

Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. Risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with estradiol rather than conjugated estrogen.
Key Words: Cancers, Cardiovascular conditions, Dementia, Menopausal hormone therapy, Survival
Abstract
Objectives
The study aims to assess the use of menopausal hormone therapy beyond age 65 years and its health implications by types of estrogen/progestogen, routes of administration, and dose strengths.
Methods
Using prescription drug and encounter records of 10 million senior Medicare women from 2007-2020 and Cox regression analyses adjusted for time-varying characteristics of the women, we examined the effects of different preparations of menopausal hormone therapy on all-cause mortality, five cancers, six cardiovascular diseases, and dementia.
Results
Compared with never use or discontinuation of menopausal hormone therapy after age 65 years, the use of estrogen monotherapy beyond age 65 years was associated with significant risk reductions in mortality (19% or adjusted hazards ratio, 0.81; 95% CI, 0.79-0.82), breast cancer (16%), lung cancer (13%), colorectal cancer (12%), congestive heart failure (CHF) (5%), venous thromboembolism (3%), atrial fibrillation (4%), acute myocardial infarction (11%), and dementia (2%). For the use of estrogen and progestogen combo-therapy, both E+ progestin and E+ progesterone were associated with increased risk of breast cancer by 10%-19%, but such risk can be mitigated using low dose of transdermal or vaginal E+ progestin. Moreover, E+ progestin exhibited significant risk reductions in endometrial cancer (45% or adjusted hazards ratio, 0.55; 95% CI, 0.50-0.60), ovarian cancer (21%), ischemic heart disease (5%), CHF (5%), and venous thromboembolism (5%), whereas E+ progesterone exhibited risk reduction only in CHF (4%).
Conclusions
Among senior Medicare women, the implications of menopausal hormone therapy use beyond age 65 years vary by types, routes, and strengths. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with E2 rather than conjugated estrogen.
In 2002, the Women's Health Initiative (WHI) trial reported that menopausal estrogen + progestogen therapy (EPT) in menopausal women average age 63 years increased the occurrence of invasive breast cancer, stroke, and coronary heart disease,1 although it reduced fractures. The press presented the negative outcomes in a dramatic manner that some described as misleading.2,3 However, most of these negative results lost significance when corrected for multiple testing.1 The second WHI study in 2004 examined the effect of estrogen therapy (ET) on these same outcomes in similar aged but hysterectomized women and reported a near significant reduction in breast cancer,4 which became a significant 22% reduction in WHI's long-term follow-up of that study.5 However, these positive results got little press attention and did little to reduce the fears about hormone therapy (HT) that had been already implanted in the public's mind. The US Food and Drug Administration has required all estrogen-containing products to include a black-box warning for serious adverse events associated with its use, even though the WHI trials only studied one type (conjugated estrogen), dosage (0.625 mg), and route (oral) of estrogen alone and in combination with one type of progestogen (medroxyprogesterone acetate 2.5 mg). Furthermore, continuing or initiating HT after 65 years is rarely recommended. Until recently, it was often thought that women do not need hormone therapy much after menopause because no serious menopausal symptoms persist in women aged 65 years or older. However, studies reported that menopausal vasomotor symptoms persisted for 7-12 years in many women,6 and some vasomotor symptoms persisted in 42.1% of women aged 60-65 years,7 which suggests that not few numbers of women continue to suffer from vasomotor symptoms even after age 65 years. According to the 2022 HT position statement of The North American Menopause Society (NAMS),8 there is no general rule for stopping HT in a woman aged 65 years. For healthy women with persistent vasomotor symptoms, continuing HT beyond age 65 years is a reasonable option with appropriate counseling and regular assessment of risks and benefits. Moreover, the mitigation of risks through the choice of low dose, nonoral, and different estrogen and progestogen becomes increasingly important as women age. However, information on the effects of different HT formulation, dosing, and route of administration is lacking.
The US Centers for Medicare and Medicaid Services (CMS) Virtual Research Data Center (VRDC)9 carries 14 years of prescription claims and 21 years of encounter claims as well as vital status for almost all US women aged 65 years or older, and thus menopausal. So, VRDC provides HT exposure data as well as outcomes data about death, dementia, cardiovascular (CV), and cancer conditions like those studied by the WHI trials. Given that at least 2%-7% of elderly women still use HT after age 65 years,10 VRDC data are large enough to shed light on the consequences of HT use after 65 years by doses, routes, and types. We implemented extended Cox regression analyses11,12 to assess the association of these factors with death, dementia, CV, and cancer outcomes. Here we report the results of these analyses.
METHODS
Study population
The CMS provided us access to all available records of Medicare Parts A (hospital insurance, 1999-2020), B (medical insurance, 1999-2020), C (Medicare Advantage [MA], 2015-2020), and D (prescription drug insurance, 2007-2020) claims data for 100% Medicare enrollees. We constrained our study individuals to women who were first entitled to Medicare near age 65 years (±1 month) and during the full years of Part D benefits (ie, 2007-2020)—a total of 14 years. We only included enrollees with at least 6 months of data to assure enough follow-up time.
We report usage trends broken down by year, HT type, and route, using the number of Part D female enrollees in each year as the denominator. We report descriptive statistics that outline the demographics, socioeconomic status, the prevalence of 49 chronic conditions among women in the study, and the corresponding crude rates of outcomes.
HT exposures
We classified HT by types, routes, and dose strengths, as applicable. We included three types of estrogen (estradiol [E2], conjugated estrogen [CEE], and ethinyl estradiol [EE]), two types of progestogen (progesterone [natural] or progestin [synthetic]), and a total of nine different estrogen-progestogen combinations (E2 alone, E2+ progesterone, E2+ progestin, CEE alone, CEE+ progesterone, CEE+ progestin, EE+ progestin, progesterone alone, and progestin alone). EE was never prescribed alone and always combined only with progestin. Routes and dose strengths were solely based on the estrogen part of preparations. The routes included oral, transdermal, vaginal, and injectable. We developed an average daily estrogen dose based on DailyMed13 dosing instructions for each of 138 individual HT products (Supplemental Digital Content 1, http://links.lww.com/MENO/B236), which accommodated intermittent regimens (eg, 21 days on and 7 days off). We defined a “standard” dose for estrogen type and route based on the literature and the distribution of daily estrogen doses as 0.625 mg, 1 mg, and 5 μg for oral CEE, E2, and EE, respectively, and 200 μg and 50 μg for nonoral CEE and E2, respectively. For each drug type, we categorized the average daily estrogen doses into high, greater than 1.45 times the standard; low, less than 0.45 times the standard; and medium, between the lower end of the high and the upper end of the low bounds. We considered each combination of estrogen-progestogen preparation, dose strength, and route as separate covariates (total 40; 16 ET and 24 EPT preparations). We considered women to be exposed to a study drug if they ever had a prescription for that drug before an outcome event.
We only included HT medications with indications for menopausal symptoms and excluded those indicated for birth control or for vaginal bleeding.
Outcomes
Our goals were to describe the usage of HT in women age ≥65 years and to determine the influence of such usage on survival and on the occurrence of WHI-like outcomes (five cancers, six CV conditions, and dementia).1,4 The five cancer outcomes included breast, lung, endometrial, colorectal, and ovarian cancers. The six CV outcomes included ischemic heart diseases (IHD), heart failure (HF), venous thromboembolism (VTE), stroke, atrial fibrillation (AF), and acute myocardial infarction (AMI). The occurrence and onset date for all but ovarian cancer and VTE were predefined by algorithm in Medicare's CCW (Chronic Condition Data Warehouse).14 We generated comparable occurrence data by examining ICD-9/ICD-10-CM codes for ovarian cancer (183.0 and C56) and VTE (415.1, 451, 453, I26, I80, I82), respectively.
Statistical analysis
We explored the independent effect of each HT drug on the 13 outcomes listed above using separate extended Cox regression analyses. To mitigate potential confounding factors influencing 13 health outcomes, we incorporated a comprehensive set of adjustments. This included 40 combinations of estrogen-progestogen type, routes, and dose ranges along with consideration for race, degree of low-income subsidy (LIS) as a surrogate for income, rural residence indicator, calendar year of Medicare Part D enrollment, and the 49 CCW chronic conditions14 with >1% prevalence, to adjust for overall medical burden. Notably, we did not include interactions between these variables. We treated all covariates except race as time-varying to avoid the risk of an immortal time bias and protect against violations of the proportional hazards assumption.11,12 When a cancer, CV condition, or dementia was the outcome, we excluded all other cancers, CV conditions, or dementia conditions as covariates, respectively.
