

Abstract
We examined the sensitivity and time‐course of recovery of neuromuscular and perceptual player monitoring measures to U‐18 English Premier League academy football match play. Eighteen players performed maximal posterior chain, hip adductor and abductor isometric strength tests, countermovement jumps (CMJ) and provided self‐report wellbeing scores around eight competitive league home games: 1 day before (MD‐1), pre‐match (MD‐PRE), post‐match (MD‐POST) and two (MD+2) and three (MD+3) days post‐match. A permutational multivariate analysis of variance and post hoc univariate analyses of variance were used to examine match‐induced responses to monitoring variables. Between MD‐1 and MD‐POST, we observed small to moderate reductions to the adductor and abductor peak force and maximal impulse and IPCS peak force; small reductions to CMJ jump height (JH) (flight time), eccentric peak force and eccentric deceleration rate of force development and moderate to large reductions to perceived fatigue, muscle soreness and mood. No match‐induced changes were observed for CMJ flight time: contraction time or eccentric duration. Posterior chain, abductor, CMJ and self‐report measures normalised by MD+3 but adductor peak force remained compromised at MD+3 (ES = small). Posterior chain, adductor and abductor peak isometric force and maximal impulse; CMJ JH, eccentric peak force and eccentric deceleration rate of force development and perceived fatigue, muscle soreness and mood are sensitive to match‐induced fatigue. Since adductor peak force remained compromised at MD+3, it is apparent that players might not achieve complete neuromuscular recovery within 3 days of match play, and that the adductor muscle group might be particularly vulnerable to match‐induced fatigue.
Keywords: fatigue, monitoring, performance, recovery, soccer
Highlights
U‐18 English Premier League (EPL) academy football match play induced acute reductions to countermovement jump (jump height [flight time], eccentric peak force and eccentric deceleration rate of force development); isometric strength (abductor, adductor and posterior chain peak force and abductor and adductor maximal impulse) and athlete self‐report (perceived fatigue, muscle soreness and mood) measures.
Match‐induced changes to countermovement jump, abductor, posterior chain and self‐report measures typically normalised between MD+2 and MD+3 but adductor peak force remained compromised at MD+3.
No meaningful match‐induced changes were observed to widely used countermovement jump movement strategy measures (i.e., flight time: contraction time ratio or eccentric duration).
U‐18 EPL academy football players might not achieve complete neuromuscular recovery by MD+3. The adductor muscle group might be particularly susceptible to match‐induced fatigue.
1. INTRODUCTION
Football is a high‐volume, high‐intensity and intermittent sport characterised by repeated bouts of acceleration, deceleration, sprint, high‐speed running and change of direction activity (Abbott et al., 2018a, 2018b; Akenhead et al., 2013; Reynolds et al., 2021). The match running demands of the English Premier League (EPL) U‐18 games are substantial. Indeed, Reynolds and colleagues (Reynolds et al., 2021) reported equivocal total (10,259 m, 10,052 m and 10,141 m), high‐speed running (626 m, 704 and 673 m), high‐metabolic load (2034 m, 2062 m and 1990 m) and sprinting (110 m, 142 and 144 m) distances during competitive EPL U‐18, U‐23 and 1st Team match play.
Neuromuscular fatigue (NMF) (i.e., specific reduction to the maximal force generating capacity of muscle) is a natural consequence of match play that can compromise physical performance potential and increase injury susceptibility (Bittencourt et al., 2016; Meeusen et al., 2013; Schwellnus et al., 2016; Soligard et al., 2016; Verschueren et al., 2020). To mitigate these risks, practitioners are advised to monitor the neuromuscular and perceptual responses of players and adjust planned training load to accommodate recovery when fatigue is detected (Akenhead et al., 2016; Meeusen et al., 2013; Salter, De Ste Croix, et al., 2021; Schwellnus et al., 2016; Soligard et al., 2016). Non‐exhaustive neuromuscular performance tests, including the countermovement jump (CMJ) and isometric tests of hip abduction (IABS), hip adduction (IADS) and posterior chain (IPCS) strength and athlete self‐report measures (ASRM), are widely used for this purpose in EPL academy teams (Akenhead et al., 2013; Bishop et al., 2022; Salter, De Ste Croix, et al., 2021).
To date, small to moderate 48‐h reductions to CMJ performance measures of jump height (JH) (Akyildiz et al., 2022; Deely et al., 2022), maximal velocity (Akyildiz et al., 2022) and reactive strength index (Deely et al., 2022) have been reported following competitive games (Akyildiz et al., 2022) and strenuous training (Deely et al., 2022) using linear positional encoder (Akyildiz et al., 2022) and optical timing (Deely et al., 2022) systems in U‐18 football players. In senior professional athletes, NMF is reported to induce changes to force plate derived CMJ movement strategy measures (i.e., flight time: contraction time ratio; FT:CT) independently of changes to JH (Cormack et al., 2008; Gathercole et al., 2015a, 2015b). For example, Cormack and colleagues (Cormack et al., 2008) reported reductions to both CMJ JH and FT:CT following the Australian Football (AFL) training and match play but reported greater and longer‐lasting changes to FT:CT (Cormack et al., 2008). However, despite popular use in practice, no scientific research has examined the match‐induced changes to CMJ movement strategy variables in EPL academy football players.
Maximal hip adduction (Ryan et al., 2019) and posterior chain (McCall et al., 2015a, 2015b) strength are reported to exert important moderating effects on injury risk, and maximal isometric strength measures in these muscle groups are commonly used to signal NMF in practice. Several investigations have examined the response of lower limb isometric strength measures to football match play (McCall, Nedelec, et al., 2015; Salter, Cresswell, & Forsdyke, 2021). Salter and colleagues reported 3%–14% (very likely substantial), 6%–16% (very likely substantial) and 3%–5% (likely substantial) reductions to IABS, IADS and IPCS peak force measures following simulated match play in high‐level U‐18 players (Salter, Cresswell, & Forsdyke, 2021). Interestingly, McCall and colleagues (McCall, Nedelec, et al., 2015) reported more severe (i.e., 11%–16%; large) post‐match reductions to IPCS peak vertical force following senior professional competitive football match play. However, despite popular use in practice, no scientific research literature has examined the match‐induced changes to these measures in EPL academy football players to examine their conceptual efficacy.
