

Abstract
Background
Switzerland is one of the few remaining European countries without a uniform national breast cancer screening program. Most Swiss cantons have initiated mammography screening programs, with the notable exceptions of the cantons of central Switzerland. The aim of this study is to compare the TNM (tumor–node–metastasis) status in woman diagnosed with screen- and non-screen-detected breast cancers. We compare TNM of breast cancers of cantonal screening cantons (Or-SC) with organized mammographic screening and opportunistic-screening cantons (Op-SC) without organized mammographic screening.
Materials and methods
We compared the TNM documented in cantons with organized screening (Or-SC) in the national cancer registry with those in the cantons of central Switzerland without organized screening (Op-SC) between 2014 and 2020. Since 2014, a total of 19 236 patients from Or-SC and 2282 from Op-SC with breast cancer were compared. Age groups were defined as younger than 50 years, between 50 and 69 years, and older than 70 years.
Results
By comparison, women aged 50-69 years in the cantons of the Op-SC group exhibited significantly larger tumors T1-3 [point estimate of the difference with 95% confidence interval (CI) for T1: −7.7% (95% CI −11.0% to −4.4%); T2: 5.3% (95% CI 2.2% to 8.5%); T3: 2.5% (95% CI 0.8% to 4.2%)] and significantly fewer proportion of N0 [−5.7% (95% CI −9.0% to −2.5%)] without significant difference in the M status (P = 0.97).
Conclusion
Our study shows that patients aged 50-69 years from Op-SC have significantly larger tumors and higher incidence of lymph node metastases than women in the corresponding Or-SC group. This globally unique case within one single small country with very high living standards, but with different screening strategies, indicates the benefits of organized breast screening programs.
Key words: breast cancer screening, breast cancer, cancer stage
Highlights
-
•
Patients from Op-SC areas have larger tumors.
-
•
Patients from Op-SC areas have higher numbers of lymph node metastases.
-
•
The Or-SC group shows higher frequency of stage I disease.
Introduction
European recommendations suggest that breast cancer screening should be organized for women between the ages of 50 and 69 years.1 Although the European Union has recommended since 2003 that states implement organized-screening programs, individual countries in Europe have followed different strategies. Almost all European countries, however, now operate national screening programs or are about to introduce them.2 Switzerland is one of the last few countries that has not established a comprehensive, nationally organized program for breast cancer screening.3,4
Switzerland is a small European country that boasts one of the most highly developed health care systems in the world, and that ranks among the three best health care systems globally in terms of quality and accessibility.5 Income and living standards are high and distributed relatively homogeneously throughout the country.
In the federated structure of Switzerland, each of the 26 cantons is responsible for its own health policy. Although most cantons now organize quality-controlled and population-based mammography screening programs, these programs are not universal across Switzerland. In a few cantons, opportunistic early detection examinations take place only after a referral from the gynecologist or family doctor. This is the case in the central Swiss cantons, consisting of Lucerne, Nidwalden, Obwalden, and Uri.6 Around one-eighth of Switzerland’s current population of 8 million lives in the central Swiss cantons.7
Due to this form of federalism, each canton is responsible for organizing cancer screening according to its own strategies. Therefore, the small differences between different screening programs cannot be described in detail in this publication.
For this reason, we aimed to compare the breast cancer data since 2014 between screening cantons (Or-SC) and opportunistic-screening cantons (Op-SC) in central Switzerland to determine whether there are differences in pathological tumor sizes [TNM (tumor–node–metastasis) and International Union Against Cancer (Union Internationale Contre le Cancer) (UICC) stages] at disease presentation. Our objective is to compare the differences in disease presentation under two different models of health care policy within a single country, in order to investigate the potential value and consequences of breast cancer screening programs.
Materials and methods
Data analysis
Data originating from the national cancer dataset of the Swiss National Cancer Registration Office (NKRS), collected between 2014 and 2020, were used for the analysis (https://www.nkrs.ch/de/daten/). All data come from the cantons in Switzerland. All oncological tumors are collected and registered there by law.
In Switzerland, all oncological cancers are documented by the NKRS for national monitoring and reporting.
Tumors were classified according to TNM and UICC stage, based on the available pathological and clinical information, using the following international criteria8:
T status
-
•
TX: Primary tumor cannot be assessed
-
•
T0: No evidence of primary tumor
-
•
T1: Tumor ≤2 cm
-
•
T2: Tumor >2 cm but <5 cm
-
•
T3: tumor >5 cm
-
•
T4: Tumor of any size with direct extension to the chest wall or skin
For the analysis of TNM distribution, in situ tumors were excluded. We only include primary invasive cancers.
N status
-
•
NX: Regional lymph nodes cannot be evaluated
-
•
N0: No regional lymph node metastases
-
•
N1: Metastasis in mobile ipsilateral axillary lymph nodes
-
•
N2: Metastases to ipsilateral axillary lymph nodes, to each other, or to other structures fixed or absent in clinically identifiable ipsilateral lymph nodes along the internal mammary artery clinically evident axillary lymph node metastases
-
•
N3: Metastases in ipsilateral infraclavicular lymph nodes with or without involvement of the axillary ones. Lymph nodes or clinically recognizable ipsilateral lymph nodes along the mammary artery in the presence of clinically evident axillary lymph node metastases or metastases in ipsilateral supraclavicular lymph nodes.
