

Abstract
Aim: To assess a patient empowerment program (PEP) for children/adolescents with primary immunodeficiency (PID) on IgG replacement therapy regarding quality of life (QoL) in patients and proxy.
Patients & methods: Health-related QoL was assessed using KIDSCREEN-27 and DISABKIDS-37 before and 6 months after PID-PEP kids in 19 children/adolescents and their parents.
Results: The following three dimensions of the KIDSCREEN-27 significantly increased in children/adolescents after PID-PEP kids as compared with baseline: Psychological Well-Being, Parents & Autonomy and School Environment. Total DISABKIDS-37 index, as well as 5 of the 6 DISABKIDS-37 dimensions, significantly increased, in other words, Independence, Emotion, Social Inclusion, Social Exclusion and Physical. Evaluation of proxy instruments showed comparable results.
Conclusion: PID-PEP kids significantly improved QoL in patients with PID.
Keywords: : DISABKIDS-37, education program, IgG replacement therapy, inborn errors of immunity, KIDSCREEN-27, patient empowerment program, primary immunodeficiency, quality of life
Plain Language Summary
What is this study about?
This study evaluated a patient empowerment program (PEP) for children and adolescents with primary immunodeficiency (PID) on immunoglobulin replacement therapy. The goal was to see if the program improved quality of life (QoL). Two commonly administered questionnaires were used to measure QoL before and 6 months after participating in the program.
What were the results?
Significant improvements were found in several dimensions including Psychological Well-Being, Parents & Autonomy and School Environment. Additionally, overall QoL scores and dimensions such as Independence, Emotion, Social Inclusion, Social Exclusion and Physical also improved. Assessments by the parents confirmed these findings.
What do the results mean?
The PID-PEP kids program significantly improved the QoL for these young patients.
Plain language summary
Article highlights.
No study so far has assessed whether a patient empowerment program (PEP) for children and adolescents with primary immunodeficiency (PID) on IgG replacement therapy improves quality of life (QoL).
Patients & PID-PEP kids
Changes in QoL before and 6 months after participation in PID-PEP for children/adolescents (PID-PEP kids) were evaluated in the present study in 19 children/adolescents with PID and their parents.
KIDSCREEN-27 & DISABKIDS-37 before & at 6 months after PID-PEP kids
Health-related QoL was measured using KIDSCREEN-27 and DISABKIDS-37 questionnaires.
Several KIDSCREEN-27 dimensions significantly improve after PID-PEP kids
In KIDSCREEN-27, significant improvements were found in Psychological Well-Being, Parents & Autonomy and School Environment.
Parents' assessments showed comparable results as in children/adolescents.
Total & several DISABKIDS-37 dimensions significantly improve after PID-PEP kids
In DISABKIDS-37, the overall QoL index and specific dimensions such as Independence, Emotion, Social Inclusion, Social Exclusion and Physical showed significant improvements.
Parents' assessments showed comparable results as in children/adolescents.
Discussion
This is the first study to assess changes in QoL in children/adolescents with PID after participating in a PEP.
Conclusion
The PID-PEP kids program significantly improved QoL in children/adolescents with PID.
Larger studies with an adequate control group are necessary to confirm these findings.
1. Background
Primary immunodeficiency (PID), recently termed Inborn Errors of Immunity, comprises a rare and heterogeneous group of more than 485 genetically defined diseases [1]. Various parts of the immune system can be affected resulting in an increased susceptibility to infections in the majority of patients [2]. B-cell development and/or maturation defects that result in primary antibody deficiency form the largest subgroup of PID [2]. Recurrent respiratory and gastrointestinal tract infections significantly contribute to increased morbidity and mortality in these patients [3]. Intravenous or subcutaneous immunoglobulin G (IgG) replacement reduces the incidence of infections [3]. PID patients have a significantly decreased quality of life (QoL) not only compared with healthy controls but also to patients with other chronic diseases [4,5].