ASRM have demonstrated superior sensitivity to changes in training load than many objective measures of fatigue in athletes (Saw et al., 2016). In elite‐level senior professional football players, ASRM subscale measures of perceived fatigue, muscle soreness and sleep quality (McLean et al., 2010) have demonstrated sensitivity to changes in training (Thorpe et al., 2017) and match (Thorpe et al., 2016) load and are reported to relate to biological fatigue measures (Springham et al., 2021). These methods are popular since they can be deployed and analysed rapidly in the applied environment, facilitating fast decision‐making relating to training load planning. Notably, Thorpe and colleagues (Thorpe et al., 2017) reported impairments to these subscale measures for ∼96 h post‐match in EPL players, but equivalent research is yet to be conducted in an EPL academy cohort.
Limited scientific research has examined the sensitivity to match play or the time‐course of recovery of IABS, IADS, IPCS or ASRM measures in U‐18 academy football players. Both research (Kelly et al., 2019) and anecdotal reports alike indicate that players most commonly return to high‐volume and high‐intensity training at ∼72 h post‐match. However, alarmingly, no scientific research has examined if academy football players achieve neuromuscular recovery by this time‐point. Accordingly, the aim of this research was to examine the sensitivity of IABS, IADS, IPCS and ASRM measures to U‐18 EPL academy football match play and to establish if players achieve neuromuscular and perceived recovery by match day (MD) +3.
2. MATERIALS AND METHODS
2.1. Study design
Eighteen U‐18 outfield players (n = 27, age = 17.0 ± 0.7; height = 1.82 ± 0.07 m and body mass = 73.5 ± 76 kg) from a category 1 EPL academy team participated in this investigation. All testing was conducted in an environmentally controlled performance centre located at the team's training facility. To examine pre‐to‐post match neuromuscular performance and perceived wellbeing responses, players attended five testing sessions around 8 separate home games played at the team training facility at: (1) ∼09:00 the day before MD, (i.e., MD‐1), (2) ∼09:00 the morning of the game (MD‐PRE), (3) ∼30 min post‐match (MD‐POST), (4) ∼09:00 44 h post‐match (MD+2) and (5) ∼09:00 68 h post‐match (MD+3). All data were collected around U‐18 Premier League Fixtures, during single‐game weeks and during the in‐season period. Data from players who played >75 min were included in the analysis (mean ± SD = 85.8 ± 8.7 min). All games kicked off at 11:00 a.m. and no data were analysed from games in which extra time was played. Weekly training and match distribution and load were consistent for all training weeks across the experimental period.
Prior to testing at MD‐1, MD‐PRE, MD+2 and MD+3, players performed a standardised warm‐up consisting of ∼4 min of dynamic mobility exercises (3 × 10 m heel flicks, hamstring kicks and walking lunges with a 10 m walk recovery between repetitions), followed by three warm‐up CMJ's at 60%, 80% and 100% of perceived maximal effort, separated by ∼30 s. For testing MD‐POST, players were tested ∼30 min after the final whistle. All players had routinely performed the monitoring tests ∼2 times per week for at least one competitive season and were therefore considered to be highly familiar with all testing protocols. Ethical approval was provided by an institutional human research ethics committee.
2.2. Athlete self‐report measures
Prior to warming up, players completed an ASRM inventory (McLean et al., 2010) composed of three questions relating to perceived: fatigue, muscle soreness and mood at each data collection time‐point. Data were collected digitally by the same experienced practitioner across the experimental period. Responses were scored on a Likert scale of 1–‐5, where 1, 2, 3, 4 and 5 = very bad, bad, normal, good and very good, respectively (McLean et al., 2010).
2.3. Countermovement jump
Countermovement jump testing was performed on dual force plates (ForceDecks FD4000, Vald Performance, Brisbane, AU) sampling at 1000 Hz. Force‐time curves were analysed using the proprietary software (ForceDecks Version 2.0.8000, Vald Performance, Brisbane, AU) and using methods described previously (Eagles et al., 2015; Howarth et al., 2022). Prior to each testing day, a known weight (20 kg) was used to test the accuracy of force measurement, with ±0.1 kg considered to be an acceptable level of measurement error (Howarth et al., 2022). The force plates were zeroed prior to testing each player. Each player was asked to stand still on the force plates with their hands on their hips for ∼5 s until a stable body mass was recorded. Players then performed three separate maximal CMJ, each separated by ∼15 s. Players were required to keep their hands on their hips for the entirety of each jump and were cued to ‘jump maximally: as high as they could and to land on the force plates’. They were then asked to reposition their feet between repetitions. All jump testing was conducted by the same experienced practitioner. In cases where a measurement error was observed (i.e., ‘tucking’ or ‘piking’ the legs during the flight phase, a double contact prior to jumping or if they did not land on the force plates), data were omitted and the player was asked to perform another repetition.
2.4. Isometric posterior chain strength
Isometric posterior chain strength was measured using portable force plates (PASCO PS‐2141, Roseville, California, UK) sampling at 1000 Hz, positioned on a fixed plinth (Figure 1) similarly to methods reported previously (McCall, Nedelec, et al., 2015). Force‐time curves were analysed using proprietary software (ForceDecks Version 2.0.8000, Vald Performance, Brisbane, AU). Three maximal tests were conducted on each limb, alternately. The heel of the testing limb was positioned in the middle of the force plate with the knee angle fixed at 30 degrees of flexion; confirmed by a hand‐held goniometer (Physio Parts, Twickenham, UK). The heel of the non‐testing limb remained in contact with the ground, under the plinth, for the duration of each test. For each test, players were instructed to push maximally, down into the force plate for 3 s, whilst keeping their buttocks, hips and head in contact with the ground and their arms fixed across their shoulders. Cueing for all testing was standardised as ‘3, 2, 1, push, push, push, relax’. All testing was conducted by the same experienced practitioner. Where a measurement error was observed (i.e., the buttocks, hips or head lifted from the ground, the non‐testing heel lifted from the floor or the arms lifted away from the shoulders) data were omitted and the player was asked to perform another repetition.
