

Abstract
Background
Recurrent respiratory papillomatosis (RRP) is a chronic condition caused primarily by human papilloma virus (HPV) types 6 and 11, leading to recurrent growths in the respiratory tract. These types of papilloma can cause significant morbidity due to airway obstruction, often requiring frequent surgical interventions. Traditional treatments, including surgical removal and adjunctive therapies like antivirals and immune modulators, often fail to prevent recurrence, impacting the patient’s quality of life.
Case description
This report presents a 25-year-old female with a long-standing history of RRP, diagnosed at age 2. Despite numerous interventions, including CO2 laser ablations, interferon therapy, HPV vaccination, and a laryngotomy with tracheal reconstruction, the patient continued to experience severe airway obstruction requiring frequent surgeries. In 2023, intravenous therapy with bevacizumab, vascular endothelial growth factor inhibitor was introduced, leading to a significant reduction in the frequency of surgical interventions from 8 to 4 per year. This reduction improved the patient’s respiratory function and quality of life, highlighting bevacizumab’s therapeutic potential.
Conclusion
The case underscores the debilitating nature of RRP and the challenges of its management. Bevacizumab, by targeting vascular endothelial growth factor (VEGF), has shown promise in reducing papilloma growth and the need for frequent surgeries. This case supports the inclusion of bevacizumab as an adjunctive therapy in RRP treatment, warranting further research to confirm its long-term efficacy and safety.
LEARNING POINTS
Recurrent respiratory papillomatosis is a rare and complex disease that severely impacts patients’ quality of life.
This case report demonstrates that bevacizumab can significantly reduce surgical interventions in recurrent respiratory papillomatosis (RRP), offering a promising treatment that improves management of this chronic condition.
Bevacizumab, already used in treating various diseases by targeting VEGF, shows promise in managing RRP as well, highlighting its potential across multiple conditions and expanding its therapeutic versatility.
Keywords: Respiratory papillomatosis, bevacizumab, bronchoscopy, VEGF
INTRODUCTION
Recurrent respiratory papillomatosis (RRP) is characterized by recurrent growth of papilloma in the respiratory tract, primarily caused by human papilloma virus (HPV) types 6 and 11 The viruses are transmitted to the host through direct contact, often during birth from an infected mother[1]. These lesions can lead to significant morbidity due to airway obstruction and severe cases require frequent surgical interventions to maintain airway patency. The infection is persistent and can cause recurrent growth of papilloma even after surgical removal, due to the persistence of HPV deoxyribonucleic acid (DNA) in the basal epithelial cells. Papilloma typically causes hoarseness, chronic cough, and respiratory distress due to airway obstruction. Although rare, there is a risk of malignant transformation to squamous cell carcinoma, especially in cases associated with HPV types other than 6 and 11 or in the presence of co-factors[2].
The primary treatment is surgical removal of the papilloma to maintain airway patency and vocal function. Adjunctive treatments include antiviral drugs, immune modulators, and vaccines to reduce recurrence rates. This case report describes a 25-year-old patient with a long history of RRP, emphasizing the impact of therapy with bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor, on reducing the frequency of surgical interventions.
CASE DESCRIPTION
The patient, a 25-year-old female, was born with a cleft palate and lip. At the age of 2, she presented with hoarseness and troubled breathing. Upon evaluation, she was diagnosed with juvenile RRP. Her early childhood was marked by frequent respiratory distress and recurrent bronchoscopies with CO2 laser ablations to remove papilloma obstructing the airway.
As the patient grew older, the frequency of surgical interventions remained high, with up to 20 CO2 laser ablations per year to manage the papillomatous growths. The repeated surgical interventions led to significant structural changes in her larynx, necessitating a tracheostomy at the age of 3, to protect her airway.
During childhood, the patient received subcutaneous interferon therapy and therapy with intralesional cidofovir as part of her treatment regimen. However, the interferon therapy was discontinued due to side effects, including delay of growth. Despite these interventions, the patient continued to experience severe recurrent dyspnoea due to obstructive lesions (Fig. 1).
Figure 1.
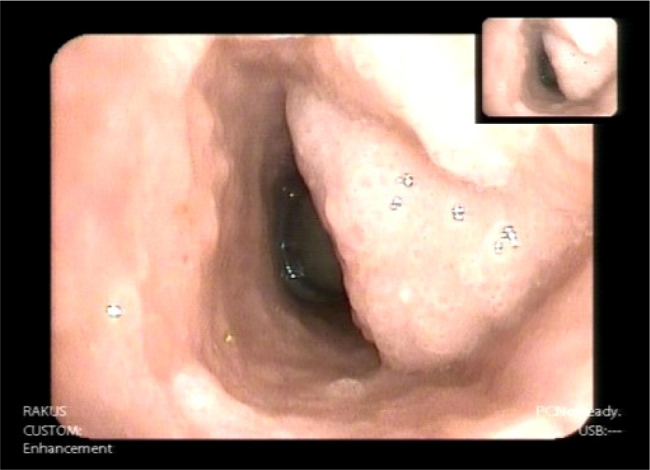
Papillomatous tissue in the trachea.
At the age of 12, the patient received an HPV vaccination, which temporarily slowed the progression of her papillomatosis. Unfortunately, the symptoms eventually recurred, and the need for frequent surgical interventions persisted. Due to obstruction of small bronchiole with papillomtous tissue, the patient developed cystic lesions in her lungs, complicating her overall respiratory health (Fig. 2).