QoL in children/adolescents can be evaluated in clinical settings by various instruments. KIDSCREEN-27 is a 27-item questionnaire that assesses the subjective health, as well as the psychological, mental and social well-being of children/adolescents between 8 and 18 years of age [6–8]. Both healthy and ill children/adolescents can complete the KIDSCREEN-27 themselves (self-assessment) [6–8]. A corresponding parent version enables proxy assessment by parents or other care givers [6–8]. In contrast to KIDSCREEN-27, DISABKIDS-37 has been exclusively developed for children/adolescents with chronic medical conditions [9,10]. It is a generic, non-disease-specific QoL assessment tool comprising 37 items which has been validated within a European cross-cultural multi-centre study [9,10]. Similar to KIDSCREEN-27, DISABKIDS-37 enables self- and proxy assessment [9,10]. More recently, cross-nationally tested condition-specific modules of the DISABKIDS-37 were developed for asthma, juvenile idiopathic arthritis, atopic dermatitis, cerebral palsy, cystic fibrosis, diabetes mellitus and epilepsy, but not for PID [11].
There is broad consensus that QoL in PID patients is significantly reduced due to recurrent infectious episodes, other chronic health issues, social determinants and stress [4,5]. Patient empowerment programs (PEP) may improve QoL by providing patients with more control regarding decisions and treatment options affecting their health [12]. In agreement with this hypothesis, it was recently reported that QoL and treatment satisfaction significantly improved 6 months after participating in a primary immunodeficiency-patient empowerment program (PID-PEP) in 26 adult PID patients as compared with baseline levels [13]. However, no study so far has assessed whether PID-PEP improves QoL also in children/adolescents. Therefore, changes in QoL before and 6 months after participation in PID-PEP for children/adolescents (PID-PEP kids) were evaluated in the present study in 19 children/adolescents with PID. We hypothesized, that PID-PEP kids would significantly improve QoL assessed by both KIDSCREEN-27 and DISABKIDS-37 and in both children/adolescents and their caregivers.
2. Patients & measurements
2.1. Patients & PID-PEP kids
PID-PEP kids was established in 2007 in Germany by members of the Task force Paediatric Immunology (Arbeitsgemeinschaft Pädiatrische Immunologie, API). The program for adults has been described in more detail recently [13]. In brief, the program is provided in a seminar venue as a weekend course by a multidisciplinary team consisting of physicians specialized in PID, psychologists and nurses specialized for patients with PID and IgG replacement therapy. It comprises three general modules and three disease-specific modules. The German curriculum of PID-PEP kids is available online [14].
Before and 6 months after participating in PID-PEP kids, QoL was assessed in 19 children/adolescents with PID receiving IgG replacement. No family with more than one affected child/adolescent was evaluated in the current study. PID-PEP kids is established for complete families, in other words, the patients, as well as their non-PID-affected siblings and parents. However, QoL questionnaires were completed exclusively by the patients and one parent at all time points. The study was approved by the ethics committee of Hannover Medical School (ethical approval number: 640-2009) and all subjects gave written informed consent before participating. Table 1 summarizes baseline characteristics of the study population.
Table 1.
Baseline characteristics of the study population.
| All subjects (n = 19) | |
|---|---|
| Age (years) Gender – Male – Female |
10 (3) 12 (63) 7 (37) |
| Duration of IgG treatment (years) | 3 (3) |
| Ethnic background – Caucasian – Asian – Other |
17 (90) 1 (5) 1 (5) |
| IgG treatment ever and current – Intravenous and subcutaneous – Intravenous – Subcutaneous |
9 (47) 5 (26) 5 (26) |
| IgG treatment location ever and current – Hospital/ outpatient care unit – Hospital/ at home – At home |
5 (26) 13 (68) 1 (5) |
| Type of immunodeficiency – CVID – CID – APDS – ARA – Complement deficiency – Specific antibody deficiency – XLF/Cernunnos deficiency – Other primary antibody deficiency |
5 (26) 3 (16) 3 (16) 1 (5) 1 (5) 1 (5) 1 (5) 4 (21) |
Values for mean (SD) or total number (percentage) are shown.
APDS: Activated PI3K delta syndrome; ARA: Autosomal recessive agammaglobulinaemia; CID: Combined immunodeficiency; CVID: Common variable immune deficiency; XLF: XRCC4-like factor.