FIGURE 1.

Standardisation of participant positioning for isometric posterior chain (left) and isometric hip abduction and adduction (right) strength testing.
2.5. Isometric hip adductor and abductor strength
Isometric hip adductor and abductor strength were measured using a portable hip strength assessment device (Vald ForceFrame Strength Testing System, Vald Performance, Brisbane, AU) sampling at 1000 Hz (Figure 1) according to methods reported previously (Ryan et al., 2019; Salter, Cresswell, & Forsdyke, 2021; O'Brien et al., 2019; Jones, Mullen, et al., 2021; Jones, Clair, et al., 2021; Desmyttere et al., 2019; Bourne et al., 2020). Force‐time curves were analysed using proprietary software (ForceDecks Version 2.0.8000, Vald Performance, Brisbane, AU). Three maximal tests were conducted for hip adduction and hip abduction, which were alternated. For hip adduction, players were positioned into 45 degrees of hip flexion; confirmed using a hand‐held goniometer, with the medial femoral epicondyles of both knees positioned centrally and perpendicular to the medial sensor pads in the force frame. Players were asked to position their feet at hips width and to keep both feet flat on the floor throughout testing. For hip abduction, this method was repeated but with the lateral femoral epicondyles of both knees positioned centrally and perpendicular to the lateral sensor pads in the force frame. For both tests, players were instructed to push maximally (‘inwards’ for hip adduction, and ‘outwards’ for hip abduction) for 3 s, whilst keeping their buttocks, hips and head in contact with the ground and their arms fixed across their shoulders. Cueing for all testing was standardised as ‘3, 2, 1, push, push, push, relax’. All testing was conducted by the same experienced practitioner. Where a measurement error was observed (i.e., the buttocks, hips or head lifted from the ground, a heel lifted from the floor or the arms lifted away from the shoulders) data were omitted and the player was asked to perform another repetition.
Variable selection for neuromuscular performance testing was based on our in‐house analysis of test–retest reliability and popularity of use in similar scientific research literature and practice (Akenhead et al., 2013; Akyildiz et al., 2022; Bishop et al., 2022; Cormack et al., 2008; Deely et al., 2022; Gathercole et al., 2015a, 2015b; McCall et al., 2015a, 2015b; Ryan et al., 2019; Salter et al., 2021a, 2021b; Saw et al., 2016; Springham et al., 2021; Thorpe et al., 2016, 2017). Indeed, we found all chosen variables to have good to excellent between‐session best absolute and relative test–retest reliability in this cohort. These data are presented below as follows: intraclass correlation coefficient (ICC), coefficient of variation (CV%) and minimal detectable change (MDC%). For the CMJ test, 7 bilateral variables were selected from the eccentric, concentric, flight and landing phases: relative concentric peak force (ICC = 0.94, CV% = 4.7% and MDC% = 13.3%), eccentric duration (ICC = 0.88, CV% = 8.1% and MDC% = 23.7%), eccentric deceleration rate of force development (ICC = 0.95, CV% = 20.7% and MDC% = 57.8%), relative eccentric peak force (ICC = 0.94, CV% = 6.4% and MDC% = 18.0%), flight time: contraction time ratio (ICC = 0.91, CV% = 8.1% and MDC% = 23.3%), JH (flight time) (ICC = 0.93, CV% = 5.1% and MDC% = 14.5%) and JH (impulse momentum) (ICC = 0.84, CV% = 7.2% and MDC% = 21.5%) defined previously (Eagles et al., 2015; Howarth et al., 2022). For IPCS, peak vertical force (ICC = 0.88, CV% = 7.5% and MDC% = 21.8%) was selected (Constantine et al., 2019; Matinlauri et al., 2019; McCall, Nedelec, et al., 2015). For IABS and IADS, peak force (IABS ICC = 0.89, CV% = 6.6% and MDC% = 19.8%; IADS ICC = 0.94, CV% = 7.5% and MDC% = 22.3%) and maximal impulse (IABS ICC = 0.86, CV% = 7.5% and MDC% = 22.2%; IADS ICC = 0.94, CV% = 8.0% and MDC% = 23.7%) were selected (Ryan et al., 2019; Salter, Cresswell, & Forsdyke, 2021; O'Brien et al., 2019; Jones, Mullen, et al., 2021; Jones, Clair, et al., 2021; Desmyttere et al., 2019; Bourne et al., 2020).
2.6. Statistical analysis
All statistical analyses were conducted using the R v.4.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Prior to analysis, data were analysed for multivariate normality; this condition was not met. Differences in dependent variables across timepoints were, therefore, assessed using the non‐parametric permutational multivariate analysis of variance (PERMANOVA) and fitted using the vegan R package. Neuromuscular and ASRM variables were included as dependent variables, whilst time‐point was included as an independent variable. Permutations were conducted within participants using the how function in the permute package. Exploratory post hoc univariate linear mixed models were used to investigate univariate differences across timepoints. Mean differences between MD‐1 and all other timepoints were calculated, with participant included as a random factor. Models were fitted using the lmertest R package. Significance was set at p < 0.05. Multiplicity adjustments were not made due to the exploratory nature of the models. Effect sizes (ES; Cohen's d) were calculated and interpreted as follows: <0.2‐trivial; 0.2–0.6‐small; 0.6–1.2‐moderate; 1.2–2‐large and >2.0‐very large.
3. RESULTS
3.1. Descriptive statistics
Team average running demands for the sample games are presented in Table 1, below.
TABLE 1.
