

Abstract
Background
Suicide is a critical global public health issue that demands a better understanding of its complex causes and effective interventions. This study examines data from the Hangzhou Mental Health Hotline (2014-2023) to explore the relationship between consultation themes and suicidal ideation, with an emphasis on gender differences and how these associations changed during different phases of the COVID-19 pandemic.
Methods
This retrospective analysis covers 128,245 calls to the hotline over a decade. Chi-square tests identified differences in suicidal ideation across consultation themes and demographics. Multivariate logistic regression models were used to examine the relationship between specific themes and suicidal ideation, adjusting for confounders. The analysis was stratified by gender and pandemic phases to assess the interaction between gender and pandemic-related changes.
Results
The incidence of suicidal ideation was highest during the mid-pandemic phase (11.95%), compared to the pre-pandemic (7.68%) and post-pandemic phases (10.66%). Additionally, the rate was slightly higher among female callers (9.8%) than male callers (9.4%). Physical illness (OR = 4.70, 95% CI: 3.71-5.91) had the strongest association with suicidal ideation, followed by mental health issues (OR = 3.35, 95% CI: 3.03-3.70). Compared to male callers, female callers were more significantly affected by physical illness (OR = 6.86 vs. OR = 3.71, p < 0.001) and mental health issues (OR = 6.81 vs. OR = 2.11, p < 0.001). In the context of romantic relationship problems, female callers had a higher likelihood of suicidal ideation (OR = 4.13 vs. OR = 1.88, p < 0.001). Similarly, marital and family issues were more strongly associated with suicidal ideation in female callers (OR = 4.58 vs. OR = 1.21, p < 0.001). During the global COVID-19 pandemic, the association between suicidal ideation and consultation themes among male callers showed a sharp upward trend, which eased after the pandemic. In contrast, the association among female callers gradually accumulated and continued to worsen in the later stages of the pandemic.
Conclusion
This study highlights the necessity of implementing gender-sensitive mental health interventions tailored to different gender groups during and after global crises such as the COVID-19 pandemic, to safeguard public mental health effectively.
Keywords: Suicidal ideation, Mental health hotline, Gender differences, COVID-19
Introduction
Suicide is a complex and multifactorial global public health issue. According to the World Health Organization, approximately 700,000 people die by suicide each year, making it the second leading cause of death among individuals aged 15 to 29 globally [1]. In China, there are about 100,000 suicide deaths per year [2]. Suicidal behavior not only brings immense pain and loss to individuals and their families but also imposes a heavy burden on society and healthcare systems. Globally, the economic losses resulting from suicide are estimated to amount to hundreds of billions of dollars annually. In the United States, the economic cost of suicide and suicide attempts was estimated at 93.3 billion dollars in 2013 [3], and in Australia, the economic cost of suicide was approximately 1.7 billion dollars in 2014 [4]. Therefore, suicide prevention has become a top priority in global public health.
Mental health hotlines are an important means of crisis intervention, providing immediate support and assistance to individuals at risk of suicide and reducing the likelihood of its occurrence [5]. Research has shown that hotline services play a significant role in identifying suicidal ideation, offering emotional support, and guiding professional interventions [6]. For example, a study on the U.S. National Suicide Prevention Lifeline found that 46.5% of callers with suicidal tendencies reported a reduction in suicidal ideation by the end of the call, and 43.1% experienced relief from psychological distress [7]. Suicidal ideation is considered one of the strongest predictors of future suicide attempts and is closely associated with various psychological and social factors [8]. Therefore, timely identification and intervention of callers’ suicidal ideation are crucial for preventing suicidal behavior. However, there is still a lack of systematic research on the relationships among caller characteristics, consultation themes, and suicidal ideation in hotline services, especially regarding dynamic changes across different genders and time periods.
Since the onset of the COVID-19 pandemic, mental health issues have significantly increased worldwide. Factors such as social isolation, economic pressure, and health anxiety resulting from the pandemic have led to a rise in anxiety, depression, and suicidal ideation [9, 10]. According to a World Health Organization report, the global prevalence of anxiety and depression increased by more than 25% during the COVID-19 pandemic [11]. In China, a study involving 52,730 participants found that 35% of respondents reported psychological distress [12]. Against this backdrop, the role of mental health hotlines has become increasingly prominent.In Shanghai, mental health hotlines experienced a 79% increase in call volume during the lockdown period [13], with calls primarily concerning issues such as anxiety, fear, and suicidal ideation [14, 15]. Additionally, mental health hotlines in other countries reported similar trends, with callers mainly concerned about pandemic-related psychological stress and suicide risk [16, 17]. Multiple studies have found that the deterioration of mental health during the pandemic may persist into the post-pandemic period, potentially leading to long-term public health challenges [18, 19]. However, research on the long-term impact of the COVID-19 pandemic on suicidal ideation at different stages, as well as the dynamic changes in related risk factors, remains limited.
Previous studies have indicated that factors such as physical illness, mental health issues, and family relationships are significantly associated with suicidal ideation. For example, the risk of suicidal ideation significantly increases in patients with chronic diseases due to the dual pressures of physical and psychological stress [20, 21]. Family conflicts and lack of social support are considered important predictors of suicide risk [22, 23]; Furthermore, gender differences play a crucial role in the incidence and manifestation of suicidal behaviors. Globally, male suicide mortality rates are usually 2 to 4 times higher than those of females [1], while females report higher rates of suicidal ideation and suicide attempts [24]. However, the changes in these associations during different stages of the COVID-19 pandemic have not been fully studied.
This study aims to fill existing research gaps by conducting a retrospective analysis of 128,245 call records from the Hangzhou Mental Health Hotline between 2014 and 2023. We will investigate the association between different consultation themes (such as physical illnesses, mental health issues, marriage and family problems) and suicidal ideation, with particular attention to how this association varies across different gender groups. For the first time, the study segments the hotline data into three chronological stages: pre-pandemic (before the COVID-19 pandemic), mid-pandemic (during the COVID-19 pandemic), and post-pandemic (after the pandemic has subsided), to explore the dynamic changes in these associations over time. The anticipated findings will provide new insights for mental health intervention strategies during and after the COVID-19 pandemic, assisting policymakers and mental health service agencies in optimizing hotline services, formulating more targeted prevention and intervention measures, enhancing the ability to identify and support high-risk individuals, and thereby effectively addressing future public health challenges.
Methods
Study design and participants
This study employs a cross-sectional design to investigate the relationship between the consultation themes of callers to the Hangzhou Mental Health Hotline and their suicidal ideation. Established by the Hangzhou Mental Health Center in 1995, this hotline is one of China’s earliest 24/7 mental health support channels. It operates with a team consisting of 3 full-time employees and 44 volunteers who take turns on duty to ensure continuous service. The call operators include psychiatrists, registered nurses, and professionals with national level two psychological consultants’ qualifications, all holding at least a bachelor’s degree. To ensure service quality and professionalism, all operators undergo specialized training and supervision related to the hotline’s operations before they start work, which is carried out by senior experts from the Seventh People’s Hospital of Hangzhou. This study focuses on calls made to the Hangzhou Mental Health Hotline from January 1, 2014, to December 31, 2023. The initial dataset comprises 130,167 call records. Exclusion Criteria: 1) Incomplete call records: Calls lacking crucial variables such as gender, consultation themes, or suicidal ideation. 2) Invalid calls: Silent calls, harassment, and repeated calls where multiple calls were made by the same individual on the same day, the earliest call is included for analysis. 3) Calls lasting less than one minute, as they may not provide sufficient information for meaningful assessment. Based on these criteria, the final analysis included 128,245 calls. The screening process is illustrated in Fig. 1.
Fig. 1.
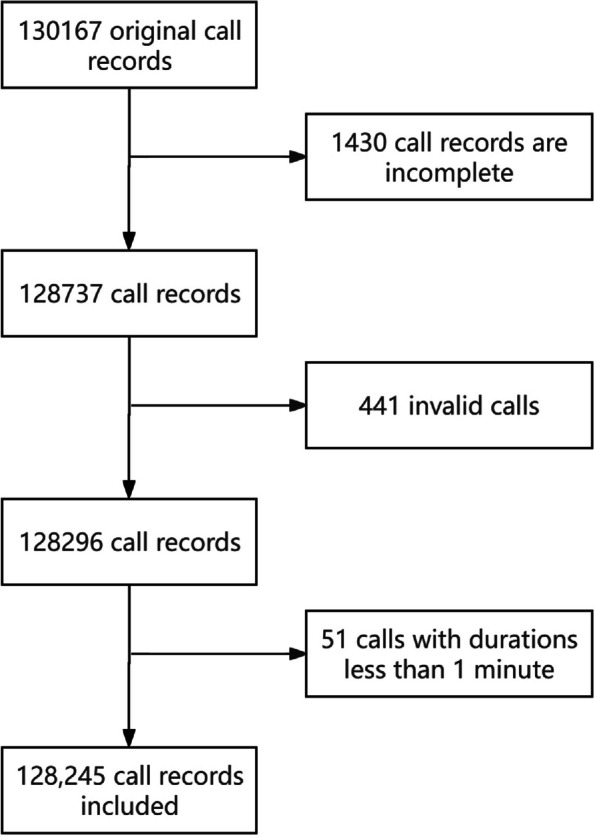
Flowchart of call records selection process
Data collection
During the consultation process, demographic information including gender, age, marital status, educational background, and occupational identity was collected. Additionally, call detail records encompassed the call time, duration of the conversation, caller’s region, date, and quarter. Suicide behavior and related factors were self-reported by the callers. Depression was assessed using a structured questionnaire [25] based on DSM-IV criteria for a major depressive episode. The tool, widely used in hotline settings, showed excellent inter-rater reliability (ICC = 1.00), test-retest reliability (ICC = 0.91), and strong consistency with the Structured Clinical Interview for DSM-IV (Kappa = 0.87) [26]. The evaluation of suicidal ideation was based on self-reports of self-harm or suicidal ideation within the two weeks prior to the call [27]. Further determination of past suicidal intent was made by asking the caller if they had ever attempted suicide [7, 28]. Main topics discussed during calls were categorized into ten consultation themes: physical illness, mental health issues, romantic relationship issues, marital and family issues, sexual issues, parenting and child education, work-related issues, interpersonal relationship issues, Learning issues, and Other issues. If multiple themes were discussed in one call, the theme with the longest discussion time or deepest exploration was selected as the consultation theme for subsequent recording and analysis. To assess the variation in the association between consultation themes and suicidal ideation during the COVID-19 pandemic, call dates were divided into three phases: pre-pandemic (January 1, 2014, to January 22, 2020), mid-pandemic (January 23, 2020, to January 8, 2023), and post-pandemic (January 9, 2023, to December 31, 2023). These phases were defined by key milestones: the implementation of Wuhan’s lockdown on January 23, 2020, marking the start of strict epidemic control, and the lifting of quarantine regulations for international travelers on January 8, 2023, indicating a transition to normalized pandemic management [29].