2.2. KIDSCREEN-27 & DISABKIDS-37 before & at 6 months after PID-PEP kids
KIDSCREEN-27 is a well-known, easy-to-use, generic multi-item scale QoL instrument for children/adolescents measuring five separate dimensions: physical well-being, psychological well-being, parents & autonomy, social support & peers and school environment [6–8]. These KIDSCREEN-27 health dimensions were transformed to a 0 (=worst status) to 100 (=best status) scale [6–8]. The KIDSCREEN-27 was completed by patients, as well as their parents/proxy, before and 6 months after PID-PEP kids.
DISABKIDS-37 is another well-known, easy-to-use, generic multi-item scale QoL instrument which has been exclusively developed for children/adolescents with chronic medical conditions [9,10]. It assesses six separate dimensions: independence, emotion, social inclusion, social exclusion, physical and medication [9,10]. Furthermore, a total DISABKIDS-37 index was calculated as a summary measure over all 37 items. The DISABKIDS-37 dimensions and the total index were transformed to a 0 (=worst status) to 100 (=best status) scale [9,10]. For patients younger than 8 years (n = 4), KIDSCREEN-27 and DISABKIDS-37 were only completed by parents/proxy. Two children/adolescents did not complete these questionnaires. Proxy evaluation was available for all 19 patients for KIDSCREEN-27 and for 18 patients for DISABKIDS-37.
2.3. Statistical analysis
IBM SPSS software version 29 (IBM, Armonk, NY) was used in all statistical analyses. Differences before and at 6 months after PID-PEP kids were assessed by Wilcoxon signed-rank test. A p-value of <0.05 was considered statistically significant in all analyses.
3. Results
3.1. Several KIDSCREEN-27 dimensions significantly improve after PID-PEP kids
In children/adolescents, mean (standard deviation (SD)) values increased significantly 6 months after PID-PEP kids as compared with baseline in three dimensions, in other words, Psychological Well-Being increased from 52 (13) to 56 (14) (p = 0.017), Parents & Autonomy from 53 (13) to 57 (12) (p = 0.007) and School Environment from 52 (16) to 57 (12) (p = 0.012) (Table 2). Mean values for the other two dimensions, in other words, Physical Well-Being and Social Support & Peers, also numerically increased. However, these changes did not reach statistical significance (Table 2).
Table 2.
KIDSCREEN-27 dimensions in children/adolescents and parents/proxy before and 6 months after PID-PEP kids.
| Before | After | p-value | |
|---|---|---|---|
| Children/adolescents (n = 13) | |||
| Physical Well-Being | 48 (15) | 50 (11) | 0.110 |
| Psychological Well-Being | 52 (13) | 56 (14) | 0.017 |
| Parents & Autonomy | 53 (13) | 57 (12) | 0.007 |
| Social Support & Peers | 49 (15) | 53 (10) | 0.168 |
| School Environment | 52 (16) | 57 (12) | 0.012 |
| Parents/proxy (n = 19) | |||
| Physical Well-Being | 43 (14) | 45 (10) | 0.313 |
| Psychological Well-Being | 46 (11) | 50 (12) | 0.033 |
| Parents & Autonomy | 54 (6) | 58 (9) | 0.033 |
| Social Support & Peers | 46 (12) | 53 (10) | 0.011 |
| School Environment | 50 (10) | 53 (10) | 0.116 |
Values for mean (SD) and number of subjects being evaluated (n) are shown. Statistical significance was tested by Wilcoxon signed-rank test and bold values indicate p < 0.05.
In line with the findings in children/adolescents, mean (SD) dimensions for Psychological Well-Being and Parents & Autonomy also significantly increased from 46 (11) to 50 (12) (p = 0.033) and from 54 (6) to 58 (9) (p = 0.033), respectively, in the proxy assessments (Table 2). Mean (SD) value for Social Support & Peers also significantly increased from 46 (12) to 53 (10) (p = 0.011, Table 2). In contrast, mean values for Physical Well-Being and School Environment numerically increased but did not reach statistical significance (Table 2).