M status
-
•
MX: Distant metastases cannot be assessed
-
•
M0: No distant metastases
-
•
M1: Distant metastases
Cantons with versus cantons without breast cancer screening
We compared the size distribution of cantons with an organized cantonal breast screening program (Or-SC) with those in central Switzerland that have no such program (Op-SC). There are still a few other cantons that offer only opportunistic screening. However, since these cantons are geographically dispersed and not contiguous, and since most cantons are already making efforts to introduce screening, these cantons were not analyzed. In the mentioned years of inclusion, there was an established and ongoing screening procedure in the respective cantons under international guidelines. The following cantons are involved:
Swiss cantons with a cantonal organized-screening program (Or-SC) since 2010 are as follows:
-
•
Vaud
-
•
Valais/Wallis
-
•
Geneva
-
•
Freiburg/Fribourg
-
•
Jura
-
•
Neuenburg/Neuchâtel
-
•
St Gallen
-
•
Thurgau
Swiss cantons with a cantonal screening program (Or-SC) since 2014 are as follows:
-
•
Grisons
-
•
Berne
-
•
Basel-City
Cantons from central Switzerland with only an Op-SC are as follows:
-
•
Lucerne
-
•
Nidwalden
-
•
Obwalden
-
•
Uri
Overall, we compared 19 236 patients in the Or-SC group and 2282 patients in the Op-SC group who had breast cancer since 2014. Patients were divided into age groups: younger than 50 years, between 50 and 69 years, and 70 years and older.
Statistical analysis
Data from individual Swiss cantons, as collected by the Swiss National Institute for Cancer Epidemiology and Registration (NICER), were collated. The data were evaluated by our statistician and an epidemiologist using the software R (version 4.2.1) (kaufmann@biostatistics.ch). P values were calculated using the chi-square test by comparing the frequencies of TNM between Or-SC and Op-SC (degrees of freedom: df = 3 for T, N, UICC; df = 1 for M) for every age group over all cancer status simultaneously (bold values in tables) as well as for every cancer status separately. Because of the explorative nature of the analysis, no adjustment for multiple testing has been made. 95% confidence intervals (CIs) were calculated with the two-sample test for equality of proportions for each stage individually.
Results
Table 1 summarizes numbers of breast cancers diagnosed in Switzerland between 2014 and 2020 for cantonal screening cantons (Or-SC) with organized mammographic screening and for opportunistic-screening cantons (Op-SC) without organized mammographic screening.
Table 1.
Number of breast cancers diagnosed in Switzerland between 2014 and 2020 for Or-SC and Op-SC
| No. of diagnosed breast cancers | |||
|---|---|---|---|
| Age (years) | Op-SC | Or-SC | Total |
| <50 | 445 | 3654 | 4099 |
| 50-69 | 1026 | 8598 | 9624 |
| 70+ | 811 | 6984 | 7795 |
| Total | 2282 | 19236 | 21518 |
Op-SC, opportunistic-screening cantons; Or-SC, organized-screening cantons.
T status
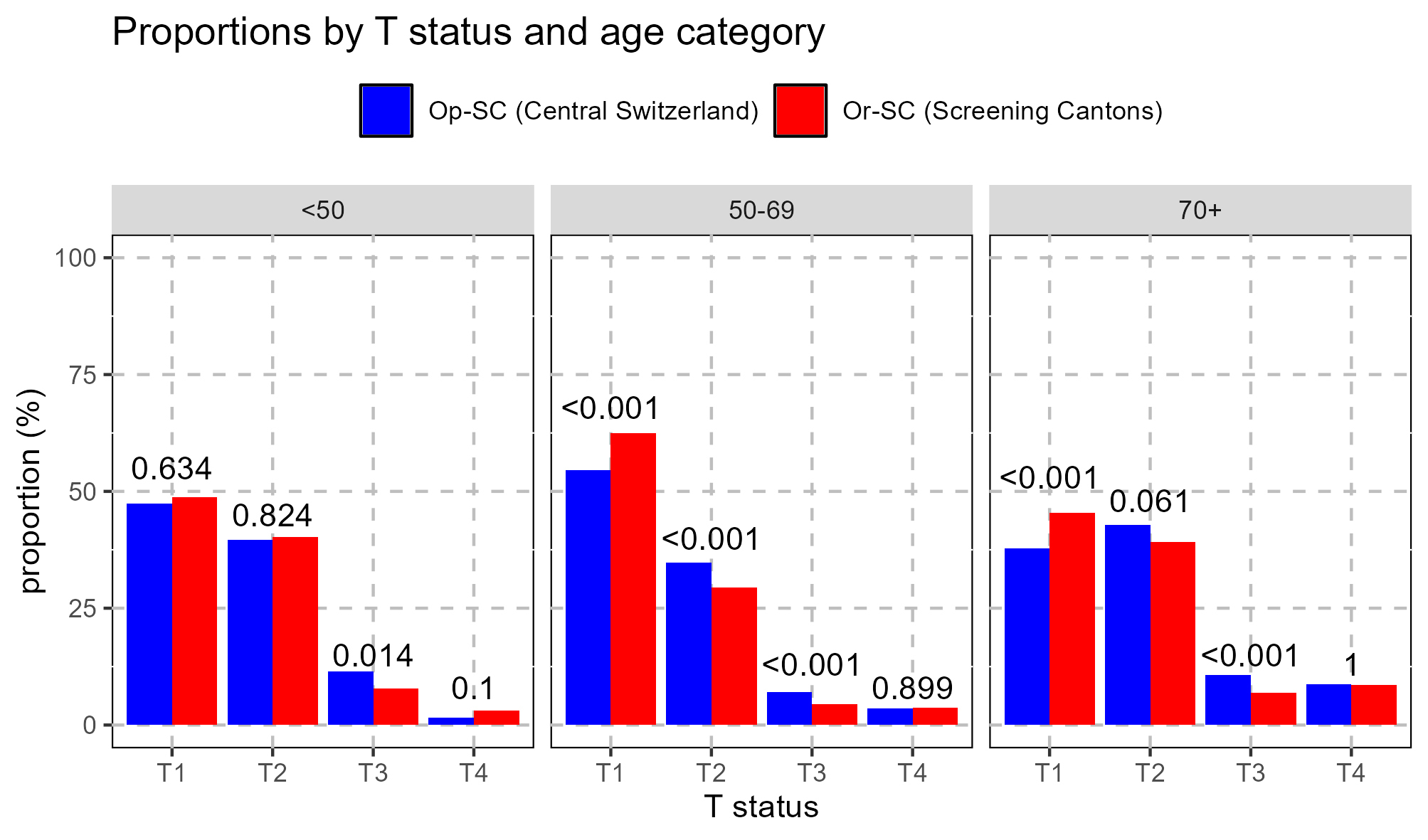
The T-status data are summarized in Table 2 and Supplementary Figure S1, available at https://doi.org/10.1016/j.esmoop.2024.103712. The chi-square test showed statistical significant differences between Op-SC and Or-SC for the age groups 50-69 and 70+ years (P < 0.001).
