

Abstract
Background
Current injury prevention programmes in football are limited by a one-size-fits-all approach, which predominantly focuses on preventive exercise programmes while ignoring differences in risk profiles between individuals and teams.
Objective
To address this gap, we developed a new data-driven, customisable approach based on the principles of risk management. We collaborated with key stakeholders to identify focus areas for injury and illness prevention and determine their priorities.
Setting
The team medical and coaching staff included members from 17 professional football clubs, the national team and a youth football academy in Qatar.
Methods
In 2015, we launched a series of annual workshops under the Aspetar Sports Injury and Illness Prevention Programme. The workshops included club medical personnel and fitness coaches in a process to develop team-specific programmes for injury and illness prevention based on the principle of risk management. Over 2 years, workshops refined focus areas through discussions, surveys and small-group presentations, culminating in the creation a novel programme for football injury prevention.
Results
Out of 44 focus areas first identified, 23 were selected as priorities for inclusion in multimodal injury and illness prevention programmes. The identified focus areas represent a variety of aspects, including social/behavioural/lifestyle, exercise programmes/training, load management, recovery and equipment. The top priorities included communication, the Nordic hamstring exercise, training load, recovery strategies, nutrition, sleep, warm-up, the Copenhagen adduction exercise and core and dynamic stability.
Conclusion
We have developed a comprehensive framework for preventing injuries and illnesses in football grounded in the general principles of risk management. This framework has proven feasible and led to the creation of a new multicomponent programme, The Aspetar IP2 (Injury and Illness Prevention for Performance) NetWork, focusing on a range of areas beyond preventive exercise programmes only.
Keywords: Sporting injuries, Prevention, Football
WHAT IS ALREADY KNOWN ON THIS TOPIC
Despite the promising evidence of their effectiveness, the uptake of standard one-size-fits-all preventive programmes remains limited in professional sports.
WHAT THIS STUDY ADDS
We have tested a comprehensive framework for preventing injuries and illnesses in football based on the principles of risk management. This data-driven, evidence-based, stakeholder-involved process has created a new multicomponent programme, The Aspetar IP2 (Injury and Illness Prevention for Performance) NetWork, including a range of focus areas beyond preventive exercise programmes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The injury and illness prevention model presented and implemented in this study for male professional football can be adapted to other athlete groups and sports.
Introduction
Football injury prevention has advanced substantially in the past two decades, with several strategies and interventions developed for amateurs and professionals. Existing methods are primarily based on strength and conditioning exercises implemented as warm-up programmes. These interventions can reduce the risk of injury, as documented in several studies.1,7 Specific exercises targeting certain injury types show even better outcomes; the Nordic hamstring exercise lowers the risk of hamstring muscle injuries by 57%–70% and even more in players with a history of recent hamstring injury.8 9 While advances have been made in reducing injury rates through exercise-based programmes, challenges remain. Despite the encouraging results from randomised controlled trials, adherence to prevention programmes is still limited.10 11
Current injury prevention programmes have several limitations that warrant attention. First, they mainly use a ‘one-size-fits-all’ approach, which fails to account for individual differences in playing level, player fitness, biomechanics, gender and injury history, which are key factors influencing injury susceptibility.12 13 Second, the process and people involved with implementing injury prevention programmes differ between teams. The compliance and engagement of players with injury prevention exercises remain inconsistent, undermining their success.13,15 Existing programmes do not take a holistic approach, primarily focusing on physical aspects while neglecting other risk factors for injury, such as equipment, lifestyle, competition schedules and player load.16 17 As such, the early evidence and real-world experience suggest that a tailored and more comprehensive approach is needed to bridge these gaps.10 11 18 19 O’Brien et al19 evaluated the development and implementation of tailored injury prevention programmes in elite youth football, highlighting the limitations of one-size-fits-all approaches. Stensø et al18 reported on the successful adoption of adductor injury prevention programmes by Norwegian male professional football teams, noting that the programme was frequently adapted to meet specific needs. Developing a framework for adaptation to meet the overall needs of the whole team and individualisation based on the unique characteristics and needs of individual players may represent a successful avenue for advancing the field. One such framework is risk management, traditionally used in multiple other sectors, where countermeasures are based on a thorough assessment of risks and their potential consequences.20,23
To address existing gaps in current injury prevention practices in football, we set out to develop a new approach—through a holistic, scalable and customisable programme developed by the stakeholders. This innovative approach integrates the involvement of the stakeholders in programme creation. It follows an evidence-based, data-driven process to create specific, made-to-measure programmes for each team and player based on the principles of risk management: The IP2 NetWork—Injury and Illness Prevention for Performance. By addressing the needs and preferences of football teams and their staff, this programme aims to improve compliance and efficacy in injury prevention. In this paper, we describe the development process of a multimodal injury prevention programme for elite football players, as well as its priorities based on input from club medical and technical staff.
Methods
Setting and participants
In 2015, Aspetar Orthopaedic and Sports Medicine Hospital in Doha, Qatar, launched a series of annual workshops under the Aspetar Sports Injury and Illness Prevention Programme. These workshops aimed to introduce and implement the principles of risk management for injury and illness prevention, engaging medical personnel from the National Sports Medicine Programme, who provide sports medicine services to various sports clubs, national federations and Aspire, the youth sports academy in Qatar. Over the years, the scope of participation expanded to include club fitness coaches, further enriching the discussions and outcomes.