3.2. Total & several DISABKIDS-37 dimensions significantly improve after PID-PEP kids
In children/adolescents, the mean (SD) total DISABKIDS-37 index significantly increased from 70 (20) at baseline to 78 (17) 6 months after PID-PEP kids (p = 0.006, Table 3). Mean (SD) values for five of the six DISABKIDS-37 dimensions significantly increased after PID-PEP kids in children/adolescents, in other words, Independence (70 (21) to 77 (17), p = 0.032), Emotion (71 (26) to 79 (17), p = 0.036), Social Inclusion (68 (20) to 78 (14), p = 0.002), Social Exclusion (78 (26) to 84 (21), p = 0.007) and Physical (69 (27) to 79 (21), p = 0.012) (Table 3). Medication increased numerically but not significantly after PID-PEP kids in children/adolescents (Table 3).
Table 3.
DISABKIDS-37 dimensions in children/adolescents and parents/proxy before and 6 months after PID-PEP kids.
| Before | After | p-value | |
|---|---|---|---|
| Children/adolescents (n = 13) | |||
| Total | 70 (20) | 78 (17) | 0.006 |
| Independence | 70 (21) | 77 (17) | 0.032 |
| Emotion | 71 (26) | 79 (17) | 0.036 |
| Social Inclusion | 68 (20) | 78 (14) | 0.002 |
| Social Exclusion | 78 (26) | 84 (21) | 0.007 |
| Physical | 69 (27) | 79 (21) | 0.012 |
| Medication | 65 (27) | 72 (22) | 0.091 |
| Parents/proxy (n = 18) | |||
| Total | 69 (17) | 74 (18) | 0.020 |
| Independence | 77 (15) | 76 (17) | 0.849 |
| Emotion | 67 (22) | 76 (17) | 0.022 |
| Social Inclusion | 66 (17) | 68 (23) | 0.392 |
| Social Exclusion | 78 (18) | 81 (21) | 0.074 |
| Physical | 67 (20) | 73 (19) | 0.050 |
| Medication | 57 (24) | 69 (21) | 0.003 |
Values for mean (SD) are shown. Statistical significance was tested by Wilcoxon signed-rank test and bold values indicate p < 0.05.
In line with the findings in children/adolescents, the mean (SD) total DISABKIDS-37 index significantly increased from 69 (17) at baseline to 74 (18) 6 months after PID-PEP kids in the proxy assessment (p = 0.020, Table 3). Furthermore, mean (SD) values for Emotion and Medication significantly increased from 67 (22) to 76 (17) (p = 0.022) and 57 (24) to 69 (21) (p = 0.003), respectively (Table 3). All other dimensions in the proxy assessment except Independence numerically increased after PID-PEP kids. However, statistical significance was not reached (Table 3).
4. Discussion
To the best of our knowledge, this is the first study to assess changes in QoL in children/adolescents with PID after participating in a PEP (PID-PEP kids). In our study, various dimensions of the KIDSCREEN-27 and the DISABKIDS-37 significantly improved after PID-PEP kids as compared with baseline prior to the program. Since almost all dimensions displayed higher mean values after the program, statistical significance may have not been reached due to the relatively small group size. The concordant results between self and proxy reports suggest a relatively homogeneous process that affected patients and parents alike.
In the present study, both QoL assessment tools show significant improvement in children/adolescents, as well as in parents/proxy, for various dimensions. Of note, the total DISABKIDS-37 index significantly increases in both groups. In contrast to our current findings, other studies present more heterogeneous results between children/adolescents and their caregivers [15–17]. Differences in diseases, type of intervention and observational periods might well explain these different findings.
Our study supports recent evidence that 6 weeks after participation in a PEP, health-related QoL is improved in children with chronic asthma and their families [18]. Furthermore, beneficial effects 6 weeks after participation in PEP have also been reported for rare chronic conditions including cystic fibrosis, phenylketonuria and chronic inflammatory bowel disease [15]. Our study extends the observed improvement of health related QoL to a substantially longer period of time after the PEP, suggesting that this healthcare intervention may have a relatively long-lasting effect on everyday life of the patients and their families. To our knowledge, there is no other study in rare chronic conditions that has assessed the effect of a PEP for a period of 6 months or beyond.
