

ABSTRACT
Inuit youth in Nunavut (NU) are resilient but face a protracted suicide crisis. The SPARX serious game and e-intervention, developed originally in New Zealand, teaches youth cognitive behavioural therapy (CBT) skills to ameliorate stress and depression. Inuit youth in NU reviewed and culturally adapted SPARX and an existing wellness outcome measure for Inuit. One hundred and twenty-one youth, aged 13 to 24, across NU then tested, played, and evaluated I(nuit)-SPARX, showing improvement in several areas of wellbeing post-play. Youth completed a CBT skills survey, engaged in sharing circles to assess CBT skill retention, and shared their thoughts about the usefulness and cultural fit of I-SPARX with Inuit Qaujimajatuqangit (IQ). Communication Skills, Listening Skills, and Problem Solving emerged as the most helpful learned CBT skills, and NU youth provided real-world examples of using I-SPARX skills to support their mental wellness. Several principles of IQ were exemplified and upheld in the content of the adapted SPARX tool and the process of the project as a whole. Empirically grounded, asynchronous e-tools, developed in collaboration with Inuit communities to ensure cultural specificity, may support psychological wellness in communities where mental health resources are scarce.
KEYWORDS: Community-based participatory action research, serious games, mental wellness, Inuit, cognitive behavioural therapy, adolescent health
Inuit youth in Northern Canada are remarkably strong in the face of extreme inequities that persist in the context of colonialism, and significant unmet mental health needs. Pervasive youth suicide is a public health emergency of epidemic proportions and the most urgent challenge facing Inuit today [1,2]. Once unheard of among youth and occurring only infrequently among the elderly and very ill, death by suicide in Inuit communities spiked during the 20th century [3,4]. Rates of suicide among Inuit male youth are nine times the Canadian national average [5]. Inuit communities have advocated an urgent imperative to generate novel, holistic approaches to address this crisis, by creating and evaluating prevention and intervention tools that build on existing cultural strengths, are appropriate to Inuit communities, and accessible and sustainable in Northern Canadian contexts where mental health resources are scarce. To effectively address these goals, it is of utmost importance that mental wellness research embraces a community-directed approach wherein Inuit define their research priorities, act as leading decision-makers in research activities, exercise control, and own research products [6,7].
This study endeavoured to meet this multivocal call: the present paper reviews Making I-SPARX Fly in Nunavut (I-SPARX), a five-year community- and youth-directed mental wellness initiative, developed in partnership with members of five Nunavut hamlets and evaluated by youth across the NU territory. Guided by principles of Inuit Qaujimajatuqangit as suggested by youth leaders and community members I-SPARX aimed to enhance resilience by empowering youth with cognitive behavioural therapy (CBT) skills to foster their own mental health and positively contribute to the collective welfare of their communities.
Inuit youth mental health: ecological stressors and unique challenges
Among youth in general, poor emotion regulation (ER) strategies, such as ruminating, catastrophizing, and endorsing hopelessness about the self, the world, and the future, predict depression [8–10]. Among Inuit youth specifically, suicidality is linked to compounding sequelae of colonialism, including family and community histories of trauma, depression, and suicide, and personal histories of childhood trauma, hopelessness, and alcohol dependence [11,12]. All are symptomatic of a loss of culture and the enduring stress inflicted on Inuit by settlers, evangelists, and governmental sovereignty efforts [4,13]. Settler colonialism, most notably forced assimilation, removal of children from their communities, and involuntary attendance at residential schools, has profound and enduring cross-generational impacts [14,15]. These crimes against Inuit included systematic emotional, physical, and sexual abuse. Colonisation disrupted family and community bonds, introduced illicit substances (such as alcohol) and diseases (such as tuberculosis; TB), and diminished Inuit’s sense of control over their lives [3,14,15]. For male Inuit youth in particular, suicidality is associated with loss of role identity and status, strife in romantic and family relationships, mimesis and contagion, loneliness, and anger [4]. Substance use to cope with trauma, geographical isolation, and boredom further exacerbate risks for self-harm [16,17]. Ongoing marginalisation further perpetuates colonial harms, with Inuit youth facing severe resource inequalities, including food insecurity and overcrowded housing [18,19], which have been linked to increased familial conflict, psychological distress, and substance use [20–22].
To add to the many challenges faced by Inuit youth, adolescents in small, remote communities are prone to avoiding help-seeking in both informal settings and with professional services, as they may fear compromised confidentiality due to a lack of privacy and the stigma associated with mental illness. It is concerning that males are less likely to seek help considering their increased risk for suicide attempts and the fact that suicidal ideation and help-seeking are negatively correlated [23,24]. Resources for the specialised treatment of youth mental health are widely available in other Canadian regions, but youth living in remote Northern communities often go without access [25,26]. Few health care professionals train or practice in the Canadian North, and frontline workers often experience burnout due to excessive workloads and personnel shortages [27,28]. Furthermore, Northern communities may have access to health services, but those are primarily mainstream Western based, may propagate colonial systems and structures, and might not always be culturally specific [29].
Resilience can overcome self-harm, with the former construed as the ability to positively cope, find hope, and foster constructive outcomes in contexts of severe adversity [30–32]. The Inuit approach to harm reduction is relational and land-based. Intergenerational mentorship, spending time in nature, cultivating positive peer relationships, and fostering connection to culture, family, and community have been identified as important promoters of mental wellness and resilience among Inuit communities [33] MacDonald et al. [34,35]. In addition to cultural healing practices, Elders and community members have recommended that intervention programmes emphasise community engagement, highlighting a person’s strengths in the face of hardship, and providing youth with positive experiences of life [15]. Indigenous communities have called for change in how resilience is defined, and resilience research conducted, advocating more ambitious aims to achieve wellness rather than merely addressing deficits or ‘closing the gap’ [36,37]. This underscores the need for exploring culture-focused, self-administered, discreet preventive and therapeutic approaches that support the mental health of youth in these communities.
Framework for the I-SPARX project
Etuaptmumk/Two-eyed seeing
Two-Eyed Seeing (TES) is an English-language approximation of Etuaptmumk, a Mi’kmaq concept describing the gift of multiple perspectives [38,39]. A reclamation and revitalisation of Indigenous knowledges must be built on decolonial methodologies [40]. Peltier [41] has written that decolonial approaches can ‘honor and flow from Indigenous paradigms’ (p. 4) through TES. This weaving process embodies the consciousness of ‘it’s us, together’ and involves several key directives derived from a study conducted by Bartlett and colleagues in 2012 [38]: a) acknowledging that we (Northern Inuit knowledge-keepers together with Western trained scientists from the Canadian “South”) benefit from learning from each other and that our learning journey must be collaborative; b) embodying an inclusive view of science; c) doing and showing rather than just talking; d) reflecting on our values, actions, and knowledges; e) weaving back and forth between worldviews.
Among Inuit, Elders and other cultural experts have indicated a propitious fit between long-established, culturally embedded helping approaches and some Western therapeutic techniques considered effective in other geographic locales [42,43]: Inuit have always adapted diverse perspectives and ideas, and innovative practices and technology to complement, existing effective practices rooted in a long-standing philosophy of life [43,44], (p. 9). Conceptualising such an integration of perspectives as a binocular vision of sorts seems appropriate, but the growing and sometimes insufficiently informed use of TES by non-Indigenous researchers is controversial and has been criticised (e.g [43,45,46]. Amongst other things, it cannot be assumed that a research approach conceived by a Mi’kmaq scholar should necessarily be suitable to Inuit culture. However, guided by the project’s Elder advisors’ and Inuit youth leaders’ endorsement (see Methods), the I-SPARX research team espoused TES as an organising principle and framework in this research, with the IQ worldview representing the Inuit eye and CBT representing the Western/Southern eye.
Inuit Qaujimajatuqangit (IQ)
Inuit Qaujimajatuqangit (IQ) is an all-encompassing complex worldview and philosophy that has guided Inuit living over millennia. IQ has recently been formally operationalised by the Government of Nunavut [47] into eight overarching principles that represent family and community bonds, collective decision-making, and respect for land and animals [44]. IQ effectively integrates cultural unity, practical knowledge, and resilience [48,49]. IQ principles promote culture as a resource for success and highlight the need to look at culture for knowledge and values to promote healing and sustainability [50]: ‘Cultural identity is central to knowing where you are, where you have been, and where you may go. It is, therefore, a central part of healing, recovery, and empowerment’ [13] (p. 8). The importance and helpfulness of IQ, especially in an Arctic environment, was central to Inuit community members’ accounts of surviving and thriving under COVID-19 [51]. Community-based participatory research, such as the I-SPARX project described here, is intended to ensure that worldviews of participants guide the project. Inuit research team members expressed their intent to integrate Inuit traditional knowledge throughout both the process and content of I-SPARX. Their personal understandings of IQ thus informed the content development of the adapted game, as well as the manner in which project activities and knowledge dissemination were conducted.
Cognitive behavioural therapy & game based e-tools
CBT is a cross-culturally researched and extensively validated intervention that teaches participants to modify unhelpful cognitions, distorted beliefs, and behaviours that can result in low mood and depression [52,53]. CBT postulates that thoughts and/or behaviours precede mood and that mood can be lifted and stabilised by changing thought patterns and unhelpful behaviours [54,55]. CBT is demonstrably more effective in treating adolescent depression than other less directive forms of therapy [56]. Despite its origins in Western/Southern culture, CBT is regarded as a well-established and often a preferential intervention for youth from non-Western cultural groups [57]. Māori youth (the Indigenous young people of Aotearoa/New Zealand), for example, thought that a CBT-based serious game intervention developed with them in mind was both appealing and applicable [58]. According to an evidence-based status evaluation by Pina et al. [59], CBT techniques accounted for over 58% of mental health treatments deemed efficacious or potentially efficacious for non-Western youth. However, notable gaps remain in the literature, with most studies failing to evaluate the effectiveness and implementation of culturally adapted CBT. This may be because adaptations are often developed by community clinicians who are not associated with university research teams. Notably, there is a dearth of studies that specifically focus on or include Indigenous youth [57].
