

Abstract
Introduction. Dental fatigue fractures are the result of occlusal overloads occurring because of increased intensity of occlusal forces or decreased resistance of dental hard tissues to habitual occlusal forces. In the COVID-19 pandemic, occlusal stress has increased significantly, and so has the number of dental fractures. The study has the aim to determine if the number of cases of dental fatigue fractures during the pandemic crisis was higher than in the immediately preceding period. Methodology. The retrospective study was carried out in a private dental clinic, selecting from the case series presented during March 2019-March 2021 the cases of dental fatigue fractures presented for diagnosis and treatment. The data collected from the patients included the reason for the presentation, the dental and medical history, and results from dental examination and radiological data. The statistical analysis was carried out with Microsoft Excel and SPSS software. Results. The study included 644 patients, 430 women and 214 men, with ages between 25 and 85 years (61±7.4 years). From a total of 2581 visits, 1534 visits were made to 383 patients between March 2019 and March 2020, and 1047 visits were made to 261 patients between March 2020 and March 2021, the number of visits decreasing by 31.75% during the pandemic. During the pandemic, the number of fractured teeth tripled, increasing from 0.53% to 1.53% (p=0.009). The most affected teeth were the maxillary premolars and the permanent first molar, both mandibular and maxillary. In most cases, the indication for treatment was extraction. Conclusions. The Sars-Cov2 virus pandemic crisis has significantly increased the number of teeth with dental fatigue fractures presented to the dental office for diagnosis and treatment.
Keywords: Cracked Teeth , Vertical Root Fracture (VRF) , Pandemic Crisis , Dental Fatigue Fractures
Introduction
Cracked teeth and vertical root fractures became an important part of the dental pathology in the late decades, because of their growing incidence and because treatment is hard to accomplish in a conservatory way.
These entities are considered a part of occlusal disease, triggered by occlusal overload [1, 2].
Repeated excessive occlusal loads generate dental stress and microtrauma. Stress results in compression, flexion, and tension on teeth.
It produces microfractures and abfractions in teeth as first signs of occlusal disease [1].
When Grippo first defined abfraction as a non-carious cervical lesion induced by occlusal stress, it was universally accepted as a common term for occlusal disease [1, 3, 4, 5].
In occlusal disease dental lesions appear as dental wear, cracked teeth, root fractures, occlusal trauma, fremitus [1, 2].
Occlusal disease with excessive occlusal loads can occur in the case of a complete dentition by increasing the intensity of occlusal forces as in bruxism [6] or in the case of a reduced teeth number that support an occlusal force abnormally distributed as in partial edentulism [7].
Cracked teeth aetiology includes the factors that increase occlusal overloads by increasing the intensity of masticatory muscle contraction as in bruxism [6, 8] and factors that reduce the resistance of teeth to forces (non-iatrogenic and iatrogenic) cited by Ellis et al. [9] and Bhanderi et al. [10] (Table 1).
Table 1.
|
Etiological factors of tooth fracture | ||
|
Factors that increase occlusal overloads |
-long term unilateral chewing -decreased number of teeth -rotation and tilting of teeth -isolated teeth -awake and sleep bruxism |
|
|
Factors that decrease tooth resistance to occlusal forces |
Non-iatrogenic |
-increased levels of dental fatigue in teeth with age -increased number of restored teeth with age -loss of dentin elasticity with age -the tooth structural defect (hypoplasia, dentinogenesis imperfecta) -tooth morphology (steep cusp inclination, deep grooves) -thermal cycling eating habits -tongue piercing |
|
Odonto-iatrogenic |
-excessive removal of tooth tissue in restorative procedures or root canal treatment -tooth dehydration and collagen depletion (higher concentration of sodium hypochlorite in root canal treatment) -large tooth restorations without cuspal protection -use of restorative materials with different thermal expansion coefficient and different mechanical properties compared with the tooth |
|
Described over time in the dental literature under different names, cracked teeth (fatigue tooth fracture) were defined by the American Association of Endodontics (AAE) as 5 types of tooth lesions: enamel craze line, cusp fractured, cracked tooth, split tooth, and vertical root fracture [11, 12].
AAE later returned with other definitions, including also abfraction, infraction (craze line), fracture, root fracture, longitudinal fracture, split root [13, 14, 15] (Table 2).