Workshop programme
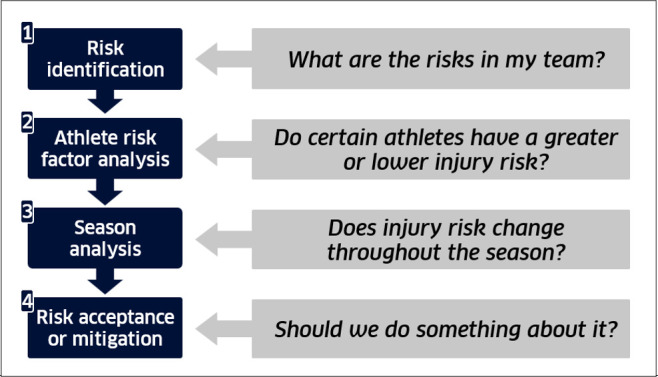
Workshops were dedicated to systematically exploring and managing injury and illness risks in Qatari elite sports, each lasting 4–5 hours. The basic model for risk management in sports (figure 1) served as the foundation for this process. The model was introduced in the first workshop and repeated at each subsequent workshop. Workshops consisted of brief lectures and extensive small-group discussions on key components of risk management planning, such as injury surveillance, periodic health evaluation, player fitness and health habits, season analysis, and discussing barriers and opportunities for injury and illness prevention in the clubs. Lectures highlighted best-practice examples from clubs and share success stories. During the small-group discussions, participants were mixed across clubs to encourage learning from each other. At all stages of the process, club staff were encouraged to base their evaluations on data from injury surveillance, player medical history, annual health evaluations and a review of their team’s training and match schedule (figure 1).
Figure 1. Basic risk management model in sports adapted from Mcintosh and Bahr,23 outlining the key steps in risk identification and assessment: assessing team, player and season risks based on team and league surveillance data, and then considering potential interventions to mitigate risks.
This paper is based on data collected during two workshops held in 2019 and 2020. In the 2019 workshop, 45 medical and technical personnel from 18 professional football teams participated. Each team was represented by a team physician, a fitness coach and a physiotherapist, though seven teams lacked a fitness coach and one was without a physiotherapist. In the 2020 workshop, all 18 teams were represented by the team physician, fitness coach and physiotherapist. The 2019 workshop aimed to identify key focus areas to optimally maintain player health, fitness and performance through discussions and surveys. The 2020 workshop built on this by refining the identified focus areas for injury and illness prevention.
Surveys
The 2019 workshop titled ‘From theory to practice: YOU build the ideal injury and illness prevention program in football’ aimed at engaging the participants in active discussions to identify the most pertinent focus areas for injury and illness prevention within Qatari football through 19 small-group and plenary discussions. Prior to the workshop, survey I was emailed to the medical and technical staff (including the team physicians, physiotherapists and fitness coaches) across the 17 football clubs in Qatar, the youth football academy and the Qatar national team (19 groups). This survey had an open format, encouraging respondents to discuss the questions with their respective team members before submitting their responses. The question mirrored the one subsequently posed during the workshop: ‘Identify the main areas to focus on or actions needed to keep your players fit and healthy and enable them to perform at the highest level’. The responses collected from 18 groups were qualitative in nature, with participants providing lists of their perceived focus areas, which were then compiled into a comprehensive dataset of an initial list of focus areas identified by the teams. During the 2019 workshop, this dataset served as the foundation for small group discussions to identify a comprehensive list of focus areas. Moderators facilitated these discussions, guiding participants to critically evaluate each focus area’s relevance, feasibility and impact. A qualitative analysis was conducted to synthesise common themes and consensus, resulting in the identification of 44 focus areas.
To further refine these areas, each of the 19 groups was tasked with prioritising the areas to focus on by assigning scores to rank the 44 identified areas on a scale from 0 to 20, with 20 indicating the highest importance and 0 indicating no importance. This scoring system allowed participants to express their priority for each focus area, reflecting its perceived significance and relevance to their teams. The scores were then aggregated to gauge the overall importance assigned to each focus area across all groups. After scoring, the groups were requested to classify which focus areas should be included in the programme. A majority consensus was required for a focus area to be included, defined as at least 10 out of the 19 groups voting in favour of its inclusion. This threshold ensured that only those focus areas with broad support were considered for inclusion in the programme. The outcome, including the sum of all points for each focus area, their categorisation and the final vote for inclusion, is presented in table 1.
Table 1. The main focus areas for injury/illness prevention and performance, identified by medical staff and their priority scores from survey I.