Many youths in Nunavut have grown up surrounded by networked digital devices that play an integral part in their lives. This applies especially after the increased online demands of the COVID-19 pandemic. Despite this, compared to the rest of Canada, broadband connectivity throughout Inuit Nunangat has historically been expensive, slow, unreliable, and vulnerable to weather conditions [60]. Nevertheless, gradual efforts are being taken to improve internet connectivity in the Canadian North. For example, in 2016, the Canadian Radio-television and Telecommunications Commission [CRTC] announced that all Canadians should have access to a standard of Internet speeds of at least 50 Mbps download and 10 Mbps upload (50/10 Mbps) [61]. In 2019, the CRTC launched the Broadband Fund, which aims to close the digital gap in Canada by improving high-speed Internet services in rural and remote communities – allowing some communities to access the national standard of 50/10 Mbps for the first time [62,63]. Through the Broadband fund, in 2024 the Government of Nunavut received funding to build a 1,300 kilometre fibre link, which will bring high-speed, fibre Internet to approximately 4,235 households across four communities: Salliq/ᓴᓪᓕᖅ/Coral Harbour, Iqaluit/ᐃᖃᓗᐃᑦ, ᑭᒻᒥᕈᑦ/Kimmirut, and Kinngait/ᑭᙵᐃᑦ/Cape Dorset [64]. Additionally, in 2023, SSi Canada received funding to upgrade its satellite transport capacity in all 25 communities in Nunavut, encompassing approximately 11,400 households [63]. Furthermore, with the recent, albeit contested arrival of low earth orbit satellite constellations such as Starlink and OneWeb [65], some Nunavummiut have additional and faster options for their Internet service [66]. Lastly, through various discussions with youth leaders and community partners, Internet speeds in some areas of Nunavut are slowly improving. In this context, digital and computerised interventions that are engaging, and effective tools for treating mental health challenges with youth [67–70] are becoming more accessible. Of particular relevance for the current project, which engages youth in remote Northern communities, digital technologies are also positioned to help overcome barriers to treatment access such as geographical isolation and stigma, and promote the scalability and reach of interventions to youth who might not normally seek help through traditional mental health services [27,68,71,72]. Additionally, digital gameplay is posited to be an effective and efficient means by which young people generate and experience positive feelings, providing youth opportunities to learn and exercise adaptive ER strategies like problem solving, acceptance, and reappraisal [67]. In the context of mental health research, video games have demonstrated effectiveness in targeting mental health symptoms and teaching positive coping and ER skills while stimulating engagement and enjoyment [68,71]. In their review of digital serious games (e-interventions that utilise gaming for serious purposes) and gamification (the use of gaming features and design elements, such as rewards, narratives, and personalisation, in programmes that are not meant as games per se), Gentry and colleagues [73] found these interventions to be at least, if not more, effective than controls for improving knowledge, skills, and user satisfaction. For instance, gamification can facilitate the visualisation of complex ideas such as negative thoughts and allow users to manipulate and overcome such images [74]. However, systematic, controlled studies about the benefits and potential drawbacks of digital interventions are still scarce [75].
SPARX and Cultural considerations
Harnessing the synergistic potential of CBT and digital gamification, SPARX (Smart, Positive, Active, Realistic, X-Factor thoughts) is a serious game, playable on computer and mobile devices, originally designed and developed at the University of Auckland by a team of Indigenous and non-Indigenous researchers. SPARX teaches users CBT and ER skills to cope with stress and depression by challenging negative thoughts, feelings, and behaviours, represented in the computer game as GNATs – Gloomy Negative Automatic Thoughts (see [74] above). The SPARX fantasy adventure game has seven sequential modules focused on five domains: problem-solving; being active; dealing with negative thoughts; social skills; and relaxation. The player, with guidance from an Elder character and narrator, navigates through these seven levels by solving mini-games (such as word puzzles, thought exercises, etc.), exploring the land, overcoming challenges, and collecting power gems to restore balance in the fantasy world of the game. The New Zealand design team tailored the game as an intervention to address the specific requirements of underserved groups of youth, including Māori rangatahi (young people) in Aotearoa, New Zealand [58,69]. Studies in Aotearoa and rural Australia reported that the programme is useful in supporting privacy and choice, combating depressive thoughts, and potentially decreasing feelings of social isolation [69,76].
With these cultural foundations and promising results in mind, the I-SPARX research team conducted a mixed-methods pilot study in 2014 with the Nunavut territorial Department of Health to evaluate the effectiveness of the original version of SPARX in boosting resilience against depression among 22 Inuit youth in 11 communities in Nunavut [26,27]. SPARX proved engaging and promising as an intervention to support Inuit youth with skill development to regulate their emotions, challenge maladaptive thoughts, and provide behavioural management techniques such as deep breathing. However, youth also expressed the need for an adaptation of SPARX that weaved Inuit culture into the game. They contended that integrated cultural elements would enhance the potential of SPARX to foster cultural pride, community resilience, youth capacity and engagement, and mental health literacy.
In 2017, with funding from the Canadian Institutes of Health Research (CIHR), the I-SPARX research team began working with Nunavut communities on Making I-SPARX Fly in Nunavut (I-SPARX). I-SPARX leveraged SPARX as part of a multi-pronged approach to develop and assess a comprehensive, ecologically appropriate intervention to address core factors that potentially contribute to suicidality in Inuit youth. By promoting healthy approaches to emotion regulation, addressing hopelessness in youth, and supporting healthy cognitions through CBT, the principal objectives of this community-based project were to harness cultural strengths to adapt a game that has the potential to bolster personal resources that might boost resilience [3,28]. Specifically, the research team worked closely with a group of Inuit youth project leaders and communities using a holistic, integrated IQ framework (see [77]) to design and culturally adapt SPARX, test the adaptation with youth using a community-designed outcome measure, share knowledge built from the intervention and the research process – and, if warranted by positive results, distribute the game itself – in a way that was helpful and meaningful to Inuit Nunavummiut.
Methods
Participants
Community members and Elders from seven communities in three regions of Nunavut, 27 youth leaders (ages 15 to 26; Female: 7; Male: 20), and 121 youth testers from 17 Nunavut communities and one Inuit Ottawa, Ontario community (ages 13 to 24; Female: 68; Male: 48; Transgender Male: 2) participated in the I-SPARX initiative between 2018 and 2022. Recruitment activities for each group are specified below for each project phase.
Procedure
The initiative consisted of four objectives and phases: 1) the introduction of CBT and adaptation of SPARX to an Inuit context directed by youth leaders and community members including Elders; 2) the development of a community compatible outcome measure for mental wellness; 3) the territory-wide testing of the adapted e-tool; and 4) the translation/mobilisation of the knowledge acquired during this project for participating communities. Along with community partners Isaksimagit Inuusirmi Katujjiqatigiit Embrace Life (a non-profit suicide prevention organisation based in Nunavut), Pinnguaq (a not-for-profit group that provides e-play experiences in Indigenous languages as a means of unifying and enabling Nunavummiut), and Nunabox (an Inuit cultural consultant and liaison), youth leaders guided and were actively involved in the project every step of the way – outreach and recruitment, outcome measure development, game (re)design, intervention testing, process evaluation, and knowledge mobilisation.
Phase 1: introduction of the project framework and adaptation of SPARX (recruitment of youth leaders; consultation with youth leaders and community representatives; design changes; review of the adapted e-tool by youth leaders)
Based on recommendations of Inuit youth and community facilitators who participated in Bohr et al. [27] the first objective was to introduce the project’s guiding framework (including TES, IQ, and the CBT model) and adapt SPARX to be a better fit for Inuit players. A council of 27 Inuit Youth Leaders was recruited during initial one-week visits to five Nunavut communities in the Spring and Summer of 2018: Qamani’tuaq/ᖃᒪᓂᑦᑐᐊᖅ/Baker Lake, Iqaluktuuttiaq/ᐃᖃᓗᒃᑑᑦᑎᐊᖅ/Cambridge Bay, Kinngait/ᑭᙵᐃᑦ/Cape Dorset, Panniqtuuq/ᐸᖕᓂᖅᑑᖅ/Pangnirtung and Mittimatalik/ᒥᑦᑎᒪᑕᓕᒃ/Pond Lake and two meetings in Nunavut in 2019. Youth from three of these communities further participated in a sharing-and-feedback youth retreat in Iqaluit/ᐃᖃᓗᐃᑦ in April 2019, which also featured workshops on mental health literacy and research ethics. When not in the communities, the York University branch of the research team maintained contact with Nunavut team members by phone and video calls, email, and social media messaging.
Throughout the initial community visits and the 2019 retreat, the York University team presented the project’s guiding framework as outlined above to youth and community members, who strongly endorsed the use of TES as a framework for the collaborative initiative. Community members also engaged in discussions to explore how I-SPARX would align with IQ principles, both in its content (i.e. the CBT skills taught within the game) and in the plan for its development. Through these discussions, five of the eight IQ principles were highlighted as relevant to the I-SPARX initiative: Pijittirniq (serving), Aajiiqatigiingniq (consensus decision-making), Pilimmakharniq (skills and knowledge acquisition), Ikajuqtigiingniq (collaborative relationships), and Qanuqtuurniq (being resourceful to solve problems) [47]. Specifically, the initiative sought to support youth mental health through CBT skill acquisition for the purpose of personal and collective problem-solving. The initiative focused on building relationships between researchers, youth, Elders, parents, teachers, community workers, and organisations through the process of developing I-SPARX and through teaching effective interpersonal skills through the intervention itself. The initiative also emphasised a holistic understanding of wellbeing, encompassing social, emotional, spiritual, cognitive, and physical wellness, through the development of a culturally appropriate community-developed outcome assessment to be used to evaluate wellness benefits accrued from playing the game (see Phase 2).
During these meetings, youth and community members also made suggestions regarding the adaptation of the SPARX game. Changes suggested were recorded and shared with Pinnguaq whose task was to stylistically adapt SPARX, resulting in an Arctic-looking game that included elements such as Inuit languages, Arctic landscapes, animals, Inuit clothing, and Inuit cultural symbols. Please see Appendix A1, A2, A3, and A4 for visuals of SPARX and I-SPARX demonstrating those adaptations. While conceptual modifications were also suggested by youth leaders (e.g. culturally-relevant challenges/activities), the adaptation was limited by funding constraints and only stylistic changes were possible. All changes and adaptations were then presented to members of the youth council and representatives from three communities for review of the new Inuit-SPARX (I-SPARX) program at the 2019 retreat. Youth leaders and community members took great pride in seeing their culture represented in the stylistic changes of the adapted game.
Phase 2: development of a community-developed outcome measure and interview questions
Prior to testing I-SPARX, the research team worked iteratively with Inuit youth and communities to develop culturally appropriate evaluation tools. Feedback was sought from youth and community members during the youth summit retreat in Iqaluit/ᐃᖃᓗᐃᑦ in April 2019, a youth group visit to York University in July 2019, several online meetings throughout 2020, and ongoing Facebook messaging and polling. Youth provided their feedback on the types of questions that should be asked and the way they should be posed (e.g. Likert scales, multiple choice options, open-ended questions). The result of these discussions was the ‘I-SPARX Wellness Questionnaire’, a 39-item Likert-scale questionnaire adapted from Wabano and Young’s ‘Aboriginal Children’s Health and Well-Being Measure’ for Indigenous communities [78]. Based on youth feedback, additional survey questions and interview questions were generated to gather further information regarding participants’ experiences playing I-SPARX. The development and psychometric properties of the I-SPARX Wellness Questionnaire are described in a forthcoming paper [79].