Table 2.
Summary of the T status in the different age groups
| T status | Op-SC |
Or-SC |
Diff |
Chi-square |
|||
|---|---|---|---|---|---|---|---|
| n | % | n | % | % | 95% CI | P value | |
| <50 years | 439/445 | 3572/3654 | 0.025 | ||||
| T1 | 208 | 47.4 | 1740 | 48.7 | −1.3 | [−6.4, 3.7] | 0.634 |
| T2 | 174 | 39.6 | 1440 | 40.3 | −0.7 | [−5.7, 4.3] | 0.824 |
| T3 | 50 | 11.4 | 280 | 7.8 | 3.6 | [0.3, 6.8] | 0.014 |
| T4 | 7 | 1.6 | 112 | 3.1 | −1.5 | [−3.0, −0.1] | 0.1 |
| 50-69 years | 1003/1026 | 8348/8598 | <0.001 | ||||
| T1 | 548 | 54.6 | 5205 | 62.4 | −7.7 | [−11.0, −4.4] | <0.001 |
| T2 | 349 | 34.8 | 2461 | 29.5 | 5.3 | [2.2, 8.5] | <0.001 |
| T3 | 70 | 7.0 | 371 | 4.4 | 2.5 | [0.8, 4.2] | <0.001 |
| T4 | 36 | 3.6 | 311 | 3.7 | −0.1 | [−1.4, 1.1] | 0.899 |
| 70+ years | 727/811 | 6364/6984 | <0.001 | ||||
| T1 | 275 | 37.8 | 2887 | 45.4 | −7.5 | [−11.3, −3.7] | <0.001 |
| T2 | 311 | 42.8 | 2489 | 39.1 | 3.7 | [−0.2, 7.5] | 0.061 |
| T3 | 78 | 10.7 | 441 | 6.9 | 3.8 | [1.4, 6.2] | <0.001 |
| T4 | 63 | 8.7 | 547 | 8.6 | 0.1 | [−2.2, 2.3] | 1 |
Diff, difference; Op-SC, opportunistic-screening cantons; Or-SC, organized-screening cantons.
The bold numbers represent the number of actually analyzed cases in relation to the total number of breast cancers diagnosed as summarized in Table 1. The bold P values refer to the comparison of the two groups over all cancer status simultaneously of the respective age group.
In the age group 50-69 years, significantly larger tumors were detected in the Op-SC group compared with the Or-SC group, stage T1: −7.7% (95% CI −11.0% to −4.4%), T2: 5.3% (95% CI 2.2% to 8.5%), T3: 2.5% (95% CI 0.8% to 4.2%) (P < 0.001). The differences for stage T4: −0.1% (95% CI −1.4% to 1.1%) between the groups became statistically insignificant.
In the oldest age group, more tumors were detected in the Op-SC compared to the Or-SC for T1: −7.5% (95% CI −11.3% to −3.7%), T2: 3.7% (95% CI −0.2% to 7.5%), T3: 3.8% (95% CI 1.4% to 6.2%). The differences for T4: 0.1% (95% CI −2.2% to 2.3%) between the groups became statistically insignificant.
Notably, in the critical age group 50-69 years as well as in the 70+ years group, there was significantly larger tumors in the Op-SC compared with the Or-SC group.
N status
The chi-square test showed statistical significant differences between Op-SC and Or-SC for the age groups 50-69 and 70+ years (P < 0.001). In the age group 50-69 years, a smaller group of N0 was observed in the Op-SC compared with the Or-SC group: −5.7% (95% CI −9.0% to −2.5%). This was also observed in the older age group beginning from the age of 70 years: −9.9% (95%CI −13.9% to −6.0%). This means that N0 situations are observed much more frequently in the Or-SC, while in central Switzerland there are statistically more N1 patients [50-69 years: 4.4% (95% CI 1.3% to 7.4%) and 70+ years: 4.4% (95% CI 0.7% to 8.1%)].
The results are summarized in Table 3 and Supplementary Figure S2, available at https://doi.org/10.1016/j.esmoop.2024.103712.
Table 3.
