccer players.31 The CAE and NHE exercises, thus seems to be safe interventions to implement in West African academy soccer players.
Clinical Implications
Although previous studies have shown lacking compliance for the CAE and NHE, these interventions can be effectively implemented under supervision in West African academy soccer players. Developing stronger adductors and hamstrings may be advantageous for soccer players, as these muscle groups experience high demands during soccer actions such as high-speed running, kicking, and cutting.32 Although a direct link to injury risk reduction cannot be made with the current study design, the CAE and NHE can increase adductor and hamstring strength, which has been shown to mitigate both adductor and hamstring injuries.5,6,14,33
Adductor squeeze strength improved 8.9% during the first intervention and 10.8% from the start to end of the study period, indicating that meaningful detectable change (>6.6%)17 occurred. Maintained improvements in adductor squeeze strength throughout the study period are evident, although strength did not further increase during the second intervention period. CAE interventions should be implemented in academy soccer populations. If additional longitudinal strength gains are desired, perhaps a novel stimulus could be added to the CAE such as increasing the exercise volume, adding external load, or increase the time under tension during the eccentric phase (3:1 eccentric-to-concentric ratio).
Hamstring strength initially improved (+10.2% in the first intervention), suggesting the dosage of the NHE was sufficient to create strength changes. However, hamstring strength returned to baseline during the rest period and did not increase in the second intervention period. Perhaps ongoing hamstring strength exercises during breaks from soccer training seems important to maintain strength. To promote more longitudinal hamstring strength gains, a novel stimulus should be introduced. This may be achieved by altering the periodization of the programming, adding band-assistance to increase time under tension,34 or include other hamstring-related demands such as a linear sprinting program.35
Limitations
Because the study was conducted in an applied soccer setting, no control group was included to consider whether injury risk reduction may have occurred. Additionally, no non-soccer control group was included to differentiate between strength changes attributed to the intervention compared to soccer exposure itself. Soccer participation seems to influence adductor strength independent of the CAE, as adductor strength differed 27% between U13 and U15 Danish soccer players even when normalized to body mass.36 The present study controlled for maturation using only values relative to body mass and did not capture leg length to examine torque. A future multifactorial approach should examine CAE and NHE interventions in conjunction with soccer training load and maturation status to better understand the interplay between these factors.
CONCLUSION
CAE and NHE interventions can be implemented at a West African soccer academy with high compliance and no adverse events. These exercises improve adductor and hamstring strength the after an eight–week intervention period, with no further improvements in adductors and a decrease in hamstring after second intervention period. Secondary interventions during the season therefore may need higher exercise volume or load if the goal is to improve longitudinal adductor and hamstring strength gains in academy players throughout the season.
Competing interests
The authors have no competing interests to report for this study.
References