Phase 3: territory-wide testing of I-SPARX
The I-SPARX trial took place during the unexpected COVID-19 pandemic. The original game-evaluation phase of the project was designed with the intention that the York University-based research team, along with a community coordinator, game developers, and youth leaders, would travel to the five Nunavut partner communities in 2020. The objective was to administer the game in schools and at community gathering spaces. The pandemic’s travel restrictions prohibited these plans and necessitated substantial changes to the evaluation procedures. In consultation with the community partners and Inuit youth leaders, the team transitioned to a Nunavut-wide hybrid evaluation model wherein the I-SPARX game was made available for download on the project’s online website (www.isparxnunavut.com), allowing youth to test the tool at home or where permitted under pandemic guidelines with support from community facilitators.
To evaluate I-SPARX, Inuit youth in Nunavut between the ages 13 and 24 were recruited through youth leaders, social media (e.g. Facebook, Instagram, Twitter/X), flyers posted in communities, schools, and local community facilitators. If needed, arrangements were made to provide youth with the necessary technology to participate (e.g. shipping a tablet, purchasing an internet package). Once registered, participants were randomly assigned to either the ‘Play Now’ group, with gameplay scheduled to start the week following their registration, or the ‘Play Later’ (waitlist control) group, with gameplay scheduled to start four weeks after registration. Prior to gameplay, youth were emailed a link to an online survey (Time 1), which included a consent form, a demographic survey, and the I-SPARX Wellness Questionnaire. Youth in the Play Later group completed the I-SPARX Wellness Questionnaire at two time points before testing the game, first at baseline (Time 0) and then again four weeks later (Time 1), to address the reliability of the measure. The ‘Play Later’ process was discontinued partway through the project in an effort to reduce participant attrition. Upon completion of the pre-intervention questionnaire, youth were sent a link to download the I-SPARX game onto their computer or mobile device and were instructed to play the first level of the game. Email reminders were sent every three to four days informing participants to play the next level of the game. Once youth had played all seven levels, they were sent the link to the post-intervention survey (Time 2), which again included the I-SPARX Wellness Questionnaire and questions about their gaming experience. Fifty-six youth from across Nunavut were recruited in this way, and 35 completed all levels of the game and the final survey.
Although non-Nunavummiut team members were prohibited from travelling to Nunavut to help facilitate in-person testing during the pandemic, select Nunavut-based community members and organisations were able to host small in-person workshops where youth could play I-SPARX as a group, when permitted under pandemic restrictions. Four workshops took place (three at Kitikmeot communities; Cambridge Bay, Taloyoak, and Gjoa Haven, and one at Tungasuvvingat Inuit, an Ottawa-based organisation for Inuit). Workshop leaders followed territorial/provincial, community-specific, and university pandemic guidelines. In this group context, participants did not play I-SPARX at a scheduled pace and could choose to play multiple levels per day. Sixty-five youth were recruited in this way, and 46 completed all levels and the final survey.
In total, 121 youth participated in the I-SPARX evaluation, and 81 completed all levels of I-SPARX and all surveys either individually or as a group. After completing the post-play survey, all participants were invited to sign up for interviews and sharing circles to discuss the skills they learned while playing, their opinion on the appropriateness of CBT with Inuit culture and IQ, and their thoughts on the cultural elements of the game. Seven interviews and sharing circles were conducted with 13 youth from five communities (see Appendix B for a list of the interview questions). Interviews were conducted either virtually over Zoom or in-person abiding by appropriate COVID-19 protocols. All youth participants were compensated for their time with local Northwest/Northern store vouchers or gift cards. Youth were paid $150 for completing all phases of testing ($200 for those in the waitlist control group), and an additional $50 for participating in virtual follow-up interviews/sharing circles. See Appendix C for a summative timeline and overview of activities.
Phase 4: knowledge mobilization
Knowledge mobilisation (KM) was an integral component of the project from the beginning. Accordingly, youth leaders and community partners in Nunavut were instrumental in the design of the I-SPARX game and outcome measures, in guiding the project launch (including recruitment and engagement strategies) and sharing results. In June 2021, the research team hosted a dedicated ‘KM planning’ virtual summit with I-SPARX youth leaders, drawing extensively from their expertise to distribute project findings in ways meaningful to youth and their communities (see Figure D1 for KM video shared during the 2021 youth summit). Youth-friendly posts and reels on social media, including Instagram, Facebook, and Twitter (now X), were instrumental to KM efforts, as directed by youth. With iterative youth feedback, the research team also created succinct, eye-catching KM posters in Inuktitut, Inuinnaqtun, and English to distribute to communities and project partners (see Figures D2, D3, and D4 for examples). I-SPARX KM, as well as youth council and community partner engagement and commitment, also catalysed the advancement of two extension projects led by Bohr et al. and funded by CIHR: the COVID-19 Resilience Project (2022–2023) and the Virtual Qaggiq Project (2022–2026).
Outcome measure
The post-play evaluation survey consisted of the I-SPARX Wellness Questionnaire and a series of multiple-choice, rank-order, and open-ended questions, including which skills taught in I-SPARX youth found most useful and how they used these skills in their everyday lives with family and friends (see Appendix E for examples of questions). The I-SPARX Wellness Questionnaire covers five outcome domains which correspond to seven levels of the I-SPARX game: Level 1 – Finding Hope, Level 2 – Being Active, Level 3 – Dealing with Emotions, Levels 4–7 – Overcoming Problems and Challenging Unhelpful Thoughts, and Overall Wellbeing.
Data analysis
This study used mixed analytic methods. Quantitative data were examined with a linear mixed-effect model analysis. By organising the data into long format (i.e. stacking the data from each time period), this model was considered an efficient way to combine three time points and compare the pre- and post-intervention variables (i.e. time 0 (base or control questionnaire) + time 1 (pre-gameplay questionnaire), and time 2 (post-gameplay questionnaire)) [80]. The mixed model approach was deemed suitable as it can handle imbalanced data (i.e. not all participants were measured at all time points), and it allows for the inclusion of all three time points (e.g [81]).
Frequency/percentage counts were used to generate descriptions of most/least useful concepts learned from playing the I-SPARX game. Inductive thematic analysis [82] was used to analyse post-play interview and sharing circles data. One of the authors (M.A.) read through the transcripts, generating codes based on the data and organising those codes into broader themes. An online computer program [83] was used to perform the coding and organise themes. An inductive approach was employed to allow for the development of themes from the data themselves, rather than fitting participant data to study objectives. This process was completed in collaboration with a second researcher (A.T.) to ensure consistency for all codes which were subsequently reviewed by a third team member (J.H.), who provided feedback on the final organisation of themes. Resulting themes were shared with and endorsed by youth leaders and community representatives at a project summit meeting in August 2022.
Ethics review
A research licence was obtained through the Nunavut Research Institute (NRI Research Licence #05-009-17 R-M). This research was guided by all Tri-Council guidelines for research with Indigenous Peoples and Communities [84] and Inuit Tapiriit Kanatami (ITK) guidelines [7]. Ethics approval for this research was also granted by the York University Human Participants Review Committee (HPRC), including the Indigenous Advisory Committee (Research Certificate # 2018–089). All licences were renewed yearly.
Results
I-SPARX wellness questionnaire data
A priori power calculations were not conducted due to anticipated difficulties with youth recruitment and retention. Engaging youth as active partners in participatory action research is known to be challenging [85]. This challenge is even more pronounced when working with Inuit youth in Nunavut primarily due to the harmful legacy of past and current research in Inuit communities as well as ongoing systemic stressors and barriers [7,26,86–88]. Therefore, prior to the launch of this project, it was acknowledged that an ideal sample size would likely be unattainable. The decision to engage 100 Inuit youth testers was based on the pilot study results and in consultation with Nunavut-based partners. The pilot study, which engaged a total of 24 Inuit youth across 11 communities in Nunavut, showed statistically significant (α = .05) improvements from hopelessness (p = .02) and decreases in self-blame (p = .03), rumination (p = .04), and catastrophizing (p = .03) following youth playing SPARX. Given these positive outcomes with a sample size of 24, the research team and Nunavut partners considered a total sample of 100 youth for the current project to be both feasible and robust.
Over a period of 19 months, 121 Inuit youth participated in testing I-SPARX. Among this sample, 81 participants (67%) completed all stages of the testing process, including playing the game and completing all pre- and post-intervention questionnaires. The remaining 40 participants (33%) attrited; but these participants completed at least one questionnaire before losing contact with the project team.
Prior to running the mixed linear model, the data were cleaned and quality-checked in accordance with procedures recommended by Aust et al. [89], Buchanan and Scofield [90], Ihme et al. [91], and Greszki et al. [92]. Specifically, duplicate entries, empty/no-response data, and data from youth outside the inclusion criteria were removed. Random responders were also detected and subsequently removed from the analysis through the implementation of attention checks and examination of survey completion time (see [79] for a comprehensive overview of the cleaning process). The final sample consisted of 118 youth from 14 communities in Nunavut. A demographic breakdown can be found in Appendix F.
Statistical analysis was carried out using the developmental environment and programming language for statistical computing in R and R-Studio. Because the community-designed measure has not yet been standardised, the questions in the outcome measure could not be analysed using an aggregate survey score. Instead, a linear model analysis was used to assess changes in participants’ scores per question. Average responses for each question were calculated and compared pre- and post- intervention using the mixed model analysis to determine if there was an increase (indicating positive intervention effect) or decrease (indicating negative intervention effect), the extent of this change, and whether this value was statistically significant (α = .05).
Interpreting results
Reverse responses (Q5, Q9, Q12, Q13, Q14, Q16, Q15, Q17, Q18) were re-coded in R for uniformity and improved interpretability. In the following results an increase in average score from pre-intervention to post-intervention represents an overall positive change or favourable change for that question, whereas a decrease in average score represents an overall negative or unfavourable change.
Results overall
Overall, 19 of 30 (63%) questions showed a statistically significant increase (i.e. improvement) in scores from pre- to post- gameplay at α = .05 (see Figure G1). The question with the highest average increase post-gameplay was Q23 - ‘I’m comfortable asking for support when I need it’ β = .55, p < .001 (n = 118, β0 = 2.92), and the question with the smallest increase was Q3 - ‘I feel like good things will happen’ β = .27, p = .014 < .05 (n = 118, β0 = 3.50). Seven questions showed a non-statistically significant increase in average scores. Four questions showed non-statistically significant decreases (i.e. unfavourable changes) in average scores post-gameplay. Across all 30 questions, there was an average change (β) of .25, indicating that overall, participants showed a 0.25 improvement in scores (on a scale of 1 to 5) on the outcome measure after playing I-SPARX.
A stratified analysis was conducted to assess differences between the workshop and individual gameplay groups. The workshop group exhibited greater improvements post-gameplay, with 17 out of 30 questions showing a statistically significant increase after playing I-SPARX. The individual gameplay group showed an increase in 27 out of the 30 questions post-gameplay, but only six of these questions were statistically significant at α = .05 (see Figure G2).