Table 2.
|
Term |
Definition |
|
abfraction |
a V-shaped lesion in the cervical part of the tooth crown, produced by the flexure of the tooth as a result of the biomechanical loading |
|
craze line (infraction) |
a crack in the enamel |
|
cracked tooth |
a disruption of the structure of the tooth |
|
root fracture |
a fracture of the root of the tooth |
|
longitudinal fracture |
a fracture that follows the axial plane of the tooth. |
|
vertical root fracture |
avertical fracture of the root |
|
split root |
avertical fracture of the root with separation of the fractured fragments |
Cracked teeth from vital teeth without dental treatments were frequently found in the upper molars, especially the first molar, but also in the lower first molars, followed by the premolars [16].
The direction of fracture evolution was in most cases mesial-distally [16].
Fatigue dental fractures are characterized as vertical fractures of the crown and/or dental roots, which occur especially in nonvital teeth, and endodontically treated teeth [17, 18], but also in vital teeth[18, 19, 20].
For crown fractures of vital teeth, the term "cracked tooth syndrome" is used, while for root fractures of vital or nonvital teeth, the term "vertical root fractures" is used [12, 13].
Vertical root fracture is a longitudinal fracture of the root of the tooth that could involve the cementum, dentin, and root canal.
Although it is commonly found in nonvital teeth, this type of fracture can also occur in vital teeth.
Vertical root fracture can be incomplete, in this case the fracture involves only partial the root, and complete when the fracture is extending from one face of the tooth to the other [21].
The direction in which the fracture propagates can be corono-apical or apico-coronal, to the same extent [22].
According to Arx et al., vertical root fractures develop especially in the buccal-lingual plane of the teeth [23].
The origin of the root fractures would be mainly in the cervical or apical part of the root [22].
When a fracture evolveswith the separation of the two parts of the tooth, the situation is called split root [13].
Because crown-root fractures propagate very slowly (they are fatigue fractures) and appear without a sign or symptom, their diagnosis is very difficult.
These fractures usually are observed in the final stage of the fracture, of separating the fragments, in nonvital teeth [17].
Unlike traumatic fractures, being unnoticed for a long period of time, the moment when they become evident is therapeutically overcome, and the only treatment is tooth extraction [17, 21].
Tooth extraction of fractured teeth because of chronic stress was encountered in 9.5% of all extracted teeth in a general dental office and in 25.8% of all extracted teeth in an endodontic practice, over 5 years [17].
In the case of vital teeth, vertical root fractures (VRF) are manifested by hypersensitivity when they have not affected the pulp and by acute pulpitis if the pulp chamber is affected [20].
Early diagnosis is essential for keeping the tooth on the arch in the case of incomplete fractures.
If extraction is necessary, it is very important that it be done early, to prevent bone resorption that can have a negative impact on the implant-prosthetic treatment in the edentulous area resulting after tooth extraction [17, 20].
The factors considered for the prevalence of catastrophic VRF are age, gender, and tooth. Vertical root fractures are more commonly associated with nonvital teeth compared to vital teeth [17, 24].
Yoshino et al. observed that 82.1% from all teeth had cast posts or screw posts, and the most affected tooth was lower first molar [24].
In vital teeth, the incidence of chronic fatigue root fracture was 0.76% in an asian population.
Vertical root fractures and horizontal root fractures occured mainly in aged men (over 70 years old), in posterior teeth with attrition, without restorations [20].
In a romanian population, vertical root fractures occured mainly in adult women (over 40 years old), in nonvital teeth, in upper premolars and lower molars [17].
Back in 2022, AAE published a paper with the theme of increasing number of cracked teeth in pandemia with Sars Cov2 [13].
The pandemic with the Sars-Cov2 virus had the effect in the first instance of the closure of dental services worldwide, followed by a period of approximately 1 year with restrictions on the performance of the dental medical act.
On the other hand, patients with dental problems had an additional stress factor that led to postponing the visit to the dentist, namely, the fear of contracting the COVID-19 disease [25, 26].
In Romania, the pandemic with the SARS CoV2 virus had negative effects on dentistry by establishing a state of emergency with the closure of dental offices and later the introduction of distancing rules that reduced patients' access to the office maintained for over a year [27].
Overall, during the pandemic, the number of visits to the dentist decreased, with patients presenting mainly for dental emergencies. Among the emergencies patients presented for, cracked teeth had an alarming increase [26].
This phenomenon happened also in other countries, such as the USA [28], Saudi Arabia [29].
Appeared as a rumour in the dental environment, this increase in the number of cracked teeth began to be documented through observational studies and retrospective studies carried out in both endodontic and general dentistry offices [28, 29, 30].