- Efficacy of the FIFA 11+ warm-up programme in male youth football: A cluster randomised controlled trial. Owoeye O. B., Akinbo S. R., Tella B. A., Olawale O. A. 2014J Sports Sci Med. 13(2):321–8. [PMC free article] [PubMed] [Google Scholar]
- Effect of the FIFA 11+ soccer specific warm up programme on the incidence of injuries: a cluster-randomised controlled trial. Nuhu A., Jelsma J., Dunleavy K., Burgess T. 2021PLoS One. 16(5):e0251839. doi: 10.1371/journal.pone.0251839. doi: 10.1371/journal.pone.0251839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Werner J., Hägglund M., Waldén M., Ekstrand J. 2009Br J Sports Med. 43(13):1036–40. doi: 10.1136/bjsm.2009.066944. doi: 10.1136/bjsm.2009.066944. [DOI] [PubMed] [Google Scholar]
- Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men's professional football: the UEFA Elite Club Injury Study from 2001/02 to 2021/22. Ekstrand J., Bengtsson H., Waldén M., Davison M., Khan K.M., Hägglund M. 2022Br J Sports Med. 57(5):292–8. doi: 10.1136/bjsports-2021-105407. doi: 10.1136/bjsports-2021-105407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Harøy J., Clarsen B., Wiger E.G.., et al. 2019Br J Sports Med. 53(3):150–157. doi: 10.1136/bjsports-2017-098937. doi: 10.1136/bjsports-2017-098937. [DOI] [PubMed] [Google Scholar]
- The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. van der Horst N., Smits D. W., Petersen J., Goedhart E. A., Backx F. J. 2015Am J Sports Med. 43(6):1316–23. doi: 10.1177/0363546515574057. doi: 10.1177/0363546515574057. [DOI] [PubMed] [Google Scholar]
- Including the Copenhagen Adduction Exercise in the FIFA 11+ provides missing eccentric hip adduction strength effect in male soccer players: a randomized controlled trial. Harøy J., Thorborg K., Serner A., Bjørkheim A., Rolstad L. E., Hölmich P., Bahr R., Andersen T. E. 2017Am J Sports Med. 45(13):3052–3059. doi: 10.1177/0363546517720194. doi: 10.1177/0363546517720194. [DOI] [PubMed] [Google Scholar]
- The 11+ of the future: a primary injury prevention framework for sub-elite football. Whalan M., Lovell R., Thorborg K., Sampson J.A. Oct 15;2020 Br J Sports Med. 2020 doi: 10.1136/bjsports-2020-102788. doi: 10.1136/bjsports-2020-102788. [DOI] [PubMed] [Google Scholar]
- Effects of a groin pain prevention program in male high school soccer players: a cluster-randomized controlled trial. Fujisaki K., Akasaka K., Otsudo T., Hattori H., Hasebe Y., Hall T. 2022Int J Sports Phys Ther. 17(5):841–850. doi: 10.26603/001c.36631. doi: 10.26603/001c.36631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Effect of pre-training and post-training Nordic exercise on hamstring injury prevention, recurrence, and severity in soccer players. Elerian A. E., El-Sayyad M. M., Dorgham H. A. A. 2019Ann Rehabil Med. 43(4):465–473. doi: 10.5535/arm.2019.43.4.465. doi: 10.5535/arm.2019.43.4.465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Large eccentric strength increase using the Copenhagen Adduction exercise in football: a randomized controlled trial. Ishøi L., Sørensen C. N., Kaae N. M., Jørgensen L. B., Hölmich P., Serner A. 2016Scand J Med Sci Sports. 26(11):1334–1342. doi: 10.1111/sms.12585. doi: 10.1111/sms.12585. [DOI] [PubMed] [Google Scholar]
- Past-season, pre-season and in-season risk assessment of groin problems in male football players: a prospective full-season study. Esteve E., Casals M., Saez M.., et al. 2022Br J Sports Med. 56(9):484–489. doi: 10.1136/bjsports-2020-102606. doi: 10.1136/bjsports-2020-102606. [DOI] [PubMed] [Google Scholar]
- The influence of hamstring muscle peak torque and rate of torque development for sprinting performance in football players: A cross-sectional study. Ishøi L., Aagaard P., Nielsen M. F.., et al. 2018Int J Sports Physiol Perform. doi: 10.1123/ijspp.2018-0464. [DOI] [PubMed]