Women became eligible for the study at the time of their Medicare entitlement, but prescription records were unavailable until their Part D enrollment. Many enrollees disenrolled from Medicare or switched from Medicare Fee-For-Service (FFS) to MA, and we only had MA encounter data after 2015. We followed women from their entry to Part D (while accounting for left truncation15) until they (1) developed a nondeath outcome, (2) died, (3) switched to an MA plan before 2015, (4) disenrolled from Medicare, or (5) reached December 31, 2020 (the end of our data availability), whichever came first. In order to (1) mitigate selection bias toward HT use and to (2) correct for potential bias from informative censoring, we developed two time-varying propensity scores (PS) using logistic regressions.16,17 The first was for the likelihood of taking any HT and the second for the likelihood of switching from Medicare FFS to MA or disenrolling from Medicare altogether and thus dropping out of the study. Both PS were conditional probabilities based on characteristics of women and were iteratively estimated every 6 months among women who remained in follow-up considering all covariate values in a given 6-month cycle.17 We ran all Cox regression analyses with these time-varying PS as additional adjustments.18,19
This study was declared not human subject research by the Office of Human Research Protection at the National Institutes of Health and by the CMS's Privacy Board.
RESULTS
Study population and secular trends
From 100% senior Medicare women, more than 19 million satisfied our selection criteria. The death cohort, our largest, included 10,944,328 women with at least 6-month follow-up, and a modest 14% of them ever used some type of HT during our study period (Table 1). The disease-specific cohorts were slightly smaller in number but had similar proportions of HT users.
Table 1.
Baseline characteristics
| Any HT | No HT | |
|---|---|---|
| N | 1,522,914 | 9,421,414 |
| Age at Part D entry, median (IQR) | 65.1 (1.8) | 65.2 (2.0) |
| White | 1,318,141 (86.6) | 7,190,911 (76.3) |
| Black | 58,046 (3.8) | 843,205 (8.9) |
| Hispanic | 74,929 (4.9) | 763,573 (8.1) |
| Asian | 29,115 (1.9) | 354,405 (3.8) |
| Other (American Indian/Alaska Native/other/unknown) | 42,683 (2.8) | 269,320 (2.9) |
| Ever dual | 137,971 (9.1) | 1,529,002 (16.2) |
| Nondual LIS | 21,272 (1.4) | 243,114 (2.6) |
| Nondual No LIS | 1,363,671 (89.5) | 7,649,298 (81.2) |
| Living in rural area | 376,104 (24.7) | 2,250,675 (23.9) |
| Hysterectomy | 344,888 (22.6) | 1,052,327 (11.2) |
| Pulmonary embolism | 34,123 (2.2) | 214,810 (2.3) |
| Deep vein thrombosis | 108,464 (7.1) | 567,378 (6.0) |
| AMI | 31,057 (2.0) | 230,171 (2.4) |
| Atrial fibrillation | 119,019 (7.8) | 673,930 (7.2) |
| Heart failure | 167,025 (11.0) | 1,079,368 (11.5) |
| Ischemic heart disease | 415,086 (27.3) | 2,155,496 (22.9) |
| Stroke/transient ischemic attack | 117,021 (7.7) | 648,402 (6.9) |
| Cataract | 1,034,791 (67.9) | 4,909,261 (52.1) |
| Chronic kidney disease | 367,841 (24.2) | 2,413,925 (25.6) |
| COPD | 275,100 (18.1) | 1,652,633 (17.5) |
| Diabetes | 360,825 (23.7) | 2,768,069 (29.4) |
| Glaucoma | 322,074 (21.1) | 1,572,196 (16.7) |
| Hip/pelvic fracture | 25,232 (1.7) | 142,053 (1.5) |
| Depression | 607,150 (39.9) | 2,850,648 (30.3) |
| Alzheimer disease or senile dementia | 94,770 (6.2) | 497,831 (5.3) |
| Osteoporosis | 436,950 (28.7) | 2,177,348 (23.1) |
| Rheumatoid arthritis/osteoarthritis | 969,801 (63.7) | 4,527,781 (48.1) |
| Breast cancer | 100,093 (6.6) | 848,430 (9.0) |
| Colorectal cancer | 23,260 (1.5) | 160,717 (1.7) |
| Lung cancer | 22,412 (1.5) | 173,300 (1.8) |
| Endometrial cancer | 21,590 (1.4) | 154,919 (1.6) |
| Cervical cancer | 7,564 (0.5) | 40,027 (0.4) |
| Ovarian cancer | 14,785 (1.0) | 85,744 (0.9) |
| Anemia | 597,850 (39.3) | 3,027,915 (32.1) |
| Asthma | 262,736 (17.3) | 1,203,273 (12.8) |
| Hyperlipidemia | 1,181,576 (77.6) | 6,729,384 (71.4) |
| Hypertension | 1,029,579 (67.6) | 6,348,246 (67.4) |
| Hypothyroidism | 570,897 (37.5) | 2,620,862 (27.8) |
| Alcohol use disorders | 33,192 (2.2) | 226,301 (2.4) |
| Anxiety disorders | 551,258 (36.2) | 2,493,674 (26.5) |
| Bipolar disorder | 61,278 (4.0) | 288,021 (3.1) |
| Major depressive affective disorder | 495,299 (32.5) | 2,344,371 (24.9) |
| Drug use disorder | 74,027 (4.9) | 408,375 (4.3) |
| Personality disorders | 46,934 (3.1) | 185,116 (2.0) |
| Schizophrenia and other psychotic disorders | 26,984 (1.8) | 168,373 (1.8) |
| Epilepsy | 30,689 (2.0) | 186,948 (2.0) |
| Cystic fibrosis and other metabolic developmental disorders | 40,678 (2.7) | 178,588 (1.9) |
| Fibromyalgia, chronic pain, and fatigue | 694,459 (45.6) | 2,967,678 (31.5) |
| Viral hepatitis (general) | 18,616 (1.2) | 131,259 (1.4) |
| Liver disease cirrhosis and other liver conditions (excluding hepatitis) | 184,114 (12.1) | 988,450 (10.5) |
| Leukemias and lymphomas | 28,341 (1.9) | 149,327 (1.6) |
| Migraine and other chronic headache | 204,319 (13.4) | 697,762 (7.4) |
| Mobility impairments | 32,956 (2.2) | 240,224 (2.5) |
| Obesity | 418,568 (27.5) | 3,148,871 (33.4) |
| Overarching OUD disorder | 45,948 (3.0) | 174,336 (1.9) |
| Peripheral vascular disease | 224,929 (14.8) | 1,415,992 (15.0) |
| Tobacco use disorders | 122,033 (8.0) | 1,128,128 (12.0) |
| Pressure ulcers and chronic ulcers | 56,123 (3.7) | 367,769 (3.9) |
| Sensory—deafness and hearing impairment | 219,459 (14.4) | 843,768 (9.0) |
Note: data are presented as n (%) of participants unless otherwise noted.
AMI, acute myocardial infarction; COPD, chronic obstructive pulmonary disease; HT, hormone therapy; IQR, interquartile range; LIS, low income subsidy; OUD, opioid use disorder.
Over 14 years of follow-up (2007-2020), the proportion of senior women taking any HT containing estrogen dropped by half, from 11.4% to 5.5%. E2 tended to replace CEE. EPT plummeted from 1.4% to a minuscule 0.2% (Fig. 1A), and the vaginal route tended to replace oral route (Fig. 1B). Overall, the number of ET users was >10 times greater than that of EPT or progestogen alone users. Among ET users, the predominant route was vaginal. Twice as many women were on vaginal and ⅓ as many on transdermal as on oral preparations. Among EPT users, the most common type of EPT was E2+ progestin, followed by CEE+ progestin, E2+ progesterone, EE+ progestin, and then CEE+ progesterone (Supplemental Digital Contents 2 and 3, http://links.lww.com/MENO/B236). All EE+ progestin preparations were a combination of EE and norethindrone, and we did not include 4% of EE+ progestin preparations indicated for birth control for consistency's sake, although that indication was not relevant for our senior women.
FIG. 1.