As it is recognized that the Sars-Cov2 virus pandemic was characterized by stressand anxiety among the population, as well as dental anxiety, the question as to whether this has resulted in an increased number of cases of tooth fractures because of increasing occlusal overload is important.
Dental fatigue fractures represent the third cause of edentulism, after periodontal disease and dental caries [31].
As far as we know, there is no other report of the situation of the fatigue tooth fractures in pandemic period compared to anterior period for the Romanian population.
For other countries, like United States [28] and Saudi Arabia [28] the reports were already published.
The aim of the retrospective study was to compare the number of cracked teeth in the period March 2020-March 2021 with the number of cracked teeth in the period March 2019-March 2020, before the pandemic in a general dentistry practice.
The null hypothesis is that the two periods present similar results.
Materials and Methods
This retrospective cohort study complied with the guidelines for Strengthening the Reporting of Observational Studies in Epidemiology [32].
Study population and design of the study
The study collected data from a General Dentistry Clinic from Craiova over two years of observations (March 2019-February 2020, March 2020-February 2021).
Thus, two groups were constituted: the study group, from the pandemic period and the control group from the period before the pandemic.
All the patients whose data was used in the study gave a previous written inform consent for use of their data in clinical studies.
All the patients gave informed written consent for all investigations and treatments received.
The dental office was closed only during the period from March 16 to May 31, 2020, the lockdown period in Romania [27].
During the pandemic period, distancing rules and screening rules were introduced at the office, with the completion of the questionnaire for detecting COVID-19 and thermometry.
In both periods, appointments were made by phone.
The doctors who worked in the two periods were the same.
Informed consent
All patients were informed about the possibility of publishing their data and their informed consent was obtained for any diagnostic and treatment procedure and for publishing the data.
The protocol of this study was approved by the Ethics Committee of University of Medicine and Pharmacy of Craiova, No. 156/25.07.2022, which certifies that the ethical principles underlying the Declaration of Helsinki and the Code of University Ethics regarding the proper conduct complied with the research process, together with the codes of practice established by the Code of Medical Ethics
Inclusion criteria
The study included all visits performed by young and adult patients (over 18 years of age) in period described.
Exclusion criteria
The study excluded all visits of the children presented to the dental clinic in the studied period.
Data collection
Data collected in this study are from the young and adult patients who visited the clinic during the two years.
The data collected from the patients included the reason for the presentation, the dental and medical history, and the data obtained from the dental examination.
These data included the degree of tooth destruction and the type of dental crown reconstruction.
Data obtained from the percussion tests, palpation, the bite test, cold and hot testing, periodontal survey, and assessment of dental mobility were used to establish a positive or negative diagnostic for vertical root fracture [33].
Also, the radiological evaluation done on RIO, OPG and CBCT in certain situations was used for diagnostic.
The collected data were noted in the patients' file.
The patients were followed up until the problem for which they presented themselves was solved.
To extract the data, the patient files, as well as the radiographs and CBCT, were reviewed.
Analyzed data included the number of patients, the number of visits, and the number of fractured teeth in the studied period.
The demographic data of age and gender, the final diagnosis of root fracture, the type of the fractured tooth (upper or lower, incisive, canine, premolar or molar), the situation of the fractured tooth (root canal treated or not, crowned tooth, tooth with post and core), as well as the treatment for the fractured tooth, were recorded.
The initial database was created in Microsoft Excel. Statistical Package for Social Sciences (SPSS), version 26 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables were expressed as mean±standard deviation (SD), nominal and ordinal variables were expressed as absolute and relative frequencies (%).
The Chi-square test was used for association, and the statistical significance was set at p <0.05.
Results
644 patients from Oltenia region were included in the study.
From them, 383 presented for dental treatment in first period of the study (March 2019-February 2020) and represented control group and 261 presented for dental treatment in the second period of the study (March 2020-February 2021) and represented study group.
Overall, the entire group was imbalanced regarding gender distribution, with a female predominance, of 66.77%.
The age for the study group was between 25 and 85 years old, (mean age 60.43±9.37 years).
The age for the control group was between 25 and 84 years old (mean age 61.52±8.61 years).
Out of the total of 2581 visits, 1534 were in the period March 2019-March 2020, and 1047 in the period March 2020-March 2021, the number of visits decreasing by 31.75% during the pandemic (Figure 1).
Figure 1.