| Focus areas | Priority score | Identified as a priority? | |
| Points | % | ||
| Social/behavioural/lifestyle | 882 | 40.8 | |
| Sleep | 258 | 11.9 | Yes |
| Nutrition | 198 | 9.2 | Yes |
| Hydration | 174 | 8.1 | Yes |
| Nutritional supplements | 59 | 2.7 | Yes |
| Players’ education level | 52 | 2.4 | Yes* |
| Motivation/mental preparation | 38 | 1.8 | Yes* |
| Fitness level (physical condition) | 38 | 1.8 | No |
| Mental strength | 30 | 1.4 | Yes* |
| Rest | 20 | 0.9 | No |
| Weight monitoring | 15 | 0.7 | No |
| Exercise programmes/training | 578 | 26.7 | |
| Nordic hamstring exercise | 147 | 6.8 | Yes |
| Training load monitoring | 82 | 3.8 | Yes |
| Strength training (eccentric) | 67 | 3.1 | No |
| Copenhagen adduction exercise | 57 | 2.6 | Yes |
| Proprioception exercises | 50 | 2.3 | No |
| Prewarmup exercises | 42 | 1.9 | Yes* |
| Balance training | 32 | 1.5 | Yes |
| Motor control and postural pattern | 24 | 1.1 | No |
| Core exercises | 20 | 0.9 | Yes† |
| Preseason preparation | 18 | 0.8 | Yes† |
| FIFA 11+ | 16 | 0.7 | Yes |
| Warm-up | 16 | 0.7 | Yes* |
| Plyometric training | 7 | 0.3 | Yes |
| Management | 285 | 13.2 | |
| Communication/cooperation between technical and medical staff | 78 | 3.6 | Yes |
| Training attendance | 37 | 1.7 | No |
| Preseason medical screening | 33 | 1.5 | No |
| Injury management | 30 | 1.4 | No |
| Annual match calendar scheduling | 30 | 1.4 | No |
| Communication between the club and the national team | 22 | 1.0 | No |
| Staff availability to look after players | 20 | 0.9 | No |
| Stability of technical and medical staff in the club | 17 | 0.8 | No |
| Non-supervised prewarm-up ball availability on the pitch | 16 | 0.7 | No |
| Player health monitoring across age categories | 2 | 0.1 | No |
| Recovery | 259 | 12.0 | |
| Recovery | 124 | 5.7 | Yes* |
| Stretching (proprioceptive neuromuscular facilitation) | 57 | 2.6 | Yes |
| Cold water immersion | 42 | 1.9 | Yes* |
| Massage | 25 | 1.2 | Yes* |
| Jacuzzi/hot tub | 11 | 0.5 | No |
| Equipment | 111 | 5.1 | |
| Shin guards | 74 | 3.4 | Yes |
| Training equipment/pitch conditions | 19 | 0.9 | No |
| Football shoes | 18 | 0.8 | Yes |
| Other | 46 | 2.1 | |
| Manual therapy presession/pregame | 20 | 0.9 | No |
| Kinesio taping | 17 | 0.8 | Yes† |
| Acclimation | 9 | 0.4 | No |
| Sum | 2161 | 100.0 | |
Focus area was combined with another through the development process of IP.2.
Focus area evolved during the development process.
During the next workshop (2020), these focus areas and their priorities were further refined. For the workshop, each working group of 4–5 team medical and technical staff prepared 5 min presentations on the scientific evidence supporting their respective focus area. The attendees then engaged in small-group discussions to assess the relevance of each focus area when developing tailor-made risk management programmes for their team. Finally, survey II, which included a table detailing the 23 focus areas, was distributed to each team during the workshop. Teams were asked to select 5 of these 23 focus areas based on their importance for their team, ranking their priority on a scale from 5 to 1, with 5 indicating the highest priority and 1 the lowest (table 2).
Table 2. Final list of focus areas included in the Aspetar IP2 (Injury and Illness Prevention for Performance) programme and their aggregate priority scores from survey II.
| Focus areas | Priority score |
| Communication | 54 |
| The Nordic hamstring exercise | 34 |
| Training load | 31 |
| Recovery strategies—massage, self-myofascial release, stretching and compression garments | 29 |
| Nutrition for football—preparing for match day | 24 |
| Sleep | 17 |
| Warm-up | 17 |
| The Copenhagen adduction exercise | 16 |
| Core and dynamic stability | 10 |
| Cold water immersion | 9 |
| Tips for the off-season | 9 |
| Mental health and well-being | 9 |
| Nutritional supplements | 5 |
| Hydration | 3 |
| Balance | 2 |
| The 11+ programme | 1 |
| Flexibility training and stretching | 0 |
| Taping and bracing | 0 |
| Football shoes | 0 |
| Shin guards | 0 |
| Plyometrics | 0 |
| Ramadan—fasting and sport | 0 |
| Concussion | 0 |
Final programme development: the Aspetar IP2 NetWork
To develop the final programme components, 23 working groups composed of medical and technical staff from the clubs, and supported by experienced sports physicians, scientists, nutritionists, psychologists, podiatrists, etc, crafted fact sheets for each focus area. These fact sheets summarised the current scientific evidence on each topic. The resulting 23 fact sheets were then sent to international experts for review and input. These experts were selected based on their research publications for their expertise within each field. This process culminated in the creation of the Aspetar multimodal injury and illness prevention programme for football, encapsulated in a booklet, the ‘Aspetar IP2 NetWork’ (online supplemental material 1).
Patient and public involvement
No patients or members of the public were involved in the planning, design, data collection, analysis or interpretation of this study’s results.
Equity, diversity and inclusion statement
The study focused exclusively on male professional players in Qatar, a diverse group from around the world, and involved their support staff, predominantly males recruited from North Africa, Asia and Europe.
Results
Survey I (response rate: 95%) identified 44 focus areas for injury and illness prevention. Of these, 25 focus areas were selected for inclusion in the multimodal injury and illness prevention programme. Some areas with overlapping content were consolidated into broader categories. (table 1). In the further development process, two additional elements, Ramadan—fasting and sport, and concussion, were added to the programme. This resulted in the ultimate inclusion of 23 focus areas constituting the programme, the IP2 Network (table 2). Table 2 also illustrates the priority assigned to each identified focus area based on the scores given by the teams.