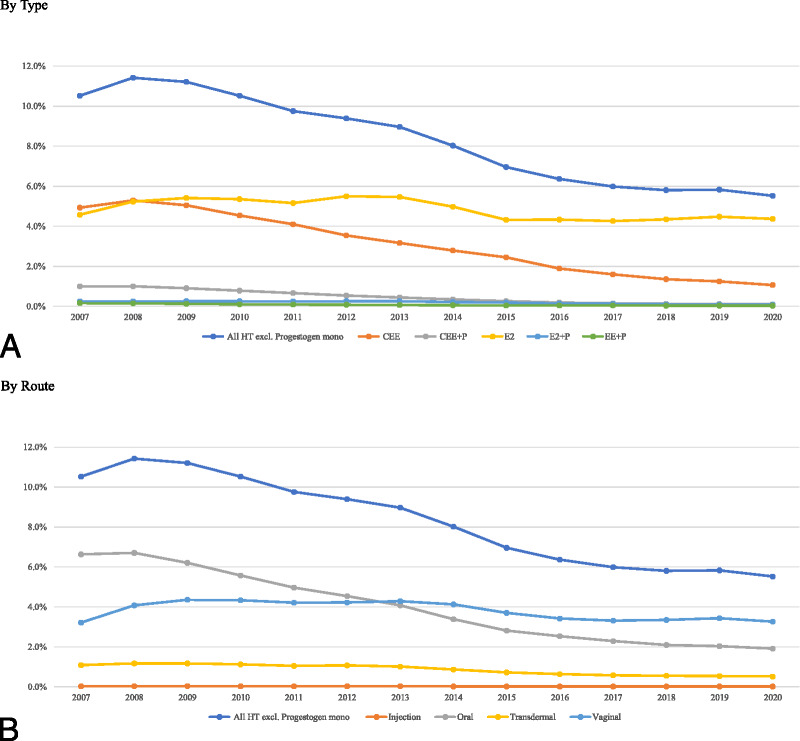
Trend in the use of hormone therapy (HT) by type and route. (A) By type. (B) By route.
Starting with Part D enrollment, the median follow-up in death cohort was 4.1 years (total of 51,813,776 person-years); it was longer among any HT users (5.7 years) than no HT users (4.0 years) (Table 1). Overall, 595,929 women died (5.4% or 11.5 per 1,000 person-years). The death incidence was lower among HT users than no HT users (6.3 vs 12.6 per 1,000 person-years) (Table 2). The number of women and follow-up duration varied somewhat across disease-specific cohorts because of different end points and censoring rates by outcomes.
Table 2.
Event/censoring points and rates of event/death by each study cohort
| End points | Rate per 1,000 PY | |||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | n | Event, n (%) | Death | MA entry | Disenrollment | 12/31/2020 | Event | Death |
| Death | ||||||||
| Any HT | 1,522,914 | N/A | 58,952 (3.9) | 44,670 (2.9) | 49,601 (3.3) | 1,369,691 (89.9) | N/A | 6.32 |
| No HT | 9,421,414 | N/A | 536,977 (5.7) | 327,489 (3.5) | 422,451 (4.5) | 8,134,497 (86.3) | N/A | 12.64 |
| Breast cancer | ||||||||
| Any HT | 1,479,715 | 56,894 (3.8) | 52,836 (3.6) | 43,427 (2.9) | 47,422 (3.2) | 1,279,136 (86.4) | 6.44 | 5.98 |
| No HT | 8,998,173 | 425,189 (4.7) | 455,477 (5.1) | 310,523 (3.5) | 396,275 (4.4) | 7,410,709 (82.4) | 10.87 | 11.65 |
| Lung cancer | ||||||||
| Any HT | 1,516,490 | 15,988 (1.1) | 49,973 (3.3) | 44,471 (2.9) | 49,272 (3.2) | 1,356,786 (89.5) | 1.73 | 5.4 |
| No HT | 9,375,994 | 127,880 (1.4) | 451,813 (4.8) | 325,721 (3.5) | 419,164 (4.5) | 8,051,416 (85.9) | 3.04 | 10.73 |
| Endometrial cancer | ||||||||
| Any HT | 1,514,965 | 13,641 (0.9) | 56,442 (3.7) | 44,444 (2.9) | 49,128 (3.2) | 1,351,310 (89.2) | 1.48 | 6.11 |
| No HT | 9,369,958 | 103,463 (1.1) | 511,688 (5.5) | 325,383 (3.5) | 418,096 (4.5) | 8,011,328 (85.5) | 2.46 | 12.19 |
| Colorectal cancer | ||||||||
| Any HT | 1,512,516 | 12,862 (0.9) | 55,738 (3.7) | 44,347 (2.9) | 49,052 (3.2) | 1,350,517 (89.3) | 1.39 | 6.04 |
| No HT | 9,364,136 | 103,439 (1.1) | 503,313 (5.4) | 324,535 (3.5) | 417,694 (4.5) | 8,015,155 (85.6) | 2.46 | 11.99 |
| Ovarian cancer | ||||||||
| Any HT | 1,517,113 | 8,984 (0.6) | 55,931 (3.7) | 44,460 (2.9) | 49,271 (3.2) | 1,358,467 (89.5) | 0.97 | 6.04 |
| No HT | 9,389,848 | 54,178 (0.6) | 510,350 (5.4) | 326,018 (3.5) | 420,059 (4.5) | 8,079,243 (86.0) | 1.28 | 12.09 |
| IHD | ||||||||
| Any HT | 1,340,868 | 233,040 (17.4) | 26,133 (1.9) | 36,347 (2.7) | 39,091 (2.9) | 1,006,257 (75.0) | 32.22 | 3.61 |
| No HT | 8,687,408 | 1,421,490 (16.4) | 251,496 (2.9) | 266,052 (3.1) | 347,347 (4.0) | 6,401,023 (73.7) | 40.9 | 7.24 |
| CHF | ||||||||
| Any HT | 1,466,865 | 110,976 (7.6) | 33,318 (2.3) | 41,880 (2.9) | 45,639 (3.1) | 1,235,052 (84.2) | 12.89 | 3.87 |
| No HT | 9,141,585 | 799,539 (8.7) | 293,609 (3.2) | 302,168 (3.3) | 387,965 (4.2) | 7,358,304 (80.5) | 20.38 | 7.49 |
| VTE | ||||||||
| Any HT | 1,481,007 | 83,297 (5.6) | 40,959 (2.8) | 42,760 (2.9) | 46,725 (3.2) | 1,267,266 (85.6) | 9.53 | 4.68 |
| No HT | 9,261,200 | 509,703 (5.5) | 381,443 (4.1) | 313,880 (3.4) | 401,838 (4.3) | 7,654,336 (82.6) | 12.63 | 9.45 |
| Stroke | ||||||||
| Any HT | 1,487,749 | 81,856 (5.5) | 44,340 (3.0) | 43,119 (2.9) | 46,737 (3.1) | 1,271,697 (85.5) | 9.27 | 5.02 |
| No HT | 9,283,342 | 510,330 (5.5) | 411,426 (4.4) | 314,944 (3.4) | 400,471 (4.3) | 7,646,171 (82.4) | 12.58 | 10.14 |
| AF | ||||||||
| Any HT | 1,478,512 | 74,617 (5.0) | 45,393 (3.1) | 43,411 (2.9) | 47,260 (3.2) | 1,267,831 (85.8) | 8.47 | 5.15 |
| No HT | 9,227,222 | 479,738 (5.2) | 415,247 (4.5) | 317,504 (3.4) | 404,976 (4.4) | 7,609,757 (82.5) | 11.87 | 10.28 |
| AMI | ||||||||
| Any HT | 1,515,118 | 23,261 (1.5) | 53,245 (3.5) | 44,375 (2.9) | 49,054 (3.2) | 1,345,183 (88.8) | 2.52 | 5.78 |
| No HT | 9,383,235 | 191,992 (2.0) | 476,113 (5.1) | 324,540 (3.5) | 416,234 (4.4) | 7,974,356 (85.0) | 4.58 | 11.36 |
| Dementia | ||||||||
| Any HT | 1,500,513 | 72,369 (4.8) | 41,445 (2.8) | 43,586 (2.9) | 46,968 (3.1) | 1,296,145 (86.4) | 8.05 | 4.61 |
| No HT | 9,333,629 | 410,046 (4.4) | 399,835 (4.3) | 318,965 (3.4) | 404,698 (4.3) | 7,800,085 (83.6) | 9.94 | 9.7 |
AF, atrial fibrillation; AMI, acute myocardial infarction; HF, heart failure; HT, hormone therapy; IHD, ischemic heart disease; MA, Medicare Advantage; PY, person-year; VTE, venous thromboembolism.
Medicaid eligibility for special supplements was our proxy for income level. Accordingly, there were three income groups: dual (15.2%) with incomes below 135% of the Federal Poverty Line (FPL); nondual LIS (2.4%) between 135% and 150% FPL; and nondual no LIS (82.4%) above 150% FPL.20 The proportions of non-Hispanic White and rural resident were 77.7% and 24.0%, respectively. Among the chronic conditions, hyperlipidemia (72.3%), hypertension (67.4%), and cataracts (54.3%) were most common. HT users were more likely to be White (86.6% vs 76.6%), nondual no LIS enrollees (thus wealthier, 89.5% vs 81.2%), from rural areas (24.7% vs 23.9%), and have hyperlipidemia (77.6% vs 71.4%), hypertension (67.6% vs 67.4%), cataracts (67.9% vs 52.1%), and more (Table 1). Because we had no claims data about hysterectomies performed before age 65 years, hysterectomy data were only available for 12.8% of women in the study, and most of it came from the ICD diagnosis codes for “acquired absence of uterus/cervix” (Supplemental Digital Content 4, http://links.lww.com/MENO/B236).