Overview of N status in different age categories
| N status | Op-SC |
Or-SC |
Diff |
Chi-square |
|||
|---|---|---|---|---|---|---|---|
| n | % | n | % | % | 95% CI | P value | |
| <50 years | 439/445 | 3549/3654 | 0.191 | ||||
| N0 | 240 | 54.7 | 1956 | 55.1 | −0.4 | [−5.5, 4.6] | 0.9 |
| N1 | 132 | 30.1 | 1172 | 33.0 | −3 | [−7.6, 1.7] | 0.234 |
| N2 | 37 | 8.4 | 233 | 6.6 | 1.9 | [−1.0, 4.7] | 0.172 |
| N3 | 30 | 6.8 | 188 | 5.3 | 1.5 | [−1.1, 4.1] | 0.221 |
| 50-69 years | 995/1026 | 8253/8598 | <0.001 | ||||
| N0 | 597 | 60.0 | 5426 | 65.7 | −5.7 | [−9.0, −2.5] | <0.001 |
| N1 | 299 | 30.1 | 2121 | 25.7 | 4.4 | [1.3, 7.4] | <0.001 |
| N2 | 44 | 4.4 | 393 | 4.8 | −0.3 | [−1.8, 1.1] | 0.691 |
| N3 | 55 | 5.5 | 313 | 3.8 | 1.7 | [0.2, 3.3] | 0.01 |
| 70+ years | 710/811 | 5983/6984 | <0.001 | ||||
| N0 | 371 | 52.3 | 3719 | 62.2 | −9.9 | [−13.9, −6.0] | <0.001 |
| N1 | 228 | 32.1 | 1659 | 27.7 | 4.4 | [0.7, 8.1] | 0.016 |
| N2 | 60 | 8.5 | 353 | 5.9 | 2.6 | [0.3, 4.8] | 0.01 |
| N3 | 51 | 7.2 | 252 | 4.2 | 3 | [0.9, 5] | <0.001 |
Diff, difference; Op-SC, opportunistic-screening cantons; Or-SC, organized-screening cantons.
The bold numbers represent the number of actually analyzed cases in relation to the total number of breast cancers diagnosed as summarized in Table 1. The bold P values refer to the comparison of the two groups over all cancer status simultaneously of the respective age group.
M status
Particularly in the older age group of 70+ years, significantly more M1-stage tumors were found in the Op-SC group compared with the Or-SC group: 5.1% (95% CI 1.8% to 8.3%). In the other age groups, no significant differences were noted between the Op-SC and Or-SC groups in the distribution of the M stages. Data are summarized in Table 4 and Supplementary Figure S3, available at https://doi.org/10.1016/j.esmoop.2024.103712.
Table 4.
Different M status between Op-SC and Or-SC
| M status | Op-SC |
Or-SC |
Diff |
Chi-square |
|||
|---|---|---|---|---|---|---|---|
| n | % | n | % | % | 95% CI | P value | |
| <50 years | 382/445 | 3215/3654 | 0.754 | ||||
| 0 | 363 | 95.0 | 3038 | 94.5 | 0.5 | [−1.9, 3.0] | 0.754 |
| 1 | 19 | 5.0 | 177 | 5.5 | −0.5 | [−3.0, 1.9] | 0.754 |
| 50-69 years | 813/1026 | 7373/8598 | 0.97 | ||||
| 0 | 762 | 93.7 | 6918 | 93.8 | −0.1 | [−1.9, 1.7] | 0.97 |
| 1 | 51 | 6.3 | 455 | 6.2 | 0.1 | [−1.7, 1.9] | 0.97 |
| 70+ years | 537/811 | 5522/6984 | <0.001 | ||||
| 0 | 454 | 84.5 | 4948 | 89.6 | −5.1 | [−8.3, −1.8] | <0.001 |
| 1 | 83 | 15.5 | 574 | 10.4 | 5.1 | [1.8, 8.3] | <0.001 |
Diff, difference; Op-SC, opportunistic-screening cantons; Or-SC, organized-screening cantons.