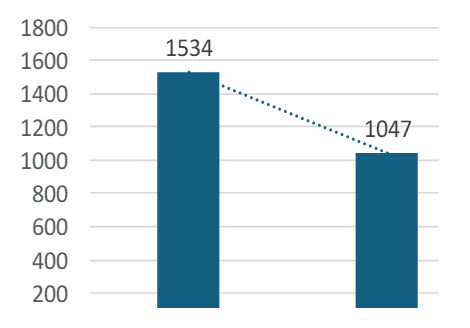
Number of dental visits in anterior pandemic period and pandemic period
During the pandemic, the number of vertical root fractures tripled, increasing from 0.52% to 1.53% (Figure 2).
Figure 2.
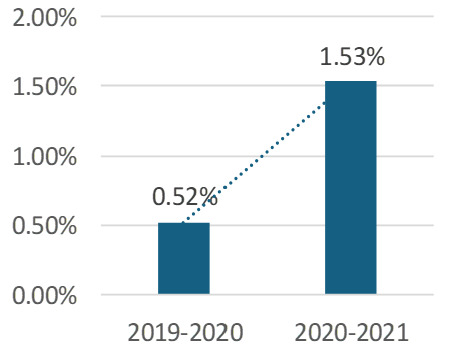
Number of tooth fractures in anterior pandemic period and pandemic period
A chi-square test for association was conducted between period (before and during the COVID pandemics) and the number of vertical root fractures.
All expected cell frequencies were greater than five.
There was a statistically significant association between period and number of vertical root fractures, χ2(1)=6.845, p=0.009.
The fractured teeth were the permanent upper first molars (26.08%), then maxillary first premolars (17.39%), and in fewer cases upper second premolars (13.04%), lower first molars (13.04%) and upper canines (13.04%).
In most cases, the indication for treatment was extraction (Figure 3).
Figure 3.
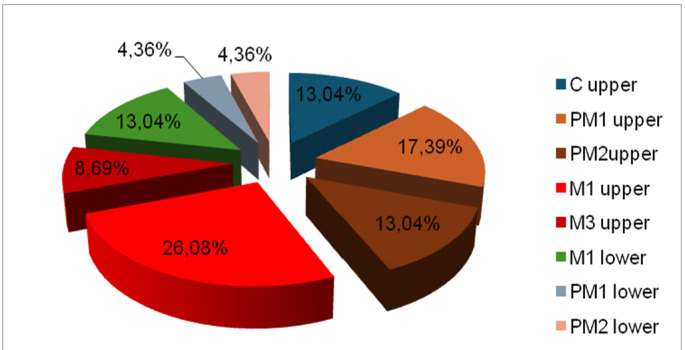
Frequency of teeth fractures in lower and upper teeth
The majority of the fractured teeth were root canal treated (RCT) (59%) and restored with crowns (43%).
Only 22% from fractured teeth had restorations with cast post and core (Figure 4).
Figure 4.
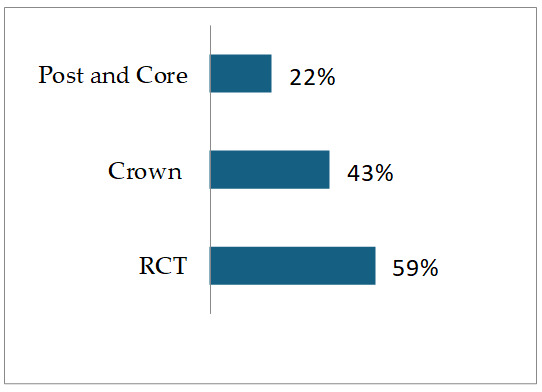
Restoration types in fractured teeth
The fractured teeth that remained on the dental arch were restored with full coverage crowns, usually monolithic zirconia.
The results of the study rejected the null hypothesis, showing a statistically significant increase in fatigue tooth fractures in pandemic crisis.
Discussion
The study showed a statistically significant increased incidence of dental fatigue fractures during the second studied period (in pandemic crisis) when compared to the anterior period, as for the number of dental visits.
This trend observed by the authors was reported also by other researchers such as Nocini et al. [34].
They observed an increased number of fractured teeth in the UK and US during the COVID pandemic through an infodemiological analysis. Earlier in 2021, the ADA reported an increased prevalence of dental fracture cases in 2021 as well as stress-related oral conditions [26].
Indeed, this phenomenon may be due to the increase in stress because of the pandemic [6] but also because of late presentation to dentist consequence of the anxiety related to the fear of contamination in the dental office [35].
The phenomenon was reported by Nosrat et al. in the study published in 2022, in which the authors showed that the number of fractured teeth increased in the period 2020-2021, compared to 2019 [28].
Their study showed that fractured teeth were more frequent in patients aged between 40-60 and over 60, male, compared with another study of our team, that established a higher frequence for root fractures in women [17].