Primary analyses
In Tables 3 and 4, we present the marginal risks of 13 study outcomes associated with the use of each HT after controlling for all time-varying and time-fixed covariates including the use of any other HT beyond the index HT, namely, adjusted hazards ratio (aHR). We report aHR as the percent of risk above (increased) or below (decreased) one by an amount of 100 × (aHR − 1)%. We present marginal aHR to highlight average differences by type, route, and dose level. We also present aHR for each of 40 combinations of type, route, and dose level in Supplemental Digital Contents 5 and 6, http://links.lww.com/MENO/B236, where oral medium dose CEE and CEE+ progestin indicate comparable drugs studied in the WHI trials.
Table 3.
Marginal effects of HT regimens on all-cause mortality and cancer outcomes
| Marginal HT | (a) Death | (b) Breast | (c) Lung | (d) Endometrial | (e) Colorectal | (f) Ovarian |
|---|---|---|---|---|---|---|
| Estrogen without progestogen | 0.81 (0.79-0.82)↡ | 0.84 (0.83-0.86)↡ | 0.87 (0.84-0.90)↡ | 0.73 (0.70-0.76)↡ | 0.88 (0.84-0.91)↡ | 0.87 (0.83-0.91)↡ |
| By type | ||||||
| CEE | 0.87 (0.85-0.88)↡ | 0.77 (0.75-0.78)↡ | 0.90 (0.87-0.93)↡ | 0.69 (0.66-0.73)↡ | 0.89 (0.86-0.93)↡ | 0.82 (0.78-0.87)↡ |
| E2 | 0.79 (0.77-0.81)↡ | 0.88 (0.86-0.90)↡ | 0.86 (0.82-0.90)↡ | 0.75 (0.71-0.79)↡ | 0.87 (0.83-0.91)↡ | 0.89 (0.83-0.95)↡ |
| By route | ||||||
| Oral | 0.89 (0.88-0.90)↡ | 0.77 (0.76-0.78)↡ | 0.91 (0.89-0.94)↡ | 0.62 (0.59-0.65)↡ | 0.87 (0.84-0.90)↡ | 0.81 (0.77-0.84)↡ |
| Transdermal | 0.80 (0.77-0.82)↡ | 0.86 (0.84-0.88)↡ | 0.86 (0.82-0.91)↡ | 0.78 (0.73-0.83)↡ | 0.87 (0.82-0.92)↡ | 0.87 (0.81-0.94)↡ |
| Vaginal | 0.70 (0.67-0.74)↡ | 0.95 (0.92-0.99)↓ | 0.79 (0.72-0.86)↡ | 0.89 (0.82-0.98)↓ | 0.84 (0.76-0.92)↡ | 1.02 (0.93-1.12) |
| Injection | 0.85 (0.76-0.94)↓ | 0.85 (0.73-0.99)↓ | 0.97 (0.79-1.18) | 0.71 (0.51-1.00) | 1.11 (0.85-1.44) | 0.69 (0.44-1.07) |
| By dose | ||||||
| Low | 0.80 (0.78-0.82)↡ | 0.88 (0.86-0.90)↡ | 0.85 (0.81-0.88)↡ | 0.77 (0.74-0.81)↡ | 0.85 (0.82-0.89)↡ | 0.87 (0.82-0.91)↡ |
| Medium | 0.77 (0.74-0.81)↡ | 0.85 (0.83-0.88)↡ | 0.84 (0.78-0.91)↡ | 0.75 (0.70-0.81)↡ | 0.86 (0.79-0.93)↡ | 0.92 (0.85-0.99)↓ |
| High | 0.85 (0.83-0.88)↡ | 0.81 (0.78-0.84)↡ | 0.92 (0.87-0.96)↓ | 0.68 (0.62-0.74)↡ | 0.91 (0.85-0.98)↓ | 0.82 (0.74-0.91)↡ |
| Progestin without estrogen | 1.11 (1.07-1.16)↟ | 1.21 (1.16-1.26)↟ | 0.95 (0.87-1.03) | 5.07 (4.82-5.34)↟ | 1.15 (1.05-1.26)↑ | 2.27 (2.08-2.48)↟ |
| Estrogen + progestin | 0.97 (0.92-1.02) | 1.10 (1.06-1.15)↟ | 1.02 (0.93-1.11) | 0.55 (0.50-0.60)↡ | 0.93 (0.84-1.03) | 0.79 (0.71-0.89)↡ |
| By type | ||||||
| CEE | 1.03 (0.97-1.09) | 1.12 (1.06-1.19)↟ | 0.91 (0.79-1.05) | 0.65 (0.58-0.72)↡ | 0.81 (0.69-0.96)↓ | 0.89 (0.76-1.04) |
| E2 | 0.98 (0.91-1.06) | 1.09 (1.03-1.16)↑ | 1.07 (0.94-1.23) | 0.52 (0.46-0.60)↡ | 0.99 (0.85-1.15) | 0.73 (0.61-0.87)↡ |
| EE | 0.83 (0.76-0.90)↡ | 1.13 (1.06-1.20)↟ | 0.96 (0.83-1.11) | 0.52 (0.41-0.66)↡ | 0.91 (0.76-1.08) | 0.94 (0.77-1.14) |
| By route | ||||||
| Oral | 0.90 (0.86-0.93)↡ | 1.15 (1.11-1.19)↟ | 0.96 (0.89-1.03) | 0.50 (0.46-0.56)↡ | 0.91 (0.84-0.99)↓ | 0.78 (0.68-0.89)↡ |
| Transdermal | 0.88 (0.75-1.04) | 1.09 (0.96-1.23) | 1.07 (0.80-1.42) | 0.54 (0.42-0.70)↡ | 0.99 (0.73-1.35) | 1.01 (0.76-1.34) |
| Vaginal | 1.26 (1.12-1.41)↟ | 1.02 (0.92-1.12) | 1.10 (0.88-1.37) | 0.68 (0.57-0.82)↡ | 0.92 (0.71-1.19) | 0.65 (0.49-0.86)↓ |
| By dose | ||||||
| Low | 0.96 (0.88-1.04) | 1.00 (0.94-1.07) | 1.06 (0.91-1.22) | 0.51 (0.44-0.59)↡ | 0.88 (0.74-1.05) | 0.83 (0.69-0.99)↓ |
| Medium | 0.93 (0.88-0.97)↓ | 1.16 (1.11-1.20)↟ | 0.92 (0.84-1.02) | 0.57 (0.52-0.63)↡ | 0.90 (0.80-1.01) | 0.87 (0.77-0.98)↓ |
| High | 1.06 (0.91-1.23) | 1.20 (1.06-1.36)↑ | 1.12 (0.85-1.48) | 0.59 (0.45-0.76)↡ | 1.09 (0.80-1.48) | 0.64 (0.44-0.93)↓ |
| Progesterone without estrogen | 0.78 (0.73-0.82)↡ | 0.90 (0.86-0.94)↡ | 0.81 (0.73-0.90)↡ | 1.38 (1.28-1.50)↟ | 0.90 (0.81-1.00) | 1.23 (1.10-1.37)↟ |
| Estrogen + progesterone | 0.98 (0.93-1.03) | 1.19 (1.14-1.24)↟ | 1.05 (0.96-1.16) | 1.33 (1.23-1.44)↟ | 0.97 (0.87-1.08) | 1.19 (1.08-1.31)↟ |
| By type | ||||||
| CEE | 0.92 (0.81-1.05) | 1.23 (1.11-1.35)↟ | 1.25 (1.02-1.52)↑ | 1.62 (1.37-1.91)↟ | 1.09 (0.86-1.38) | 1.28 (1.02-1.59)↑ |
| E2 | 1.00 (0.95-1.06) | 1.17 (1.12-1.23)↟ | 0.99 (0.89-1.10) | 1.24 (1.14-1.35)↟ | 0.93 (0.83-1.05) | 1.16 (1.04-1.29)↑ |
| By route | ||||||
| Oral | 0.87 (0.80-0.95)↓ | 1.24 (1.16-1.33)↟ | 1.12 (0.97-1.29) | 1.64 (1.46-1.85)↟ | 0.98 (0.83-1.17) | 1.32 (1.13-1.55)↟ |
| Transdermal | 1.01 (0.92-1.11) | 1.16 (1.08-1.23)↟ | 0.79 (0.66-0.95)↓ | 1.22 (1.07-1.39)↑ | 0.90 (0.75-1.08) | 1.11 (0.94-1.31) |
| Vaginal | 1.14 (1.02-1.28)↑ | 1.13 (1.04-1.23)↑ | 1.27 (1.06-1.52)↑ | 1.03 (0.88-1.20) | 1.03 (0.83-1.27) | 1.07 (0.89-1.29) |
| By dose | ||||||
| Low | 0.96 (0.87-1.06) | 1.17 (1.10-1.25)↟ | 1.07 (0.91-1.25) | 1.39 (1.23-1.58)↟ | 0.90 (0.75-1.08) | 1.27 (1.09-1.48)↑ |
| Medium | 1.01 (0.93-1.11) | 1.19 (1.11-1.28)↟ | 1.10 (0.95-1.28) | 1.44 (1.28-1.62)↟ | 1.07 (0.91-1.27) | 1.18 (1.00-1.40)↑ |
| High | 0.96 (0.85-1.08) | 1.21 (1.10-1.32)↟ | 0.97 (0.78-1.21) | 1.14 (0.95-1.36) | 0.95 (0.74-1.20) | 1.10 (0.88-1.37) |
Notes: Data are presented as adjusted hazards ratio (aHR) and its 95% CI.