The bold numbers represent the number of actually analyzed cases in relation to the total number of breast cancers diagnosed as summarized in Table 1. The bold P values refer to the comparison of the two groups over all cancer status simultaneously of the respective age group.
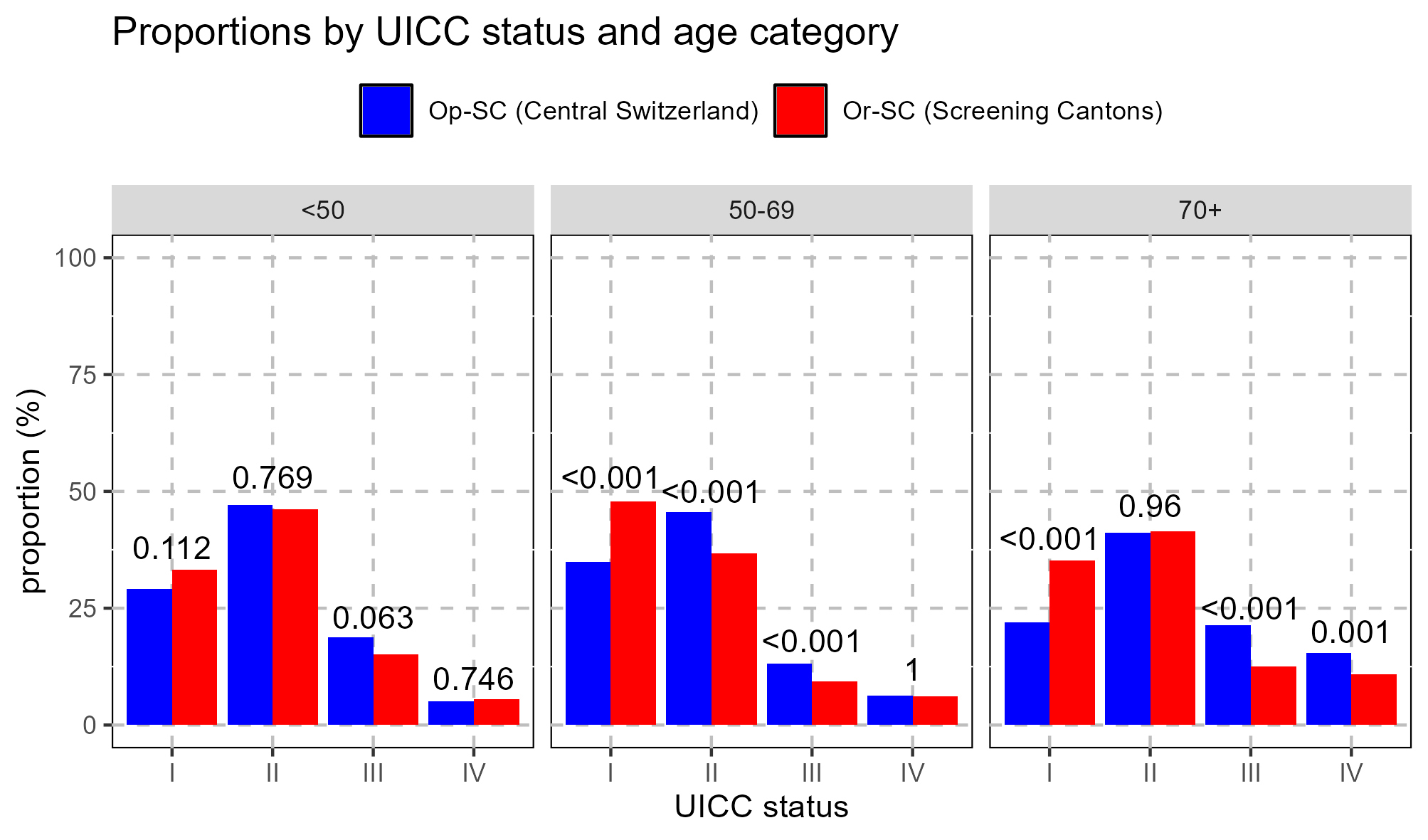
UICC stage
Given the larger size of tumors and higher relative of node-positive patients in the age group of 50-69 years, we grouped patients according to UICC stage.8 The chi-square test showed statistical significant differences between Op-SC and Or-SC for the age groups 50- 69 and 70+ years (P < 0.001). For 50-69 years, significantly more stage II patients were seen in the Op-SC group compared with the Or-SC group: 8.9% with (95% CI 5.2% to 12.5%) (Supplementary Figure S4, available at https://doi.org/10.1016/j.esmoop.2024.103712). The shift toward stage I in Or-SC is numerically evident in all age groups. However, within the age group typically included into screening programs (50-69 years) the shift toward higher stages, driven by more node-positive breast cancer and tumors larger than 2 cm, is clearly more pronounced in the Op-SC group (Supplementary Figure S4, available at https://doi.org/10.1016/j.esmoop.2024.103712 and Table 5).
Table 5.
Different UICC stages between Op-SC and Or-SC
| UICC status | Op-SC |
Or-SC |
Diff |
Chi-square |
|||
|---|---|---|---|---|---|---|---|
| n | % | n | % | % | 95% CI | P value | |
| <50 years | 382/445 | 3207/3654 | 0.155 | ||||
| I | 111 | 29.1 | 1066 | 33.2 | −4.2 | [−9.2, 0.8] | 0.112 |
| II | 180 | 47.1 | 1481 | 46.2 | 0.9 | [−4.5, 6.4] | 0.769 |
| III | 72 | 18.8 | 483 | 15.1 | 3.8 | [−0.5, 8.0] | 0.063 |
| IV | 19 | 5.0 | 177 | 5.5 | −0.5 | [−3.0, 1.9] | 0.746 |
| 50-69 years | 813/1026 | 7325/8598 | <0.001 | ||||
| I | 284 | 34.9 | 3499 | 47.8 | −12.8 | [−16.4, −9.3] | <0.001 |
| II | 371 | 45.6 | 2693 | 36.8 | 8.9 | [5.2, 12.5] | <0.001 |
| III | 107 | 13.2 | 678 | 9.3 | 3.9 | [1.4, 6.4] | <0.001 |
| IV | 51 | 6.3 | 455 | 6.2 | 0.1 | [−1.8, 1.9] | 1 |
| 70+ years | 534/811 | 5322/6984 | <0.001 | ||||
| I | 117 | 21.9 | 1871 | 35.2 | −13.2 | [−17.1, −9.4] | <0.001 |
| II | 220 | 41.2 | 2204 | 41.4 | −0.2 | [−4.7, 4.3] | 0.96 |
| III | 114 | 21.3 | 673 | 12.6 | 8.7 | [5.0, 12.4] | <0.001 |
| IV | 83 | 15.5 | 574 | 10.8 | 4.8 | [1.5, 8.0] | 0.001 |
Diff, difference; Op-SC, opportunistic-screening cantons; Or-SC, organized-screening cantons; UICC, Union Internationale Contre le Cancer.
The bold numbers represent the number of actually analyzed cases in relation to the total number of breast cancer diagnosed as summarized in Table 1. The bold P values refer to the comparison of the two groups over all cancer status simultaneously of the respective age group.