In the present study, most of the fractures that occurred were crown-root fractures in nonvital teeth, which required tooth extraction.
The prevalence of vertical root fractures was higher in the nonvital teeth compared to vital teeth in studies conducted on Western populations, ranging from 2-5% to 3.9-25% for endodontically treated teeth, according to the analysis carried out by Liao et al. [36].
According to another analysis published in 2022, the prevalence of VRF in endodontically treated teeth would be even higher, between 4-32% [21].
For the Chinese population, two studies showed a higher prevalence of VRFNETT (VRF in teeth not treated in the root canal) among teeth with vertical fractures-40% of 315 cases of VRF [37] and 80% in 51 cases by VRF [38].
Also, in a study published in 2023 that analyzed the prevalence of VRF in the population, Ek et al. [29] compared the prevalence of VRF in 21156 patients from a university endodontic program (UEP) with the prevalence of VRF in 7209 patients from a private dental practice.
The retrospective study carried out over a long period of time, between the years 2006-2022, showed a combined prevalence of VRF of 2.01%, this being lower in the UEP (1.8%) and higher in the private practice (2.62%).
Comparing the pre-Covid (2006-2019) and the COVID (2020-2022) periods, a statistically significant increase in the prevalence of vertical root fractures was found (1.72% in the pre-COVID-19 to 3.82% in the COVID-19 period).
The prevalence of suspected VRF cases was 0.99% pre-pandemic, increasing statistically significantly in the pandemic to 2.31%.
The prevalence of confirmed cases of VRF was also increasing from 0.65% to 1.01%, statistically significant [29].
The most affected teeth in the present study were nonvital teeth, and as the type of tooth, the 1st upper molars and the two upper premolars.
In a previous study of root fractures on Romanian population, most affected teeth were also nonvital teeth (88.2%), and as tooth type, upper premolars, and lower molars [17].
In a study in the Japanese population conducted on 288 endodontically treated teeth with isolated periodontal pockets larger than 5mm, Lee et al. [39] observed a 32% prevalence of vertical root fractures.
Lower first molars (31.5%) and premolars (30.2%) were the teeth most affected by VRF.
The type of periodontal pocket encountered was narrow buccolingual with a frequency in VRF of 78.1%.
A narrow buccolingual periodontal pocket, premolars, crown restorations and post tooth quality showed significant associations with VRF.
The cited study [39] is even more relevant compared to another studies on the prevalence of vertical root fractures (VRF), since these studies analyzed extracted teeth or teeth with apical surgery [17].
In our study, upper molars and premolars were most affected teeth.
Analysis of the mechanism of stress propagation through teeth structures showed that vertical and horizontal excessive loading accumulate in the buccal cusp and buccal cervical area of the tooth [40].
Enamel layer was most affected by maximum stress generated by vertical excessive occlusal load [41].
If tooth did not wear horizontally and its form has sharp edges, these act as mechanical stress concentrators, favoring tooth fracture [42].
The type of restoration frequently encountered in fractured teeth from the current study was dental filling in endodontically treated tooth, while crowned teeth had a proportion of 43%.
Other studies have shown that teeth covered with crowns resist stress better and fracture less often [21].
Unfortunately, many Romanian adult patients choose to not cover a root canal treated tooth with crown for financial reason [17, 43, 44].
Regarding the treatment of fractured teeth, this was extraction for teeth with total crown-root fractures.
However, for vital teeth with cusp fractures and vital teeth where the fracture was only in the crown, the metal-ceramic or zirconium dental crown was chosen as treatment.
Thus, in a 3D finite element analysis (FEA) study, Jiang et al. [45] showed that crown restoration materials with a higher MOE (material of enamel), a more economical coronal preparation and a sufficiently large size of the abutment are factors that prevent fractures of teeth covered with crown restorations, in case of the crown fracture.
Regarding the materials tested, it seems that the use of zirconium for restorations decreases the probability of the extension of already existing fractures.
That is why the use of high MOE ceramics (Zr has 200,000 MPa) is recommended for teeth prone to fractures, or already fractured [45].
Restoration options for fractured teeth depend on the type of the fracture, of the tooth and of the patient.
The study by Gokturk et al. [46] showed that an intact molar can fracture at an occlusal overload of 2500 N.
From another study [45] it emerged that the tooth that already has a fracture should be coronally prepared with a very low threshold, of maximum 0.7mm (so the thickness of the crown at the package of 0.7mm), with a coronal length covering the fracture of 0.8mm.