In recent years, patient-centered clinical medicine has increased its focus on well-being of patients [12]. QoL is an important complement to more traditional end points such as mortality and morbidity. It is important to note in this context that QoL assessed by the KIDSCREEN-27 is markedly lower in all five dimensions for self, as well as proxy, assessment in children/adolescents with PID as compared with an age-related normal German population-representative control group (Figure 1) [19]. The current findings of a beneficial effect by PEP supports the integration of PEP into the services offered by healthcare providers. It is important to note that PID-PEP for all age groups is now partly covered by German public health insurance following a thorough validation of beneficial effects that included the present and a recent [13] study. The cost-effectiveness of PID-PEP kids should be elucidated in future cost-benefit analyses.
Figure 1.
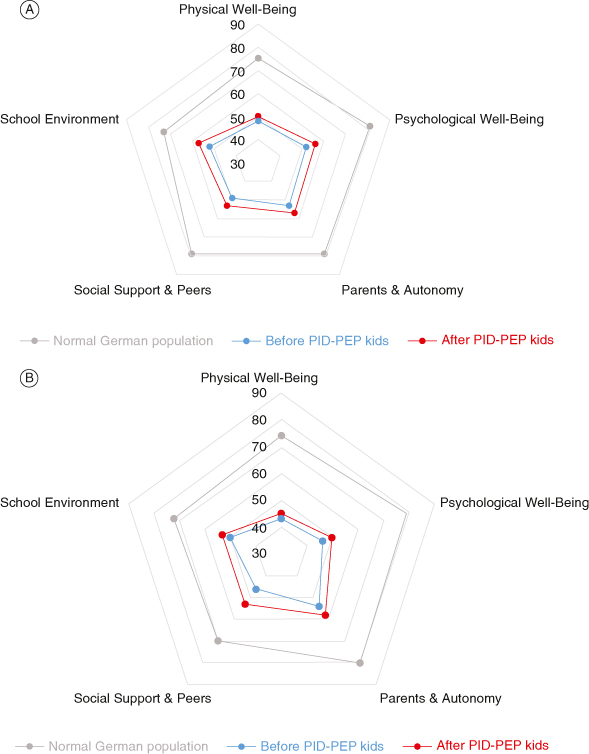
Mean KIDSCREEN-27 dimensions in a German population-representative study, as well as in (A) children/adolescents with PID (n = 13) and (B) their parents/proxy (n = 19) before and 6 months after PID-PEP kids.
Data taken from [19].
A strength of the current study is a longer follow-up period of 6 months which indicates that PID-PEP kids might have sustainable effects on QoL. However, there are limitations as to the lack of a control group, e.g., PID patients only receiving written advice or being on a waiting list and a rather small number of patients which is due to the low prevalence of PID. QoL benefits of PID-PEP kids can, therefore, not be proven by the current results. However, over time QoL dimensions decrease in patients with well-defined antibody deficiency syndromes, in other words, Common Variable Immune Deficiencies [4]. Future multi-center studies evaluating larger patient cohorts with an adequate control group over a longer period of time will provide even more definitive conclusions. Furthermore, DISABKIDS-37 is not validated for patients with Inborn Errors of Immunity and this could mislead the QoL results of these patients.
5. Conclusion
We show for the first time that QoL in children/adolescents with PID significantly improves after PID-PEP kids. Larger studies with an adequate control group are necessary to confirm these findings. Future studies need to address whether the positive effects of PID-PEP kids are maintained over an even longer period of time and whether QoL can be further increased by repeated participation in PID-PEP kids.
Acknowledgments
We thank all participating patients and their families for supporting this study. This paper is dedicated to our dear colleague and beloved friend G Notheis who passed away during preparation of this article.
Funding Statement
This study was supported by a grant to the PID-PEP working group by the Federal Ministry of Education and Research (BMBF), Germany, FKZ: 01GM0894, project A6. PID-PEP kids has received support from the following pharmaceutical and medicinal product companies: Biotest (Dreieich, Germany), CSL Behring (Marburg, Germany), Grifols (Frankfurt am Main, Germany), Kedrion (Gräfelfing, Germany), Octapharma (Langenfeld, Germany), OMT (Minden/Frittlingen, Germany), Takeda (formerly Shire) Deutschland (Berlin, Germany). The IDCL receives funding for research and clinical trials from Takeda (formerly Shire, Berlin, Germany), CSL Behring (Marburg, Germany) and Octapharma (Langenfeld, Germany) which is managed by Klinikum St. Georg Leipzig. Ulrich Baumann received honoraria and reimbursement for travel expenses by CSL Behring, Octapharma and Takeda.