- Eccentric hamstring strength deficit and poor hamstring-to-quadriceps ratio are risk factors for hamstring strain injury in football: a prospective study of 146 professional players. Lee J. W. Y., Mok K. M., Chan H. C. K., Yung P. S. H., Chan K. M. 2018J Sci Med Sport. 21(8):789–793. doi: 10.1016/j.jsams.2017.11.017. doi: 10.1016/j.jsams.2017.11.017. [DOI] [PubMed] [Google Scholar]
- Copenhagen adduction exercise can increase eccentric strength and mitigate the risk of groin problems: but how much is enough! Ishøi L., Thorborg K. 2021Br J Sports Med. 55(19):1066–1067. doi: 10.1136/bjsports-2020-103564. doi: 10.1136/bjsports-2020-103564. [DOI] [PubMed] [Google Scholar]
- A 10-week randomized trial comparing eccentric vs concentric hamstring strength training in well-trained soccer players. Mjølsnes R., Arnason A., Osthagen T., Raastad T., Bahr R. 2004Scand J Med Sci Sports. 14:311–317. doi: 10.1046/j.1600-0838.2003.367.x. [DOI] [PubMed] [Google Scholar]
- The precision and torque production of common hip adductor squeeze tests used in elite football. Light N., Thorborg K. 2016J Sci Med Sport. 19(11):888–892. doi: 10.1016/j.jsams.2015.12.009. doi: 10.1016/j.jsams.2015.12.009. [DOI] [PubMed] [Google Scholar]
- Copenhagen five-second squeeze: a valid indicator of sports-related hip and groin function. Thorborg K., Branci S., Nielsen M. P.., et al. 2017Br J Sports Med. 51:594–599. doi: 10.1136/bjsports-2016-096675. [DOI] [PubMed] [Google Scholar]
- Hip adduction strength and provoked groin pain: A comparison of long-lever squeeze testing using the ForceFrame and the Copenhagen 5-second squeeze test. Nielsen M. F., Thorborg K., Krommes K.., et al. 2022Phys Ther Sport. 55:28–36. doi: 10.1016/j.ptsp.2022.02.002. [DOI] [PubMed] [Google Scholar]
- R Core Team . R: A language and environment for statistical computing. R Foundation for Statistical Computing; Vienna, Austria: https://www.R-project.org/ [Google Scholar]
- Acute adaptations and subsequent preservation of strength and speed measures following a Nordic hamstring curl intervention: a randomised controlled trial. Siddle J., Greig M., Weaver K., Page R. M., Harper D., Brogden C. M. 2019J Sports Sci. 37(8):911–920. doi: 10.1080/02640414.2018.1535786. doi: 10.1080/02640414.2018.1535786. [DOI] [PubMed] [Google Scholar]
- Razor hamstring curl and Nordic hamstring exercise architectural adaptations: impact of exercise selection and intensity. Pollard C. W., Opar D. A., Williams M. D., Bourne M. N., Timmins R. G. 2019Scand J Med Sci Sports. 29(5):706–715. doi: 10.1111/sms.13381. doi: 10.1111/sms.13381. [DOI] [PubMed] [Google Scholar]
- Effects of Copenhagen Adduction Exercise on muscle architecture and adductor flexibility. Alonso-Fernández D., Fernández-Rodríguez R., Taboada-Iglesias Y., Gutiérrez-Sánchez Á. 2022Int J Environ Res Public Health. 19(11):6563. doi: 10.3390/ijerph19116563. doi: 10.3390/ijerph19116563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eccentric strengthening effect of hip-adductor training with elastic bands in soccer players: a randomised controlled trial. Jensen J., Hölmich P., Bandholm T., Zebis M.K., Andersen L.L., Thorborg K. 2014Br J Sports Med. 48(4):332–8. doi: 10.1136/bjsports-2012-091095. doi: 10.1136/bjsports-2012-091095. [DOI] [PubMed] [Google Scholar]
- In-season monitoring of hip and groin strength, health and function in elite youth soccer: implementing an early detection and management strategy over two consecutive seasons. Wollin M., Thorborg K., Welvaert M., Pizzari T. 2018J Sci Med Sport. 21(10):988–993. doi: 10.1016/j.jsams.2018.03.004. doi: 10.1016/j.jsams.2018.03.004. [DOI] [PubMed] [Google Scholar]