Statistical analysis
Data analysis was conducted using the R software (version 4.3.1; R Core Team, 2023). Continuous variables such as age, call duration, and depression level were transformed into categorical variables based on their clinical relevance and data distribution characteristics to ensure model compatibility and interoperability among data. Chi-square tests were employed to assess the differences in suicidal ideation across demographic features and associated clinical variables. A multivariate logistic regression analysis was performed to explore the relationship between suicidal ideation and consultation themes, with “other issues” as the reference category due to its lower relevance to other main problem categories and suicidal ideation. Covariates were incrementally adjusted in the model construction to establish independent associations. The analysis was stratified by gender to compare the association between consultation themes and suicidal ideation in males and females. Additionally, the data were stratified by pandemic phases (pre-pandemic, mid-pandemic, and post-pandemic) to assess how these associations varied across phases. Z-tests were applied to compare the odds ratios (OR) of each counseling topic associated with suicidal ideation within different pandemic stages, and statistical significance was determined by a two-tailed p-value less than 0.05.
Results
Demographic and call characteristics & prevalence of suicidal ideation
Tables 1 and 2 summarize the demographic information and call characteristics of 128,245 callers to Hangzhou’s mental health hotline, exploring the association between these features and suicidal ideation. The data reveals that males constitute 45.9% (n = 58,878) of all callers, while females make up 54.1% (n = 69,367). In terms of gender, 9.4% (n = 5,511) of males and 9.8% (n = 6,774) of females reported suicidal ideation, with this difference reaching statistical significance (P = 0.014). Age distribution shows that the highest proportion is in the 20-29 age group (26.7%, n = 34,183), followed by 30-39 (18.4%, n = 23,598), where the 20-29 and 10-19 age groups have significantly higher numbers reporting suicidal ideation (P < 0.001). Among those who called, 46.7% (n = 59,913) were single, with this group having the highest rate of suicidal ideation at 14.3% (n = 8,594), which was also statistically significant (P < 0.001). In terms of education background, 28.3% (n = 36,306) of callers had a bachelor’s degree or above, indicating higher risk for suicidal ideation in those with lower educational attainment (P < 0.001). In the occupational distribution, the white-collar class accounted for 40.2% (n = 51,527), with 13.5% (n = 6,963) expressing suicidal ideation, while the highest proportion of unemployed callers (20.9%, n = 2,569) showed a significant phenomenon (P < 0.001). Analysis of call times indicates that calls were evenly distributed throughout the day and night (48.8% vs. 51.2%, n = 62,593 vs. n = 65,652, p = 0.074). Regarding call duration, over 62.4% (n = 80,045) of calls lasted between 1-15 minutes, with a higher rate of suicidal ideation observed as call duration increased (p < 0.001). Geographically, 35.2% (n = 45,161) of calls originated from Hangzhou, where the suicidal ideation rate was 5.7%. Callers from Zhejiang province had a suicidal ideation rate of 10.3% (n = 3,322), while callers from other provinces had the highest rate of 12.5% (n = 6,389), with statistically significant differences (p < 0.001). Most calls (87.3%, n = 112,018) were made for personal needs, with those calling for their own needs showing more pronounced signs of suicidal ideation compared to those calling for others (P < 0.001). In terms of emotional state, 95.4% (n = 122,329) of callers reported normal emotions, but moderate to severe depression was closely linked to suicidal ideation (P < 0.001). Concerning suicide behavior, 96.9% (n = 124,252) of callers had no record of suicide attempts, with a significantly higher risk of suicidal ideation among those who had attempted suicide (P < 0.001).The analysis during the pandemic reveals that the rate of suicidal ideation was highest during the mid-pandemic phase (11.95%, n = 5,421), compared to the pre-pandemic (7.68%, n = 5,093) and post-pandemic phases (10.66%, n = 1,771), with statistically significant differences (p < 0.001).Among the consultation themes, mental health issues were the most prevalent (45.1 %, n = 57,872), followed by relationship problems in romantic partnerships (6.5 %, n = 8,312) and marriage and family issues (9.0 %, n = 11,593). Notably, there is a particularly strong association between mental health issues and suicidal ideation (P < 0.001).
Table 1.
Demographic and call characteristics of callers to the Hangzhou Mental Health Hotline(Part 1)
| Suicidal ideation | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 128,2451 | Absent, N = 115,9601 | Present, N = 12,2851 | P value2 |
| Sex | 0.014 | |||
| Male | 58878 (45.9%) | 53367 (46.0%) | 5511 (44.9%) | |
| Female | 69367 (54.1%) | 62593 (54.0%) | 6774 (55.1%) | |
| Age | <0.001 | |||
| 10-19 | 13497 (10.5%) | 10370 (8.9%) | 3127 (25.5%) | |
| 20-29 | 34183 (26.7%) | 29063 (25.1%) | 5120 (41.7%) | |
| 30-39 | 23598 (18.4%) | 21633 (18.7%) | 1965 (16.0%) | |
| 40-49 | 12637 (9.9%) | 12052 (10.4%) | 585 (4.8%) | |
| 50-59 | 3888 (3.0%) | 3726 (3.2%) | 162 (1.3%) | |
| >60 | 742 (0.6%) | 715 (0.6%) | 27 (0.2%) | |
| Unknown | 39700 (31.0%) | 38401 (33.1%) | 1299 (10.6%) | |
| Marital Status | <0.001 | |||
| Single | 59913 (46.7%) | 51319 (44.3%) | 8594 (70.0%) | |
| Married | 24639 (19.2%) | 22669 (19.5%) | 1970 (16.0%) | |
| Divorced or widowed | 8337 (6.5%) | 7754 (6.7%) | 583 (4.7%) | |
| Unknown | 35356 (27.6%) | 34218 (29.5%) | 1138 (9.3%) | |
| Educational Background | <0.001 | |||
| Junior high school or below | 14664 (11.4%) | 12535 (10.8%) | 2129 (17.3%) | |
| High school and secondary school | 21708 (16.9%) | 18861 (16.3%) | 2847 (23.2%) | |
| Undergraduate degree or college | 36306 (28.3%) | 31954 (27.6%) | 4352 (35.4%) | |
| Master’s or PhD degree | 4082 (3.2%) | 3686 (3.2%) | 396 (3.2%) | |
| Unknown | 51485 (40.1%) | 48924 (42.2%) | 2561 (20.8%) | |
| Occupation | <0.001 | |||
| White-collar | 51527 (40.2%) | 44564 (38.4%) | 6963 (56.7%) | |
| Blue-collar | 10521 (8.2%) | 9505 (8.2%) | 1016 (8.3%) | |
| Unemployment | 20037 (15.6%) | 17468 (15.1%) | 2569 (20.9%) | |
| Retirement | 1851 (1.4%) | 1790 (1.5%) | 61 (0.5%) | |
| Unknown | 44309 (34.6%) | 42633 (36.8%) | 1676 (13.6%) | |
| Call Time | 0.074 | |||
| Daytime | 62593 (48.8%) | 56503 (48.7%) | 6090 (49.6%) | |
| Overnight | 65652 (51.2%) | 59457 (51.3%) | 6195 (50.4%) | |
| Duration (min) | <0.001 | |||
| 1-15 minutes | 80045 (62.4%) | 75908 (65.5%) | 4137 (33.7%) | |
| 16-30 minutes | 27713 (21.6%) | 23777 (20.5%) | 3936 (32.0%) | |
| 31-45 minutes | 12031 (9.4%) | 9818 (8.5%) | 2213 (18.0%) | |
| 46-60 minutes | 5242 (4.1%) | 4143 (3.6%) | 1099 (8.9%) | |
| >60 minutes | 3214 (2.5%) | 2314 (2.0%) | 900 (7.3%) | |
| Quarter | <0.001 | |||
| Q1 | 29928 (23.3%) | 27158 (23.4%) | 2770 (22.5%) | |
| Q2 | 32366 (25.2%) | 29405 (25.4%) | 2961 (24.1%) | |
| Q3 | 34503 (26.9%) | 31013 (26.7%) | 3490 (28.4%) | |
| Q4 | 31448 (24.5%) | 28384 (24.5%) | 3064 (24.9%) | |
| Region | <0.001 | |||
| Hangzhou | 45161 (35.2%) | 42587 (36.7%) | 2574 (21.0%) | |
| Zhejiang province | 32102 (25.0%) | 28780 (24.8%) | 3322 (27.0%) | |
| Other province | 50982 (39.8%) | 44593 (38.5%) | 6389 (52.0%) | |
| Caller | <0.001 | |||
| Calls for oneself | 112018 (87.3%) | 100351 (86.5%) | 11667 (95.0%) | |
| Calls for others | 16227 (12.7%) | 15609 (13.5%) | 618 (5.0%) | |
1n (%); Mean (IQR)
2Pearson’s Chi-squared test
Table 2.