Discussion
This is the first study to employ a structured risk management procedure engaging key stakeholders, who are thoroughly trained in principals of risk management and have years of field experience, to develop a toolbox addressing focus areas aimed at mitigating injury and illness risks within their teams. Previous literature has mainly examined various singular preventive strategies such as neuromuscular training programmes,1 24 protective equipment25 and nutrition/hydration strategies.26
In line with existing evidence, the programme incorporates well-established preventive measures such as the FIFA 11+warm up routine,1 27 Nordic hamstring exercises8 28 and Copenhagen adduction exercises.18 29 The inclusion of these exercise programmes not only reflects their proven efficacy in reducing lower extremity, hamstring and groin injuries but also that these represented the largest injury burden in the Qatari professional football.30,35 It should be noted that when starting the risk management process, the participants had access to injury surveillance data for their own team and players from a long-term Injury and Illness Surveillance Programme and data from annual health evaluations.1130,35
Additionally, our participants highlighted the importance of training load management, recovery strategies, optimal nutrition, sleep and hydration, which were consistently identified as key factors in injury prevention and performance optimisation.36,38 These findings emphasise the need for a holistic approach to injury prevention. Novel components were also incorporated based on stakeholder input. Communication consistently scored with a high priority across all teams, focusing on effective communication between different roles within the team (medical, coaching and technical staff) and clear and consistent communication with players. Strategies for the Ramadan period, a unique challenge for Muslim players, were also among the focus areas identified, although not ranked among the top five by any of the teams.
Real-world injury prevention practices
Several studies have attempted to describe the preventive measures employed in professional football. McCall et al have published four questionnaire-based studies to map elite club and national team medical staff practices and opinions.39,42 In 2014, they first surveyed international (mainly European) clubs identified as premier league teams39 and then teams participating in the 2014 FIFA World Cup.40 These studies were followed by a 2015 survey of clubs participating in the UEFA Elite Club41 before the 2020 publication of a Delphi-styled survey to 21 experienced sports practitioners from 18 teams from the Big-5 European leagues specifically addressing the prevention of muscle injuries.42
Their first survey revealed that the exercises used to prevent non-contact injuries, listed in order of prevalence, were eccentric exercises, balance/proprioception, hamstring eccentric training, core stability, Nordic hamstring and gluteus activation exercises.39 The FIFA 2014 World Cup teams reported that the most important preventive exercises were flexibility, core, combined contractions, balance and eccentric training.40 In the UEFA Elite Club Injury Study survey, the top three preventive exercises applied by the teams were eccentric, balance/proprioception and core training.41 The Delphi survey showed that the practitioners perceived sprinting and high-speed running as ‘very effective’ in preventing non-contact muscle injuries and exercises with an eccentric focus as ‘effective’. In contrast, some other exercise modes (concentric focus, horizontal plyometrics, vertical plyometrics, isometric focus, activation/coordination, dynamic flexibility, core stability, static flexibility) were considered ‘somewhat effective’42
O’Brien et al recently evaluated how football academies develop and implement individualised injury prevention programmes based on four European academy teams. Through data analysis, interviews and focus group meetings with the technical team, physical therapists and players, they examined how exercises specifically aimed at preventing musculoskeletal injuries were implemented. Instead of generic exercises, the teams used various methods to design custom programmes. Still, these tailored programmes had high adherence rates, with 76% completed exactly as planned and another 11% with some modifications.19 Injury prevention practices have also been explored in other football settings.43 44 Meurer et al43 surveyed team physiotherapists from 16 Brazilian first-division clubs, reporting that strength training, functional training and core and balance/proprioception exercises were incorporated into their injury prevention programmes. In contrast, a qualitative study interviewing 17 players, 8 medical personnel and 7 head coaches working in women’s elite football in Ireland showed that while jumping and landing exercises were frequently used to mitigate injury risk, evidence-based prevention exercises and programmes such as the Nordic hamstring curl, Copenhagen adduction exercise and FIFA 11+ were rarely applied.44
The existing literature shows that the focus primarily revolves around preventive exercise programmes and that strong evidence supports their effectiveness.45 Our findings also reveal that preventive exercises such as the Nordic hamstring, Copenhagen adduction and core stability training emerged as significant focus areas in the Qatari professional league. However, only Nordic hamstring training ranked among the top priorities, and it should be noted that teams emphasised a range of other focus areas beyond exercise programmes to keep their players healthy.
In contrast to the questionnaire-based surveys described above, our study is the first to engage the medical team and coaching staff in a structured and guided process after providing extensive training on the principles and methods of risk management. Additionally, the process differed by not asking teams what they were currently doing to keep their players healthy and performing but instead what they planned on doing going forward. In identifying and prioritising focus areas, they were encouraged to actively use their data on team members and players to guide their decisions. We also emphasised the crucial role of identifying injury and illness risks and risk factors before initiating the selection and implementation of prevention strategies, as McCall et al39 acknowledged in their international club survey. The participatory approach strengthens internal validity by ensuring the programme addresses relevant risks identified by the teams. In this way, the IP2 Network programme was developed by the stakeholders for the stakeholders. Programme ownership was also strengthened by engaging the medical and technical teams in reviewing the evidence base for each focus area before deciding on their priority for their team. It is not surprising that priorities differed between teams; the outcome was expected to be bespoke programmes for each team, not a one-size-fits-all programme. The IP2 Network should be seen as a flexible framework to build a risk management plan tailored to teams’ and individual players’ specific risk profiles and needs. The programme’s adaptability allows for the customisation of interventions, ensuring they are suited to each team’s unique conditions and challenges. This approach acknowledges the diversity in player conditions, team strategies and environmental factors, allowing for individualised and adaptable injury prevention strategies that align with the need for a tailored approach.