Results by domains on the I-SPARX wellness questionnaire
General wellness
At α = .05, six out of the seven questions selected to measure general feelings of wellness showed a statistically significant improvement in scores (β) following I-SPARX gameplay. Question 28, ‘I get a good night’s sleep’ showed the highest pre- to post change with an average increase of β = .44, p < .001 (β0 = 3.02) post gameplay. This was closely followed by Q24, ‘I appreciate what I have’ which had an average increase of β = .41, p < .001 (β0 = 3.76).
Overcoming problems
Seven questions measured participants ’perceived ability to overcome problems and recognise and challenge unhelpful thoughts. At α = .05, five of these questions showed a statistically significant increase in scores post-gameplay. Question 23, ‘I’m comfortable asking for support when I need it’, showed the highest average response increase, by β = .55 points, p < .001 (β0 = 2.90).
Dealing with emotions
Seven questions assessed participants ’ability to regulate negative emotions (i.e. anger, sadness, etc.). At α = .05, three out of seven questions showed a statistically significant increase post-gameplay, with the greatest improvement appearing for Q10, ‘When I feel a bad mood coming on, I have tools I can use to make myself feel better’ with an increase of β = .40 points, p < .001 (β0 = 3.06).
Being active
Six questions measured participant activity levels. This section included questions about perceived physical energy, the frequency of engagement in activities, and the availability of these activities in their community. At α = .05, three out of six questions showed a statistically significant increase in scores post-gameplay. The greatest improvement was for Q8, ‘I have time on my own to relax with an activity I like’ with an increase of β = .42, p < .001 (β0 = 3.35), followed by Q7, ‘I have activities that can help me when I’m feeling upset’ (β = .38, p = .0012 < .01, β0 = 3.39) and Q6, ‘I have enough energy’, (β = .36, p < .001, β0 = 2.31). Question 4 showed an increase in post-intervention score that approached significance, ‘I am physically active’ (β = .23, p = .056, β0 = 3.19).
Finding hope
Three questions assessed participants’ ability to find hope and stay positive for the future. At α = .05, two questions showed a statistically significant increase in scores following gameplay. The question with the highest average response increase post-intervention was Q2. ‘Even when things aren’t going well for me, I remind myself that things will get better’ by β = .36, p < .001 (β0 = 3.50), followed by Q3, ‘I feel like good things will happen’ (β = .27, p = .014 > .05, β0 = 3.50).
Usefulness of specific CBT skills
In the post-play survey, participants were asked to rank which of the 12 core CBT skills taught throughout I-SPARX they found most useful in their everyday lives (see Appendix H). Controlled Breathing, Communication Skills, and Asking for Help were all equally ranked as the topmost useful skills learned, with each endorsed by 16% of youth. Communication Skills, Listening Skills, and Problem-Solving were all ranked among the top five most useful skills by more than 60% of participants.
Post-play interviews: the appropriateness of I-SPARX’s CBT model for Inuit youth
Youth were asked to share their thoughts about I-SPARX’s CBT model and the usefulness of different CBT skills taught in the game across real-world contexts. Overall, youth found the model intuitive and provided examples of the perceived connections to their own thoughts, feelings, and actions. Participants described how CBT had become a helpful component of their everyday toolkit, including the management of difficult emotions (i.e. sadness, anxiety, anger), and the navigation and cultivation of healthy relationships:
I think the way CBT helps me is that I find real facts about how the world works, and so if I change my outer world, hopefully my inner world will perceive, or view, it differently and I will change my thoughts for the better. And if my inner world changes, my outer world will go change too. (Participant 1, male, age 20)
I learned how to control my feelings around others. I also learned … don’t take your anger out on them. Just breathe and try calming yourself down. (Participant 2, female, age 20)
The tools and the resources, ways for conflict resolution, it was always lingering in the back of my head after I played, and that came up like I always think like ‘oh I can learn something from this’, so I felt like that helped in all my relationships. (Participant 3, female, age 21)
Youth were also asked to share their thoughts on the fit of CBT with IQ principles and with Inuit culture in general. One interviewee commented on the general similarity between the CBT model and the tenets of IQ. Another youth expressed concerns regarding the acceptability of the CBT model in Inuit culture:
Just being a respectable [person] is the goal of the IQ principles, in my personal view, and I think it goes pretty well with CBT because a lot of it is … to just to be a better person for yourself and for others. And I feel like the IQ principles are just the same thing, it’s just values to be better for yourself and others. (Participant 3, female, age 21)
It doesn’t go together sometimes cause … two cultures cannot mix, I believe, it cannot mix, and that’s why it doesn’t go well … .It wouldn’t fit together ‘cause we can only have one culture, no matter who you are … ‘Cause if you put them together, things can go really bad too. (Participant 4, male, age 21)
Notably, no youth reported any specific perceived conflicts between the CBT model and IQ principles. A more complete discussion of Inuit youth’s feedback on the usefulness and cultural appropriateness of this CBT-based tool, including additional themes and reference to alignment with specific IQ principles, can be found in a forthcoming paper (see [93]).
Cultural pride
It is notable that many of the youth who participated in the redesign of SPARX and in the evaluation of the resulting I-SPARX commented on the feeling of pride they experienced seeing their culture represented in both the process of development and content of the new tool, which helped them feel like ‘they owned the game’ [94]. In their own words:
I feel like having it more involved with Inuit culture made it way better, in my opinion I don’t think you would meet many Inuks in New Zealand, and having actual people from the Inuit culture involved in the creation was one of the best decisions made. (Participant 5, male, age 14)
The Inuit culture was nice to see in a game. You don’t see that often. (Participant 6, male, age 16)
I remember loving the fact that the kakivak was used as a magical weapon. Some of the clothes were cool. Most of all I loved the voice actors, made me feel right at home most of all. (Participant 7, female, age 24)
I really like how it had more to do with Inuit culture like riding on the big tulugaq because it creates a nice safe zone for Inuit so they don’t feel left out of things. (Participant 8, male, age 14)
It was cool. It felt like I belonged. (Participant 9, female, age 19)
Discussion
Nunavummiut have called for action to address the mental health crises that burden their communities and result in unacceptable rates of youth self-harm. The purpose of this project was to introduce CBT and adapt an existing CBT e-tool to an Inuit context in collaboration with Inuit youth and community members; to test the culturally adapted e-tool with a community-developed outcome measure in a territory wide trial; and lastly to share results and the knowledge acquired from this project with participating communities. Outcomes such as skills acquired in domains associated with resilience by youth advisors were assessed using the I-SPARX Wellness Questionnaire, short survey questions, sharing circles, and interviews. Results suggest that I-SPARX may have been effective at promoting several aspects of wellness for Inuit youth participants and at inculcating skills useful for regulating emotions and communication related to solving problems, while generally aligning with IQ. Skills improvements were noted in many areas of wellness as measured by the questionnaire designed by youth and the responses to interview questions.
Two-thirds of items assessing youth’s ability to find hope in their lives by thinking positively about the future reflected a significant improvement, suggesting that after playing the I-SPARX game participants may have learned new skills to reframe the way they think about various aspects of their future. Thinking positively about the future may be a particularly helpful skill, considering the noted link between endorsing hopelessness about the future, depression and the risk for self-harm in research with youth [8–10].
Similarly, half of the items assessing youth’s tendency to be active by engaging in healthy activities they enjoy showed a significant improvement, suggesting that gameplay may have facilitated learning to identify and engage in healthy, adaptive activities that bring participants joy. Considering the known role, in CBT, of behavioural activation in reducing symptoms of depression and anxiety and improving quality of life in young people with depression [95], these results warrant further exploration in future research. Indeed, many youth leaders in this project shared anecdotally how very important activities such as involvement in team sports are in their communities when it comes to boosting mental wellness.
Close to half of the items assessing youth’s ability to deal with emotions showed a positive change. Difficulty with emotion regulation involves a diminished ability to respond constructively to an emotionally charged situation and is associated with anxiety and depressive disorders [96], unhealthy coping strategies such as substance use, withdrawal, and self-harm [97], and suicidality among young people [98]. Given the documented colonial harms experienced by Inuit communities, the resulting intergenerational trauma, and its repercussions for the development of healthy emotional coping skills, identifying strategies that are demonstrably helpful for youth in those communities is imperative. CBT has shown promise in reducing triggers and the intensity and duration of negative emotions, thus mitigating negative responses [96]. The findings of the current study corroborate the potential utility of CBT in supporting Inuit youth with specific skills to manage strong emotions and cope in healthy ways. In future, research should build on these results, and assess the usefulness of more culturally focused strategies that address trauma-related emotion regulation challenges specifically.
Finally, over two thirds of items assessing youth’s ability to problem solve, and recognise and challenge unhelpful thoughts significantly improved. At its core, CBT challenges unhelpful, self-defeating beliefs, negative views about the world, self, and the future [99] which are associated with increased risk of depression and self-harm [100]. It was reasonable to expect, and establish that learning skills to recognise and challenge unhelpful thoughts might contribute, however indirectly, to the I-SPARX project’s central objectives to mitigate depressive symptoms and enhance resilience against self-harm. It is noteworthy however that the framing of unhelpful thoughts as ‘unrealistic’ in I-SPARX was seen as problematic by some youth leaders. Such terminology was interpreted as minimising the legitimacy of negative thoughts youth had experienced. Future research will need to address in greater depth the complicated notion of modifying self-defeating thoughts in a context that is marked by social and economic inequities and discrimination, which continues to be the case for Inuit youth in Nunavut, and provide more nuanced interventions that address this dilemma. Pairing the cultivation of hope through CBT with concrete resource and opportunity mapping may be a promising avenue for future research, especially considering that less significant change was seen on the item ‘I feel like good things will happen’ - a finding that highlights the legitimacy of negative thoughts youth may experience. It will be important for future CBT interventions with Inuit communities to couple skill development with envisioning concrete, realistically accessible opportunities.
Of note, the five most noteworthy specific skills acquired by youth from playing I-SPARX as indicated by nominated usefulness, were Communication Skills, Listening Skills, Problem-Solving, Asking for Help and Controlled Breathing. The latter three are illustrative of social problem-solving which has been positively correlated with reduced suicidality in adults [101,102] and adolescents [103,104]. Research with young people in remote communities suggests that many suffer in silence, their ability and willingness to seek help impeded by a youthful penchant for self-reliance, debilitating stigma around mental illness, inadequate and inaccessible professional health services, and intergenerational fracturing and trauma [3,25,28,105,106]. Given the evidence that help-seeking and suicidality are negatively correlated [23,24], findings from I-SPARX indicating that the game promotes help-seeking behaviours among its users are especially encouraging.
When individualised support is unavailable, controlled breathing is a demonstrably useful coping skill (see also the pilot study [27]), one that some youth leaders in this project reported helped get them through challenging situations, for example the isolation of the COVID-19 pandemic [51]. Indeed, other studies employing deep breathing and breathwork techniques have evinced ER and mental wellness benefits with children and adolescents in schools [107] and demonstrated potential to mitigate stress, depressive symptoms and suicidality, and improve quality of life among adults [108–110].