The crown should be made of zirconium and cemented with a glass ionomer cement.
Acknowledgments
This research project did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors
Conclusion
The current study showed a significantly higher number of fatigue fractured teeth during the pandemic compared to the period from the anterior year.
The most affected teeth were nonvital teeth, upper first molars and upper first premolars.
Treatment was tooth extraction in most cases.
In cases when teeth could be preserved, a zirconia monolithic crown was used to protect the tooth, cemented with a glass ionomer cement.
Conflict of interests
The authors have no conflict of interest to declare.
References
- 1. Dawson P. In: Functional Occlusion: From TMJ to Smile Design. 1. Dawson P, editor. St. Louis Missouri : Mosby Elsevier; 2007 . Chapter 3. Occlusal Disease ; pp. 17 – 26 . [Google Scholar]
- 2.Ruiz JL. Seven signs and symptoms of occlusal disease: the key to an easy diagnosis. Dent Today. 2009;28(8):112–3. [PubMed] [Google Scholar]
- 3.Grippo JO, Simring M, Coleman TA. Abfraction, abrasion, biocorrosion, and the enigma of noncarious cervical lesions: a 20-year perspective. J EsthetRestor Dent. 2012;24(1):10–23. doi: 10.1111/j.1708-8240.2011.00487.x. [DOI] [PubMed] [Google Scholar]
- 4.Grippo JO. Abfractions: a new classification of hard tissue lesions of teeth. J Esthet Dent. 1991;3(1):14–19. doi: 10.1111/j.1708-8240.1991.tb00799.x. [DOI] [PubMed] [Google Scholar]
- 5.Stănuși A, Ionescu M, Cerbulescu C, Popescu SM, Osiac E, Mercuț R, Scrieciu M, Pascu RM, Stănuși AŞ, Mercuț V. Modifications of the Dental Hard Tissues in the Cervical Area of Occlusally Overloaded Teeth Identified Using Optical Coherence Tomography. Medicina (Kaunas) 2022;58(6):702–702. doi: 10.3390/medicina58060702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vlăduțu D, Popescu SM, Mercuț R, Ionescu M, Scrieciu M, Glodeanu AD, Stănuși A, Rîcă AM, Mercuț V. Associations between Bruxism, Stress, and Manifestations of Temporomandibular Disorder in Young Students. Int J Environ Res Public Health. 2022;19(9):5415–5415. doi: 10.3390/ijerph19095415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jankulovski P, Bundevska J, Velevska M, Fiser V. Occlusal Analysis Of Parameters In Subjects With Partial Edentulism Kennedy Class I. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 2023;22(11):13–17. [Google Scholar]
- 8.Li F, Diao Y, Wang J, Hou X, Qiao S, Kong J, Sun Y, Lee ES, Jiang HB. Review of Cracked Tooth Syndrome: Etiology, Diagnosis, Management, and Prevention. Pain Res Manag. 2021;1:1–1. doi: 10.1155/2021/3788660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ellis SGS, McCord JF, Burke FJT. Predisposing and Contributing Factors for Complete and Incomplete Tooth Fractures. Dent Update. 1999;26:150–158. doi: 10.12968/denu.1999.26.4.150. [DOI] [PubMed] [Google Scholar]
- 10.Bhanderi S. Facts About Cracks in Teeth. Prim Dent J. 2021;10(1):20–27. doi: 10.1177/2050168420980987. [DOI] [PubMed] [Google Scholar]
- 11.Yap RC, Alghanem M, Martin N. A narrative review of cracks in teeth: Aetiology, microstructure and diagnostic challenges. J Dent. 2023;138:104683–104683. doi: 10.1016/j.jdent.2023.104683. [DOI] [PubMed] [Google Scholar]
- 12.Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. 2008 Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/07/crackedteethecfe_onlineversion.pdf .
- 13.Cracked Teeth and Vertical Root Fractures: A New Look at a Growing Problem . 2022 Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2022/12/ecfe-2022-edition-FINAL.pdf.
- 14.Glossary of Endodontic . 2020 Available from: https://www.aae.org/specialty/download/glossary-of-endodontic-terms/ .