Author contributions
Study conception and design: M Fasshauer, G Schuermann, N Gebert, I Schulze, U Baumann; extracted clinical data: M Fasshauer, G Schuermann, N Gebert, U Baumann; analysis and interpretation of data: M Fasshauer, G Schuermann, U Baumann; drafting of manuscript: M Fasshauer, G Schuermann; critical revision: U Baumann. All authors cared for patients, read and worked on the manuscript, as well as approved the final manuscript.
Financial disclosure
This study was supported by a grant to the PID-PEP working group by the Federal Ministry of Education and Research (BMBF), Germany, FKZ: 01GM0894, project A6. PID-PEP kids has received support from the following pharmaceutical and medicinal product companies: Biotest (Dreieich, Germany), CSL Behring (Marburg, Germany), Grifols (Frankfurt am Main, Germany), Kedrion (Gräfelfing, Germany), Octapharma (Langenfeld, Germany), OMT (Minden/Frittlingen, Germany), Takeda (formerly Shire) Deutschland (Berlin, Germany). The IDCL receives funding for research and clinical trials from Takeda (formerly Shire, Berlin, Germany), CSL Behring (Marburg, Germany) and Octapharma (Langenfeld, Germany) which is managed by Klinikum St. Georg Leipzig. Ulrich Baumann received honoraria and reimbursement for travel expenses by CSL Behring, Octapharma and Takeda. No other conflicts of interest are to be declared.
None of the above-named companies was involved in the development and scientific evaluation of PID-PEP kids. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Competing interests disclosure
The authors have no competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, stock ownership or options and expert testimony.
Ethical conduct of research
The study was approved by the ethics committee of Hannover Medical School (ethical approval number: 640-2009) and all subjects gave written informed consent before participating.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
- 1.Bousfiha A, Moundir A, Tangye SG, et al. The 2022 Update of IUIS Phenotypical Classification for Human Inborn Errors of Immunity. J Clin Immunol. 2022;42(7):1508–1520. doi: 10.1007/s10875-022-01352-z [DOI] [PubMed] [Google Scholar]
- 2.McCusker C, Upton J, Warrington R. Primary immunodeficiency. Allergy Asthma Clin Immunol. 2018;14(Suppl. 2):61. doi: 10.1186/s13223-018-0290-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Syed MN, Kutac C, Miller JM, et al. Risk factors of pneumonia in primary antibody deficiency patients receiving immunoglobulin therapy: data from the US Immunodeficiency Network (USIDNET). J Clin Immunol. 2022;42(7):1545–1552. doi: 10.1007/s10875-022-01317-2 [DOI] [PubMed] [Google Scholar]
- 4.Tabolli S, Giannantoni P, Pulvirenti F, et al. Longitudinal study on health-related quality of life in a cohort of 96 patients with common variable immune deficiencies. Front Immunol. 2014;5:605. doi: 10.3389/fimmu.2014.00605 [DOI] [PMC free article] [PubMed] [Google Scholar]; •• Showed that QoL in CVID patients is significantly reduced.
- 5.Jiang F, Torgerson TR, Ayars AG. Health-related quality of life in patients with primary immunodeficiency disease. Allergy Asthma Clin Immunol. 2015;11:27. doi: 10.1186/s13223-015-0092-y [DOI] [PMC free article] [PubMed] [Google Scholar]; •• Showed that QoL in PID patients is significantly reduced.