Team average whole‐match running demands for selected performance measures for the sample games.
| GPS/MEMS variable | Variable definition | Mean ± SD |
|---|---|---|
| Total distance (TD) | The total distance completed (m) | 10,229 ± 944 |
| Relative high speed running distance (HSR) | Distance completed between 5.5 m/s and 80% of the individualised maximal running velocity (m) | 982 ± 279 |
| High metabolic load distance (HMLd) | Total distance completed >20 W/kg−1 (m) | 2056 ± 396 |
| Explosive distance (ED) | Total distance completed >25.5 W/kg−1 (m) | 1295 ± 242 |
| Relative (‘zone 6’) sprint distance (SD) | Total distance completed >70% of the individualised maximal running velocity (m) | 249 ± 109 |
| Number of maximal accelerations | Total number of accelerations >3 m/s2 | 64 ± 13 |
| Number of maximal decelerations | Total number of decelerations >‐3 m/s2 | 72 ± 16 |
Note: Outfield player data only. Data were collected using the Statsports Apex (Statsports, Belfast, Northern Ireland, UK), global positioning (GPS) and micro‐electrical mechanical (MEMS) sensors sampling at 10 Hz (GPS) and 100 Hz (tri‐axial accelerometer, gyroscope and magnetometer) and proprietary software: Sonra V4.5.7 (Statsports, Belfast, Northern Ireland, UK).
The PERMANOVA revealed no significant main effect of time (p = 0.084) on multivariate outcomes. The results of univariate models are presented in Figure 2.
FIGURE 2.
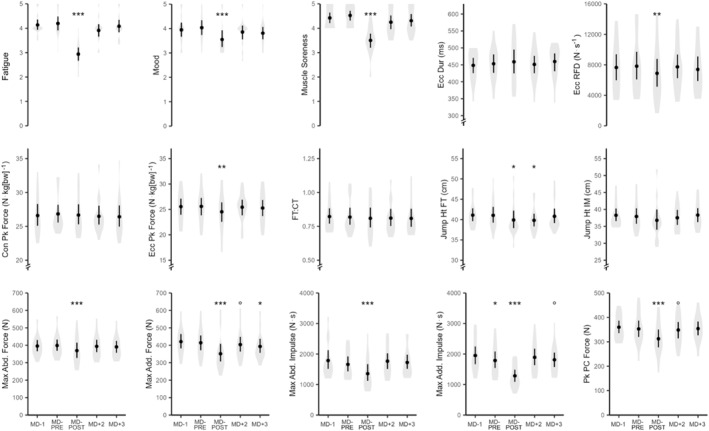
Athlete self‐report, countermovement jump and isometric adductor, abductor and posterior chain strength responses to English Premier League U‐18 academy football match play. Con Pk Force, Concentric Peak Force; Ecc Dur, Eccentric Duration; Ecc Pk Force, Eccentric Peak Force; Eccentric RFD, Eccentric Rate of Force Development; FT:CT, flight time: contraction time ratio; Jump Ht FT, jump Height (Flight Time Equation); Jump Ht IM, Jump Height (Impulse Momentum Equation); Max Abd Force, Maximal Abductor Force; Max Abd Impulse, Maximal Abductor Impulse; Max Add Force, Maximal Adductor Force; Max Add Impulse, Maximal Adductor Impulse; Peak PC Force, Peak Posterior Chain Vertical Force. Symbols denote change relative to MD‐1: O, p = 0.1; *, p = 0.05; **, p = 0.01 and ***, p = 0.001.
3.2. Athlete self‐report measures
Relative to MD‐1, perceived fatigue (d = 1.80, large and p < 0.001), mood (d = 0.61, moderate and p < 0.001) and muscle soreness (d = 1.00, moderate and p < 0.001) reduced at MD‐POST and returned to MD‐1 levels by MD+2.
3.3. Countermovement jump
Relative to MD‐1, eccentric peak force (d = 0.43, small and p = 0.004) and eccentric deceleration rate of force development (d = 0.41, small and p = 0.007) reduced at MD‐POST and returned to MD‐1 levels by MD+2. JH (flight time) reduced at MD‐POST (d = 0.33, small and p = 0.031), remained compromised at MD+2 (d = 0.35, small and p = 0.023) and returned to MD‐1 levels by MD+3. A small (d = 0.22 and p = 0.142) reduction to flight time: contraction was observed between MD‐1 and MD‐POST whereas, eccentric duration, concentric peak force and JH (impulse momentum) did not change around match play (p > 0.050) Figure 2.
3.4. Isometric posterior chain strength
Relative to MD‐1, IPCS peak force reduced at MD‐POST (d = 1.07, moderate and p < 0.001) and returned to MD‐1 levels by MD+2 (d = 0.27, small and p = 0.070) Figure 2.
3.5. Isometric hip adductor and abductor strength
Relative to MD‐1, IABS peak force reduced at MD‐POST (d = 0.85, moderate and p < 0.001) and returned to MD‐1 levels by MD+2. IADS peak force reduced at MD‐POST (d = 1.13, moderate and p < 0.001) and remained low at MD+2 (d = 0.27, small and p = 0.079) and MD+3 (d = 0.37, small and p = 0.017). IABS maximal impulse was reduced at MD‐POST (d = 0.93, moderate and p < 0.001) and returned to MD‐1 levels by MD+2. IADS maximal impulse was reduced at MD‐POST (d = 1.10, moderate and p < 0.001) and at MD+3 (d = 0.26, small and p = 0.095) Figure 2.
4. DISCUSSION
The first aim of this investigation was to examine the sensitivity of CMJ, IABS, IADS, IPCS and ASRM measures to U‐18 EPL academy football match play. We report match‐induced reductions to all IABS, IADS, IPCS and ASRM measures. For CMJ, we report reductions to JH (flight time), eccentric peak force and eccentric deceleration rate of force development, equivocal changes to flight time: contraction time and eccentric duration and no change to peak concentric force or JH (impulse momentum). The second aim of this investigation was to examine if players achieve neuromuscular and perceived recovery by MD+3. Our finding is that match‐induced changes to all CMJ, IABS, IPCS and ASRM measures normalised by MD+2 and that IADS peak force remained compromised at MD+3.