- 15.McClanahan SB, Crepps JT, Maranga MC, Worrell DE, Behnia A. Special Committee to Revise the Glossary (2020). American Association of Endodontists (2020) Glossary of endodontic terms Tenth Edition. 2020 Available from: https://www.aae.org/specialty/clinical-resources/glossary-endodontic-terms/
- 16.Roh BD, Lee YE. Analysis of 154 cases of teeth with cracks. Dent Traumatol. 2006;22(3):118–123. doi: 10.1111/j.1600-9657.2006.00347.x. [DOI] [PubMed] [Google Scholar]
- 17.Popescu SM, Diaconu OA, Scrieciu M, Marinescu IR, Drăghici EC, Truşcă AG, Bănică AC, Vătu M, MercuŢ V. Root fractures: epidemiological, clinical, and radiographic aspects. Rom J Morphol Embryol. 2017;58(2):501–506. [PubMed] [Google Scholar]
- 18.Petcu CM, Niţoi D, Mercuţ V, Tuculină MJ, Iliescu AA, Croitoru CI, Diaconu OA, Iliescu MG, Gheorghiţă LM, Iliescu A. Masticatory tensile developed in upper anterior teeth with chronic apical periodontitis. A finite-element analysis study. Rom J Morphol Embryol. 2013;54(3):587–592. [PubMed] [Google Scholar]
- 19.Yahyazadehfar M, Ivancik J, Majd H, An B, Zhang D, Arola D. On the Mechanics of Fatigue and Fracture in Teeth. Appl Mech Rev. 2014;66(3):0308031–3080319. doi: 10.1115/1.4027431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yang S-F, Chen Y-W, Tsai C-L, Cheng H-C, Wu S-L, Tamse A, Ho Y-C. Incidence and contributing factors of non-root canal treated teeth with chronic fatigue root fracture: A cross-sectional study. Journal of the Formosan Medical Association. 2023;122(12):1338–1344. doi: 10.1016/j.jfma.2023.06.002. [DOI] [PubMed] [Google Scholar]
- 21.Patel S, Bhuva B, Bose R. Present status and future directions: vertical root fractures in root filled teeth. Int Endod J. 2022;55 Suppl 3(Suppl 3):804–826. doi: 10.1111/iej.13737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sugaya T, Nakatsuka M, Inoue K, Tanaka S, Miyaji H, Sakagami R, Kawamami M. Comparison of fracture sites and post lengths in longitudinal root fractures. J Endod. 2015;41(2):159–63. doi: 10.1016/j.joen.2014.09.017. [DOI] [PubMed] [Google Scholar]
- 23.von Arx, Bosshardt D. Vertical root fractures of endodontically treated posterior teeth: A histologic analysis with clinical and radiographic correlates. Swiss Dent J. 2017;127(1):14–23. doi: 10.61872/sdj-2017-01-233. [DOI] [PubMed] [Google Scholar]
- 24.Yoshino K, Ito K, Kuroda M, Sugihara N. Prevalence of vertical root fracture as the reason for tooth extraction in dental clinics. Clin Oral Investig. 2015;19(6):1405–1409. doi: 10.1007/s00784-014-1357-4. [DOI] [PubMed] [Google Scholar]
- 25.Nosrat A, Yu P, Dianat O, Verma P, Taheri S, Wu D, Fouad AF. Endodontic Specialists' Practice During the Coronavirus Disease 2019 Pandemic: 1 Year after the Initial Outbreak. J Endod. 2022;48(6):699–706. doi: 10.1016/j.joen.2022.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.HPI Poll ADA . 2021 Available from: https://adanews.ada.org/ada-news/2021/march/hpi-poll-dentists-see-increased-prevalence-of-stress-related-oral-health-conditions/
- 27.Military Ordinance no. 2/2020 for preventive measures for COVID-19 spreading. 2020 Available from: https://gov.ro/fisiere/pagini_fisiere/ORDONAN%C5%A2%C4%82_MILITAR%C4%82_nr.2-2020_privind_m%C4%83suri_de_prevenire_a_r%C4%83sp%C3%A2ndirii_COVID-19.pdf .
- 28.Nosrat A, Yu P, Verma P, Dianat O, Wu D, Fouad AF. Was the Coronavirus Disease 2019 Pandemic Associated with an Increased Rate of Cracked Teeth. J Endod. 2022;48(10):1241–1247. doi: 10.1016/j.joen.2022.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ek B, Zweig S, Roges RG, Berdan Y, Roges RA, Abulhamael A, Kutbi A, Alqutub AW, Alothmani OS, Siddiqui AY. Prevalence of Vertical Root Fractures in a University Endodontics Program versus a Private Endodontics Office. Int J Dent. 2023;1:1–1. doi: 10.1155/2023/2098629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Espinosa TA. Incidence of vertical dental fractures reported in Chihuahua City and its relationship with the evolution of the COVID-19 pandemic. Rev ADM. 2022;79(3):136–145. [Google Scholar]
- 31.Mamoun JS, Napoletano D. Cracked tooth diagnosis and treatment: An alternative paradigm. Eur J Dent. 2015;9(2):293–303. doi: 10.4103/1305-7456.156840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):31–34. doi: 10.4103/sja.SJA_543_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Guidelines for the methodology of cracked tooth studies. 2016 Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/06/crackedtoothstudiesguidelines.pdf.