The key focus areas
The top three focus areas prioritised by our teams were communication, the Nordic hamstring exercise and training load. They consistently highlighted the critical role of effective communication as a key focus area, recognising the complex interpersonal dynamics involved in implementing a successful injury prevention programme. Fostering quality communication between players, coaches and medical staff regarding injury concerns is correlated with injury rates.46 Tabben et al,13 interviewing key stakeholders in the Qatari professional league, also identified the importance of communication within the team and how it affects the implementation of injury prevention. Their study also identified the crucial role of fitness coaches as pivotal figures in the implementation process and as liaisons between the medical and coaching teams. While communication is often overlooked in injury prevention programmes, our stakeholders recognised its importance in facilitating seamless collaboration among medical and performance staff and ensuring clear and consistent messaging to athletes. Horan et al44 also reported that insufficient communication among players, head coaches and medical personnel hindered the application of evidence-based injury prevention protocols in Irish women’s football, and McCall et al identified poor internal communication as one of the most significant extrinsic risk factors for injuries among UEFA Elite Club teams.41
Our stakeholders also placed significant emphasis on the Nordic hamstring exercise, which was identified as the second most important focus area. This exercise has been extensively studied, consistently demonstrating efficacy in reducing the risk of hamstring injuries.8 9 Training load management also emerged as a key focus area. While previous research has explored the relationship between training load and injury risk,37 47 the high priority reflects the understanding of our stakeholders of the unique demands and challenges faced by professional football players in Qatar, where environmental and cultural factors may influence training load and recovery.
Strength and limitations
Existing injury prevention strategies in football often operate in silos, focusing on specific areas such as biomechanics, strength exercises or psychological training.2948,50 While valuable on their own, these interventions lack a holistic approach that addresses the complex interplay of factors contributing to injuries and illnesses. Furthermore, most existing programmes are ‘one-size-fits-all’, not based on a rigorous risk identification process to tailor them to the needs of the athlete or team.20 22 We emphasise the importance of conducting sport-specific, data-driven risk assessments.13 This allows for tailoring the programme to address the specific needs and vulnerabilities of each team and individual player.
While our study provides valuable insights into the injury prevention priorities of team staff working with male professional footballers in Qatar, its applicability to other populations remains to be established. Therefore, our findings did not encompass focus areas relevant to other sports or groups, such as menstrual status, relative energy deficiency in sport and growth and maturation, which we would expect to emerge in women’s and youth football. Still, we would argue that following the same approach—a structured risk management process—is equally appropriate for other settings, but where the focus areas and their priorities would be expected to differ.
Conclusions
We have developed a comprehensive multimodal framework for preventing injuries and illnesses in male professional football. This framework integrates data-driven injury and illness risk assessment, stakeholder engagement, customisable intervention and a holistic approach to address the multifaceted nature of injury prevention. This process has led to the creation of a new multicomponent programme, the Aspetar IP2 (Injury and Illness Prevention for Performance) NetWork, focusing on various areas beyond preventive exercise programmes. Importantly, our findings underscore the pivotal role of effective communication between the medical team, coaching staff and players. By allowing for adaptation and individualisation, this framework offers a flexible, evidence-based structure that teams can modify to meet their needs and optimise player health and performance.
supplementary material
Acknowledgements
This research was conducted at Aspetar Orthopedic and Sports Medicine Hospital in collaboration with the Aspetar Injury and Illness Prevention Program (ASPREV), the National Sports Medicine Programme, the Qatar Football Federation and the league organisation. We thank the experts in the IP2 Network booklet for reviewing its contents.
Footnotes
Funding: The Aspetar Orthopaedic and Sports Medicine Hospital, Doha, Qatar, funded this study.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Not applicable.
Ethics approval: This study involves human participants the Aspire Zone Institutional Review Board approved this study, approval code E202301050. Participants gave informed consent to participate in the study before taking part.
Collaborators: IP2 NetWork group: Ihsan Abdullah, Anas Abu Esba, Akram Abid, Ahmed Khellil Abbasi, Abdulaziz Jaham Al-Kuwari, Dennis Artuz, Nizar Baccouche, Mondher Barboura, Fawzi Bendimerad, Anis Belhadj, Radhouane Ben Ghorbal, Zaher Ben Soltane, Brahim Boubaker, Selim Boubaker, Marco Cardinale, Karim Chamari, Mokhtar Chaabane, Souhail Chebbi, Imad Daaji, Ramadan Daoud, Pieter D’Hooghe, Ovidiu Dragos, Boudiaf ElHocine, Zied Ellouze, Konstantinos Epameinontidis, Ahmed Gdhami, Ahmed Gharbi, Mondher Haddar, Miguel Heitor, Louis Holtzhausen, Cosmin Horobeanu, Mourad Jelassi, Karim Khalladi, Daniel Kings, Hafid Maameri, Olivier Materne, Pierre McCourt, Nidhal Meddeb, Riadh Miladi, Mourad Mokrani, Hicham Moutaouakkil, Anthony Padayao, Michail Pantouveris, Darren Paul, Ricardo Pinto, Alaaeddine Rahali, Czarlon Ramos, Paul Read, Raouf Nader Rekik, Jim Roa, Daniel Sebo, Djamel Senoussi, Andreas Serner, Oussama Skhiri, Sofiane Souissi, Athol Thomson, Mouloud Toumi, Antonio Tramullas, Nicol Van Dyk, Amine Zouani and Eirik Halvorsen Wik.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Contributor Information
Bahar Hassanmirzaei, Email: bahariane@yahoo.com.