Discussion
In order to understand the meaning of this study, the reader needs to be aware of the political situation in Switzerland. In Switzerland, health policy is generally organized by the 26 cantons themselves. There has been a controversy in Switzerland for years about the benefits of mammography screening. For this reason, Switzerland is one of the last countries in Europe where organized mammography screening is not offered in the whole country.3,4
The majority of the 26 cantons have decided to introduce breast cancer screening. However, few cantons in central Switzerland decided not to begin implementing breast cancer screening. This study was carried out to describe tumor differences between cantons with an organized-screening program (Or-SC) and cantons in central Switzerland without organized screening (Op-SC).
In this study, we showed statistical significant differences between Op-SC and Or-SC for the age groups 50-69 and 70+ years for T, N, and UICC (P < 0.001). We showed that women aged 50-69 years in the Op-SC group of cantons in central Switzerland exhibited significantly larger tumors [T2: 5.3% (95% CI 2.2% to 8.5%) and T3: 2.5% (95% CI 0.8% to 4.2%) and fewer N0: −5.7% (95% CI −9.0% to −2.5%)], but without significant difference in the M status (P = 0.97) by comparison with cantons with Or-SC. These results are also observed for the elderly population >70 years of age, where the trend toward larger tumors with more node-positive situations in the Op-SC was observed (P < 0.001). The shift toward stage I in Or-SC is evident in all age groups.
Organized breast cancer screening usually consists of an officially recommended mammography, often including asymptomatic women (depending on the regulations in various countries).9 Almost all European countries have now established national screening programs,2 whereas opportunistic mammography—sought out by women on their own initiative or following the advice of their gynecologist or general practitioner—is an uncommon prevention strategy in Europe. Switzerland is the last remaining country in Europe without a national organized breast cancer screening program.3,4 While a small number of Swiss cantons, all of which are located in central Switzerland, employ only opportunistic mammography (Op-SC), the vast majority now prefer or plan an organized, cantonal screening program (Or-SC).
Reasons to doubt the efficacy of breast cancer screening include a large Canadian study which showed that annual mammography in women aged 40-59 years does not reduce mortality from breast cancer. In that study, 22% of detected invasive breast cancers were overdiagnosed, representing one overdiagnosed breast cancer for every 424 women who received a mammography.10 In Switzerland, such reports fueled controversy and led various ethics committees to reject general breast cancer screening, contrary to the position of many researchers worldwide.11, 12, 13
As a result of these discussions, health policy in Switzerland in recent years has been heterogeneous. While most cantons are opting for screening, several are following a policy of opportunistic screening.
The independence of the 26 Swiss cantons creates a unique situation in that each of them decides for itself whether or not to carry out official or opportunistic screening3,4,14 To our knowledge, there is no other country in Europe where individual parts of the country have implemented different policies regarding breast cancer screening.
In our view, the inconsistency of Swiss policies offers a unique chance to study the effects of screening within a fairly homogenous group of patients. Switzerland is a small country with one of the highest standards of medical care in the world and is homogeneous with high socioeconomic living standards.5
This presents an opportunity to compare cantons that have endorsed screening with those that have rejected it. In this study, we did not focus on overall mortality, as was the case in the Canadian and other studies.10
Our study demonstrates that women in the central Swiss cantons, particularly in the age group between 50 and 70 years, have larger tumors and a markedly higher number of lymph node metastases compared with the rest of Switzerland, where breast cancer screening is officially organized. With 25.7% of N1 patients, substantially fewer women between the ages of 50 and 69 years were documented as node-positive in the Or-SC group, compared with 30.1% women documented as node-positive in the Op-SC group. This difference is significant [4.4% (95% CI 1.3% to 7.4%)]. This shift especially toward higher node-positive disease is likely to require more aggressive local and systemic treatment,15, 16, 17, 18, 19, 20, 21, 22 with both health and economic consequences.
As far as the authors are aware, the benefits of breast cancer screening in potentially reducing the risk of lymph node metastases have never been inferred in this way. It would not be ethically justifiable to carry out such a study in which some regions of a country implemented breast cancer screening while some did not, which is also why there have been no such studies worldwide.
A study in Denmark23 showed that breast cancer screening was not associated with a reduction in the incidence of advanced cancer. However, this Danish study differed from our observations: Such studies were undertaken in countries that already have good health care for women and with organized-screening programs.
Our study also demonstrated that the M1 status in the groups of women up to 69 years of age was not statistically higher in the Op-SC group compared with the Or-SC group (P = 0.97). However, in the group of women aged >70 years in the Op-SC/Or-SC, there were patients who showed more extensive involvement when they were first diagnosed with distant metastases: 5.1% (95% CI 1.8% to 8.3%), P < 0.001. This fits very well with previous international studies, which showed that mammography screening reduces the extent of M1 diseases.24
An interesting phenomenon was observed among the older age group of >70 years. The tumors in this age group were larger in the Op-SC group than in the Or-SC group. This phenomenon is rarely described in the literature since it is considered that older people tend not to benefit from breast screening.25 We assume that in the Or-SC there is possibly a more established culture of conducting breast cancer screening, whereas in the Op-SC there is less experience with mammography. However, this is pure speculation and should be pursued in further studies.
Historically, the results of deviating from scientifically backed advice in health management have been well documented. Regional differences in breast cancer types in Switzerland have been reported for years, correlating to whether screening has been implemented or not.26,27
The effects of these differences on the mastectomy rate in Switzerland are also important. A recent study showed that the mastectomy rate has fallen significantly in Swiss regions with cantonal screening programs.28 We did not analyze our data for mastectomy rates. However, because of the large tumor stages, the therapies in central Switzerland are likely to be more extensive and potentially more costly. We will endeavor to analyze this data in the future. In Switzerland, the value of mammography screening has, until now, only been discussed from the perspective of mortality. What is completely forgotten is that the extent of therapy may have an impact on the quality of life.29 We have not specifically examined this aspect of breast cancer treatment in Switzerland. However, we assume that the large tumor stages in central Switzerland requiring extensive therapy may have a significant impact on the quality of life in survivors.