Demographic and call characteristics of callers to the Hangzhou Mental Health Hotline(Part 2)
| Suicidal ideation | ||||
|---|---|---|---|---|
| Characteristic | Overall, N = 128,2451 | Absent, N = 115,9601 | Present, N = 12,2851 | P value2 |
| Mood Status | <0.001 | |||
| Normal | 122329 (95.4%) | 114653 (98.9%) | 7676 (62.5%) | |
| Mild depression | 1281 (1.0%) | 685 (0.6%) | 596 (4.9%) | |
| Moderate depression | 1915 (1.5%) | 384 (0.3%) | 1531 (12.5%) | |
| Severe depression | 2720 (2.1%) | 238 (0.2%) | 2482 (20.2%) | |
| Suicide Behavior | <0.001 | |||
| No | 124252 (96.9%) | 115407 (99.5%) | 8845 (72.0%) | |
| Used to be | 3435 (2.7%) | 531 (0.5%) | 2904 (23.6%) | |
| Preparing | 558 (0.4%) | 22 (0.0%) | 536 (4.4%) | |
| Pandemic phase | <0.001 | |||
| Pre-pandemic | 66,276 (51.7%) | 61,183 (52.8%) | 5,093 (41.5%) | |
| Mid-pandemic | 45,360 (35.4%) | 39,939 (34.4%) | 5,421 (44.1%) | |
| Post-pandemic | 16,609 (13.0%) | 14,838 (12.8%) | 1,771 (14.4%) | |
| Consultation Themes | <0.001 | |||
| Physical illness | 943 (0.7%) | 784 (0.7%) | 159 (1.3%) | |
| Mental health issues | 57872 (45.1%) | 49334 (42.5%) | 8538 (69.5%) | |
| Romantic relationship issues | 8312 (6.5%) | 7205 (6.2%) | 1107 (9.0%) | |
| Marital and family issues | 11593 (9.0%) | 10456 (9.0%) | 1137 (9.3%) | |
| Sexual issues | 2435 (1.9%) | 2420 (2.1%) | 15 (0.1%) | |
| Parenting and child education | 2853 (2.2%) | 2809 (2.4%) | 44 (0.4%) | |
| Work-related issues | 3708 (2.9%) | 3477 (3.0%) | 231 (1.9%) | |
| Interpersonal relationship issues | 4892 (3.8%) | 4753 (4.1%) | 139 (1.1%) | |
| Learning issues | 2127 (1.7%) | 1942 (1.7%) | 185 (1.5%) | |
| Other issues | 33510 (26.1%) | 32780 (28.3%) | 730 (5.9%) | |
1n (%); Mean (IQR)
2Pearson’s Chi-squared test
Overall analysis of the association between consultation themes and suicidal ideation
Table 3 presents the results of logistic regression analyses examining the association between consultation themes and suicidal ideation, with “Other issues” as the reference category. The analysis includes multiple models, progressively adjusting for key covariates: Model 1 is unadjusted, providing the raw association between consultation themes and suicidal ideation; Model 2 adjusts for demographic factors, including sex, age, marital status, educational background, and occupation; Model 3 further includes call-related variables such as call duration, region, quarter, call time, as well as clinical factors like mood status and suicide behavior;Model 4 includes adjustments for the pandemic phase, accounting for the potential variation in the association between consultation themes and suicidal ideation during different phases of the COVID-19 pandemic.
Table 3.
Logistic regression analysis of the association between consultation themes and suicidal ideation across multiple models
| Model 11 | Model 22 | Model 33 | Model 44 | |||||
|---|---|---|---|---|---|---|---|---|
| Consultation themes | OR | 95% CI5 | OR | 95% CI5 | OR | 95% CI5 | OR | 95% CI5 |
| Other issues (Reference) | ||||||||
| Physical illness | 9.11 | [7.54, 10.9] | 5.86 | [4.82, 7.09] | 4.83 | [3.82, 6.07] | 4.70 | [3.71, 5.91] |
| Mental health issues | 7.77 | [7.20, 8.40] | 4.27 | [3.93, 4.65] | 3.39 | [3.07, 3.74] | 3.35 | [3.03, 3.70] |
| Romantic relationship issues | 6.90 | [6.26, 7.60] | 3.34 | [3.01, 3.71] | 2.42 | [2.13, 2.74] | 2.43 | [2.14, 2.76] |
| Marital and family issues | 4.88 | [4.44, 5.37] | 2.63 | [2.37, 2.92] | 2.11 | [1.87, 2.39] | 2.15 | [1.90, 2.43] |
| Sexual issues | 0.28 | [0.16, 0.45] | 0.12 | [0.07, 0.20] | 0.15 | [0.08, 0.26] | 0.20 | [0.11, 0.33] |
| Parenting and child education | 0.70 | [0.51, 0.94] | 0.59 | [0.42, 0.79] | 0.71 | [0.51, 0.97] | 0.65 | [0.46, 0.89] |
| Work-related issues | 2.98 | [2.56, 3.47] | 1.69 | [1.44, 1.98] | 1.57 | [1.30, 1.88] | 1.56 | [1.29, 1.87] |
| Interpersonal relationship issues | 1.31 | [1.09, 1.57] | 0.63 | [0.52, 0.76] | 0.65 | [0.52, 0.80] | 0.68 | [0.54, 0.83] |
| Learning issues | 4.28 | [3.61, 5.05] | 1.35 | [1.13, 1.60] | 1.35 | [1.10, 1.66] | 1.36 | [1.10, 1.67] |
1Unadjusted model
2Adjusted for Sex,Age,Marital status,Educational background,Occupation
3Adjusted for Sex,Age,Marital status,Educational background,Occupation,Duration (min),Region, Caller,Quarter,Call time,Mood status,Suicide behavior
4Adjusted for Sex,Age,Marital status,Educational background,Occupation,Duration (min), Region, Caller,Quarter,Call time,Mood status,Suicide behavior,Pandemic phase
5OR Odds Ratio, CI Confidence Interval, bold figures are statistically significant (P < 0.05)
Physical illness consistently showed the strongest association with suicidal ideation across all models. In the unadjusted model (Model 1), the odds ratio (OR) was 9.11 (95% CI: 7.54, 10.9), which decreased to 4.70 (95% CI: 3.71, 5.91) in the fully adjusted model (Model 4). This reduction suggests that, even after accounting for other factors, physical illness remains strongly associated with suicidal ideation. Mental health issues also showed a strong association with suicidal ideation, with an OR of 7.77 (95% CI: 7.20, 8.40) in Model 1, decreasing to 3.35 (95% CI: 3.03, 3.70) after full adjustment in Model 4. The attenuation in ORs after adjusting for covariates suggests that while demographic and clinical factors contribute to this association, mental health issues remain an important factor related to suicidal ideation.
Romantic relationship issues were significantly linked to suicidal ideation, with an OR of 6.90 (95% CI: 6.26, 7.60) in the unadjusted model, which reduced to 2.43 (95% CI: 2.14, 2.76) in Model 4. The decrease across models suggests that the association is moderated by other factors, such as the individual’s emotional state and the context of the call. Marital and family issues had an initial OR of 4.88 (95% CI: 4.44, 5.37) in Model 1, which decreased to 2.15 (95% CI: 1.90, 2.43) in Model 4. This finding suggests that while marital and family issues are relevant, their association with suicidal ideation is influenced by various other factors, including socio-demographic and situational variables.
Sexual issues showed a relatively weak and protective association with suicidal ideation, with the OR reducing from 0.28 (95% CI: 0.16, 0.45) in Model 1 to 0.20 (95% CI: 0.11, 0.33) in Model 4. This pattern suggests that discussing sexual issues might be associated with lower risk, potentially reflecting differences in the type of distress leading to suicidal ideation. Parenting and child education also demonstrated a protective effect, with the OR reducing from 0.70 (95% CI: 0.51, 0.94) in the unadjusted model to 0.65 (95% CI: 0.46, 0.89) in the fully adjusted model, indicating that these concerns might buffer against suicidal ideation when controlling for other factors. Work-related issues had an initial OR of 2.98 (95% CI: 2.56, 3.47), which decreased to 1.56 (95% CI: 1.29, 1.87) after full adjustment. This suggests that the stress associated with work issues is significantly associated with suicidal ideation, though this relationship is moderated by other variables.