The most important findings from this investigation relate to the response of isometric strength measures to football match play. We observed small to moderate post‐match reductions to IABS and IADS peak force and maximal impulse and IPCS peak force (Figure 2). Importantly, these findings are consistent with previous scientific research literature (McCall, Nedelec, et al., 2015; Salter, Cresswell, & Forsdyke, 2021). For example, Salter and colleagues (Salter, Cresswell, & Forsdyke, 2021) reported 3%–14% (very likely substantial), 6%–16% (very likely substantial) and 3%–5% (likely substantial) reductions to IABS, IADS and IPCS peak force measures following simulated match play in high‐level U‐18 players (Salter, Cresswell, & Forsdyke, 2021). Additionally, McCall and colleagues (McCall, Nedelec, et al., 2015) reported large (11%–16%) pre‐to‐post‐match reductions to IPCS peak force immediately following competitive match play in senior professional players. Both investigations attributed their findings to match‐induced muscle damage, which appears to be a likely explanatory mechanism for our finding also. Indeed, post‐match reductions to neuromuscular performance herein were accompanied by moderate increases to perceived muscle soreness at the same time‐point (Figure 2). Overall, our findings indicate that peak isometric force (for IABS, IADS and IPCS) and maximal impulse (for IABS and IADS) are sensitive to match‐induced fatigue in U‐18 EPL academy football players.
A novel aspect of the current investigation is that we repeated measures at MD+2 and MD+3 to facilitate further understanding of the time‐course of neuromuscular recovery. Though NMF can originate at central (i.e., central nervous system (CNS)) and peripheral (i.e., impaired skeletal muscle contractile function) levels along the motor pathway, recent scientific literature indicates a greater magnitude and slower recovery rate of peripheral compared to central fatigue post‐match in football players (Deely et al., 2022; Thomas et al., 2017). Thus, physiological processes relating to the resolution of muscle contractile function are thought to explain the rate of recovery of NMF post‐match (Deely et al., 2022; Thomas et al., 2017). Interestingly, we observed that the IABS peak force, IABS maximal impulse, IADS maximal impulse and IPCS peak force had typically normalised by MD+2, whereas the IADS peak force remained compromised at MD+3 (ES = small; Figure 2). This finding points to a particular vulnerability of the adductor muscle group to match‐induced fatigue and might help to explain previous adductor injury research findings in academy football players. Indeed, Materne and colleagues (Materne et al., 2021) reported that U‐18 and U‐19 players had the highest injury burden across all academy age groups and that adductor injury incidence represented between 5.9% and 8% all off injuries recorded. Moreover, Wik and colleagues (Wik et al., 2021) reported that hip and groin muscle injuries lead to 4 days of time loss per 1000 h, with players losing 19 days per incidence on average. Collectively, these findings suggest that particular attention should be afforded to the adductor muscle group in fatigue monitoring protocols, weekly training schedules and in individual strength and conditioning programmes.
Importantly, we observed meaningful match‐induced reductions to CMJ JH (flight time) (p = 0.031 and d = 0.35), eccentric peak force (p = 0.004 and d = 0.44) and eccentric deceleration rate of force development (p = 0.007 and d = 0.41) that had normalised by MD+3 and MD+2, respectively (Figure 2). We observed limited match‐induced changes to CMJ movement strategy variables (i.e., FT:CT p = 0.142 and d = 0.22 and Explosive distance (ED) p = 0.309 and d = 0.07). Despite a general paucity of scientific research available to describe the acute response of force plate derived CMJ measures in elite young football players, our findings largely contrast similar research in elite‐level adult cohorts. Indeed, previous investigations typically report significant changes to CMJ movement strategy measures following high training and match loads, independently of changes to JH (Cormack et al., 2008; Gathercole et al., 2015a, 2015b). For example, Cormack and colleagues (Cormack et al., 2008) reported substantial (−16.7% and −17.1%) reductions to CMJ FT:CT and CMJ flight time (−3.6% and −3.5%) immediately post‐ and 24 h post‐AFL match play (Cormack et al., 2008); popularising the use of these measures in football (Akenhead et al., 2016). Disparity between our findings and those reported previously (Cormack et al., 2008) might be explained by higher movement variability in the U‐18 cohort herein (Cormack et al., 2008). Indeed, greater jump variability might be expected in less experienced football players, which in‐turn might serve to negate the sensitivity of movement strategy measures. However, we consider this unlikely, since our in‐house analysis reported good to excellent relative and absolute reliability for FT:CT and ED measures in a similar aged EPL academy cohort. Overall, our findings indicate that CMJ JH (flight time), eccentric peak force and eccentric deceleration rate of force development have greater merit in signalling match‐induced fatigue than FT:CT and ED in elite‐level young football players.
We also observed large (fatigue) and moderate (mood and muscle soreness) match‐induced reductions to ASRM subscale measures that had normalised at MD+2 (mood and muscle soreness) and MD+3 (fatigue) (Figure 2). Interestingly, the time‐course of restoration for these measures appears to be shorter than what has been reported for similar measures following senior professional EPL match play. For example, Thorpe and colleagues (Thorpe et al., 2016) reported match‐induced perturbations to perceived fatigue and muscle soreness for 96 h post‐match, and in a later investigation, reported a large correlation between perceived fatigue and match play high‐intensity running distance (Thorpe et al., 2015). Of note, the match running demands observed in the current investigation are similar to what has been reported in senior professional EPL match play (Reynolds et al., 2021) (Table 1). Consequently, we consider it unlikely that differences in the time‐course of perceptual recovery can be attributed to differences in the physical demands of match play between studies. Indeed, it is more likely that differences relate to the greater levels of holistic stress (i.e., summated physical and psychological stress) expected around senior professional‐compared to academy‐level EPL match play (Thorpe et al., 2016). Overall, our findings indicate that ASRM measures of perceived fatigue, mood and muscle soreness have good sensitivity to match‐induced fatigue in young football players and that they typically normalise by MD+2. These measures provide a rapidly deployable and highly accessible method for monitoring match‐induced fatigue responses in U‐18 EPL academy football players.