Overall, there were several direct and indirect pathways to reduced suicidality that may manifest through the enhanced skill building facilitated by I-SPARX.
For the most part, Inuit youth participants in the current study appreciated the integration of CBT within the I-SPARX game. They also endorsed its compatibility with principles of IQ more generally. The notion of holism and interconnectedness was mentioned, as was the idea that each component of CBT has the betterment of self and others at its core, which is in line with the overarching IQ philosophy. Indeed, Indigenous scholars have emphasised the importance in Indigenous ways of knowing and being of interrelationships among the spiritual, the natural and the self [111], which provide opportunities to ‘embark on healing journeys’ [112].
Notwithstanding the above results, the use of CBT with Indigenous communities continues to be controversial (see [113]). While caution must be taken not to universalise Indigeneity, common elements appear in the ways Indigenous cultures conceptualise and understand health and wellness [114] and CBT may not always be compatible with those conceptualisations. However, Nelson et al. [115] persuasively suggested that the dismissal of CBT as a Westernised therapy incongruent with Indigenous ways of life risks doing Indigenous communities a disservice by denying them access to effective therapeutic techniques and approaches. In the words of an Elder: ‘Today, Inuit say they also want to develop counselling that is a combination of the best old ways and effective modern methods’ [43] (p. 9).
With its self-empowerment philosophy, pragmatic here-and-now approach, focus on skills acquisition and somatic techniques such as deep breathing, and capacity for low-intensity, self-help that potentiates cultural safety, including anonymity, CBT is a highly versatile and adaptable intervention [115,116]. CBT has been adapted with success for diverse cultures experiencing anxiety and depression across the globe, including children and youth in Japan [117], U.S. Armed Forces veterans [118], North American Indigenous children and youth [119], Indigenous South Africans [120], Māori youth in New Zealand [116], Aboriginal Australians [115,116], and Pakistani adults [121]. These cultural adaptations take many forms, including language, imagery, and metaphor, with consummate adaptation an elusive ideal. In future, researchers should aspire to engender more culturally responsive and embedded CBT, where the emphasis is on reconsidering the complexity – rather than the validity or rationality [122]—of certain negative thoughts and replacing self-defeating thoughts with self-empowering ones, and where there is a greater focus on the effect of unhelpful thinking not just on the individual, but also the community.
Compared to those in other Canadian provinces and territories, youth in Nunavut face disproportionate mental health struggles, exacerbated by lack of consistent access to mental health services. Mounting evidence endorses the use of e-interventions, including serious games, as successful therapeutic tools that could be used in private but also in a variety of clinical contexts. Now that internet connectivity has arguably improved in Arctic regions, electronic mental health programmes, such as low-intensity, self-guided CBT e-tools like I-SPARX that do not require direct, synchronous staff support, may be viable options in supporting resilience against self-harm [76,123,124]. Beyond their clinical benefit, research suggests that these tools are engaging and accessible for youth, promoting enhanced quality of life with the added benefit of decreased costs compared with traditional services [125]. These programmes may be especially effective with remote and Indigenous communities, increasing access, dismantling barriers, and filling key gaps in service provision [26,126–128] while empowering youth, enhancing their resilience and self-efficacy, and reducing depressive symptoms [27,58,68,76,129,130]. Indeed, while not assessed directly in the current study, developing a culturally adapted version of SPARX into I-SPARX, in addition to combatting depression, stress and promoting wellbeing, may have served to enhance cultural pride [94], as evidenced by comments such as this one:
It was nice to see my culture in a video game. (Participant 10, male, age 16)
In future, how CBT could reliably be delivered in an approach that is consistent with Inuit pedagogy and Inunnguiniq should be further explored.
Last, the current study’s results may prove useful to especially non-Inuit mental health clinicians working with youth in remote Northern communities, given the insights gained about the specific cognitive and behavioural skills that were deemed most helpful by youth who tested I-SPARX, and the importance accorded to the inclusion of cultural symbolic elements in that intervention. I-SPARX might prove to be a helpful adjunct tool for initiating a course of cognitive behavioural therapy provided by a clinician, or if mental health support staff are not available, can be a stand-in that at the very least is known to provide some beneficial strategies to Inuit youth.
Limitations and dilemmas
The I-SPARX project conferred promising insights into mental wellness supports and resilience among Inuit youth, but community-driven research, especially with youth in isolated remote communities, brings significant practical challenges and ethical conundra – obstacles that were exacerbated by the COVID-19 pandemic. An authentic Etuaptmumk/Two-Eyed Seeing framework may have become more elusive in early 2020 when the project transitioned to a virtual model until mid-2022, with the onset of the pandemic and its social distancing and travel restrictions. Remotely conducted research may inadvertently privilege the Western/Southern eye; even as the non-Inuit research team strived to be nimble and responsive, the authenticity with which a TES model can be implemented is limited under strictly digital modalities like Zoom, email, and social media, where there is a potential loss of genuine human connection and ‘cultural resolution’.
Another significant limitation surrounds the issue of Inuit representation on the research team, and particularly among the leadership, at the beginning of the project. While youth leaders and community advisors took on increasingly active roles as the project progressed, directed especially the later phases of the project and participated as authors in any knowledge mobilisation activity including the present paper, the initial application for funding was led by community organisations that were not all lead by Inuit, and an academic team that, while including First Nations researchers, did not include Inuit. Inuit Tapiriit Kanatami (the national organisation representing and advocating for Inuit across Inuit Nunangat and the rest of Canada) declared in their National Inuit Strategy on Research that having Inuit represented in research leadership is necessary for not only advancing Inuit governance and social equity, but for producing research that is accountable, impactful, and useful to Inuit [6]. The late 20th and early 21st century witnessed a shift towards participatory and community-based research, meant to promote respectful and meaningful relationships between non-Indigenous researchers and Indigenous communities, but much work remains in addressing power imbalances and the resulting epistemic injustices. These persistent effects of ongoing colonialism [131] tacitly sanction the oppression of Indigenous ways of knowing under Western research paradigms [132].
Two-Eyed Seeing was a guiding principle of the current research, but whether decolonial Indigenous research is genuinely achievable when projects are led by non-Indigenous researchers, and particularly White settlers, is critically debated. Indeed, as researchers, it’s important to consider whether it is genuinely possible to support Inuit-self determination without Inuit governance at all levels of a project. This situation represents an agonising paradox for academic research: Inuit ways of knowing are vital to research and mental health, however there is a severe shortage of Inuit available with the formal training for academic research or mental health support, due in part to the absence of a university in the territory of Nunavut [13]. Moreover, participation in multi-year research projects demands a significant amount of time and commitment; sustained involvement in such initiatives can be challenging for Nunavummiut [86] who already have numerous competing priorities in their service to their families and communities; yet, without interventive projects propelled by grant monies awarded to mental health advocates, the mental health crisis in the North might further intensify. The best answer, for our current project and team, was an incomplete solution pending structural and institutional paradigm shifts, which consisted in an earnest community-directed Two-Eyed Seeing approach rooted in the ‘Southern’ team’s continuous critical self-examination, checking in with Indigenous partners, and in a concerted effort to interest and engage young people in mental health research; building this type of capacity was indeed one of the objectives of the I-SPARX project as a whole. However, given that there are Inuit researchers, Nunavut-based researchers, and academics working both in Nunavut and in the South, we feel it is important to acknowledge that a TES approach will not be the best solution for every project and context.
Another paradox involved one of the key strengths of the project: the community-developed outcome measure. The co-design of a proprietary, culturally syntonic questionnaire is consistent with a TES approach. While the case for the face validity of an Indigenous-derived measure for Indigenous populations is strong, the generalisability of the measure, which is not yet standardised, and associated metrics of scientific rigour are under investigation [79]. This study assessed outcomes for Inuit Nunavummiut youth as a group and did not evaluate the potential benefits of the tool for groups of youth with formal clinical diagnoses.
Additional limitations linked to the digital nature of the intervention and concomitant accessibility and connectivity issues. The game was played entirely offline, but the download was a multi-step process requiring an Internet connection with significant data available. The game was also only available for download on PC and Android (not Apple/Mac) operating systems. Accordingly, it is likely that some youth who may have benefitted from testing the game were unable to participate due to technological incompatibilities even though the research team offered to send tablets to anyone who required equipment to participate.
The research team was also challenged to temper youth leaders’ expectations of what can be accomplished with a serious game generally, and with the stylistic re-design (‘reskinning’ in the video game industry) of an existing tool in particular. Youth-directed cultural adaptations were bound by a strict research budget and were ultimately limited to changes such as the addition of Inuit symbols, language, typical Inuit clothing and appearance for game avatars and an Arctic setting and background. Additional, more fundamental and conceptual adaptations and augmentations were desired by the youth but could not be implemented in the current study. Ultimately, a more comprehensive cultural adaptation of SPARX, as hoped for by Inuit youth, was precluded by limited resources. However, suggestions which the research team could not incorporate in I-SPARX are currently under careful consideration in the development of additional, bespoke mental wellness e-interventions.
Future research and next steps
The current study demonstrates support for the effectiveness of the I-SPARX game in boosting well-being for Nunavummiut youth. Participants’ reports suggest that they had acquired useful skills after playing and that they saw improvement in several areas of personal wellbeing. However, it is questionable whether the 121 participants from 17 of 25 existing communities in this study were representative of all Nunavut youth. Future larger-scale trials should be organised across the territory that would be more representative and offer the opportunity to examine in greater detail who benefits the most or the least from playing serious games such as I-SPARX, and who may experience adverse effects. The outcomes reported here are based on average improvement of groups as opposed to the mapping of individual trajectories of acquired skills and wellbeing. As noted, the current study was unexpectedly conducted in the context of a pandemic; it would be beneficial to conduct a similar trial under less restrictive circumstances. Future studies should also explore factors that enable community engagement in research processes in Northern Inuit communities.
Furthermore, CBT as taught in I-SPARX remains a rather individualistic approach. It will be important, in future, to consider more systems-based adaptations of this modality for collectivist cultures (see e.g [133]).
Finally, the I-SPARX findings provided insight into youths’ desires to learn helpful skills that extend beyond CBT, in a virtual setting. Future research should continue to develop and assess culturally appropriate tools to enhance resilience and wellness in Northern communities. Future studies might emphasise virtual tools that enhance resilience and mental wellness as related to the mitigation of disengagement, relational conflict, loss of agency, substance use, and self-harm. Moreover, the process of implementing I-SPARX highlights the importance of integrating culture in future studies that aim to support Nunavummiut youth resilience in the form of culturally embedded activities and tools and in ways in which outcomes are assessed. Future studies should also attempt randomised controlled methodologies and longitudinal designs, both of which should be guided by culturally acceptable values [134].
The I-SPARX game is being made available for download free of charge to any community or agency that requests it by contacting isparx.nunavut@gmail.com. However, to improve reach of this e-tool to Nunavummiut youth who may not normally seek help through conventional mental wellness services, the I-SPARX game can be taken up broadly, and made freely available to youth through schools, recreation centres, health centres, libraries, and resource centres.