Interpersonal relationship issues showed a modest association with suicidal ideation, starting with an OR of 1.31 (95% CI: 1.09, 1.57) in Model 1, which decreased to 0.68 (95% CI: 0.54, 0.83) in Model 4. The reduction indicates that when other factors are considered, interpersonal issues alone are less predictive of suicidal ideation. Learning issues had a strong association with suicidal ideation in the unadjusted model (OR = 4.28, 95% CI: 3.61, 5.05), which remained significant even after full adjustment in Model 4, with an OR of 1.36 (95% CI: 1.10, 1.67). This suggests that learning-related stressors are independently linked to suicidal ideation, highlighting the need for targeted interventions.
Gender-stratified analysis
Table 4 presents a gender-stratified logistic regression analysis of the association between various consultation themes and suicidal ideation among callers to the Hangzhou Mental Health Hotline. For physical illness, the odds ratio (OR) for suicidal ideation was significantly higher in females (OR = 6.86, 95% CI: 4.58, 10.1) compared to males (OR = 3.71, 95% CI: 2.75, 4.94), with a Z-score of -2.45 and a P-value of 0.014, indicating a statistically significant gender difference. This suggests that physical illness is more strongly associated with suicidal ideation among female callers. Mental health issues showed a strong association with suicidal ideation in both genders, but the effect was more pronounced in females (OR = 6.81, 95% CI: 5.75, 8.09) than in males (OR = 2.11, 95% CI: 1.86, 2.40), with a highly significant Z-score of -10.78 (P < 0.001), highlighting that Mental health issues are a critical concern for both genders, with a stronger association observed in females. Romantic relationship issues were associated with an increased risk of suicidal ideation in both males (OR = 1.88, 95% CI: 1.59, 2.23) and females (OR = 4.13, 95% CI: 3.36, 5.07), with a Z-score of -5.79 (P < 0.001) indicating a significant gender difference, with females being more affected by these issues than males. Marital and family issues were significantly associated with suicidal ideation, with a stronger association in females (OR = 4.58, 95% CI: 3.78, 5.57) compared to males (OR = 1.21, 95% CI: 1.01, 1.46), as indicated by a Z-score of -9.76 (P < 0.001).
Table 4.
Stratified logistic regression analysis of the association between consultation themes and suicidal ideation by gender
| Male | Female | Comparison | ||||
|---|---|---|---|---|---|---|
| Consultation themes | OR1 | 95% CI1 | OR1 | 95% CI1 | Z–score | P-value |
| Other issues (Reference) | ||||||
| Physical illness | 3.71 | [2.75, 4.94] | 6.86 | [4.58, 10.1] | -2.45 | 0.014 |
| Mental health issues | 2.11 | [1.86, 2.40] | 6.81 | [5.75, 8.09] | -10.78 | <0.001 |
| Romantic relationship issues | 1.88 | [1.59, 2.23] | 4.13 | [3.36, 5.07] | -5.79 | <0.001 |
| Marital and family issues | 1.21 | [1.01, 1.46] | 4.58 | [3.78, 5.57] | -9.76 | <0.001 |
| Sexual issues | 0.16 | [0.09, 0.28] | 0.12 | [0.01, 0.94] | 0.24 | 0.809 |
| Parenting and child education | 0.27 | [0.13, 0.52] | 1.52 | [1.02, 2.21] | -4.27 | <0.001 |
| Work-related issues | 1.15 | [0.90, 1.46] | 2.56 | [1.89, 3.43] | -4.09 | <0.001 |
| Interpersonal relationship issues | 0.32 | [0.22, 0.46] | 1.54 | [1.16, 2.03] | -6.65 | <0.001 |
| Learning issues | 1.02 | [0.72, 1.41] | 2.45 | [1.84, 3.24] | -3.91 | <0.001 |
1OR Odds Ratio, CI Confidence Interval, bold figures are statistically significant (P < 0.05)
Sexual issues showed a protective effect against suicidal ideation in males (OR = 0.16, 95% CI: 0.09, 0.28), but this effect was not significant in females (OR = 0.12, 95% CI: 0.01, 0.94), with the Z-score of 0.24 (P = 0.809) indicating no significant gender difference. Parenting and child education concerns were associated with a lower likelihood of suicidal ideation, particularly among males (OR = 0.27, 95% CI: 0.10, 0.52), compared to females (OR = 1.52, 95% CI: 1.02, 2.21), with a Z-score of -4.27 (P < 0.001), indicating significant gender differences in how these issues are related to suicidal ideation. Work-related issues were found to increase the risk of suicidal ideation, more so in females (OR = 2.56, 95% CI: 1.89, 3.43), while the association was not significant in males (OR = 1.15, 95% CI: 0.90, 1.46), with a significant Z-score of -4.09 (P < 0.001). Interpersonal relationship issues had a stronger protective effect against suicidal ideation in males (OR = 0.32, 95% CI: 0.22, 0.46) compared to females (OR = 1.54, 95% CI: 1.16, 2.03), as indicated by a Z-score of -6.65 (P < 0.001).Learning issues were significantly associated with suicidal ideation in females (OR = 2.45, 95% CI: 1.84, 3.24), but not in males (OR = 1.02, 95% CI: 0.72, 1.41), with a Z-score of -3.91 (P < 0.001), indicating a significant gender difference in the association between learning issues and suicidal ideation.
Pandemic phase-stratified analysis
Association between consultation themes and suicidal ideation across different pandemic phases (male callers)
The analysis of male callers reveals notable changes in the association between various consultation themes and suicidal ideation across the three pandemic phases: pre-pandemic, mid-pandemic, and post-pandemic (Tables 5 and 6). Between the pre-pandemic and mid-pandemic phases, there was a significant intensification in the association between several consultation themes and suicidal ideation among male callers. Mental health issues saw a dramatic increase in their association with suicidal ideation, with the odds ratio (OR) rising from a non-significant 1.07 (95% CI: 0.90, 1.28) pre-pandemic to a significant 4.66 (95% CI: 3.79, 5.76) mid-pandemic, confirmed by a highly significant Z-test (Z = -10.54, P < 0.001). Romantic relationship issues became significantly associated with suicidal ideation mid-pandemic, with the OR increasing from a non-significant 1.03 (95% CI: 0.79, 1.33) pre-pandemic to 3.98 (95% CI: 3.04, 5.21) mid-pandemic (Z = -7.07, P < 0.001). Marital and family issues also showed a significant increase, with the OR rising from a significant 0.51 (95% CI: 0.39, 0.67) pre-pandemic to 2.79 (95% CI: 2.08, 3.74) mid-pandemic (Z = -8.34, P < 0.001). Work-related issues saw their OR increase from a non-significant 0.78 (95% CI: 0.54, 1.12) pre-pandemic to 1.89 (95% CI: 1.27, 2.77) mid-pandemic, with a significant change confirmed by the Z-test (Z = -3.25, P = 0.001). Interpersonal relationship issues increased significantly from a protective OR of 0.10 (95% CI: 0.05, 0.15) pre-pandemic to 0.86 (95% CI: 0.48, 1.44) mid-pandemic, with the Z-test showing a significant reduction in this protective effect (Z = -4.99, P < 0.001). Learning issues also became significantly associated with suicidal ideation mid-pandemic, with the OR rising from a protective 0.55 (95% CI: 0.31, 0.94) pre-pandemic to 1.96 (95% CI: 1.16, 3.17) mid-pandemic (Z = -3.33, P < 0.001). These results suggest that the mid-pandemic period intensified the association between these themes and suicidal ideation among male callers, as stressors related to mental health, relationships, work, and education became more pronounced.
Table 5.
Stratified logistic regression analysis of the association between consultation themes and suicidal ideation among males across different pandemic phases
| Pre-pandemic1 | Mid-pandemic1 | Post-pandemic1 | ||||
|---|---|---|---|---|---|---|
| Consultation themes | OR2 | 95% CI2 | OR2 | 95% CI2 | OR2 | 95% CI2 |
| Other issues (Reference) | – | – | – | – | – | – |
| Physical illness | 2.91 | [1.81, 4.54] | 4.67 | [2.74, 7.66] | 5.08 | [2.57, 9.79] |
| Mental health issues | 1.07 | [0.90, 1.28] | 4.66 | [3.79, 5.76] | 2.77 | [1.83, 4.28] |
| Romantic relationship issues | 1.03 | [0.79, 1.33] | 3.98 | [3.04, 5.21] | 2.46 | [1.49, 4.10] |
| Marital and family issues | 0.51 | [0.39, 0.67] | 2.79 | [2.08, 3.74] | 2.10 | [1.26, 3.55] |
| Sexual issues | 0.05 | [0.02, 0.12] | 0.55 | [0.17, 1.35] | 0.87 | [0.20, 2.62] |
| Parenting and child education | 0.08 | [0.01, 0.31] | 0.56 | [0.19, 1.31] | 0.58 | [0.29, 2.06] |
| Work-related issues | 0.78 | [0.54, 1.12] | 1.89 | [1.27, 2.77] | 1.37 | [0.70, 2.56] |
| Interpersonal relationship issues | 0.10 | [0.05, 0.15] | 0.86 | [0.48, 1.44] | 0.64 | [0.25, 1.45] |
| Learning issues | 0.55 | [0.31, 0.94] | 1.96 | [1.16, 3.17] | 1.17 | [0.47, 2.65] |
1Pre-pandemic refers to the period from January 1, 2014, to January 22, 2020; Mid-pandemic covers January 23, 2020, to January 8, 2023; Post-pandemic starts from January 9, 2023, to December 31, 2023
2OR Odds Ratio, CI Confidence Interval. Bold figures indicate statistical significance (P < 0.05)
Table 6.