↡ = very significantly low with P value < 0.001, ↓ = significantly low with 0.001 ≤ P value < 0.05.
↟ = very significantly high with P value < 0.001, ↑ = significantly high with 0.001 ≤ P value < 0.05.
Table 4.
Marginal effects of HT regimens on CV outcomes and dementia
| Marginal HT | (a) IHD | (b) CHF | (c) VTE | (d) Stroke | (e) AF | (f) AMI | (g) Dementia |
|---|---|---|---|---|---|---|---|
| Estrogen without progestogen | 1.04 (1.03-1.05)↟ | 0.95 (0.94-0.96)↡ | 0.97 (0.96-0.98)↡ | 1.01 (0.99-1.02) | 0.96 (0.95-0.98)↡ | 0.89 (0.87-0.92)↡ | 0.98 (0.97-1.00)↓ |
| By type | |||||||
| CEE | 1.04 (1.03-1.05)↟ | 0.99 (0.98-1.01) | 0.98 (0.97-1.00)↓ | 1.05 (1.04-1.07)↟ | 1.00 (0.98-1.01) | 0.94 (0.91-0.96)↡ | 1.01 (1.00-1.03) |
| E2 | 1.03 (1.02-1.05)↟ | 0.94 (0.92-0.95)↡ | 0.97 (0.95-0.99)↡ | 0.99 (0.97-1.01) | 0.95 (0.93-0.97)↡ | 0.88 (0.85-0.91)↡ | 0.97 (0.95-0.99)↓ |
| By route | |||||||
| Oral | 1.04 (1.03-1.04)↟ | 1.01 (1.00-1.02) | 0.98 (0.97-1.00)↓ | 1.06 (1.05-1.07)↟ | 1.00 (0.99-1.02) | 0.93 (0.91-0.95)↡ | 1.02 (1.01-1.03)↑ |
| Transdermal | 1.01 (1.00-1.03) | 0.90 (0.88-0.91)↡ | 0.94 (0.92-0.97)↡ | 0.95 (0.93-0.97)↡ | 0.93 (0.90-0.95)↡ | 0.86 (0.82-0.90)↡ | 0.92 (0.89-0.94)↡ |
| Vaginal | 1.03 (1.00-1.05)↑ | 0.87 (0.84-0.90)↡ | 0.96 (0.93-0.99)↓ | 0.96 (0.93-0.99)↓ | 0.93 (0.90-0.97)↡ | 0.83 (0.77-0.89)↡ | 0.95 (0.92-0.99)↓ |
| Injection | 1.17 (1.10-1.25)↟ | 1.17 (1.07-1.27)↟ | 1.02 (0.91-1.13) | 1.06 (0.96-1.18) | 0.94 (0.84-1.05) | 1.05 (0.89-1.25) | 1.08 (0.97-1.19) |
| By dose | |||||||
| Low | 0.99 (0.98-1.00)↓ | 0.87 (0.86-0.88)↡ | 0.93 (0.92-0.95)↡ | 0.94 (0.92-0.95)↡ | 0.94 (0.92-0.95)↡ | 0.82 (0.79-0.85)↡ | 0.92 (0.90-0.94)↡ |
| Medium | 1.02 (1.01-1.04)↑ | 0.93 (0.90-0.95)↡ | 0.96 (0.94-0.99)↓ | 0.99 (0.96-1.02) | 0.96 (0.93-0.99)↓ | 0.89 (0.84-0.95)↡ | 0.98 (0.95-1.02) |
| High | 1.09 (1.08-1.11)↟ | 1.05 (1.03-1.07)↟ | 1.01 (0.98-1.04) | 1.08 (1.05-1.11)↟ | 0.99 (0.96-1.01) | 0.96 (0.92-1.00) | 1.03 (1.00-1.06)↑ |
| Progestin without estrogen | 1.00 (0.98-1.02) | 1.08 (1.05-1.11)↟ | 1.12 (1.08-1.16)↟ | 0.97 (0.94-1.01) | 1.08 (1.04-1.13)↟ | 1.00 (0.93-1.07) | 1.00 (0.96-1.04) |
| Estrogen + progestin | 0.95 (0.93-0.97)↡ | 0.95 (0.91-0.98)↓ | 0.95 (0.91-0.99)↓ | 0.98 (0.94-1.02) | 0.98 (0.94-1.02) | 0.97 (0.89-1.05) | 1.03 (0.98-1.07) |
| By type | |||||||
| CEE | 0.98 (0.95-1.01) | 0.96 (0.91-1.01) | 0.94 (0.89-0.99)↓ | 0.91 (0.86-0.97)↓ | 0.93 (0.87-0.98)↓ | 0.92 (0.83-1.03) | 1.00 (0.94-1.06) |
| E2 | 0.94 (0.90-0.97)↓ | 0.96 (0.91-1.01) | 0.94 (0.89-1.00) | 1.02 (0.96-1.08) | 1.00 (0.94-1.06) | 1.03 (0.91-1.16) | 1.03 (0.97-1.10) |
| EE | 0.96 (0.92-1.00) | 0.88 (0.83-0.94)↡ | 0.98 (0.92-1.05) | 0.92 (0.86-0.99)↓ | 0.96 (0.90-1.04) | 0.81 (0.70-0.94)↓ | 1.04 (0.97-1.12) |
| By route | |||||||
| Oral | 0.96 (0.94-0.98)↡ | 0.91 (0.88-0.93)↡ | 0.95 (0.92-0.98)↓ | 0.94 (0.90-0.97)↡ | 0.93 (0.90-0.96)↡ | 0.89 (0.83-0.95)↓ | 1.07 (1.03-1.10)↟ |
| Transdermal | 0.90 (0.83-0.97)↓ | 0.97 (0.86-1.09) | 0.94 (0.83-1.07) | 1.15 (1.02-1.29)↑ | 1.04 (0.92-1.18) | 1.13 (0.88-1.44) | 1.00 (0.87-1.14) |
| Vaginal | 0.99 (0.93-1.05) | 1.02 (0.94-1.12) | 0.96 (0.87-1.05) | 0.91 (0.82-1.02) | 1.03 (0.93-1.14) | 1.01 (0.82-1.24) | 0.96 (0.87-1.07) |
| By dose | |||||||
| Low | 0.93 (0.89-0.97)↡ | 0.96 (0.90-1.02) | 0.95 (0.89-1.02) | 0.96 (0.90-1.04) | 0.97 (0.90-1.04) | 0.95 (0.82-1.09) | 0.92 (0.85-0.99)↓ |
| Medium | 0.98 (0.96-1.01) | 0.93 (0.90-0.97)↡ | 0.95 (0.92-0.99)↓ | 0.93 (0.89-0.97)↓ | 0.93 (0.89-0.97)↓ | 0.96 (0.88-1.04) | 1.05 (1.01-1.10)↑ |
| High | 0.93 (0.86-1.01) | 0.95 (0.85-1.07) | 0.93 (0.82-1.06) | 1.07 (0.95-1.21) | 1.07 (0.94-1.22) | 1.02 (0.80-1.31) | 1.19 (1.05-1.35)↑ |
| Progesterone without estrogen | 1.08 (1.06-1.11)↟ | 0.94 (0.90-0.97)↓ | 0.94 (0.90-0.98)↓ | 1.01 (0.97-1.05) | 0.98 (0.94-1.03) | 0.79 (0.72-0.86)↡ | 0.95 (0.91-1.00) |
| Estrogen + progesterone | 0.98 (0.96-1.01) | 0.96 (0.92-1.00)↓ | 1.02 (0.98-1.06) | 0.97 (0.93-1.01) | 0.98 (0.94-1.03) | 0.96 (0.88-1.05) | 1.01 (0.97-1.06) |
| By type | |||||||
| CEE | 0.98 (0.93-1.03) | 0.91 (0.83-1.00)↓ | 1.02 (0.93-1.12) | 0.91 (0.82-1.00) | 0.96 (0.86-1.06) | 0.98 (0.80-1.21) | 1.07 (0.97-1.18) |
| E2 | 0.99 (0.96-1.01) | 0.98 (0.94-1.02) | 1.02 (0.98-1.06) | 0.99 (0.95-1.03) | 0.99 (0.95-1.04) | 0.95 (0.87-1.05) | 0.99 (0.95-1.04) |
| By route | |||||||
| Oral | 0.97 (0.93-1.01) | 0.90 (0.84-0.95)↓ | 1.01 (0.94-1.08) | 0.95 (0.89-1.01) | 0.92 (0.86-0.99)↓ | 0.95 (0.82-1.09) | 1.01 (0.94-1.08) |
| Transdermal | 1.00 (0.96-1.03) | 1.01 (0.95-1.07) | 1.02 (0.96-1.09) | 0.95 (0.89-1.02) | 1.01 (0.94-1.08) | 0.88 (0.75-1.02) | 0.98 (0.91-1.05) |
| Vaginal | 1.00 (0.96-1.05) | 1.03 (0.96-1.11) | 1.04 (0.96-1.12) | 1.02 (0.94-1.11) | 1.06 (0.98-1.15) | 1.09 (0.91-1.30) | 1.06 (0.98-1.15) |
| By dose | |||||||
| Low | 0.98 (0.94-1.02) | 0.94 (0.88-1.01) | 0.95 (0.89-1.02) | 0.97 (0.90-1.04) | 0.98 (0.91-1.05) | 0.99 (0.85-1.16) | 0.99 (0.92-1.06) |
| Medium | 0.97 (0.94-1.01) | 0.95 (0.90-1.02) | 1.06 (0.99-1.13) | 0.91 (0.85-0.98)↓ | 0.97 (0.90-1.04) | 0.91 (0.78-1.05) | 1.07 (1.00-1.14) |
| High | 1.00 (0.95-1.05) | 0.99 (0.92-1.08) | 1.06 (0.97-1.15) | 1.05 (0.97-1.14) | 1.01 (0.92-1.11) | 1.00 (0.82-1.21) | 0.98 (0.89-1.08) |
Notes: Data are presented as adjusted hazards ratio (aHR) and its 95% CI.
AF, atrial fibrillation; AMI, acute myocardial infarction; HF, heart failure; IHD, ischemic heart diseases; VTE, venous thromboembolism.
↡ = very significantly low with P value < 0.001, ↓ = significantly low with 0.001 ≤ P value < 0.05.
↟ = very significantly high with P value < 0.001, ↑ = significantly high with 0.001 ≤ P value < 0.05.
The risk of all-cause mortality associated with HT