Notwithstanding the practical importance of our findings, we acknowledge several limitations to this investigation. Firstly, we only examined responses from competitive home games played by one team at their training facility owing to the location of equipment and personnel required to conduct this research. Secondly, we were unable to repeat measures at MD+1 post‐match due to team scheduling restraints. We acknowledge that the measurement at this time‐point might provide further insights relating to the time‐course of restoration of measures; however, this was not practically possible. Thirdly, though players only performed light recovery activities on MD+2 across the research period (i.e. <45 min, CR10 RPE <2), we acknowledge that the absence of training load data for this day in our statistical modelling might be considered as a limitation. Finally, we examined U‐18 male players and acknowledge that our findings might not be generalisable across female cohorts or younger (i.e., <U‐18) and older (i.e., senior professional) male cohorts. As such, we encourage similar research to be conducted in these groups.
5. PRACTICAL APPLICATIONS
To the author's knowledge, this is the first investigation to collectively examine the response of CMJ, isometric strength and perceptual monitoring measures to U‐18 EPL academy football match play. Our results further existing knowledge relating to the efficacy of these measures to signal match‐induced fatigue and the time‐course of neuromuscular and perceptual recovery post‐match. These findings can be used to inform variable selection in longitudinal player monitoring protocols and to help inform training load planning in practice.
Our results identify several neuromuscular performance test measures that should be considered to signal match‐induced fatigue in elite‐level young football players. These are peak isometric force for IABS, IADS and IPCS and maximal impulse for IABS and IADS, CMJ JH (flight time), CMJ eccentric peak force, CMJ eccentric deceleration rate of force development and ASRM measures of perceived fatigue, muscle soreness and mood. Contrary to popular use in practice, our results do not fully support the use of CMJ FT:CT or ED for this purpose.
Since IADS peak force remained compromised at MD+3, it is evident that not all players can achieve complete neuromuscular recovery by MD+3. This finding supports the use of post‐match recovery strategies targeting the resolution of muscle contractile function and the adjustment of planned training loads to accommodate individual player recovery thereafter. Since it might not be appropriate for all players to resume high‐volume and high‐intensity training on MD+3, we suggest the deployment of individualised player monitoring on MD+2 to check neuromuscular status, with repeated measures on MD+3 for players showing incomplete recovery. This might help to reduce training load errors and to mitigate player injury risk.
Our results highlight a particular vulnerability of the adductor muscle group to match‐induced fatigue. Where reasonably possible, this should be considered in training planning and strength and conditioning programing. For example, by utilising strategies to improve maximal strength and reduce fatigability in this muscle group.
6. CONCLUSION
Measures of peak isometric force (IABS, IADS and IPCS) and maximal impulse (IABS and IADS); CMJ JH (flight time), eccentric peak force and eccentric deceleration rate of force development and ASRM measures of perceived fatigue, muscle soreness and mood are sensitive to match‐induced fatigue in U‐18 EPL academy football players. Though match‐induced changes typically normalise within by MD+2 to MD+3, IADS peak force remained compromised at MD+3. Consequently, we conclude that U‐18 EPL academy football players might not achieve complete neuromuscular recovery within three days of match play.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflicts of interest.
ACKNOWLEDGEMENTS
This research was supported by a UEFA Research Grant Program (UEFA RGP) award.
REFERENCES
- Abbott, W. , Brickley G., and Smeeton N. J.. 2018. “Physical Demands of Playing Position within English Premier League Academy Soccer.” Journal of Human Sport and Exercise 13(2). 10.14198/jhse.2018.132.04. [DOI] [Google Scholar]
- Abbott, W. , Brickley G., Smeeton N. J., and Mills S.. 2018. “Individualizing Acceleration in English Premier League Academy Soccer Players.” The Journal of Strength & Conditioning Research 32(12): 3503–3510. 10.1519/jsc.0000000000002875. [DOI] [PubMed] [Google Scholar]
- Akenhead, R. , Hayes P. R., Thompson K. G., and French D.. 2013. “Diminutions of Acceleration and Deceleration Output during Professional Football Match Play.” Journal of Science and Medicine in Sport 16(6): 556–561. 10.1016/j.jsams.2012.12.005. [DOI] [PubMed] [Google Scholar]
- Akenhead, R. , and Nassis G. P.. 2016. “Training Load and Player Monitoring in High‐Level Football: Current Practice and Perceptions.” International Journal of Sports Physiology and Performance 11(5): 587–593. 10.1123/ijspp.2015-0331. [DOI] [PubMed] [Google Scholar]
- Akyildiz, Z. , Ocak Y., Clemente F. M., Birgonul Y., Günay M., and Nobari H.. 2022. “Monitoring the Post‐match Neuromuscular Fatigue of Young Turkish Football Players.” Scientific Reports 12(1): 13835. 10.1038/s41598-022-17831-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bishop, C. , Turner A., Jordan M., Harry J., Loturco I., Lake J., and Comfort P.. 2022. “A Framework to Guide Practitioners for Selecting Metrics during the Countermovement and Drop Jump Tests.” Strength and Conditioning Journal 44(4): 95–103. 10.1519/ssc.0000000000000677. [DOI] [Google Scholar]