Z-Test Comparison of odds ratios for consultation themes associated with suicidal ideation among males across different pandemic phases
| Pre vs Mid | Mid vs Post | Pre vs Post | ||||
|---|---|---|---|---|---|---|
| Consultation theme | Z-score1 | P-value | Z-score1 | P-value | Z-score1 | P-value |
| Physical illness | -1.34 | 0.179 | -0.20 | 0.845 | -1.35 | 0.18 |
| Mental health issues | -10.54 | <0.001 | 2.15 | 0.031 | -4.05 | <0.001 |
| Romantic relationship issues | -7.07 | <0.001 | 1.64 | 0.1 | -2.99 | 0.003 |
| Marital and family issues | -8.34 | <0.001 | 0.94 | 0.35 | -4.75 | <0.001 |
| Sexual issues | -3.58 | <0.001 | -0.54 | 0.58 | -3.69 | <0.001 |
| Parenting and child education | -1.93 | 0.053 | -0.04 | 0.97 | -1.67 | 0.09 |
| Work-related issues | -3.25 | 0.001 | 0.828 | 0.408 | -1.47 | 0.141 |
| Interpersonal relationship issues | -4.99 | <0.001 | 0.56 | 0.577 | -3.35 | <0.001 |
| Learning issues | -3.33 | <0.001 | 1.01 | 0.312 | -1.44 | 0.149 |
1Bold figures indicate statistical significance (P < 0.05)
In the transition from mid-pandemic to post-pandemic, there was a general trend of decreasing associations between certain consultation themes and suicidal ideation. Mental health issues saw their OR decrease from 4.66 (95% CI: 3.79, 5.76) mid-pandemic to 2.77 (95% CI: 1.83, 4.28) post-pandemic, with the Z-test confirming a significant decrease (Z = 2.15, P = 0.031). This indicates some recovery or adaptation as the pandemic progressed, though the risk remained elevated compared to pre-pandemic levels. Romantic relationship issues also showed a decrease in their OR from 3.98 mid-pandemic to 2.46 post-pandemic, but this change was not statistically significant. Marital and family issues saw a decrease from 2.79 mid-pandemic to 2.10 post-pandemic, with no significant change indicated by the Z-test. Learning issues decreased in significance, with the OR falling from 1.96 mid-pandemic to 1.17 post-pandemic, and the Z-test indicating no significant change. While some themes, like mental health issues, showed a significant decrease in association post-pandemic, the risk for suicidal ideation generally remained higher than pre-pandemic levels, reflecting the lingering effects of the pandemic.
When comparing the pre-pandemic and post-pandemic periods, several themes maintained a significantly higher association with suicidal ideation. Mental health issues remained significantly associated with suicidal ideation post-pandemic (OR = 2.77, 95% CI: 1.83, 4.28) compared to pre-pandemic (OR = 1.07), with a significant increase confirmed by the Z-test (Z = -4.05, P < 0.001). Romantic relationship issues also remained significantly higher post-pandemic (OR = 2.46) compared to pre-pandemic, as indicated by a significant Z-score (Z = -2.99, P = 0.003). Marital and family issues continued to be more strongly associated with suicidal ideation post-pandemic (OR = 2.10) compared to pre-pandemic levels, with a significant Z-score (Z = -4.75, P < 0.001). These findings highlight that while the immediate changes related to the pandemic may have eased post-pandemic, the association between certain themes-especially mental health and relationship issues-and suicidal ideation remained significantly stronger than in the pre-pandemic period.
Association between consultation themes and suicidal ideation across different pandemic phases (female callers)
The analysis of female callers reveals significant changes in the association between various consultation themes and suicidal ideation across the pre-pandemic, mid-pandemic, and post-pandemic phases (Tables 7 and 8). From the pre-pandemic to mid-pandemic phases, several consultation themes showed an increase in their association with suicidal ideation among female callers. Mental health issues saw an increase in the odds ratio (OR) from 5.14 (95% CI: 3.97, 6.73) pre-pandemic to 7.36 (95% CI: 5.76, 9.50) mid-pandemic, although this increase was not statistically significant (Z = -1.94, P = 0.053). Romantic relationship issues also showed a rise in OR from 3.19 (95% CI: 2.29, 4.47) pre-pandemic to 4.70 (95% CI: 3.50, 6.34) mid-pandemic, though the change was not statistically significant (Z = -1.70, P = 0.089). Marital and family issues increased in OR from 3.69 (95% CI: 2.73, 5.04) pre-pandemic to 4.80 (95% CI: 3.62, 6.41) mid-pandemic, without statistical significance (Z = -1.23, P = 0.219). Work-related issues saw the OR rise from 1.68 (95% CI: 0.97, 2.82) pre-pandemic to 3.12 (95% CI: 2.02, 4.74) mid-pandemic, nearing statistical significance (Z = -1.78, P = 0.076). Learning issues slightly decreased in OR from 2.34 (95% CI: 1.46, 3.71) pre-pandemic to 1.93 (95% CI: 1.24, 2.96) mid-pandemic, with no statistical significance (Z = 0.59, P = 0.553). Despite these increases, none of these changes reached statistical significance, indicating a trend toward stronger associations with suicidal ideation but without strong evidence.
Table 7.
Stratified logistic regression analysis of the association between consultation themes and suicidal ideation among females across different pandemic phases
| Pre-pandemic1 | Mid-pandemic1 | Post-pandemic1 | ||||
|---|---|---|---|---|---|---|
| Consultation themes | OR2 | 95% CI2 | OR2 | 95% CI2 | OR2 | 95% CI2 |
| Other issues (Reference) | – | – | – | – | – | – |
| Physical illness | 5.80 | [2.87, 11.1] | 7.12 | [3.94, 12.3] | 12.7 | [4.04, 36.1] |
| Mental health issues | 5.14 | [3.97, 6.73] | 7.36 | [5.76, 9.50] | 15.5 | [8.74, 30.1] |
| Romantic relationship issues | 3.19 | [2.29, 4.47] | 4.70 | [3.50, 6.34] | 6.88 | [3.59, 14.2] |
| Marital and family issues | 3.69 | [2.73, 5.04] | 4.80 | [3.62, 6.41] | 10.2 | [5.52, 20.6] |
| Sexual issues | 0.06 | [0.00, 1.12] | 0.33 | [0.01, 4.22] | 0.00 | [0.00, 0.00] |
| Parenting and child education | 1.33 | [0.62, 2.57] | 1.11 | [0.58, 1.97] | 5.18 | [2.14, 12.4] |
| Work-related issues | 1.68 | [0.97, 2.82] | 3.12 | [2.02, 4.74] | 4.49 | [1.98, 10.4] |
| Interpersonal relationship issues | 1.29 | [0.82, 2.00] | 1.47 | [0.94, 2.24] | 3.06 | [1.38, 6.94] |
| Learning issues | 2.34 | [1.46, 3.71] | 1.93 | [1.24, 2.96] | 5.00 | [2.22, 11.5] |
1Pre-pandemic refers to the period from January 1, 2014, to January 22, 2020; Mid-pandemic covers January 23, 2020, to January 8, 2023; Post-pandemic starts from January 9, 2023, to December 31, 2023
2OR Odds Ratio, CI Confidence Interval. Bold figures indicate statistical significance (P < 0.05)
Table 8.
Z-Test Comparison of odds ratios for consultation themes associated with suicidal ideation among females across different pandemic phases
| Consultation theme | Pre vs Mid | Mid vs Post | Pre vs Post | |||
|---|---|---|---|---|---|---|
| Z-score1 | P-value | Z-score1 | P-value | Z-score1 | P-value | |
| Physical illness | -0.46 | 0.649 | -0.92 | 0.358 | -1.19 | 0.233 |
| Mental health issues | -1.94 | 0.053 | -2.19 | 0.028 | -3.22 | 0.001 |
| Romantic relationship issues | -1.70 | 0.089 | -1.00 | 0.319 | -1.97 | 0.049 |
| Marital and family issues | -1.23 | 0.219 | -2.06 | 0.040 | -2.74 | 0.006 |
| Sexual issues | 0.00 | 1.000 | ||||
| Parenting and child education | 0.38 | 0.705 | -2.82 | 0.005 | -2.36 | 0.018 |
| Work-related issues | -1.78 | 0.076 | -0.77 | 0.444 | -1.95 | 0.051 |
| Interpersonal relationship issues | -0.41 | 0.680 | -1.57 | 0.117 | -1.84 | 0.067 |
| Learning issues | 0.59 | 0.553 | -2.01 | 0.045 | -1.57 | 0.115 |
1Bold figures indicate statistical significance (P < 0.05)
During the transition from mid-pandemic to post-pandemic, the associations between certain consultation themes and suicidal ideation continued to increase. Mental health issues showed a significant rise in OR from 7.36 (95% CI: 5.76, 9.50) mid-pandemic to 15.5 (95% CI: 8.74, 30.1) post-pandemic (Z = -2.19, P = 0.028). Romantic relationship issues increased from an OR of 4.70 (95% CI: 3.50, 6.34) mid-pandemic to 6.88 (95% CI: 3.59, 14.2) post-pandemic, with the Z-test confirming a significant increase (Z = -1.97, P = 0.049). Marital and family issues also saw a significant increase in OR from 4.80 (95% CI: 3.62, 6.41) mid-pandemic to 10.2 (95% CI: 5.52, 20.6) post-pandemic (Z = -2.74, P = 0.006). Parenting and child education issues exhibited a significant rise in OR from 1.93 (95% CI: 1.24, 2.96) mid-pandemic to 5.18 (95% CI: 2.14, 12.4) post-pandemic (Z = -2.82, P = 0.005). Learning issues also showed a significant increase from an OR of 1.93 (95% CI: 1.24, 2.96) mid-pandemic to 5.00 (95% CI: 2.22, 11.5) post-pandemic (Z = -2.01, P = 0.045). Work-related issues saw an OR increase from 3.12 (95% CI: 2.02, 4.74) mid-pandemic to 4.49 (95% CI: 1.98, 10.4) post-pandemic, with the Z-test indicating a near-significant change (Z = -1.95, P = 0.051). These findings suggest that themes such as mental health, marital and family issues, romantic relationships, parenting/child education, learning issues, and work-related issues became more strongly associated with suicidal ideation as the pandemic progressed.