A recently published study in Switzerland showed that the introduction of screening programs does not reduce income inequality among the women examined. In this study it could be shown that there were much larger differences between married and unmarried women when it came to preventive breast examinations.30 For this reason, when introducing screening programs, attention should not only be paid to the screening itself, but above all women must be carefully informed about the benefits of such screening programs.
This study has limitations. Firstly, the epidemiological data in Switzerland are challenging to compare. We do not know what percentage of women in central Switzerland has taken part in opportunistic screening. There is no independent registration of how many women have examinations each year. In a more detailed analysis, it would be interesting to further differentiate the age groups, e.g. <40, 40-49, 50-69, >70 years. We have not received these data at the moment and are trying to investigate this in further analysis. Secondly, there are also differences among the screening cantons in how breast screening is carried out. Thirdly is the fact that we have no survival data. Further studies are urgently needed to show whether the unfavorable tumor stages also have an impact on survival and prognosis. Fourthly, the central Swiss registry follows international guidelines. It cannot be ruled out that there may be minor documentation errors, especially in clinical information such as metastatic disease. Finally, in a recently published discussion, considerable doubts were expressed about the scientific quality of the Canadian study mentioned above.10,31, 32, 33 If these doubts were to be confirmed, the entire scientific discussion in recent years would have to be reopened. Indirectly, these Swiss data would be the direct consequence, as political decision makers have repeatedly referred to this Canadian study to reject mammography screening in Switzerland.10,11 Since this is currently an open discussion, we do not want to speculate here and will wait for the final judgments.
Conclusions
The large region of central Switzerland with the cantons of Lucerne, Nidwalden, Uri, and Schwyz is the last big contiguous region in Europe that does not offer organized breast cancer screening, unlike most other Swiss cantons, where it has been established.
This study shows that women in central Switzerland have significantly larger tumors with significantly more cases of lymph node metastases than the other majority of Swiss regions with cantonal organized-screening programs. This study provides a unique insight into the benefits of organized breast cancer screening programs while also highlighting the potential negative consequences when the scientific evidence is not fully translated into clinical practice.
Acknowledgements
We thank the Swiss Cancer Registry (NICER), especially Ms Lea Wildisen, who collected the data for us. We also thank Ms Evelyne Kaufmann, who helped us as a statistician, especially analyzing and correcting all original data and providing support with the figures.
Funding
This work was supported with a total of 6000 CHF by the Cancer League of Central Switzerland in Krebsliga Luzern.
Disclosure
The authors have declared no conflicts of interest.
Supplementary data
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
- 1.European Commission Initiative on Breast Cancer Cancer Screening, Diagnosis and Care. https://healthcare-quality.jrc.ec.europa.eu/ecibc Available at.
- 2.Deandrea S., Molina-Barceló A., Uluturk A., et al. Presence, characteristics and equity of access to breast cancer screening programmes in 27 European countries in 2010 and 2014. Results from an international survey. Prev Med. 2016;91:250–263. doi: 10.1016/j.ypmed.2016.08.021. [DOI] [PubMed] [Google Scholar]
- 3.Herrmann C., Vounatsou P., Thürlimann B., Probst-Hensch N., Rothermundt C., Ess S. Impact of mammography screening programmes on breast cancer mortality in Switzerland, a country with different regional screening policies. BMJ Open. 2018;8(3) doi: 10.1136/bmjopen-2017-017806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ess S., Savidan A., Frick H., et al. Geographic variation in breast cancer care in Switzerland. Cancer Epidemiol. 2010;34(2):116–121. doi: 10.1016/j.canep.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 5.GBD 2015. Healthcare access and quality index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990–2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet. 2017;390:231–266. doi: 10.1016/S0140-6736(17)30818-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.https://www.swisscancerscreening.ch/de/ Available at.
- 7.https://ec.europa.eu/eurostat/en/web/population-demography-migration-projections/statistics-illustrated Available at.
- 8.Teichgraeber D.C., Guirguis M.S., Whitman G.J. Breast cancer staging: updates in the AJCC Cancer Staging Manual, 8th edition, and current challenges for radiologists, from the AJR special series on cancer staging. AJR Am J Roentgenol. 2021;217(2):278–290. doi: 10.2214/AJR.20.25223. [DOI] [PubMed] [Google Scholar]
- 9.Peisl S., Zimmermann S., Camey B., et al. Comparison between opportunistic and organised breast cancer mammography screening in the Swiss canton of Fribourg. BMC Cancer. 2019;19:469. doi: 10.1186/s12885-019-5706-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miller A.B., Wall C., Baines C.J., Sun P., To T., Narod S.A. Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ. 2014;348 doi: 10.1136/bmj.g366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Biller-Andorno N., Jüni P. Abolishing mammography screening programs? A view from the Swiss Medical Board. N Engl J Med. 2014;370(21):1965–1967. doi: 10.1056/NEJMp1401875. [DOI] [PubMed] [Google Scholar]
- 12.Arie S. Switzerland debates dismantling its breast cancer screening programme. BMJ. 2014;348:g1625. doi: 10.1136/bmj.g1625. [DOI] [PubMed] [Google Scholar]
- 13.Swiss Medical Board Systematisches Mammographie-Screening. https://www.swissmedicalboard.ch/fileadmin/public/news/2013/bericht_smb_mammographie_screening_lang_2013.pdf Available at.