Figure 2.

Computed tomography scan of the patients’ lungs, showing multiple cystic lesions.
At the age of 20, the patient underwent a successful laryngotomy with reconstruction of the larynx. During this procedure, the dorsal wall of her trachea was reconstructed with a fascial flap, and a silicone stent was placed below the larynx to support healing and prevent tracheal collapse. Following this surgery, her tracheostomy was closed, and she regained the ability to speak. Despite this significant intervention, she continued to require up to 8 bronchoscopies with argon plasma coagulation per year due to ongoing obstruction of the trachea, below the distal end of the silicone stent, caused by papillomatous tissue (Fig. 3).
Figure 3.
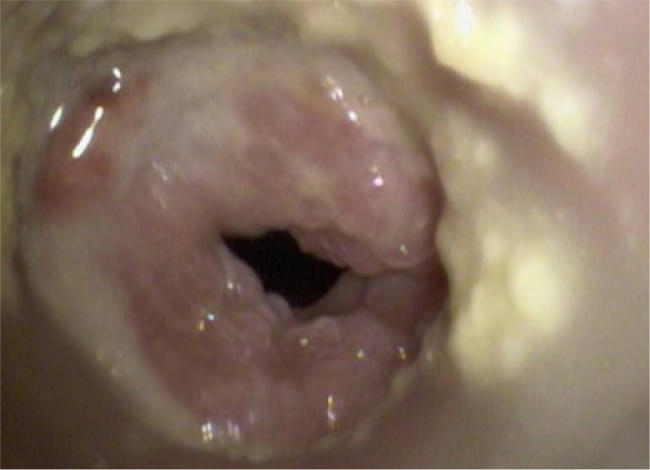
Papillomatous tissue in the trachea below silicone stent.
A biopsy of the lesions was performed, and the tissue was tested for HPV DNA using polymerase chain reaction (PCR), which identified the presence of HPV type 11.
In 2023, the patient was presented with the possibility of therapy with intravenous bevacizumab. As the patient agreed, therapy was started, administrating 600 mg (10 mg/kg) of bevacizumab every 3 weeks. Since the initiation of bevacizumab therapy, the patient has experienced a significant reduction in the frequency of bronchoscopies with argon plasma coagulations, from 8 to 4 per year. This reduction has had a profound impact on the patient’s quality of life, decreasing the morbidity associated with frequent surgeries and improving respiratory function. Recently, the stent was removed from the trachea as it was suspected of causing local irritation of mucous tissue and tissue proliferation.
DISCUSSION
The management of RRP is challenging due to the recurrent nature of the disease and the need for frequent surgical interventions. This case highlights the potential of bevacizumab as an adjunctive therapy in reducing the burden of disease. Bevacizumab, a recombinant humanized monoclonal antibody targeting human VEGF-A, has shown promising efficacy in treating RRP. In this condition, the overexpression of VEGF contributes to the proliferation and vascularization of papillomas. Bevacizumab binds to VEGF, inhibiting its interaction with VEGF receptors on endothelial cells, thereby reducing angiogenesis and tumour growth. Clinical observations have demonstrated significant regression of papillomas and symptomatic relief in patients with RRP following bevacizumab treatment, highlighting its potential as a therapeutic option for this challenging condition[3].
CONCLUSION
Before the introduction of bevacizumab, the patient’s quality of life was severely impacted by the need for frequent surgeries and the complications associated with RRP. The reduction in surgical interventions with bevacizumab therapy has not only improved the patient’s quality of life but also provided insights into the pathophysiology of RRP and the role of VEGF in its progression. The successful outcome in this case aligns with other reports in the literature[4], suggesting that bevacizumab can be a valuable addition to the therapeutic arsenal for RRP.
Footnotes
Conflicts of Interests: The Authors declare that there are no competing interests.
Patient Consent: The patient has given an informed consent.
REFERENCES
- 1.Ouda Amr Mohamed, Elsabagh Ahmed Adel, Elmakaty Ibrahim Mohamed, Gupta Ishita, Vranic Semir, Al-Thawadim Hamda, et al. HPV and Recurrent Respiratory Papillomatosis: A Brief Review. Life. 2021;11:1279. doi: 10.3390/life11111279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cem Sievers Yvette, Robbins Ke, Bai Xinping, Yang Paul E, Friedman Clavijo Jay, et al. Comprehensive multiomic characterization of human papillomavirus-driven recurrent respiratory papillomatosis reveals distinct molecular subtypes. Communications Biology. 2021;4:1416. doi: 10.1038/s42003-021-02942-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lepine Charles, Leboulanger Nicolas, Badoual Cécile. Juvenile onset recurrent respiratory papillomatosis: What do we know in 2024? Tumour Virus Research. 2024;17:200281. doi: 10.1016/j.tvr.2024.200281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pogoda Louis, Ziylan Fuat, Smeeing Diederik PJ, Dikkers Frederik G, Rinkel Rico NPM. Bevacizumab as treatment option for recurrent respiratory papillomatosis: a systematic review. Eur Arch Otorhinolaryngol. 2022;279:4229–4240. doi: 10.1007/s00405-022-07388-6. [DOI] [PMC free article] [PubMed] [Google Scholar]