Comparing the pre-pandemic and post-pandemic phases highlights significant long-term increases in associations. Mental health issues showed a substantial increase in OR from 5.14 (95% CI: 3.97, 6.73) pre-pandemic to 15.5 (95% CI: 8.74, 30.1) post-pandemic, with a significant Z-test result (Z = -3.22, P = 0.001). Romantic relationship issues also increased significantly from an OR of 3.19 (95% CI: 2.29, 4.47) pre-pandemic to 6.88 (95% CI: 3.59, 14.2) post-pandemic, as confirmed by the Z-test (Z = -1.97, P = 0.049). Marital and family issues saw a significant rise in OR from 3.69 (95% CI: 2.73, 5.04) pre-pandemic to 10.2 (95% CI: 5.52, 20.6) post-pandemic (Z = -2.74, P = 0.006). Parenting and child education issues showed a significant increase in OR from 1.33 (95% CI: 0.62, 2.57) pre-pandemic to 5.18 (95% CI: 2.14, 12.4) post-pandemic, confirmed by the Z-test (Z = -2.36, P = 0.018). Work-related issues also increased significantly from an OR of 1.68 (95% CI: 0.97, 2.82) pre-pandemic to 4.49 (95% CI: 1.98, 10.4) post-pandemic, with the Z-test indicating a near-significant change (Z = -1.95, P = 0.051).
In summary, the pandemic led to significant increases in the association between suicidal ideation and various consultation themes among female callers. While the changes from the pre-pandemic to mid-pandemic phases were not always statistically significant, indicating a more gradual shift, the associations continued to strengthen throughout the pandemic. Unlike what was observed in male callers, the associations for female callers did not weaken post-pandemic; instead, they persisted and, in many cases, further intensified. This trend highlights a continuous and escalating association between the pandemic and female mental health, particularly in areas such as mental health issues, marital and family issues, parenting/child education issues, and romantic relationship issues, underscoring the critical need for sustained and targeted mental health support and intervention even as the pandemic’s immediate changes subside.
Discussion
Key findings
In this study, we conducted a detailed analysis of 128,245 calls to the Hangzhou Mental Health Hotline from 2014 to 2023, revealing several key findings closely related to suicidal ideation among callers.Overall, the incidence of suicidal ideation was 9.6%, which varied significantly across different phases of the pandemic. The highest incidence was observed during the mid-pandemic phase (11.95%), compared to the pre-pandemic (7.68%) and post-pandemic phases (10.66%). A study from Japan reported that about 14% of mental health hotline callers experienced suicidal ideation [30], which is higher than the overall rate observed in this analysis. The difference may be attributed to variations in the study period, socio-economic conditions, cultural backgrounds, as well as differing levels of awareness and responses to mental health issues across different populations. The incidence of suicidal ideation among female callers was slightly higher than that among male callers (9.8% vs. 9.4%), consistent with the widely observed phenomenon in previous literature that women are more prone to suicidal ideation under psychological stress [31].
According to multivariable logistic regression analysis, different consultation themes showed significant associations with suicidal ideation among callers. Firstly, physical illness had the strongest association with suicidal ideation, even though it accounted for only 0.7% of all calls. This finding echoes the existing literature, which highlights the significant increase in suicide risk associated with chronic or severe physical health problems. For example, in Canada, the association between physical illness and suicidal ideation is particularly pronounced among young people with chronic physical conditions [32]. Similarly, in the general population of the United States, individuals with multiple physical illnesses have a higher risk of engaging in suicidal behavior [33]. Secondly, mental health issues accounted for 45.1% of all calls, and their significant association with suicidal ideation is widely recognized in the literature. Mental health problems such as depression and anxiety are considered important predictors of suicidal ideation [34]. Additionally, romantic relationship problems and marital and family issues accounted for 6.5% and 9.0% of all calls, respectively, and showed a significant association with suicidal ideation. Research indicates that family conflicts, betrayal in romantic relationships, and lack of family support exacerbate emotional distress, increasing the likelihood of suicide attempts and ultimately leading to suicidal behavior [35]. A lack of social support and emotional isolation often aggravates psychological distress, further increasing the risk of suicide [36]. Although work-related issues and academic problems accounted for a smaller proportion of all calls, they still showed a significant association with suicidal ideation. Work pressure and academic stress are common sources of stress in modern society, which, in certain circumstances, can lead to severe psychological distress and trigger suicidal ideation [37].
Gender-specific analysis
The gender-specific analysis of this study revealed significant differences in the association between various consultation themes and suicidal ideation among male and female callers to the Hangzhou Mental Health Hotline. Female callers exhibited a stronger association between suicidal ideation and several consultation themes compared to male callers. Specifically, females showed higher suicidal ideation in relation to physical illness, mental health issues, romantic relationship problems, marital and family issues, parenting and child education issues, work-related problems, and interpersonal relationship issues. This finding aligns with existing research indicating that women are generally more susceptible to emotional and social stress, and may experience greater psychological distress when facing these challenges [38, 39]. The study found that physical health issues have a gender-intersecting effect on suicide risk, with women under 60 being more likely to experience suicidal ideation [40]. Similarly, female callers showed a stronger association between mental health issues and suicidal ideation. Data indicates that women are twice as likely as men to be diagnosed with anxiety and depression, which are strong predictors of suicidal ideation [41]. The additional responsibilities of managing interpersonal relationships, family, and career may exacerbate these mental health issues, further increasing the risk of suicidal ideation.
Moreover, women are generally more likely to seek help for mental health issues compared to men. Due to traditional male norms, stigma, and lower mental health literacy, men often exhibit reluctance to seek help [42]. Women tend to be more open in expressing emotional distress, whereas men may downplay symptoms and find it difficult to disclose emotions. This tendency can be observed in the gender ratio of hotline users (45.9% male vs. 54.1% female). This inclination to seek support may explain why women show a stronger association between these themes and suicidal ideation; they are more likely to openly discuss these issues and, therefore, are more likely to report suicidal ideation during such calls. On the other hand, men may be less inclined to seek help for emotional or interpersonal issues, which may explain the lower observed association in some themes. When men do seek help, it may be for issues where they feel particularly vulnerable or isolated, such as sexual issues. Sexual issues, which accounted for 2.1% of consultations, showed a protective effect against suicidal ideation in male callers, while no significant association was found in female callers. Although this result lacks direct support in existing literature, it suggests a phenomenon worthy of further exploration. Men may be reluctant to seek help for mental health issues, including those related to sexual problems, and the hotline may provide a unique and important form of support, potentially offering emotional relief or psychological comfort that reduces the risk of suicidal ideation. learning issues were significantly associated with suicidal ideation in female callers but not in male callers. This may be related to social expectations and gender roles; women may experience greater pressure to succeed academically, which could exacerbate feelings of inadequacy and lead to higher rates of suicidal ideation [43]. In contrast, men may face different societal pressures, such as financial stress, which has been identified as a significant risk factor for suicidal ideation in men [44].
These findings underscore the necessity of adopting gender-sensitive approaches in mental health interventions. For female callers, personalized support should focus on managing chronic physical illnesses, mental health issues, and interpersonal conflicts, with an emphasis on providing emotional support and stress relief strategies. Given that women are more likely to seek help proactively, it is crucial to enhance the accessibility and responsiveness of hotline services and psychological counseling. For men, given their lower likelihood of seeking help for emotional and interpersonal issues but the protective effect seen in consultations about sexual issues, interventions should aim to reduce the stigma associated with seeking help, promote mental health education, provide anonymous support services, and establish male-friendly support channels. Additionally, targeted interventions addressing academic pressure for women and financial stress for men, along with enhancing the gender sensitivity of mental health hotline services, will effectively improve the outcomes of mental health services, reduce the risk of suicide, and enhance overall mental health.