Conclusions
I-SPARX is a community-participatory action mental wellness initiative designed to harmonise long-established Inuit principles with Western therapeutic techniques to ameliorate stress and depression and the potential for self-harm among Inuit youth in Nunavut, Canada. The Mi’kmaq concept of Etuaptmumk or Two-Eyed Seeing, embodying multiple perspectives in synergistic reciprocity, was a guiding principle for this project, weaving together Inuit Qaujimajatuqangit and Cognitive Behavioural Therapy throughout the youth-driven cultural adaptation and testing the I-SPARX electronic serious game. The study used a community- and youth-designed survey to measure wellness outcomes and usefulness.
Findings derived from this study indicate that there was some evidence that I-SPARX may effectively promote wellness for Inuit youth game players. Improvements were observed in the domains of hopefulness, behavioural activation, emotion regulation, and overcoming problems and challenging unhelpful thoughts. Ameliorations in each of these domains may have important implications for suicide prevention. Youth testers reported acquiring deep-breathing, communication, listening, and help-seeking skills, all of which may work in concert to promote problem-solving, another key skill youth learned in the game. In conversation, youth described finding CBT skills helpful to understanding wellness. Many youth reported that CBT aligned with IQ and Inuit culture, although a minority expressed doubts that everyone in their communities would feel the same way.
Results of this study suggest that empirically grounded, discreetly self-administrable asynchronous serious games, when developed in collaboration with Inuit communities to ensure cultural specificity, may effectively engage youth to support psychological wellness in communities where mental health resources are scarce. Such work is burdened with spectres of colonialism that endure in settler-led initiatives such as I-SPARX, and by the practical challenges of establishing meaningful and lasting relationships with members of remote Northern territories to facilitate effective collaborative knowledge-building in the spirit of Two-Eyed Seeing. In the absence of immediately viable alternatives, the investigators carry on in this work as allies-in-training, that is supporters and advocates on a learning path, following the lead of our Indigenous partners and collaborators, in the spirit of reconciliation, of reflexivity, cooperation, and hope.
Acknowledgments
We thank the Inuit youth project leaders and their communities for their devoted efforts in adapting the SPARX serious game and to create Inuit-SPARX and designing a community-specific outcome measure to assess its usefulness. We are especially thankful to the Hamlets of Qamani’tuaq/ᖃᒪᓂᑦᑐᐊᖅ/Baker Lake, Iqaluktuuttiaq/ᐃᖃᓗᒃᑑᑦᑎᐊᖅ/Cambridge Bay, Kinngait/ᑭᙵᐃᑦ/Cape Dorset, Panniqtuuq/ᐸᖕᓂᖅᑑᖅ/Pangnirtung and Mittimatalik/ᒥᑦᑎᒪᑕᓕᒃ/Pond Inlet and three leaders from Ikpiarjuk/ᐃᒃᐱᐊᕐᔪᒃ/Arctic Bay and Talurjuaq/ᑕᓗᕐᔪᐊᖅ/Taloyoak for partnering on the I-SPARX initiative. We are grateful for the enduring relationships built with community members and partner organisations in Nunavut over the past nine years. In particular, we thank Isaksimagit Inuusirmi Katujjiqatigiit Embrace Life Council, Nunabox, and Iqaluk for sharing their knowledge and guiding our work together. We also thank Pinnguaq for adapting the SPARX serious game to reflect the ideas and wishes of the youth leaders. I-SPARX would not have been possible without their support. Nakurmiik, Quana, Qujannamiik. Furthermore, we note that the original development of SPARX was carried out by a team including Associate Professor Matt Shepherd (Ngāti Tama nō Taranaki) with oversight from Kaumatua Rawiri Wharemate (Ngāti Wai. Ngāti Moerewa, Ngāpuhi) and a cultural advisory group. The software was developed by Metia Interactive, a company led by Maru Nihoniho (Ngāti Porou, Te Whānau-ā-Apanui, Ngāi Tahu).
Appendices.
Figure A1.

Screenshot of a video demonstrating several stylistic adaptations made to the original SPARX to develop I-SPARX. Stylistic adaptations depicted in the “after” section include elements such as Arctic landscapes and Inuit clothing. Please see: https://youtu.Be/rZuh3giJYMM?si=irpnrfloxydx6vpg for the full video.
Figure A2.

A visual demonstrating several stylistic adaptations made to the original SPARX to develop I-SPARX. Stylistic adaptations depicted in the “after” section include elements such as Arctic landscapes and animals (Tulugaq/Raven), Inuit clothing and tools (kakivak). Used with permission of the copyright owner © Auckland UniServices limited.
Figure A3.

Screenshot of character customisation in Inuktitut.
Figure A4.

Screenshot of the circle of hope. The figures around the circle of hope represent Arctic animals and include a polar bear, arctic fox, narwhal, muskox, arctic hare, beluga, and snowy owl.
Appendix.
Figure B1.
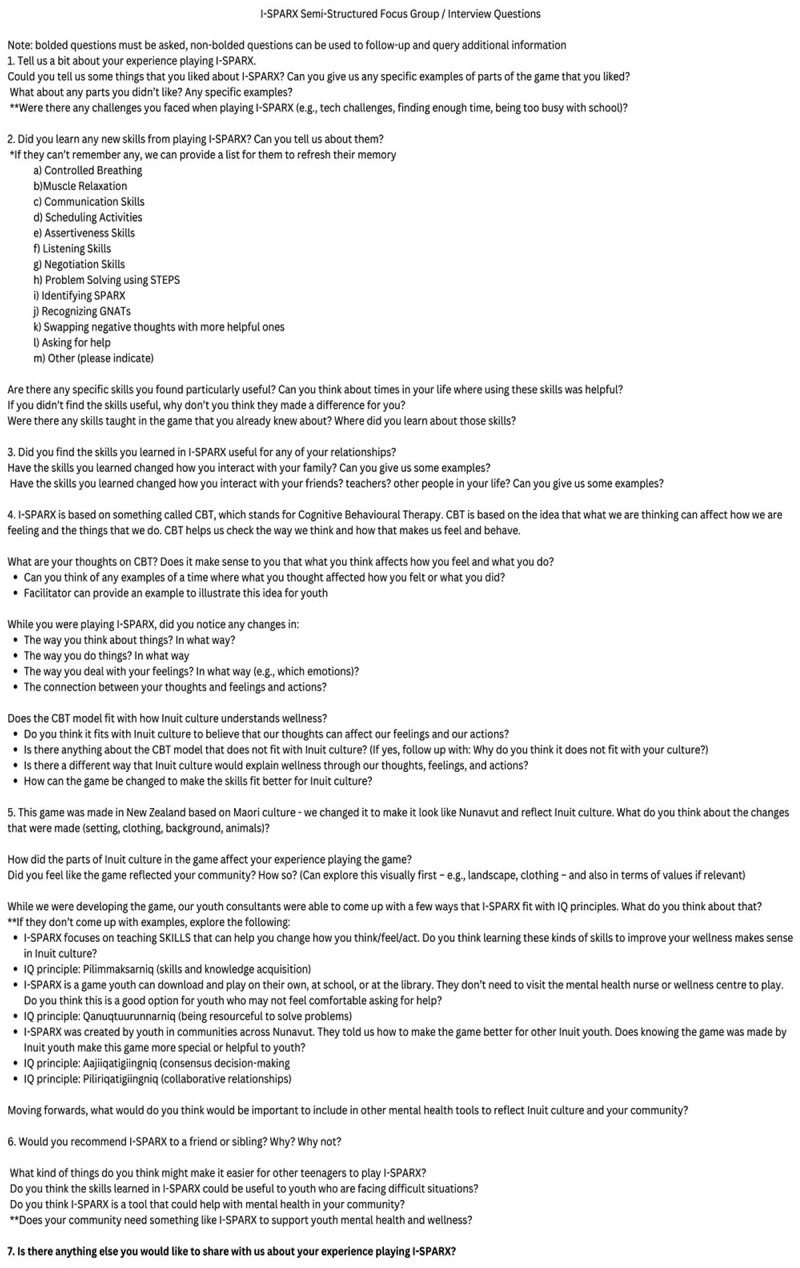
List of questions used during the interviews/sharing circles conducted with youth post-play to discuss the skills they learned while playing, their opinion on the appropriateness of CBT with Inuit culture and IQ, and their thoughts on the cultural elements of the game. Questions were posed using a semi-structured approach to guide discussion.
Appendix.
Figure C1.
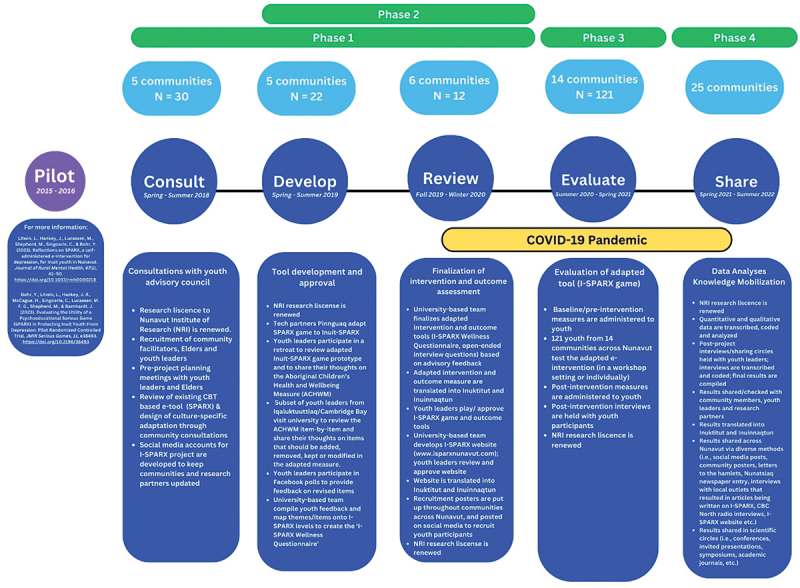
A summative timeline and overview of project activities from adaptation of the SPARX game (phase 1) to the territory-wide testing and knowledge mobilisation (phases 3-4) phases of the I-SPARX project.
Appendix.
We created an introductory knowledge mobilisation (KM) video, posted on the project website to share with youth and communities. Based on youth feedback, we also created KM posters in Inuktitut, Inuinnaqtun, and English to distribute the I-SPARX findings to communities and project partners. Posters were put up across Nunavut in youth recreation centres, grocery stores, hamlets, etc.
https://www.isparxnunavut.com/post/6-ways-to-use-instagram-for-ecommerce-marketing https://video.wixstatic.com/video/10d5ed_1457f33f0cc14f5a9f31a0ec648a82ed/720p/mp4/file.mp4
D1. Examples of knowledge mobilisation entry and video posted to the I-SPARX project website blog.
Figure D2.