On average, ET use beyond age 65 years was associated with a significant 19% reduction in mortality risk relative to no ET use (Table 3A), which translated to 113,226 fewer expected deaths in our large population. All combinations of ET type, route, and dose were also associated with reduced mortality risk. The marginal mortality risk reduction of E2 was significantly greater than that of CEE (21% vs 13%). Vaginal, transdermal, and oral ET was associated with 30%, 20%, and 11% reduction of mortality risk, respectively. The mortality risks associated with low and medium dose ET were significantly less than high dose but were not different from each other. Overall, EPT, regardless type of progestogen, had no significant association with mortality. Oral, medium dose, or EE preparations of E+ progestin exhibited 7%-17% reduction in mortality risk. Progesterone monotherapy was associated with a 22% reduced mortality risk, whereas progestin monotherapy was associated an 11% increased risk. Interestingly, oral CEE medium dose, a preparation comparable in strength to the dose studied in the WHI trial, exhibited a 9% reduction in mortality, a smaller reduction than that of overall ET in our analysis (Supplemental Digital Content 5A, http://links.lww.com/MENO/B236), although the WHI trial of ET reported an insignificant 4% mortality risk reduction. Both WHI trial dose of EPT and the comparable oral medium dose of CEE+ progestin in our analysis showed no significant association.
The risk of breast, lung, endometrial, colorectal, and ovarian cancers associated with HT
During our study period, breast cancer incidence was at least three times that of any other study cancer (Table 2). ET use beyond age 65 years was associated with a significant reduction in marginal risk of breast cancer, 16% overall, as well as each combination of ET type, route, and dose size (Table 3B). Oral ET exhibited significantly greater risk reductions than transdermal and vaginal ET. Furthermore, CEE was associated with a greater (23%) reduction of breast cancer risk than E2 (12%). The WHI's 13-year postintervention study reported a significant 21% risk reduction of breast cancer risk associated with oral CEE 0.625 mg.5 Approximately 70% of the oral CEE medium doses in our study were 0.625 mg, and its use was associated with a significant 26% risk reduction of breast cancer. To the negative, both estrogen+progestin and estrogen+progesterone were associated with significant increase in the risk of breast cancer by 19% and 10%, respectively. Such increased risk, however, was not observed in low-dose vaginal and transdermal E2+ progestin. Progesterone, when used alone, was associated with a 10% reduction in breast cancer risk, but progestin increased the risk by 21% (Table 3B and Supplemental Digital Content 5B, http://links.lww.com/MENO/B236).
Overall, ET was associated with a 13% and 12% reduction in lung and colorectal cancer risk, respectively. Both estrogen+progestin and estrogen+progesterone exhibited null risks marginally for these two cancers. Of 24 different preparations of EPT, oral medium dose E2+ progestin exhibited significant 16% risk reduction for lung cancer, and oral low-dose CEE/E2+ progestin exhibited 17%-20% risk reduction for colorectal cancer. Among two progestogen monotherapies, progesterone was associated with a 19% reduced lung cancer risk, in contrast, progestin was associate with a 14% risk of this cancer (Table 3C and E and Supplemental Digital Content 5C and E, http://links.lww.com/MENO/B236).
More than half of hysterectomized women likely also had bilateral oophorectomy.21 So, observed reduction in endometrial and ovarian cancer from ET use might be an artifact of the selective use of ET in hysterectomized women who lack the organs where such cancers could arise. On the other hand, risk of endometrial cancer associated with EPT use is probably meaningful because it is usually prescribed for women with an intact uterus. Only with E+ progestin use, endometrial cancer risk declined significantly by 45%, whereas E+ progesterone exhibited a significant 33% increase in such risk (Table 3D and F).
The risk of IHD, HF, VTE, stroke, AF, AMI, and dementia, associated with HT
IHD occurred in more than 1.6 million women in the study, almost twice that of the next most frequent CV condition, HF. Therefore, a 4% increase in the risk of IHD associated with ET could potentially lead to an additional 64,000 cases of IHD. Most types, routes, and dose levels of ET were also associated with increased risk of IHD, up to 17% with injectables, but much less (3%-4%) with other types, routes, and doses. Importantly, the use of low dose oral CEE/E2 was associated with a significant, but very small, 1%-2% risk reduction for IHD. Progestin monotherapy exhibited no risk for IHD, whereas progesterone monotherapy was associated with an increased risk (8%) for IHD. Likewise, E+ progestin, overall, was associated with a significant 5% risk reduction of IHD, whereas E+ progesterone had no association with IHD (Table 4A and Supplemental Digital Content 6A, http://links.lww.com/MENO/B236).
To the positive, ET use, overall, was associated with 5% risk reduction of HF, but high dose and injectable ET increased its risk by 5%-17%. Marginally, both EPT formulations were associated with 4%-5% reduced HF risk, but such reductions were concentrated on E+ progestin (Table 4B and Supplemental Digital Content 6B, http://links.lww.com/MENO/B236).
ET use, overall, had no association or small reductions in risk of stroke and dementia. Transdermal and vaginal ET preparations exhibited small (<10%) but significant risk reductions for these two conditions, whereas high-dose ET increased the risks of both conditions, by 8% and 3%, respectively. EPT use, on average, had no such associations. Low doses of oral CEE/E2+ progestin and E2+ progesterone were associated with 6%-10% and 10% decreased risks of stroke and dementia, respectively. In addition, low dose of oral CEE+ progestin exhibited 5%-13% decreased risks of all six CV conditions (Table 4D and G and Supplemental Digital Content 6D and G, http://links.lww.com/MENO/B236).