- 6.KIDSCREEN - health-related quality of life questionnaire for children and young people and their parents [Internet]. Hamburg: Universitätsklinikum Hamburg-Eppendorf; 2011–2023. [cited 2024 May 18]. Available from: http://www.kidscreen.org/english/ [Google Scholar]
- 7.Robitail S, Ravens-Sieberer U, Simeoni M-C, et al. Testing the structural and cross-cultural validity of the KIDSCREEN-27 quality of life questionnaire. Qual Life Res. 2007;16(8):1335–1345. doi: 10.1007/s11136-007-9241-1 [DOI] [PubMed] [Google Scholar]
- 8.Ravens-Sieberer U, Auquier P, Erhart M, et al. The KIDSCREEN-27 quality of life measure for children and adolescents: psychometric results from a cross-cultural survey in 13 European countries. Qual Life Res. 2007;16(8):1347–1356. doi: 10.1007/s11136-007-9240-2 [DOI] [PubMed] [Google Scholar]
- 9.Petersen C, Schmidt S, Power M, Bullinger M. DISABKIDS Group . Development and pilot-testing of a health-related quality of life chronic generic module for children and adolescents with chronic health conditions: a European perspective. Qual Life Res. 2005;14(4):1065–1077. doi: 10.1007/s11136-004-2575-z [DOI] [PubMed] [Google Scholar]
- 10.Bullinger M, Schmidt S, Petersen C. DISABKIDS Group . Assessing quality of life of children with chronic health conditions and disabilities: a European approach. Int J Rehabil Res. 2002;25(3):197–206. doi: 10.1097/00004356-200209000-00005 [DOI] [PubMed] [Google Scholar]
- 11.Baars RM, Atherton CI, Koopman HM, Bullinger M, Power M. DISABKIDS group . The European DISABKIDS project: development of seven condition-specific modules to measure health related quality of life in children and adolescents. Health Qual Life Outcomes. 2005;3:70. doi: 10.1186/1477-7525-3-70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Health 2020: a European policy framework and strategy for the 21st century [Internet]. Regional Office for Europe: World Health Organization; 2013. [cited 2024 May 18]. Available from: https://iris.who.int/handle/10665/326386 [Google Scholar]; • Summarized the value of well-being in patient-centered clinical medicine.
- 13.Fasshauer M, Schuermann G, Gebert N, et al. A structured patient empowerment program for primary immunodeficiency significantly improves general and health-related quality of life. Cent-Eur J Immunol. 2021;46(2):244–249. doi: 10.5114/ceji.2021.107088 [DOI] [PMC free article] [PubMed] [Google Scholar]; • Showed significant improvement of health-related QoL in adults after PID-PEP.
- 14.Modulares Schulungsprogramm ModuS Training for patients with primary immunodeficiencies (PID) under immunoglobulin substitution and their parents [German] [Internet]. Osnabrück: Kompetenznetz Patientenschulung e.V.; 2019. [cited 2024 May 18]. Available from: https://www.pabst-publishers.com/fileadmin/user_upload/_modus_9783899678987/modus_9783958530751.pdf [Google Scholar]
- 15.Menrath I, Ernst G, Lange K, et al. Evaluation of a generic patient education program in children with different chronic conditions. Health Educ Res. 2019;34(1):50–61. doi: 10.1093/her/cyy045 [DOI] [PubMed] [Google Scholar]; •• Showed beneficial effects in health-related QoL of PEPs in rare chronic conditions.
- 16.Ellert U, Ravens-Sieberer U, Erhart M, Kurth B-M. Determinants of agreement between self-reported and parent-assessed quality of life for children in Germany-results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Health Qual Life Outcomes. 2011;9:102. doi: 10.1186/1477-7525-9-102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.White-Koning M, Arnaud C, Dickinson HO, et al. Determinants of child-parent agreement in quality-of-life reports: a European study of children with cerebral palsy. Pediatrics. 2007;120(4):e804–814. doi: 10.1542/peds.2006-3272 [DOI] [PubMed] [Google Scholar]
- 18.Ernst G, Menrath I, Lange K, et al. Development and evaluation of a generic education program for chronic diseases in childhood. Patient Educ Couns. 2017;100(6):1153–1160. doi: 10.1016/j.pec.2017.01.001 [DOI] [PubMed] [Google Scholar]
- 19.Germany National Normdata KIDSCREEN females & males, children & adolescents age 8–18 (self report & proxy report; Table A7_B-32; KIDSCREEN-27) [Internet]. Hamburg: Universitätsklinikum Hamburg-Eppendorf; 2011–2023. [cited 2024 May 18]. Available from: https://www.kidscreen.org/deutsch/auswertung/manual-anh%C3%A4nge/ [Google Scholar]