Example of a knowledge mobilisation poster detailing the I-SPARX results in Inuktitut.
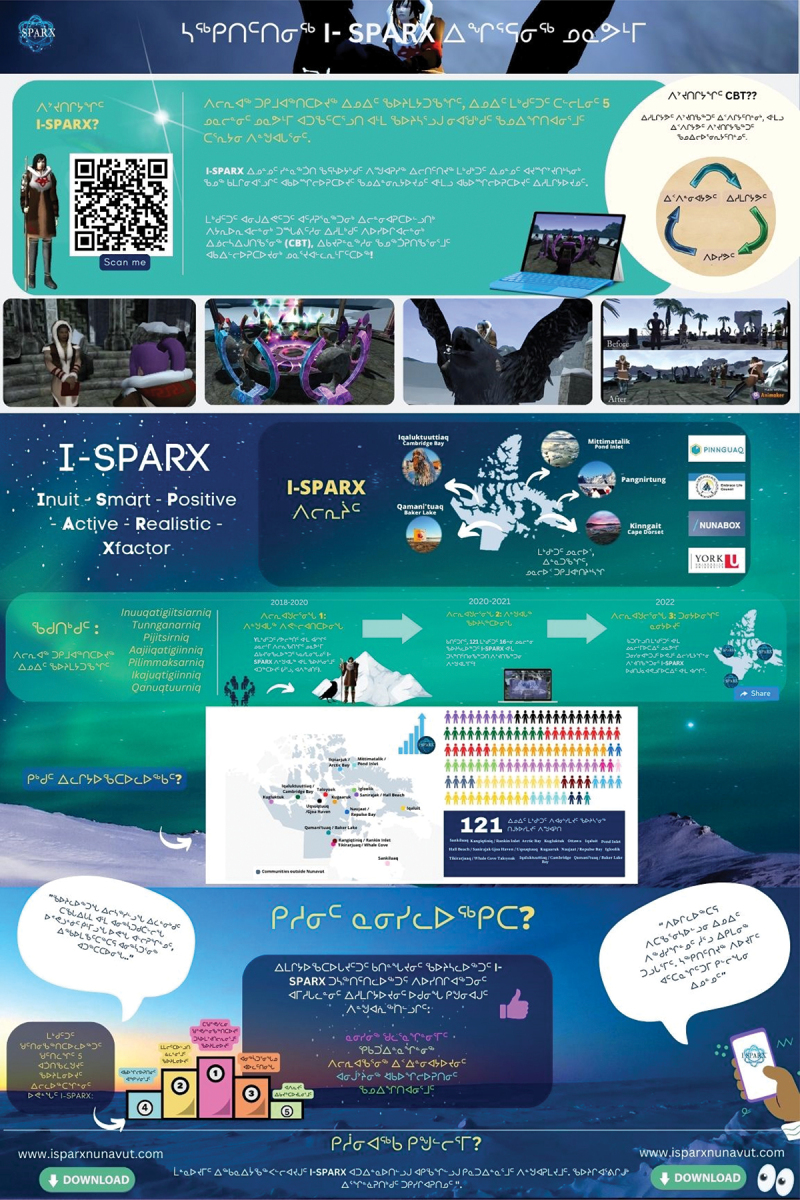
Figure D3.
Example of a knowledge mobilisation poster detailing the I-SPARX results in Inuinnaqtun.
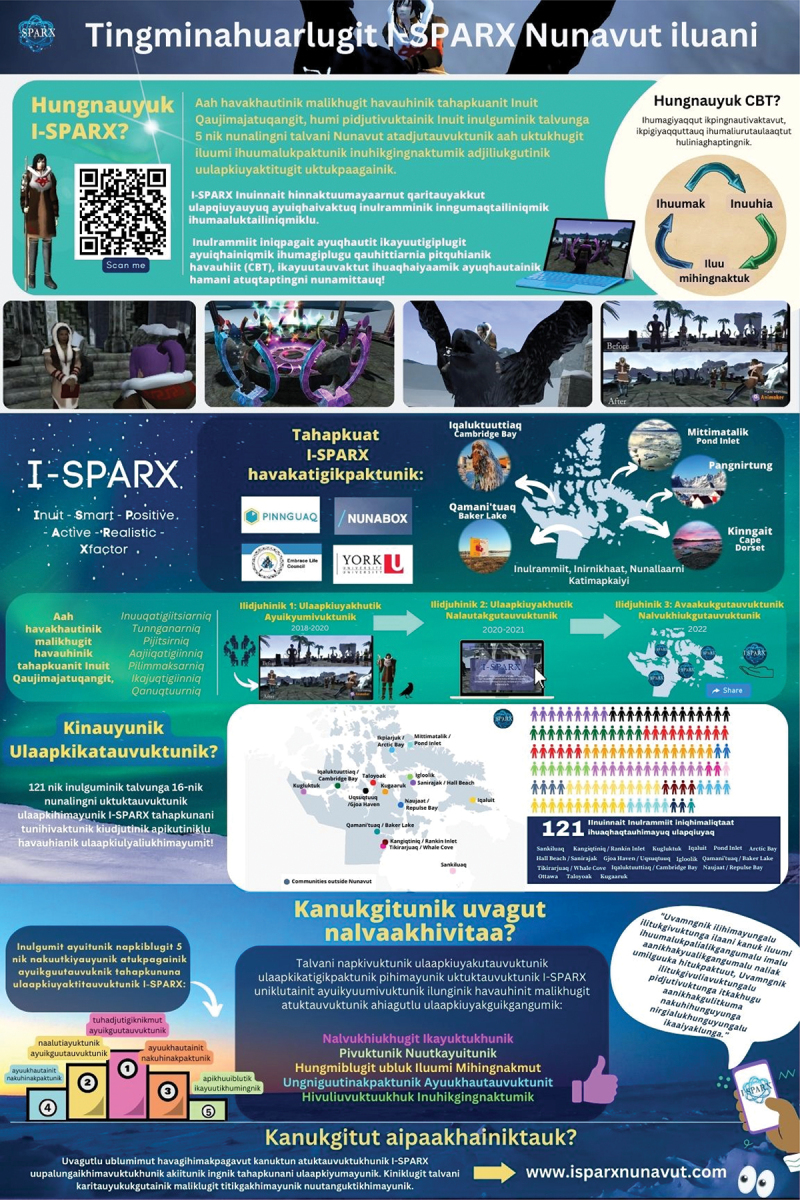
Figure D4.

Example of a knowledge mobilisation poster detailing the I-SPARX results in English.
Appendix.
Figure E1.
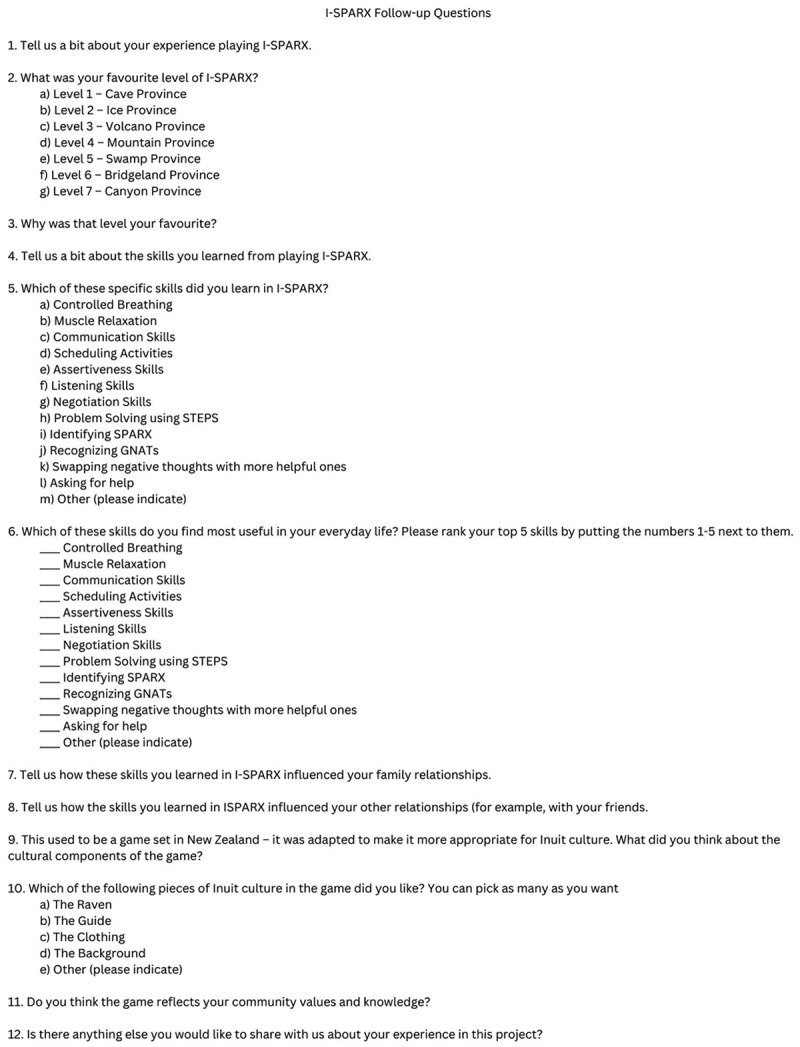
List of questions used in the post-play evaluation survey to understand which of the skills taught in I-SPARX youth found most useful and how they used these skills in their everyday lives.