COVID-19 pandemic phases analysis
The analysis of the association between different consultation themes and suicidal ideation across various pandemic phases revealed significant gender differences. The effects of the pandemic on male callers were more rapid and severe, particularly concerning mental health issues, romantic relationships, and marital and family problems. The association between these themes and suicidal ideation significantly increased during the mid-pandemic period but showed a slight reduction post-pandemic, although it remained higher than pre-pandemic levels. This phenomenon can be explained by several factors:1)Economic Pressure: The pandemic-induced global economic recession led to unemployment, income reduction, or job instability for many men. Traditional gender roles often designate men as the primary economic providers, and thus, economic uncertainty had a profound impact on their mental health [45]. 2)Increased Social Isolation: Lockdowns and social distancing measures heightened feelings of loneliness and isolation, which are critical factors contributing to mental health issues. This is particularly significant for men, who may have less access to or are less likely to seek social support at levels comparable to women, thereby exacerbating stress in romantic and marital contexts [46, 47]. 3)Cultural Taboos Around Emotional Expression: Men typically refrain from expressing emotions or seeking psychological help, leading to feelings of isolation and helplessness [42]. This emotional suppression can result in a rapid deterioration of mental health, increasing the risk of suicidal ideation. However, post-pandemic, as society gradually returned to normalcy with improved economic conditions and the resumption of social activities, men likely regained some stability and support networks, which may explain the observed reduction in suicidal ideation, though it remained above pre-pandemic levels. For instance, in Spain, the relaxation of lockdowns led to a 42% decrease in male suicidal ideation and behavior [48].
In contrast, changes in female callers’mental health during the pandemic were slower and more sustained. Although the increase in the association between various consultation themes and suicidal ideation was relatively modest for female callers during the mid-pandemic period, this association continued to rise post-pandemic, particularly concerning mental health issues, romantic relationships, and marital and family problems. This trend can be attributed to several factors:1)Burden of Multiple Roles: During the pandemic, women typically bore more responsibilities within the family, such as childcare, managing household chores, and balancing remote work with family life [49]. The cumulative stress from these multiple roles continued to affect women’s mental health into the post-pandemic period [50].2)Ongoing Emotional Investment and Psychological Stress: Women often invest more emotionally in managing marital and family issues. The increased family conflicts and relationship problems during the pandemic gradually intensified the psychological stress of women, which, in many cases, did not abate post-pandemic and, in fact, worsened [51].3)Disruption of Social Support Networks: Although women are more likely to seek help, the reduction in social activities during the pandemic may have deprived them of traditional support systems such as emotional support from friends and family, or community activities [52]. This disruption likely contributed to the continued psychological distress experienced by women in the post-pandemic phase. Furthermore, the long-term uncertainty brought by the pandemic, ongoing health threats, and pressure related to social roles may have exacerbated mental health problems in women [53], particularly in areas related to mental health, romantic relationships, and marital and family problems [54].
The pandemic not only exacerbated existing mental health problems but also introduced new sources of psychological stress. Social isolation, unemployment, economic pressure, and heightened tensions within families during lockdowns all emerged as significant stressors [55, 56]. For women, these issues likely manifested as increased anxiety and depression, while for men, the effects were more likely to include anger, helplessness, and diminished self-esteem. These gender-specific differences underscore the critical importance of gender-sensitive interventions through mental health hotlines during the pandemic. For men, hotlines should provide counseling services focused on managing economic pressure, connecting them with economic aid and job retraining resources to help address financial difficulties exacerbated by the pandemic. Additionally, hotlines should promote male-friendly social support networks, organizing both virtual and in-person social activities to reduce feelings of isolation. To address the cultural stigma around emotional expression, hotlines should enhance mental health education campaigns, offer anonymous counseling services, and encourage men to express their emotions and seek help more openly.For women, who have faced pronounced stress from multiple roles during the pandemic, hotlines should offer resources to help them balance work and family responsibilities, including the establishment of specialized psychological support groups. Furthermore, hotlines should offer long-term emotional support and personalized psychological counseling services to help women address the ongoing psychological challenges related to marital and family issues. To help women rebuild social support networks disrupted during the pandemic, hotlines can guide them to participate in community support and virtual platform activities, fostering emotional exchange and support.
Limitations and future research directions
This study has several limitations that need to be acknowledged. The reliance on individuals who voluntarily called the mental health hotline limits the generalizability of the findings, as it excludes those who may not seek help. The cross-sectional design hinders the exploration of causal relationships between consultation themes and suicidal ideation. Furthermore, the limited demographic and background information of callers restricts the understanding of confounding factors such as socioeconomic status and preexisting mental health conditions. The focus on immediate crisis intervention may overlook chronic issues, while the anonymity of calls poses challenges for follow-up and long-term evaluation. Future research should employ longitudinal designs to track the relationship between consultation themes and suicidal ideation over time and collect more comprehensive demographic data to better understand influencing factors. Developing safe follow-up mechanisms and using mixed methods will enable a deeper exploration of the relationship between consultation themes and suicidal ideation. Lastly, developing gender-sensitive strategies and exploring the experiences of marginalized groups are crucial for enhancing the inclusivity and effectiveness of mental health hotlines.
Conclusion
This study reveals a significant association between suicidal ideation and consultation themes such as physical health issues, mental health problems, romantic relationships, and family issues among callers to the Hangzhou Mental Health Hotline over the past decade. The gender differences are notable, with female callers being more heavily affected. During the global COVID-19 pandemic, the association between suicidal ideation and consultation themes among male callers exhibited a sharp upward trend, which eased after the pandemic. In contrast, among female callers, the association between suicidal ideation and consultation themes showed gradual accumulation and continued to worsen in the later stages of the pandemic. These findings strongly advocate for the development and implementation of gender-sensitive mental health intervention strategies to more effectively address this challenge.
Acknowledgements
Gratitude to Dr. Haidong Song for guidance and to Zhejiang’s Science and Tech Department for funding.
Authors' contributions
DW contributed to the analyses/interpretation of results/writing of original draft preparation; YW performed formal analysis. HS contributed to supervision/project administration/guidance; QC contributed to the data collation; YW oversaw project administration. All authors were involved in preparing and revising the manuscript. All authors have read and approved the final manuscript.
Funding
Public Projects of Science and Technology Department of Zhejiang Province (LGF21H090006).
Availability of data and materials
The datasets generated during the current study are not publicly available due to Involving some personal information about the caller but are available from the corresponding author upon reasonable request.
Declarations
Ethics approval and consent to participate
The investigation was approved by the Ethics Committee of Hangzhou Seventh People’s Hospital, which highlighted that all hotline data utilized in this study were recorded following prior notification to callers about the collection of information. Importantly, informed consent was obtained from the callers before any data gathering occurred. Furthermore, considering that the hotline operates anonymously and the study is retrospective, not involving sensitive personal information, the Ethics Committee of Hangzhou Seventh People’s Hospital concluded that the study did not present any ethical concerns.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.World Health Organization. Suicide worldwide in 2019: global health estimates. 2021. https://www.who.int/publications/i/item/9789240026643. Accessed 19 Sept 2024.