- Bittencourt, N. F. N. , Meeuwisse W. H., Mendonca L. D., Nettel‐Aguirre A., Ocarino J. M., and Fonseca S. T.. 2016. “Complex Systems Approach for Sports Injuries: Moving from Risk Factor Identification to Injury Pattern Recognition‐Narrative Review and New Concept.” British Journal of Sports Medicine 50(21): 1309–1314. 10.1136/bjsports-2015-095850. [DOI] [PubMed] [Google Scholar]
- Bourne, M. N. , Williams M., Jackson J., Williams K. L., Timmins R. G., and Pizzari Tania. 2020. “Preseason Hip/Groin Strength and HAGOS Scores Are Associated with Subsequent Injury in Professional Male Soccer Players.” Journal of Orthopaedic & Sports Physical Therapy 50(5): 234–242. 10.2519/jospt.2020.9022. [DOI] [PubMed] [Google Scholar]
- Constantine, E. , Taberner M., Richter C., Willett M., and Cohen D. D.. 2019. “Isometric Posterior Chain Peak Force Recovery Response Following Match‐Play in Elite Youth Soccer Players: Associations with Relative Posterior Chain Strength.” Sports (Basel) 7(10): 218. 10.3390/sports7100218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cormack, S. J. , Newton R. U., and McGuigan M. R.. 2008. “Neuromuscular and Endocrine Responses of Elite Players to an Australian Rules Football Match.” International Journal of Sports Physiology and Performance 3(3): 359–374. 10.1123/ijspp.3.3.359. [DOI] [PubMed] [Google Scholar]
- Deely, C. , Tallent Jamie, Bennett Ross, Woodhead A., Goodall S., Thomas K., and Howatson G.. 2022. “Etiology and Recovery of Neuromuscular Function Following Academy Soccer Training.” Frontiers in Physiology 13: 911009. 10.3389/fphys.2022.911009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desmyttere, G. , Gaudet S., and Begon M.. 2019. “Test‐retest Reliability of a Hip Strength Assessment System in Varsity Soccer Players.” Physical Therapy in Sport 37: 138–143. 10.1016/j.ptsp.2019.03.013. [DOI] [PubMed] [Google Scholar]
- Eagles, A. N. , Sayers M. G. L., Bousson M., and Lovell D. I.. 2015. “Current Methodologies and Implications of Phase Identification of the Vertical Jump: A Systematic Review and Meta‐Analysis.” Sports Medicine 45(9): 1311–1323. 10.1007/s40279-015-0350-7. [DOI] [PubMed] [Google Scholar]
- Gathercole, R. , Sporer B., Stellingwerff T., and Sleivert G.. 2015a. “Alternative Countermovement‐Jump Analysis to Quantify Acute Neuromuscular Fatigue.” International Journal of Sports Physiology and Performance 10(1): 84–92. 10.1123/ijspp.2013-0413. [DOI] [PubMed] [Google Scholar]
- Gathercole, R. J. , Sporer B. C., Stellingwerff T., and Sleivert G. G.. 2015b. “Comparison of the Capacity of Different Jump and Sprint Field Tests to Detect Neuromuscular Fatigue.” The Journal of Strength & Conditioning Research 29(9): 2522–2531. 10.1519/jsc.0000000000000912. [DOI] [PubMed] [Google Scholar]
- Howarth, D. J. , Cohen D. D., McLean B. D., and Coutts A. J.. 2022. “Establishing the Noise: Interday Ecological Reliability of Countermovement Jump Variables in Professional Rugby Union Players.” The Journal of Strength & Conditioning Research 36(11): 3159–3166. 10.1519/jsc.0000000000004037. [DOI] [PubMed] [Google Scholar]
- Jones, S. , Clair Z., Wrigley R., Mullen R., Andersen T. E., and Williams M.. 2021. “Strength Development and Non‐contact Lower Limb Injury in Academy Footballers across Age Groups.” Scandinavian Journal of Medicine & Science in Sports 31(3): 679–690. 10.1111/sms.13889. [DOI] [PubMed] [Google Scholar]
- Jones, S. , Mullen R., Clair Z., Wrigley R., Andersen T. E., and Williams M.. 2021. “Field Based Lower Limb Strength Tests Provide Insight into Sprint and Change of Direction Ability in Academy Footballers.” Scandinavian Journal of Medicine & Science in Sports 31(12): 2178–2186. 10.1111/sms.14039. [DOI] [PubMed] [Google Scholar]
- Kelly, D. M. , Strudwick A. J., Atkinson G., Drust B., and Gregson W.. 2019. “Quantification of Training and Match‐Load Distribution across a Season in Elite English Premier League Soccer Players.” Science and Medicine in Football 4: 1–9. 10.1080/24733938.2019.1651934. [DOI] [Google Scholar]
- Materne, O. , Chamari K., Farooq A., Weir A., Hölmich P., Bahr R., Greig M., and McNaughton L. R.. 2021. “Injury Incidence and Burden in a Youth Elite Football Academy: a Four‐Season Prospective Study of 551 Players Aged from under 9 to under 19 Years.” British Journal of Sports Medicine 55(9): 493–500. 10.1136/bjsports-2020-102859. [DOI] [PubMed] [Google Scholar]
- Matinlauri, A. , Alcaraz P. E., Freitas T. T., Mendiguchia J., Abedin‐Maghanaki A., Castillo A., Martínez‐Ruiz E., Carlos‐Vivas J., and Cohen D. D.. 2019. “A Comparison of the Isometric Force Fatigue‐Recovery Profile in Two Posterior Chain Lower Limb Tests Following Simulated Soccer Competition.” PLoS One 14(5): e0206561. 10.1371/journal.pone.0206561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCall, A. , Carling C., Davison M., Nedelec M., Le Gall F., Berthoin S., and Dupont G.. 2015. “Injury Risk Factors, Screening Tests and Preventative Strategies: a Systematic Review of the Evidence that Underpins the Perceptions and Practices of 44 Football (Soccer) Teams from Various Premier Leagues.” British Journal of Sports Medicine 49(9): 583–589. 10.1136/bjsports-2014-094104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCall, A. , Nedelec M., Carling C., Le Gall F., Berthoin S., and Dupont G.. 2015. “Reliability and Sensitivity of a Simple Isometric Posterior Lower Limb Muscle Test in Professional Football Players.” Journal of Sports Sciences 33(12): 1298–1304. 10.1080/02640414.2015.1022579. [DOI] [PubMed] [Google Scholar]