- 14.Eichholzer M., Richard A., Rohrmann S., et al. Breast cancer screening attendance in two Swiss regions dominated by opportunistic or organized screening. BMC Health Serv Res. 2016;16:519. doi: 10.1186/s12913-016-1760-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nottegar A., Veronese N., Senthil M., et al. Extra-nodal extension of sentinel lymph node metastasis is a marker of poor prognosis in breast cancer patients: a systematic review and an exploratory meta-analysis. Eur J Surg Oncol. 2016;42:919–925. doi: 10.1016/j.ejso.2016.02.259. [DOI] [PubMed] [Google Scholar]
- 16.Stranzl H., Ofner P., Peintinger F. Postoperative irradiation in breast cancer patients with one to three positive axillary lymph nodes. Is there an impact of axillary extranodal tumor extension on locoregional and distant control? Strahlenther Onkol. 2006;182(10):583–588. doi: 10.1007/s00066-006-1562-4. [DOI] [PubMed] [Google Scholar]
- 17.Bucci J.A., Kennedy C.W., Burn J., et al. Implications of extranodal spread in node positive breast cancer: a review of survival and local recurrence. Breast. 2001;10(3):213–219. doi: 10.1054/brst.2000.0233. [DOI] [PubMed] [Google Scholar]
- 18.Dobi E., Bazan F., Dufresne A., et al. Is extracapsular tumour spread a prognostic factor in patients with early breast cancer? Int J Clin Oncol. 2013;18(4):607–613. doi: 10.1007/s10147-012-0439-z. [DOI] [PubMed] [Google Scholar]
- 19.Neri A., Marrelli D., Roviello F., et al. Prognostic value of extracapsular extension of axillary lymph node metastases in T1 to T3 breast cancer. Ann Surg Oncol. 2005;12(3):246–253. doi: 10.1245/ASO.2005.02.029. [DOI] [PubMed] [Google Scholar]
- 20.Choi A.H., Surrusco M., Rodriguez S., et al. Extranodal extension on sentinel lymph node dissection: why should we treat it differently? Am Surg. 2014;80(10):932–935. [PubMed] [Google Scholar]
- 21.Stitzenberg K.B., Meyer A.A., Stern S.L., et al. Extracapsular extension of the sentinel lymph node metastasis: a predictor of nonsentinel node tumor burden. Ann Surg. 2003;237(5):607–612. doi: 10.1097/01.SLA.0000064361.12265.9A. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Aziz S., Wik E., Knutsvik G., et al. Extra-nodal extension is a significant prognostic factor in lymph node positive breast cancer. PLoS One. 2017;12(2) doi: 10.1371/journal.pone.0171853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jørgensen K.J., Gøtzsche P.C., Kalager M., Zahl P.H. Breast cancer screening in Denmark: a cohort study of tumor size and overdiagnosis. Ann Intern Med. 2017;166(5):313–323. doi: 10.7326/M16-0270. [DOI] [PubMed] [Google Scholar]
- 24.Duffy S.W., Tabár L., Yen A.M., et al. Mammography screening reduces rates of advanced and fatal breast cancers: results in 549,091 women. Cancer. 2020;126(13):2971–2979. doi: 10.1002/cncr.32859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Collins K., Winslow M., Reed M., et al. The views of older women towards mammographic screening: a qualitative and quantitative study. Br J Cancer. 2010;102:1461–1467. doi: 10.1038/sj.bjc.6605662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bulliard J.L., La Vecchia C., Levi F. Diverging trends in breast cancer mortality within Switzerland. Ann Oncol. 2006;17(1):57–59. doi: 10.1093/annonc/mdj035. [DOI] [PubMed] [Google Scholar]
- 27.Ess S., Savidan A., Frick H., et al. Geographic variation in breast cancer care in Switzerland. Cancer Epidemiol. 2010;34(2):116–121. doi: 10.1016/j.canep.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 28.Herrmann C., Morant R., Walser E., Mousavi M., Thürlimann B. Screening is associated with lower mastectomy rates in eastern Switzerland beyond stage effects. BMC Cancer. 2021;21(1):229. doi: 10.1186/s12885-021-07917-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ghislain I., Zikos E., Coens C., et al. European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life Group; Breast Cancer Group; EORTC Headquarters. Health-related quality of life in locally advanced and metastatic breast cancer: methodological and clinical issues in randomised controlled trials. Lancet Oncol. 2016;17(7):e294–e304. doi: 10.1016/S1470-2045(16)30099-7. [DOI] [PubMed] [Google Scholar]
- 30.Jolidon V., De Prez V., Bracke P., Bell A., Burton-Jeangros C., Cullati S. Revisiting the effects of organized mammography programs on inequalities in breast screening uptake: a multilevel analysis of nationwide data from 1997 to 2017. Front Public Health. 2022;10 doi: 10.3389/fpubh.2022.812776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yaffe M.J., Seely J.M., Gordon P.B., Appavoo S., Kopans D.B. The randomized trial of mammography screening that was not—a cautionary tale. J Med Screen. 2022;29(1):7–11. doi: 10.1177/09691413211059461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wilkinson A.N., Ellison L.F., Billette J.M., Seely J.M. Impact of breast cancer screening on 10-year net survival in Canadian women age 40-49 years. J Clin Oncol. 2023;41(29):4669–4677. doi: 10.1200/JCO.23.00348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wilkinson A.N., Billette J.M., Ellison L.F., Killip M.A., Islam N., Seely J.M. The impact of organised screening programs on breast cancer stage at diagnosis for Canadian women aged 40-49 and 50-59. Curr Oncol. 2022;29(8):5627–5643. doi: 10.3390/curroncol29080444. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.