Yorck Schumacher, Email: Yo.Schumacher@aspetar.com.
Montassar Tabben, Email: Montassar.Tabben@aspetar.com.
Roald Bahr, Email: roaldb@nih.no.
IP2 NetWork Group, Email: IP2@aspetar.com.
IP2 NetWork Group:
Ihsan Abdullah, Anas Abu Esba, Akram Abid, Ahmed Khellil Abbasi, Abdulaziz Jaham Al-Kuwari, Dennis Artuz, Nizar Baccouche, Mondher Barboura, Fawzi Bendimerad, Anis Belhadj, Radhouane Ben Ghorbal, Zaher Ben Soltane, Brahim Boubaker, Selim Boubaker, Marco Cardinale, Karim Chamari, Mokhtar Chaabane, Souhail Chebbi, Imad Daaji, Ramadan Daoud, Pieter D’Hooghe, Ovidiu Dragos, Boudiaf ElHocine, Zied Ellouze, Konstantinos Epameinontidis, Ahmed Gdhami, Ahmed Gharbi, Mondher Haddar, Miguel Heitor, Louis Holtzhausen, Cosmin Horobeanu, Mourad Jelassi, Karim Khalladi, Daniel Kings, Hafid Maameri, Olivier Materne, Pierre McCourt, Nidhal Meddeb, Riadh Miladi, Mourad Mokrani, Hicham Moutaouakkil, Anthony Padayao, Michail Pantouveris, Darren Paul, Ricardo Pinto, Alaaeddine Rahali, Czarlon Ramos, Paul Read, Raouf Nader Rekik, Jim Roa, Daniel Sebo, Djamel Senoussi, Andreas Serner, Oussama Skhiri, Sofiane Souissi, Athol Thomson, Mouloud Toumi, Antonio Tramullas, Nicol Van Dyk, Amine Zouani, and Eirik Halvorsen Wik
Data availability statement
Data are available on reasonable request.
References
- 1.Bizzini M, Dvorak J. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br J Sports Med. 2015;49:577–9. doi: 10.1136/bjsports-2015-094765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to prevent injuries in young female footballers: cluster randomised controlled trial. BMJ. 2008;337:a2469. doi: 10.1136/bmj.a2469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Waldén M, Atroshi I, Magnusson H, et al. Prevention of acute knee injuries in adolescent female football players: cluster randomised controlled trial. BMJ. 2012;344:e3042. doi: 10.1136/bmj.e3042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Finch CF, Twomey DM, Fortington LV, et al. Preventing Australian football injuries with a targeted neuromuscular control exercise programme: comparative injury rates from a training intervention delivered in a clustered randomised controlled trial. Inj Prev. 2016;22:123–8. doi: 10.1136/injuryprev-2015-041667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lindblom H, Sonesson S, Torvaldsson K, et al. Extended Knee Control programme lowers weekly hamstring, knee and ankle injury prevalence compared with an adductor strength programme or self-selected injury prevention exercises in adolescent and adult amateur football players: a two-armed cluster-randomised trial with an additional comparison arm. Br J Sports Med. 2023;57:83–90. doi: 10.1136/bjsports-2022-105890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Núñez JF, Fernandez I, Torres A, et al. Strength Conditioning Program to Prevent Adductor Muscle Strains in Football: Does it Really Help Professional Football Players? Int J Environ Res Public Health. 2020;17:6408. doi: 10.3390/ijerph17176408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Owoeye OBA, Palacios-Derflingher LM, Emery CA. Prevention of Ankle Sprain Injuries in Youth Soccer and Basketball: Effectiveness of a Neuromuscular Training Program and Examining Risk Factors. Clin J Sport Med. 2018;28:325–31. doi: 10.1097/JSM.0000000000000462. [DOI] [PubMed] [Google Scholar]
- 8.van der Horst N, Smits D-W, Petersen J, et al. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43:1316–23. doi: 10.1177/0363546515574057. [DOI] [PubMed] [Google Scholar]
- 9.van Dyk N, Behan FP, Whiteley R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br J Sports Med. 2019;53:1362–70. doi: 10.1136/bjsports-2018-100045. [DOI] [PubMed] [Google Scholar]
- 10.Ekstrand J, Bengtsson H, Walden M, et al. Still poorly adopted in male professional football: but teams that used the Nordic Hamstring Exercise in team training had fewer hamstring injuries - a retrospective survey of 17 teams of the UEFA Elite Club Injury Study during the 2020-2021 season. BMJ Open Sport Exerc Med. 2022;8:e001368. doi: 10.1136/bmjsem-2022-001368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chebbi S, Chamari K, Van Dyk N, et al. Hamstring Injury Prevention for Elite Soccer Players: A Real-World Prevention Program Showing the Effect of Players’ Compliance on the Outcome. J Strength Cond Res. 2022;36:1383–8. doi: 10.1519/JSC.0000000000003505. [DOI] [PubMed] [Google Scholar]
- 12.O’Brien J, Finch CF. The implementation of musculoskeletal injury-prevention exercise programmes in team ball sports: a systematic review employing the RE-AIM framework. Sports Med. 2014;44:1305–18. doi: 10.1007/s40279-014-0208-4. [DOI] [PubMed] [Google Scholar]