- Markers of muscle damage and strength performance in professional football (soccer) players during the competitive period. Khaitin V., Bezuglov E., Lazarev A.., et al. 2021Ann Transl Med. 9(2):113. doi: 10.21037/atm-20-2923. doi: 10.21037/atm-20-2923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The effects of football match congestion in an international tournament on hip adductor squeeze strength and pain in elite youth players. Wollin M., Pizzari T., Spagnolo K., Welvaert M., Thorborg K. 2018J Sports Sci. 36(10):1167–1172. doi: 10.1080/02640414.2017.1363452. doi: 10.1080/02640414.2017.1363452. [DOI] [PubMed] [Google Scholar]
- Hamstring eccentric strengthening program: does training volume matter? Lacome M., Avrillon S., Cholley Y., Simpson B. M., Guilhem G., Buchheit M. 2019Int J Sports Physiol Perform. 2019:1–27. doi: 10.1123/ijspp.2018-0947. doi: 10.1123/ijspp.2018-0947. [DOI] [PubMed] [Google Scholar]
- Evidence-based hamstring injury prevention is not adopted by the majority of Champions League or Norwegian Premier League football teams: the Nordic Hamstring survey. Bahr R., Thorborg K., Ekstrand J. 2015Br J Sports Med. 49(22):1466–71. doi: 10.1136/bjsports-2015-094826. doi: 10.1136/bjsports-2015-094826. [DOI] [PubMed] [Google Scholar]
- Effective but not adhered to: how can we improve adherence to evidence-based hamstring injury prevention in amateur football? van der Horst N., Hoef S. V., Otterloo P. V., Klein M., Brink M., Backx F. 2021Clin J Sport Med. 31(1):42–48. doi: 10.1097/JSM.0000000000000710. doi: 10.1097/JSM.0000000000000710. [DOI] [PubMed] [Google Scholar]
- A multidisciplinary assessment of 320 athletes with long-standing groin pain syndrome in keeping with the Italian consensus agreement: the high incidence and the multiple causes of inguinal and hip pathologies and pubic osteopathy. Bisciotti G. N., Auci A., Bona S.., et al. 2021J Sports Med Phys Fitness. 61(7):960–970. doi: 10.23736/S0022-4707.20.11575-5. doi: 10.23736/S0022-4707.20.11575-5. [DOI] [PubMed] [Google Scholar]
- Muscle activity of cutting manoeuvres and soccer inside passing suggests an increased groin injury risk during these movements. Dupré T., Tryba J., Potthast W. 2021Scientific reports. 11(1):7223. doi: 10.1038/s41598-021-86666-5. doi: 10.1038/s41598-021-86666-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Which factors differentiate athletes with hip/groin pain from those without? A systematic review with meta-analysis. Mosler A. B., Agricola R., Weir A., Hölmich P., Crossley K. M. 2015Br J Sports Med. 49(12):810. doi: 10.1136/bjsports-2015-094602. doi: 10.1136/bjsports-2015-094602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Assisted or unassisted Nordic Hamstring Exercise? - Resistance exercise determinants at a glance. Alt T., Knicker A. J., Nodler Y. T., Strüder H. K. 2021Sports Biomech. 16:1–15. doi: 10.1080/14763141.2021.1893376. doi: 10.1080/14763141.2021.1893376. [DOI] [PubMed] [Google Scholar]
- The effects of sprint training and the Nordic hamstring exercise on eccentric hamstring strength and sprint performance in adolescent athletes. Freeman B. W., Young W. B., Talpey S. W., Smyth A. M., Pane C. L., Carlon T. A. 2019J Sports Med Phys Fit. 59(7):1119–1125. doi: 10.23736/S0022-4707.18.08703-0. doi: 10.23736/S0022-4707.18.08703-0. [DOI] [PubMed] [Google Scholar]
- Rapid spike in hip adduction strength in early adolescent footballers: a study of 125 elite male players from youth to senior. Light N., Thorborg K., Krommes K.., et al. 2022Int J Sports Physiol Perform. 17(9):1407–1414. doi: 10.1123/ijspp.2022-0025. doi: 10.1123/ijspp.2022-0025. [DOI] [PubMed] [Google Scholar]