- 34.Nocini R, Lippi G, Mattiuzzi C. Increased burden of cracked teeth in US and UK during the COVID-19 pandemic: Evidence from an infodemiological analysis. J Dent Sci. 2023;18(3):1398–1399. doi: 10.1016/j.jds.2023.01.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Nikolić M, Mitić A, Petrović J, Dimitrijević D, Popović J, Barac R, Todorović A. COVID-19: Another Cause of Dental Anxiety. Med Sci Monit. 2022;28:e936535–e936535. doi: 10.12659/MSM.936535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Liao WC, Chen CH, Pan YH, Chang MC, Jeng JH. Vertical Root Fracture in Non-Endodontically and Endodontically Treated Teeth: Current Understanding and Future Challenge. J Pers Med. 2021;11(12):1375–1375. doi: 10.3390/jpm11121375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Chan CP, Lin CP, Tseng SC, Jeng JH. Vertical root fracture in endodontically versus nonendodontically treated teeth: A survey of 315 cases in Chinese patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 1999;87:504–507. doi: 10.1016/s1079-2104(99)70252-0. [DOI] [PubMed] [Google Scholar]
- 38.Yeh CJ. Fatigue root fracture: A spontaneous root fracture in non-endodontically treated teeth. Br Dent. J. 1997;182:261–266. doi: 10.1038/sj.bdj.4809363. [DOI] [PubMed] [Google Scholar]
- 39.Lee K, Ahlowalia M, Alfayate RP, Patel S, Foschi F. Prevalence of and Factors Associated With Vertical Root Fracture in a Japanese Population: An Observational Study on Teeth With Isolated Periodontal Probing Depth. J Endod. 2023;49(12):1617–1624. doi: 10.1016/j.joen.2023.08.018. [DOI] [PubMed] [Google Scholar]
- 40.Stănuşi A, Mercuţ V, Scrieciu M, Popescu SM, Iacov CrăiţoiuMM, DăguciL undefined, Castravete S, Amărăscu MO. Analysis of stress generated in the enamel of an upper first premolar: a finite element study. Stomatology Edu Journal. 2020;7(1):28–34. [Google Scholar]
- 41.Stănuşi A, Mercuţ V, Scrieciu M, Popescu SM, Iacov Crăiţoiu, Dăguci L, Castravete S, Vintila DD, Vătu M. Effects of occlusal loads in the genesis of non-carious cervical lesions-a finite element study. Romanian Journal of Oral Rehabilitation. 2019;11(1):73–81. [Google Scholar]
- 42.Vatu M, Vintilă D, Popa DL, MercuţV undefined, Popescu SM, Vintila G. Determining Mechanical Causes that Produce Dental Wear Using Finite Element Method. Applied Mechanics and Materials. 2020;896:15–22. [Google Scholar]
- 43.Murariu A, Hanganu C, Bobu L, Vasluianu R, GelețuG undefined, Baciu R, Stafie CS, Forna NC. Comparative study of oral health systems in Europe. Romanian Journal of Oral Rehabilitation. 2020;12(4):11–17. [Google Scholar]
- 44.Oancea R, Amariei C, Eaton KA, Widström E. The healthcare system and the provision of oral healthcare in European Union member states: Part 5: Romania. Br Dent J. 2016;220(7):361–366. doi: 10.1038/sj.bdj.2016.265. [DOI] [PubMed] [Google Scholar]
- 45.Jiang J, Sun J, Ma H, Wang J, Huang Z, Zhou S. Stress intensity factor of a cracked molar restored with different materials and designs: A 3D-FEA. J Mech Behav Biomed Mater. 2023;142:105818–105818. doi: 10.1016/j.jmbbm.2023.105818. [DOI] [PubMed] [Google Scholar]
- 46.Göktürk H, Karaarslan EŞ, Tekin E, Hologlu B, Sarıkaya I. The effect of the different restorations on fracture resistance of root-filled premolars. BMC Oral Health. 2018;29;18(1):196–196. doi: 10.1186/s12903-018-0663-7. [DOI] [PMC free article] [PubMed] [Google Scholar]