- 13.Tabben M, Verhagen E, Warsen M, et al. Obstacles and opportunities for injury prevention in professional football in Qatar: exploring the implementation reality. BMJ Open Sport Exerc Med. 2023;9:e001370. doi: 10.1136/bmjsem-2022-001370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Frank BS, Register-Mihalik J, Padua DA. High levels of coach intent to integrate a ACL injury prevention program into training does not translate to effective implementation. J Sci Med Sport. 2015;18:400–6. doi: 10.1016/j.jsams.2014.06.008. [DOI] [PubMed] [Google Scholar]
- 15.Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50:273–80. doi: 10.1136/bjsports-2015-095788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ekstrand J. Preventing injuries in professional football: thinking bigger and working together. Br J Sports Med. 2016;50:709–10. doi: 10.1136/bjsports-2016-096333. [DOI] [PubMed] [Google Scholar]
- 17.Brito J, Mendes R, Figueiredo P, et al. Is it Time to Consider Quaternary Injury Prevention in Sports? Sports Med. 2023;53:769–74. doi: 10.1007/s40279-022-01765-1. [DOI] [PubMed] [Google Scholar]
- 18.Stensø J, Andersen TE, Harøy J. Adductor Strengthening Programme is successfully adopted but frequently modified in Norwegian male professional football teams: a cross-sectional study. BMJ Open. 2022;12:e060611. doi: 10.1136/bmjopen-2021-060611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.O’Brien J, Santner E, Kröll J. Moving Beyond One-Size-Fits-All Approaches to Injury Prevention: Evaluating How Tailored Injury Prevention Programs Are Developed and Implemented in Academy Soccer. J Orthop Sports Phys Ther. 2021;51:432–9. doi: 10.2519/jospt.2021.10513. [DOI] [PubMed] [Google Scholar]
- 20.Fuller C, Drawer S. The application of risk management in sport. Sports Med. 2004;34:349–56. doi: 10.2165/00007256-200434060-00001. [DOI] [PubMed] [Google Scholar]
- 21.Fuller CW. Managing the risk of injury in sport. Clin J Sport Med. 2007;17:182–7. doi: 10.1097/JSM.0b013e31805930b0. [DOI] [PubMed] [Google Scholar]
- 22.Fuller CW, Junge A, Dvorak J. Risk management: FIFA’s approach for protecting the health of football players. Br J Sports Med. 2012;46:11–7. doi: 10.1136/bjsports-2011-090634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.McIntosh A, Bahr R. In: Handbook of Sports Medicine and Science Sports Injury Prevention. Bahr R, Engebretsen L, editors. Wiley Blackwell; 2008. Developing and managing an injury prevention program within the team; pp. 17–29. [Google Scholar]
- 24.Emery CA, Rose MS, McAllister JR, et al. A prevention strategy to reduce the incidence of injury in high school basketball: a cluster randomized controlled trial. Clin J Sport Med. 2007;17:17–24. doi: 10.1097/JSM.0b013e31802e9c05. [DOI] [PubMed] [Google Scholar]
- 25.Yang J, Marshall SW, Bowling JM, et al. Use of discretionary protective equipment and rate of lower extremity injury in high school athletes. Am J Epidemiol. 2005;161:511–9. doi: 10.1093/aje/kwi077. [DOI] [PubMed] [Google Scholar]
- 26.Turnagöl HH, Koşar ŞN, Güzel Y, et al. Nutritional Considerations for Injury Prevention and Recovery in Combat Sports. Nutrients. 2021;14:53. doi: 10.3390/nu14010053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Silvers-Granelli HJ, Bizzini M, Arundale A, et al. Does the FIFA 11+ Injury Prevention Program Reduce the Incidence of ACL Injury in Male Soccer Players? Clin Orthop Relat Res. 2017;475:2447–55. doi: 10.1007/s11999-017-5342-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Petersen J, Thorborg K, Nielsen MB, et al. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296–303. doi: 10.1177/0363546511419277. [DOI] [PubMed] [Google Scholar]
- 29.Harøy J, Clarsen B, Wiger EG, et al. The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med. 2019;53:150–7. doi: 10.1136/bjsports-2017-098937. [DOI] [PubMed] [Google Scholar]
- 30.Bakken A, Targett S, Bere T, et al. Muscle Strength Is a Poor Screening Test for Predicting Lower Extremity Injuries in Professional Male Soccer Players: A 2-Year Prospective Cohort Study. Am J Sports Med. 2018;46:1481–91. doi: 10.1177/0363546518756028. [DOI] [PubMed] [Google Scholar]
- 31.Bakken A, Targett S, Bere T, et al. The functional movement test 9+ is a poor screening test for lower extremity injuries in professional male football players: a 2-year prospective cohort study. Br J Sports Med. 2018;52:1047–53. doi: 10.1136/bjsports-2016-097307. [DOI] [PubMed] [Google Scholar]
- 32.Chamari K, Schumacher YO, Chaabane M, et al. Impact of COVID-19 lockdown on injury risk in Qatar’s professional football. J Sci Med Sport. 2023;26:522–7. doi: 10.1016/j.jsams.2023.09.008. [DOI] [PubMed] [Google Scholar]