DISCUSSION
For decades, menopausal HT after age 65 years was considered to be unnecessary because symptoms due to estrogen withdrawal rarely persisted beyond age 65. However, a growing body of evidence suggests that some vasomotor symptoms do persist in many elderly women,7 and thus HT can benefit them. Recognizing this reality, in 2022, The Menopause Society changed their position about use of HT in women aged 65 years and older,8 suggesting that the decision to start or continue HT beyond age 65 years should be individualized (ie, based on the individual's specific needs, overall health, and medical history) and highlighted the use of lower doses and nonoral preparation to minimize risks of adverse effects. In this study, we explored the initiation/continuation of menopausal HT beyond age 65 years and effects of 40 different HT preparations on 13 health outcomes. We found important variations across different types, routes, and strengths of HT.
Compared with never use or discontinuation of HT after 65 years, ET use beyond age 65, overall, was associated with significant reductions in mortality risk. It was also associated with reduced risks of three cancers (breast, lung, and colorectal), four CV conditions (congestive heart failure [CHF], VTE, AF, and AMI), and dementia. Generally, risk reduction was greater for E2 (vs CEE), vaginal and transdermal (vs oral), and low or medium (vs high dose). For EPT use, E+ progestin marginally exhibited risk reductions in endometrial and ovarian cancers, IHD, CHF, and VTE, whereas E+ progesterone exhibited risk reduction only in CHF.
Association with all-cause mortality
Oral CEE 0.625 mg, the sole preparation studied in the WHI trials, exhibited a close to significant 6% mortality reduction in the 18-year cumulative follow-up of the WHI trials,22 which gives plausibility to the 9% mortality reduction we observed with use of medium dose oral CEE. The 19% mortality reduction we observed with ET overall is consistent with the results from a meta-analysis of 31 observational and RCT studies that reported reduced mortality among HT users23 and with the reanalyses of the Prostate, Lung, Colorectal, and Ovarian Cancer Screening RTC, which reported a 23% decrease in all-cause mortality among current users of any HT. Medium (or 0.625 mg) dose of oral CEE+ progestin exhibited no mortality risk reduction in both our study and the 18-year cumulative follow-up of the WHI trials.22 However, our study found significant mortality reduction associated with different EPT preparations: low dose of oral CEE+ progestin, CEE+ progesterone, E2+ progestin, and medium dose of oral and transdermal E2+ progestin, confirming The Menopause Society's 2022 position statement advice on mitigation of risk through use of the low dose, nonoral route of administration, and different types of estrogen and progestogen.8
Associations with cancers
Overall ET and medium dose of oral CEE, in our study, were associated with 16% and 26% reductions of breast cancer risk, respectively. Overall EPT and medium dose oral CEE+ progestin were associated with the opposite—a 10%-19% increase in breast cancer risk. The WHI postintervention study reported a significant, and similarly sized, 21% decreased risk of breast cancer with CEE alone and a 28% increase with CEE + medroxyprogesterone,5 giving credence to our results. Importantly, our study found an insignificant but numerically reduced risk of breast cancer associated with two EPT (low dose of transdermal and vaginal E2+ progestin). On average, ET use was also associated with significant 13% and 12% risk reductions for lung and colorectal cancers, but EPT had no association with these two cancers. In contrast, the WHI postintervention study only reported insignificant associations for lung and colorectal cancers. However, our results were based on at least 100,000 cases of each cancer, 1,000 times more cases than that of the WHI postintervention study, providing much greater statistical power to see associations. A few observational studies support our findings of reduced lung cancer risk in association with HT use.24,25 Two observational studies26,27 and a reanalysis of the Prostate, Lung, Colorectal, and Ovarian trial data28 support our protective associations between HT use and colorectal cancer. The greater incidence of colorectal (79%)29 and lung cancer (26%)30 among women with lower levels of estrogen due to oophorectomy as part of their hysterectomy compared with hysterectomized women without ovary removal also supports our results of ET use by implying that estrogen protects against these two cancers.
Associations with CV diseases and dementia
Similar to the results of oral CEE 0.625 mg in the WHI postintervention study,5 our medium dose of oral CEE exhibited no risk reductions in either six CV conditions or dementia. Our results also suggest significant risk increases for IHD and stroke associated with medium dose of oral CEE. However, low-dose ET was associated with significant risk reductions for all CV conditions and dementia. Transdermal and vaginal ET which should avoid the procoagulant and proinflammatory effects ascribed to liver passage31,32 exhibited reduced risk of both dementia and stroke, in accord with the results of other studies.33
When used alone, progesterone was associated with significantly decreased risks of three CV conditions (CHF, VTE, and AMI), whereas progestin exhibited no risk reductions at all. However, when combined with estrogen, E+ progestin did exhibit significant risk reductions in IHD, CHF, and VTE, whereas E+ progesterone exhibited risk reduction for CHF alone.
Strengths and limitation
Our data availability only began at age 65 years, and information on hysterectomy and other health conditions before Medicare year was unavailable, and thus we did not have a way to correct for them. We depended on claims for encounter diagnoses and could not validate them through chart review. As is true for all observational studies, differential influences of unmeasured confounders, such as adherence to healthy behavior among HT users, could have been present.
One strength was the use of filled prescription records, rather than recall, to ascertain HT use. Another strength was its sample size (>10 million) including almost all menopausal women aged ≥65 years and the incidence of each outcome (up to 1.6 million)—nearly an order of magnitude greater than any previous HT study.34 Its massive sample size and incidence enabled us to estimate differential effects of 40 different HT type, route, and dose combinations on study outcomes.
CONCLUSIONS
Our study suggests the possibility of important health benefits with use of menopausal HT beyond age 65 years. The use of ET, mostly prescribed to women without intact uterus, can protect against risks of all-cause mortality, developing cancers (breast, lung, and colorectal), CHF, VTE, AF, AMI, and dementia. The implications of EPT for women who still have their uterus are less clear. The use of EPT does not increase risks for almost all conditions but does increase the risk of breast cancer. However, low dose of transdermal and vaginal EPT (especially E+ progestin) can mitigate the risk of breast cancer. In general, risk reductions appear to be greater with low rather than medium or high doses, vaginal or transdermal rather than oral preparations, and with E2 rather than CEE as emphasized by others.35
Our follow-up began when women entered Medicare at about age 65 years, but it is likely that many of them started taking HT closer to the time of their menopausal symptoms and continued it into their Medicare years. If so, our positive results align with the timing hypotheses36 that asserts that HT use early in menopauses is better than later, but extend it by reporting positive effects with usage continued into Medicare years. Our findings offer important insights into the variations among different menopausal hormone therapies, which could assist in tailoring postmenopausal HT on an individual basis.
Footnotes
Funding/support: This research was supported by the Intramural Research Program of the National Library of Medicine, National Institutes of Health.
Financial disclosures/conflicts of interest: None reported.
Disclaimers: Three previous editions of the paper have been published on two preprint servers, Authorea (https://doi.org/10.22541/au.167895234.48153899/v1, https://doi.org/10.22541/au.161873076.60547427/v1) and MedRxiv (https://doi.org/10.1101/2022.05.25.22275595). Previous editions included different number of women and/or different number of distinct hormone therapy preparations.
Supplemental digital content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article on the journal’s Website (www.menopause.org).
Contributor Information
Fitsum Baye, Email: fitsum.baye@nih.gov.
Clement J. McDonald, Email: clemmcdonald@mail.nih.gov.
REFERENCES
- 1.Rossouw JE Anderson GL Prentice RL, et al.; Writing Group for the Women's Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA J Am Med Assoc 2002;288:321–333. doi: 10.1001/jama.288.3.321 [DOI] [PubMed] [Google Scholar]
- 2.Brown S. Shock, terror and controversy: how the media reacted to the Women's Health Initiative. Climacteric 2012;15:275–80. doi: 10.3109/13697137.2012.660048 [DOI] [PubMed] [Google Scholar]
- 3.Langer RD. The evidence base for HRT: what can we believe? Climacteric 2017;20:91–96. doi: 10.1080/13697137.2017.1280251 [DOI] [PubMed] [Google Scholar]
- 4.Anderson GL Limacher M Assaf AR, et al.; Women's Health Initiative Steering Committee. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA 2004;291:1701–1712. doi: 10.1001/jama.291.14.1701 [DOI] [PubMed] [Google Scholar]
- 5.Manson JE Chlebowski RT Stefanick ML, et al. Menopausal hormone therapy and health outcomes during the intervention and extended poststopping phases of the Women's Health Initiative randomized trials. JAMA 2013;310:1353–1368. doi: 10.1001/jama.2013.278040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Avis NE Crawford SL Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med 2015;175:531–539. doi: 10.1001/jamainternmed.2014.8063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gartoulla P, Worsley R, Bell RJ, Davis SR. Moderate to severe vasomotor and sexual symptoms remain problematic for women aged 60 to 65 years. Menopause 2015;22:694–6701. doi: 10.1097/GME.0000000000000383 [DOI] [PubMed] [Google Scholar]
- 8.The 2022 Hormone Therapy Position Statement of The North American Menopause Society” Advisory Panel . The 2022 hormone therapy position statement of The North American Menopause Society. Menopause 2022;29:767–794. doi: 10.1097/GME.0000000000002028 [DOI] [PubMed] [Google Scholar]
- 9.The Centers for Medicare & Medicaid Services . CMS Announces New Data Sharing Tool | CMS [Internet]. 2013. Available at: https://www.cms.gov/newsroom/press-releases/cms-announces-new-data-sharing-tool. Accessed January 11, 2019.