- McLean, B. D. , Coutts A. J., Kelly V., McGuigan M. R., and Cormack S. J.. 2010. “Neuromuscular, Endocrine, and Perceptual Fatigue Responses during Different Length Between‐Match Microcycles in Professional Rugby League Players.” International Journal of Sports Physiology and Performance 5(3): 367–383. 10.1123/ijspp.5.3.367. [DOI] [PubMed] [Google Scholar]
- Meeusen, R. , Duclos M., Foster C., Fry A., Gleeson M., Nieman D., Raglin J. et al. 2013. “Prevention, Diagnosis, and Treatment of the Overtraining Syndrome: Joint Consensus Statement of the European College of Sport Science and the American College of Sports Medicine.” Medicine & Science in Sports & Exercise 45(1): 186–205. 10.1249/mss.0b013e318279a10a [DOI] [PubMed] [Google Scholar]
- O'Brien, M. , Bourne M., Heerey J., Timmins R. G., and Pizzari T.. 2019. “A Novel Device to Assess Hip Strength: Concurrent Validity and Normative Values in Male Athletes.” Physical Therapy in Sport 35: 63–68. [DOI] [PubMed] [Google Scholar]
- Reynolds, J. , Connor M., Jamil M., and Beato M.. 2021. “Quantifying and Comparing the Match Demands of U18, U23, and 1ST Team English Professional Soccer Players.” Frontiers in Physiology 12: 706451. 10.3389/fphys.2021.706451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan, S. , Kempton T., Pacecca E., and Coutts A. J.. 2019. “Measurement Properties of an Adductor Strength‐Assessment System in Professional Australian Footballers.” International Journal of Sports Physiology and Performance 14(2): 256–259. 10.1123/ijspp.2018-0264. [DOI] [PubMed] [Google Scholar]
- Salter, J. , Cresswell R., and Forsdyke D.. 2021. “The Impact of Simulated Soccer Match‐Play on Hip and Hamstring Strength in Academy Soccer Players.” Science and Medicine in Football 6(4): 1–8. 10.1080/24733938.2021.1973080. [DOI] [PubMed] [Google Scholar]
- Salter, J. , De Ste Croix M. B. A., Hughes J. D., Weston M., and Towlson C.. 2021. “Monitoring Practices of Training Load and Biological Maturity in UK Soccer Academies.” International Journal of Sports Physiology and Performance 16(3): 395–406. 10.1123/ijspp.2019-0624. [DOI] [PubMed] [Google Scholar]
- Saw, A. E. , Main L. C., and Gastin P. B.. 2016. “Monitoring the Athlete Training Response: Subjective Self‐Reported Measures Trump Commonly Used Objective Measures: a Systematic Review.” British Journal of Sports Medicine 50(5): 281–291. 10.1136/bjsports-2015-094758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwellnus, M. , Soligard T., Alonso J.‐M., Bahr R., Clarsen B., Dijkstra H. P., Gabbett T. J., et al. 2016. “How Much Is Too Much? (Part 2) International Olympic Committee Consensus Statement on Load in Sport and Risk of Illness.” British Journal of Sports Medicine 50(17): 1043–1052. 10.1136/bjsports-2016-096572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soligard, T. , Schwellnus M., Alonso J.‐M., Bahr R., Clarsen B., Dijkstra H. Paul, Gabbett T., et al. 2016. “How Much Is Too Much? (Part 1) International Olympic Committee Consensus Statement on Load in Sport and Risk of Injury.” British Journal of Sports Medicine 50(17): 1030–1041. 10.1136/bjsports-2016-096581. [DOI] [PubMed] [Google Scholar]
- Springham, M. , Williams S., Waldron M., Strudwick A. J., Mclellan C., and Newton R. U.. 2021. “Salivary Immunoendocrine and Self‐Report Monitoring Profiles across an Elite‐Level Professional Football Season.” Medicine & Science in Sports & Exercise 53(5): 918–927. 10.1249/mss.0000000000002553. [DOI] [PubMed] [Google Scholar]
- Thomas, K. , Dent J., Howatson G., and Goodall S.. 2017. “Etiology and Recovery of Neuromuscular Fatigue after Simulated Soccer Match Play.” Medicine & Science in Sports & Exercise 49(5): 955–964. 10.1249/mss.0000000000001196. [DOI] [PubMed] [Google Scholar]
- Thorpe, R. T. , Strudwick A. J., Buchheit M., Atkinson G., Drust B., and Gregson W.. 2015. “Monitoring Fatigue during the In‐Season Competitive Phase in Elite Soccer Players.” International Journal of Sports Physiology and Performance 10(8): 958–964. 10.1123/ijspp.2015-0004. [DOI] [PubMed] [Google Scholar]
- Thorpe, R. T. , Strudwick A. J., Buchheit M., Atkinson G., Drust B., and Gregson W.. 2016. “Tracking Morning Fatigue Status across In‐Season Training Weeks in Elite Soccer Players.” International Journal of Sports Physiology and Performance 11(7): 947–952. 10.1123/ijspp.2015-0490. [DOI] [PubMed] [Google Scholar]
- Thorpe, R. T. , Strudwick A. J., Buchheit M., Atkinson G., Drust B., and Gregson W.. 2017. “The Influence of Changes in Acute Training Load on Daily Sensitivity of Morning‐Measured Fatigue Variables in Elite Soccer Players.” International Journal of Sports Physiology and Performance 12(Suppl 2): S2107–S2113. 10.1123/ijspp.2016-0433. [DOI] [PubMed] [Google Scholar]
- Verschueren, J. , Tassignon B., De Pauw K., Proost M., Teugels A., Van Cutsem J., Roelands B., Verhagen E., and Meeusen R.. 2020. “Does Acute Fatigue Negatively Affect Intrinsic Risk Factors of the Lower Extremity Injury Risk Profile? A Systematic and Critical Review.” Sports Medicine 50(4): 767–784. 10.1007/s40279-019-01235-1. [DOI] [PubMed] [Google Scholar]
- Wik, E. H. , Lolli L., Chamari K., Materne O., Di Salvo V., Gregson W., and Bahr R.. 2021. “Injury Patterns Differ with Age in Male Youth Football: a Four‐Season Prospective Study of 1111 Time‐Loss Injuries in an Elite National Academy.” British Journal of Sports Medicine 55(14): 794–800. 10.1136/bjsports-2020-103430. [DOI] [PubMed] [Google Scholar]