- 2.Jiang H, Niu L, Hahne J, Hu M, Fang J, Shen M, et al. Changing of suicide rates in China, 2002–2015. J Affect Disord. 2018;240:165–70. [DOI] [PubMed] [Google Scholar]
- 3.Shepard DS, Gurewich D, Lwin AK, Reed GA Jr, Silverman MM. Suicide and suicidal attempts in the United States: costs and policy implications. Suicide Life Threat Behav. 2016;46(3):352–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kinchin I, Doran CM. The economic cost of suicide and non-fatal suicide behavior in the Australian workforce and the potential impact of a workplace suicide prevention strategy. Int J Environ Res Public Health. 2017;14(4):347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.De Leo D, Heller T. Intensive case management in suicide attempters following discharge from psychiatric care. Aust J Prim Health. 2007;13(3):49–58. [Google Scholar]
- 6.Goldsmith SK. Suicide prevention and intervention: summary of a workshop. National Academies Press; 2001. [PubMed]
- 7.Gould MS, Kalafat J, HarrisMunfakh JL, Kleinman M. An evaluation of crisis hotline outcomes. Part 2: Suicidal callers. Suicide Life Threat Behav. 2007;37(3):338–52. [DOI] [PubMed]
- 8.Youn HM, Kang SH, Jang SI, Park EC. Association between social participation and mental health consultation in individuals with suicidal ideation: a cross-sectional study. BMC Psychiatry. 2020;20:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord. 2020;277:55–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav Immun. 2020;89:531–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Santomauro DF, Herrera AMM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Su Y, Jin J, Zhu L, Cai J. Emerging psychological crisis issues during lockdown in Shanghai. Lancet Reg Health–West Pac. 2022;25:100536. [DOI] [PMC free article] [PubMed]
- 14.Liu S, Yang L, Zhang C, Xiang YT, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7(4):e17–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Li W, Yang Y, Liu ZH, Zhao YJ, Zhang Q, Zhang L, et al. Progression of mental health services during the COVID-19 outbreak in China. Int J Biol Sci. 2020;16(10):1732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hermida JRF, Santolaya F, García-Vera M, et al. The COVID-19 psychological helpline of the Spanish Ministry of Health and Spanish Psychological Association: characteristics and demand. Rev Esp Salud Pública. 2020;94:e202010138–e202010138. [PubMed] [Google Scholar]
- 17.Eslami Jahromi M, Ayatollahi H, Ebrazeh A. Covid-19 hotlines, helplines and call centers: a systematic review of characteristics, challenges and lessons learned. BMC Public Health. 2024;24(1):1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Matsumoto N, Kadowaki T, Takanaga S, Shigeyasu Y, Okada A, Yorifuji T. Longitudinal impact of the COVID-19 pandemic on the development of mental disorders in preadolescents and adolescents. BMC Public Health. 2023;23(1):1308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Troisi A. Mental Health Challenges during the COVID-19 Pandemic. J Clin Med. 2023;12(3):1213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Scott KM, Hwang I, Chiu WT, Kessler RC, Sampson NA, Angermeyer M, et al. Chronic physical conditions and their association with first onset of suicidal behavior in the world mental health surveys. Psychosom Med. 2010;72(7):712–9. [DOI] [PubMed] [Google Scholar]
- 21.Ahmedani BK, Peterson EL, Hu Y, Rossom RC, Lynch F, Lu CY, et al. Major physical health conditions and risk of suicide. Am J Prev Med. 2017;53(3):308–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Kleiman EM, Liu RT. Social support as a protective factor in suicide: Findings from two nationally representative samples. J Affect Disord. 2013;150(2):540–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Foster T. Adverse life events proximal to adult suicide: a synthesis of findings from psychological autopsy studies. Arch Suicide Res. 2011;15(1):1–15. [DOI] [PubMed] [Google Scholar]
- 24.Schrijvers DL, Bollen J, Sabbe BG. The gender paradox in suicidal behavior and its impact on the suicidal process. J Affect Disord. 2012;138(1–2):19–26. [DOI] [PubMed] [Google Scholar]
- 25.Phillips MR, Shen Q, Liu X, Pritzker S, Streiner D, Conner K, et al. Assessing depressive symptoms in persons who die of suicide in mainland China. J Affect Disord. 2007;98(1–2):73–82. [DOI] [PubMed] [Google Scholar]
- 26.Li X, Phillips M, Zhang Y, Wang Z. Development and validity of a diagnostic screening instrument for depression. Chin J Nerv Ment Dis. 2007;33(5):257–63. [Google Scholar]
- 27.An J, Yin Y, Zhao L, Tong Y, Liu NH. Mental health problems among hotline callers during the early stage of COVID-19 pandemic. PeerJ. 2022;10:e13419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Witte TK, Gould MS, Munfakh JLH, Kleinman M, Joiner TE Jr, Kalafat J. Assessing suicide risk among callers to crisis hotlines: A confirmatory factor analysis. J Clin Psychol. 2010;66(9):941–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Centers for Disease Control and Prevention. COVID-19 Timeline. 2023. https://www.cdc.gov/museum/timeline/covid19.html. Accessed 27 Aug 2024.
- 30.Ohtaki Y, Oi Y, Doki S, Kaneko H, Usami K, Sasahara S, et al. Characteristics of telephone crisis hotline callers with suicidal ideation in Japan. Suicide Life Threat Behav. 2017;47(1):54–66. [DOI] [PubMed] [Google Scholar]
- 31.Russo NF, Green BL. Women and mental health. Greenwood Press/Greenwood Publishing Group; 1993.
- 32.Virk P, Doan Q, Karim ME. Chronic physical conditions and suicidal ideation: a population-level analysis of Canadian school-attending young adults. J Ment Health. 2024;33(3):304–11. [DOI] [PubMed] [Google Scholar]
- 33.Stickley A, Koyanagi A, Ueda M, Inoue Y, Waldman K, Oh H. Physical multimorbidity and suicidal behavior in the general population in the United States. J Affect Disord. 2020;260:604–9. [DOI] [PubMed] [Google Scholar]
- 34.Oliva V, Roberto N, Andreo-Jover J, Bobes T, Rivero MC, Cebriá A, et al. Anxious and depressive symptoms and health-related quality of life in a cohort of people who recently attempted suicide: A network analysis. J Affect Disord. 2024;355:210–9. [DOI] [PubMed] [Google Scholar]
- 35.Fallahi-Khoshknab M, Amirian Z, Maddah SSB, Khankeh HR, Dalvandi A. Instability of emotional relationships and suicide among youth: a qualitative study. BMC Psychiatry. 2023;23(1):50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Darvishi N, Poorolajal J, Azmi-Naei B, Farhadi M. The Role of Social Support in Preventing Suicidal Ideations and Behaviors: A Systematic Review and Meta-Analysis. J Res Health Sci. 2024;24(2):e00609–e00609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Moran M. Academic Stress, Failure May Be Underrecognized Trigger for Suicidal Thoughts, Behaviors. American Psychiatric Publishing, Inc.; 2022.
- 38.Kang M, Yu S, Choe SA, Moon D, Ki M, Chun BC. Gender Differences in Psychosocial Stress During the COVID-19 Pandemic: A Population-based Study in South Korea. J Prev Med Public Health Yebang Uihakhoe Chi. 2023;56(5):413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Matud MP, Díaz A, Bethencourt JM, Ibáñez I. Stress and psychological distress in emerging adulthood: A gender analysis. J Clin Med. 2020;9(9):2859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Phillips JA, Hempstead K. The role of context in shaping the relationship between physical health and suicide over the life course. SSM-Popul Health. 2022;17:101059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Pavlidi P, Kokras N, Dalla C. Sex differences in depression and anxiety. In: Sex Differences in Brain Function and Dysfunction. Springer; 2022. pp. 103–132.
- 42.Parent MC, Hammer JH, Bradstreet TC, Schwartz EN, Jobe T. Men’s mental health help-seeking behaviors: An intersectional analysis. Am J Men’s Health. 2018;12(1):64–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Faraj RNH. Gender disparities in suicidal ideation among university students: A quantitative study. PsychTech Health J. 2023;7(1):24–9. [Google Scholar]
- 44.Logoz F, Weber R, Eggenberger L, Walther A. Thoughts about dropping out of studies as warning sign for suicidal ideation and mental health problems in male university students. J Men’s Health Online. 2023;19(8):60–9. [Google Scholar]
- 45.Fox AB, Baier AL, Alpert E, Nillni YI, Galovski TE. Psychosocial and Economic Impacts of the COVID-19 Pandemic on the Mental Health of Veteran Men and Women. J Women’s Health. 2023;32(10):1041–51. [DOI] [PubMed] [Google Scholar]
- 46.Lee CKK, Chan KNJ, Wong SMC, Wong HSG, Lei HCJ, So YK, et al. Relationships between psychopathological symptoms, pandemic-related stress, perceived social support, and COVID-19 infection history: a network analysis in Chinese college students. Front Psychiatry. 2024;15:1340101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Sheikh A, Payne-Cook C, Lisk S, Carter B, Brown JS. Why do young men not seek help for affective mental health issues? A systematic review of perceived barriers and facilitators among adolescent boys and young men. Eur Child Adolesc Psychiatry. 2024. 10.1007/s00787-024-02520-9. [DOI] [PubMed]
- 48.Gómez-Revuelta M, Sánchez-Lafuente CG, Yáñez JS, Pindado LMG, Echevarría LESE, Meseguer TC, et al. Long-term COVID-19 pandemic impact on suicide Thoughts and Behaviors (STB): An interrupted time series analysis in Spain 2-year after pandemic outbreak. Psychiatry Res. 2024;339:116086. [DOI] [PubMed] [Google Scholar]
- 49.Indrastuti M, Herawati T. The multiple role of woman, coping strategy, and family resilience during Covid-19 pandemic. J Child Fam Consum Stud. 2023;2(2):138–46. [Google Scholar]
- 50.Muafiah E, Susanto S, Sofiana NE, Khasanah U. The Role of Female Lecturers of IAIN Ponorogo in Family Care During The Covid-19 Pandemic Period. Samarah Jurnal Hukum Keluarga Dan Hukum Islam. 2023;7(2):1054–76. [Google Scholar]
- 51.Keskin G, Gümüşsoy S, Taşdemir Yiğitoğlu G. Spouses’ coping with stress during the COVID-19 pandemic: is there a difference between male and female attitudes? Women Health. 2023;63(10):801–17. [DOI] [PubMed] [Google Scholar]
- 52.Keilholtz B, Spencer C, Vail S, Palmer M. COVID-19-related stress and its association with intimate partner violence perpetration and victimization. Behav Sci. 2023;13(7):593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kopylova N, Greyling T, Rossouw S. Women’s Mental Health During COVID-19 in South Africa. Appl Res Qual Life. 2024;19(3):959–90. [Google Scholar]
- 54.Neises-Rudolf M. The Impact on Women’s Mental Health During Times of Pandemic. In: Women’s Health and Pandemic Crisis. Springer; 2023. pp. 11–24.
- 55.Patrono A, Renzetti S, Guerini C, Macgowan M, Moncada SM, Placidi D, et al. Social isolation consequences: lessons from COVID-19 pandemic in a context of dynamic lock-down in Chile. BMC Public Health. 2024;24(1):599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Wang MT, Scanlon CL, Del Toro J, Schall JD. Employment status and psychosocial adjustment among adolescents and parents during the COVID-19 pandemic: multi-informant data from ecological momentary assessments. Dev Psychol. 2024;60(2):335. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during the current study are not publicly available due to Involving some personal information about the caller but are available from the corresponding author upon reasonable request.