- 10.Shreibati JB, Manson JAE, Margolis KL, Chlebowski RT, Stefanick ML, Hlatky MA. Impact of hormone therapy on Medicare spending in the Women's Health Initiative randomized clinical trials. Am Heart J 2018;198:108–114. doi: 10.1016/j.ahj.2017.12.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shintani AK, Girard TD, Eden SK, Arbogast PG, Moons KGM, Ely EW. Immortal time bias in critical care research: application of time-varying Cox regression for observational cohort studies. Crit Care Med 2009;37:2939–2945. doi: 10.1097/CCM.0b013e3181b7fbbb [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Husain H, Thamrin SA, Tahir S, Mukhlisin A, Apriani M. The application of extended cox proportional hazard method for estimating survival time of breast cancer. IOP Conf Ser J Phys Conf Ser 2018;979:12087. doi: 10.1088/1742-6596/979/1/012087 [DOI] [Google Scholar]
- 13.National Library of Medicine . DailyMed. Available at: https://dailymed.nlm.nih.gov/dailymed/. Accessed October 29, 2020. [DOI] [PubMed]
- 14.The Chronic Condition Warehouse . Chronic Conditions Data Warehouse: CCW Chronic Condition Algorithms [Internet]. Available at: https://www.ccwdata.org/web/guest/condition-categories. Accessed January 23, 2017.
- 15.Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: competing risks and multi-state models. Stat Med 2007;26:2389–2430. doi: 10.1002/sim.2712 [DOI] [PubMed] [Google Scholar]
- 16.Willems SJW, Schat A, van Noorden MS, Fiocco M. Correcting for dependent censoring in routine outcome monitoring data by applying the inverse probability censoring weighted estimator. Stat Methods Med Res 2018;27:323–335. doi: 10.1177/0962280216628900 [DOI] [PubMed] [Google Scholar]
- 17.Wyss R Gagne JJ Zhao Y, et al. Use of time-dependent propensity scores to adjust hazard ratio estimates in cohort studies with differential depletion of susceptibles. Epidemiology 2020;31:82–89. doi: 10.1097/EDE.0000000000001107 [DOI] [PubMed] [Google Scholar]
- 18.Spreeuwenberg MD Bartak A Croon MA, et al. The multiple propensity score as control for bias in the comparison of more than two treatment arms: an introduction from a case study in mental health. Med Care 2010;48:166–174. doi: 10.1097/MLR.0b013e3181c1328f [DOI] [PubMed] [Google Scholar]
- 19.Adams H, Adams HHH, Jackson C, Rincon-Torroella J, Jallo GI, Quiñones-Hinojosa A. Evaluating extent of resection in pediatric glioblastoma: a multiple propensity score-adjusted population-based analysis. Childs Nerv Syst 2016;32:493–503. doi: 10.1007/s00381-015-3006-x [DOI] [PubMed] [Google Scholar]
- 20.Samson LW, Finegold K, Ahmed A, Jensen M, Filice CE, Joynt KE. Examining measures of income and poverty in medicare administrative data. Med Care 2017;55:e158–e163. doi: 10.1097/MLR.0000000000000606 [DOI] [PubMed] [Google Scholar]
- 21.Parker WH. Bilateral oophorectomy versus ovarian conservation: effects on long-term women's health. J Minim Invasive Gynecol 2010;17:161–166. doi: 10.1016/j.jmig.2009.12.016 [DOI] [PubMed] [Google Scholar]
- 22.Manson JE Aragaki AK Rossouw JE, et al. Menopausal hormone therapy and long-term all-cause and cause-specific mortality: the Women's Health Initiative randomized trials. JAMA 2017;318:927–938. doi: 10.1001/jama.2017.11217 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stute P, Stadler A, Heufelder A. The impact of menopausal hormone therapy on overall mortality—a comprehensive review. JClimacteric 2020;23:447–459. doi: 10.1080/13697137.2020.1767568 [DOI] [PubMed] [Google Scholar]
- 24.Schwartz AG Wenzlaff AS Prysak GM, et al. Reproductive factors, hormone use, estrogen receptor expression and risk of non small-cell lung cancer in women. J Clin Oncol 2007;25:5785–5792. doi: 10.1200/JCO.2007.13.3975 [DOI] [PubMed] [Google Scholar]
- 25.Pesatori AC Carugno M Consonni D, et al. Hormone use and risk for lung cancer: a pooled analysis from the International Lung Cancer Consortium (ILCCO). Br J Cancer 2013;1091954–1964. doi: 10.1038/bjc.2013.506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Newcomb PA Zheng Y Chia VM, et al. Estrogen plus progestin use, microsatellite instability, and the risk of colorectal cancer in Women. Cancer Res 2007;67:7534–9. doi: 10.1158/0008-5472.CAN-06-4275 [DOI] [PubMed] [Google Scholar]
- 27.Delellis Henderson K Duan L Sullivan-Halley J, et al. Menopausal hormone therapy use and risk of invasive colon cancer: the California Teachers Study. Am J Epidemiol 2010;171:415–25. doi: 10.1093/aje/kwp434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Symer MM, Wong NZ, Abelson JS, Milsom JW, Yeo HL. Hormone replacement therapy and colorectal cancer incidence and mortality in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Clin Colorectal Cancer 2018;17:e281–e288. doi: 10.1016/j.clcc.2018.01.003 [DOI] [PubMed] [Google Scholar]
- 29.Koch T Therming Jørgensen J Christensen J, et al. Bilateral oophorectomy and rate of colorectal cancer: a prospective cohort study. Int J Cancer 2022;150:38–46. doi: 10.1002/ijc.33776. [DOI] [PubMed] [Google Scholar]
- 30.Parker WH. Ovarian conservation versus bilateral oophorectomy at the time of hysterectomy for benign disease. Menopause 2014;21:192–194. doi: 10.1097/GME.0b013e31829be0a0 [DOI] [PubMed] [Google Scholar]
- 31.Vehkavaara S Silveira A Hakala-Ala-Pietilä T, et al. Effects of oral and transdermal estrogen replacement therapy on markers of coagulation, fibrinolysis, inflammation and serum lipids and lipoproteins in postmenopausal women. Thromb Haemost 2001;85:619–625. [PubMed] [Google Scholar]
- 32.Luyer MDP, Khosla S, Owen WG, Miller VM. Prospective randomized study of effects of unopposed estrogen replacement therapy on markers of coagulation and inflammation in postmenopausal women. J Clin Endocrinol Metab 2001;86:3629–3634. doi: 10.1210/jcem.86.8.7768 [DOI] [PubMed] [Google Scholar]
- 33.Mohammed K Dabrh AMA Benkhadra K, et al. Oral vs transdermal estrogen therapy and vascular events: a systematic review and meta-analysis. J Clin Endocrinol Metab 2015;100:4012–4020. doi: 10.1210/jc.2015-2237 [DOI] [PubMed] [Google Scholar]
- 34.Beral V; Million Women Study Collaborators. Breast cancer and hormone-replacement therapy in the Million Women Study. Lancet 2003;362:419–427. doi: 10.1016/s0140-6736(03)14065-2 [DOI] [PubMed] [Google Scholar]
- 35.Speth RC, D'ambra M, Ji H, Sandberg K. A heartfelt message, estrogen replacement therapy: use it or lose it. Am J Physiol Heart Circ Physiol 2018;315:H1765–H1778. doi: 10.1152/ajpheart.00041.2018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hodis HN, Collins P, Mack WJ, Schierbeck LL. The timing hypothesis for coronary heart disease prevention with hormone therapy: past, present and future in perspective. Climacteric 2012;15:217–228. doi: 10.3109/13697137.2012.656401 [DOI] [PMC free article] [PubMed] [Google Scholar]