- 33.Eirale C, Farooq A, Smiley FA, et al. Epidemiology of football injuries in Asia: a prospective study in Qatar. J Sci Med Sport. 2013;16:113–7. doi: 10.1016/j.jsams.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 34.Rekik RN, Tabben M, Eirale C, et al. ACL injury incidence, severity and patterns in professional male soccer players in a Middle Eastern league. BMJ Open Sport Exerc Med. 2018;4:e000461. doi: 10.1136/bmjsem-2018-000461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tabben MBR, Chamari K. Injury surveillance in qatar stars leagues: 8 seasons epidemiological study [in submission]
- 36.Holway FE, Spriet LL. Sport-specific nutrition: practical strategies for team sports. J Sports Sci. 2011;29 Suppl 1:S115–25. doi: 10.1080/02640414.2011.605459. [DOI] [PubMed] [Google Scholar]
- 37.Malone S, Owen A, Newton M, et al. The acute:chonic workload ratio in relation to injury risk in professional soccer. J Sci Med Sport. 2017;20:561–5. doi: 10.1016/j.jsams.2016.10.014. [DOI] [PubMed] [Google Scholar]
- 38.Nédélec M, McCall A, Carling C, et al. Recovery in soccer: part I - post-match fatigue and time course of recovery. Sports Med. 2012;42:997–1015. doi: 10.2165/11635270-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 39.McCall A, Carling C, Nedelec M, et al. Risk factors, testing and preventative strategies for non-contact injuries in professional football: current perceptions and practices of 44 teams from various premier leagues. Br J Sports Med. 2014;48:1352–7. doi: 10.1136/bjsports-2014-093439. [DOI] [PubMed] [Google Scholar]
- 40.McCall A, Davison M, Andersen TE, et al. Injury prevention strategies at the FIFA 2014 World Cup: perceptions and practices of the physicians from the 32 participating national teams. Br J Sports Med. 2015;49:603–8. doi: 10.1136/bjsports-2015-094747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.McCall A, Dupont G, Ekstrand J. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club Injury Study teams: a survey of teams’ head medical officers. Br J Sports Med. 2016;50:725–30. doi: 10.1136/bjsports-2015-095259. [DOI] [PubMed] [Google Scholar]
- 42.McCall A, Pruna R, Van der Horst N, et al. Exercise-Based Strategies to Prevent Muscle Injury in Male Elite Footballers: An Expert-Led Delphi Survey of 21 Practitioners Belonging to 18 Teams from the Big-5 European Leagues. Sports Med. 2020;50:1667–81. doi: 10.1007/s40279-020-01315-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Meurer MC, Silva MF, Baroni BM. Strategies for injury prevention in Brazilian football: Perceptions of physiotherapists and practices of premier league teams. Phys Ther Sport. 2017;28:1–8. doi: 10.1016/j.ptsp.2017.07.004. [DOI] [PubMed] [Google Scholar]
- 44.Horan D, Kelly S, Hägglund M, et al. Players’, Head Coaches’, And Medical Personnels’ Knowledge, Understandings and Perceptions of Injuries and Injury Prevention in Elite-Level Women’s Football in Ireland. Sports Med Open. 2023;9:64. doi: 10.1186/s40798-023-00603-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Barrera J, Figueiredo AJ, Clemente FM. Injury Prevention Programmes in Male Soccer Players: An Umbrella Review of Systematic Reviews. JOMH. 2022;18:1. doi: 10.31083/j.jomh1810200. [DOI] [Google Scholar]
- 46.Ekstrand J, Lundqvist D, Davison M, et al. Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs. Br J Sports Med. 2019;53:304–8. doi: 10.1136/bjsports-2018-099411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Boullosa D, Casado A, Claudino JG, et al. Do you Play or Do you Train? Insights From Individual Sports for Training Load and Injury Risk Management in Team Sports Based on Individualization. Front Physiol. 2020;11:995. doi: 10.3389/fphys.2020.00995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Li S, Wu Q, Chen Z. Effects of Psychological Interventions on the Prevention of Sports Injuries: A Meta-analysis. Orthop J Sports Med. 2020;8:2325967120928325. doi: 10.1177/2325967120928325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.McBain K, Shrier I, Shultz R, et al. Prevention of sports injury I: a systematic review of applied biomechanics and physiology outcomes research. Br J Sports Med. 2012;46:169–73. doi: 10.1136/bjsm.2010.080929. [DOI] [PubMed] [Google Scholar]
- 50.Fanchini M, Steendahl IB, Impellizzeri FM, et al. Exercise-Based Strategies to Prevent Muscle Injury in Elite Footballers: A Systematic Review and Best Evidence Synthesis. Sports Med. 2020;50:1653–66. doi: 10.1007/s40279-020-01282-z. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data are available on reasonable request.