Appendix.
| Individual Play |
Group Play |
Entire Sample |
||||
|---|---|---|---|---|---|---|
| n | %n | n | %n | N | %N | |
| Registered Participants | 56 | 65 | 121 | |||
| Completed All Levels & Surveys | 35 | 62.50% | 45 | 69.23% | 80 | 66.12% |
| Play Now Completions | 26 | 74.29% | 45 | 100% | 71 | 88.89% |
| Play Later Completions | 9 | 25.71% | 0 | 0.00% | 9 | 11.11% |
| Incomplete Participation | 21 | 37.50% | 20 | 30.77% | 41 | 33.88% |
| Self-identified Gender | ||||||
| Female | 28 | 50.00% | 40 | 61.54% | 68 | 56.20% |
| Male | 24 | 42.86% | 24 | 36.92% | 48 | 39.67% |
| Transgender Male | 2 | 3.57% | 0 | 0.00% | 2 | 1.65% |
| Missing | 2 | 3.57% | 1 | 1.54% | 3 | 2.48% |
| Age of Participant | ||||||
| 12 or younger | 1 | 1.79% | 0 | 0.00% | 1 | 0.83% |
| 13 | 5 | 8.93% | 2 | 3.08% | 7 | 5.79% |
| 14 | 3 | 5.36% | 5 | 7.69% | 8 | 6.61% |
| 15 | 2 | 3.57% | 4 | 6.15% | 6 | 4.96% |
| 16 | 3 | 5.36% | 29 | 44.62% | 32 | 26.45% |
| 17 | 4 | 7.14% | 16 | 24.62% | 20 | 16.53% |
| 18 | 4 | 7.14% | 1 | 1.54% | 5 | 4.13% |
| 19 | 3 | 5.36% | 4 | 6.15% | 7 | 5.79% |
| 20 | 8 | 14.29% | 3 | 4.62% | 11 | 9.09% |
| 21 | 9 | 16.07% | 0 | 0.00% | 9 | 7.44% |
| 22 | 5 | 8.93% | 1 | 1.54% | 6 | 4.96% |
| 23 | 1 | 1.79% | 0 | 0.00% | 1 | 0.83% |
| 24 or older | 6 | 10.71% | 0 | 0.00% | 6 | 4.96% |
| Missing | 2 | 3.57% | 0 | 0.00% | 2 | 1.65% |
| Community of Residence | ||||||
| Ikpiarjuk (Arctic Bay) | 5 | 8.93% | 0 | 0.00% | 5 | 4.13% |
| Qamani’tuaq (Baker Lake) | 1 | 1.79% | 0 | 0.00% | 1 | 0.83% |
| Iqaluktuuttiaq (Cambridge Bay) | 3 | 5.36% | 10 | 15.38% | 13 | 10.74% |
| Uqsuqtuuq (Gjoa Haven) | 2 | 3.57% | 9 | 13.85% | 11 | 9.09% |
| Sanirajak (Hall Beach) | 9 | 16.07% | 0 | 0.00% | 9 | 7.44% |
| Igloolik | 8 | 14.29% | 0 | 0.00% | 8 | 6.61% |
| Iqaluit | 11 | 19.64% | 0 | 0.00% | 11 | 9.09% |
| Kugaaruk (Arviligjuaq) | 0 | 0.00% | 15 | 23.08% | 15 | 12.40% |
| Kugluktuk | 0 | 0.00% | 13 | 20.00% | 13 | 10.74% |
| Naujaat (Repulse Bay) | 2 | 3.57% | 0 | 0.00% | 2 | 1.65% |
| Mittimatalik (Pond Inlet) | 8 | 14.29% | 0 | 0.00% | 8 | 6.61% |
| Kangiqtiniq (Rankin Inlet) | 3 | 5.36% | 0 | 0.00% | 3 | 2.48% |
| Taloyoak | 3 | 5.36% | 14 | 21.54% | 17 | 14.05% |
| Tikirarjuaq (Whale Cove) | 1 | 1.79% | 0 | 0.00% | 1 | 0.83% |
| Ottawa (originally from NU) | 0 | 0.00% | 4 | 6.15% | 4 | 3.31% |
| Receiving Mental Health Treatment | ||||||
| No | 48 | 85.71% | 57 | 87.69% | 105 | 86.78% |
| Yes (Medication) | 4 | 7.14% | 5 | 7.69% | 9 | 7.44% |
| Yes (Non-Medication) | 2 | 3.57% | 2 | 3.08% | 4 | 3.31% |
| Missing | 2 | 3.57% | 1 | 1.54% | 3 | 2.48% |
| Previous experience with I-SPARX? | ||||||
| Yes | 0 | 0.00% | 3 | 4.62% | 3 | 2.48% |
| No | 54 | 96.43% | 52 | 80.00% | 106 | 87.60% |
| Missing | 2 | 3.57% | 10 | 15.38% | 12 | 9.92% |
Appendix.
Figure G1.
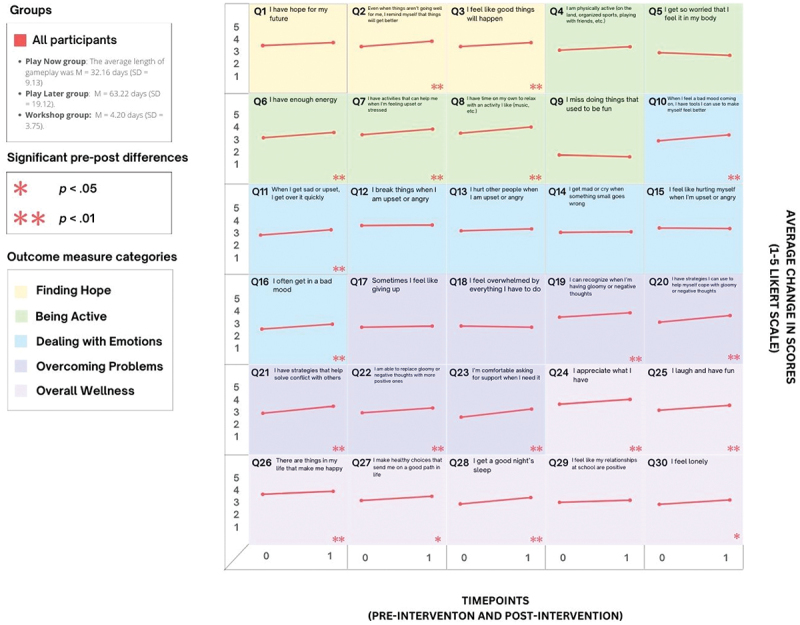
Lattice plot showing changes in scores on each item of the outcome measure from pre- to post-gameplay at α = .05.
Figure G2.
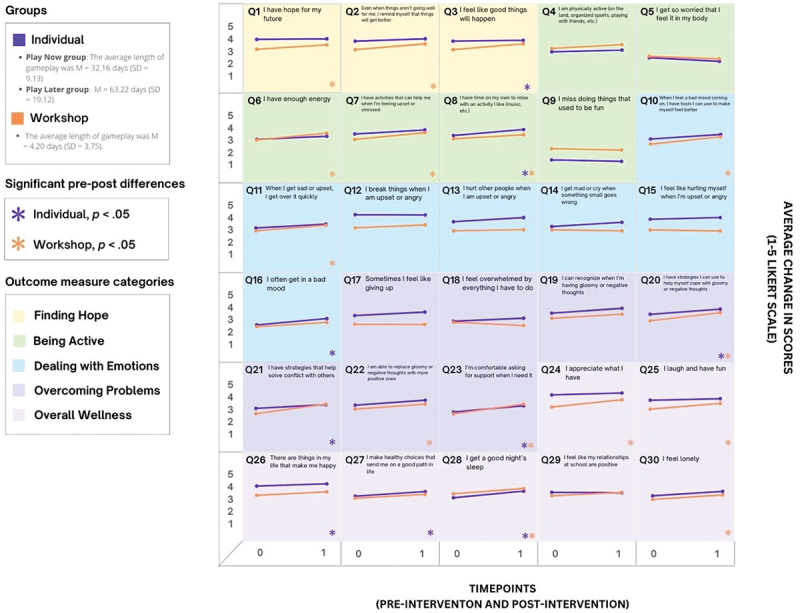
Lattice plot showing changes in scores on each item of the outcome measure from pre- to post- gameplay at α = .05 for the workshop and individual gameplay groups to assess differences in improvement between the groups from pre- to post- gameplay.
Appendix.
Figure H1.
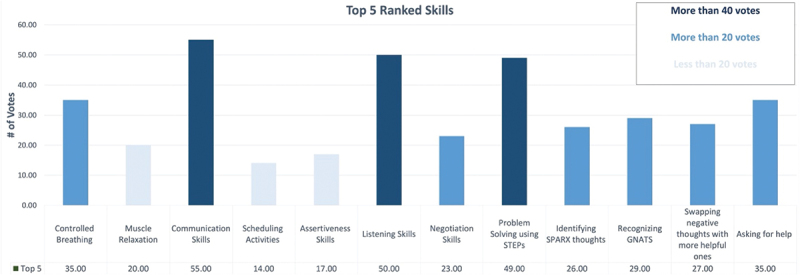
In the post-play survey, participants were asked to rank which of the 12 core CBT skills taught throughout I-SPARX they found most helpful in their everyday lives.
Funding Statement
The project team thanks the Canadian Institutes of Health Research for awarding Project Grant [#152865].
Disclosure statement
No potential conflict of interest was reported by the author(s).
Authors’ note
We are dedicated to accountability to the Inuit communities we serve and collaborate with and believe that it is important to acknowledge that our research team is diverse and consists of Indigenous and non-Indigenous team members. Authors C.S., R.Q. and I.O. are Inuit; author J.B. is part of the Kenhte:ke Kanien’kehaka First Nation of the Mohawks of the Bay of Quinte; author M.S. is Māori; author M.O identifies as Indigenous; principal investigator, Y.B., along with the majority of the research team (J.H., A.T., M.A., H.M., N.G., Y.S., C.D., M.L., S.M., M.B., F.A., S.S., and J.W.) are settlers who strive to be allies. We have endeavoured to conduct the project that is described here in a manner that embodies a decolonising approach to research, and we are continuously engaged in an imperfect learning process. We strive to conform to the guidelines set out by Inuit Tapiriit Kanatami and the Nunavut Research Institute to honour our commitment to Nunavummiut youth and their communities. Likewise, as pertains to SPARX, the Treaty of Waitangi signed in 1840 informed the importance of working with indigenous Māori in Aotearoa/New Zealand.
References
- [1].Anang P, Naujaat Elder EH, Gordon E, et al. Building on strengths in Naujaat: the process of engaging Inuit youth in suicide prevention. Int J Circumpolar Health. 2019;78(2):1508321. doi: 10.1080/22423982.2018.1508321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Inuit Tapiriit Kanatami [ITK] . Promising practices in suicide prevention across Inuit Nunangat; 2019. Available from: https://www.itk.ca/wp-content/uploads/2019/07/20190611-NISPS-ScanOfPromisingPractices-FINAL-EN.pdf
- [3].Kral MJ, Wiebe PK, Nisbet K, et al. Canadian Inuit community engagement in suicide prevention. Int J Circumpolar Health. 2009;68(3):292–33. doi: 10.3402/ijch.v68i3.18330 [DOI] [PubMed] [Google Scholar]
- [4].Kral MJ. “The weight on our shoulders is too much, and we are falling”: suicide among Inuit male youth in Nunavut, Canada. Med Anthropol Q. 2013;27(1):63–83. doi: 10.1111/maq.12016 [DOI] [PubMed] [Google Scholar]
- [5].Kumar MB, Tjepkema M. Suicide among first nations people, métis and Inuit (2011-2016): findings from the 2011 Canadian census health and environment cohort (CanCHEC). Statistics Canada; 2019. June 28. Available from: https://www150.statcan.gc.ca/n1/pub/99-011-x/99-011-x2019001-eng.htm [Google Scholar]
- [6].Inuit Tapiriit Kanatami [ITK] . National Inuit Suicide Prevention Strategy; 2016. Available from: https://www.itk.ca/wp-content/uploads/2016/07/ITK-National-Inuit-Suicide-Prevention-Strategy-2016.pdf
- [7].Inuit Tapiriit Kanatami [ITK] . National Inuit Strategy on Research; 2018. Available from: https://www.itk.ca/national-strategy-on-research-launched/
- [8].Abela JRZ, Hankin BL. Cognitive vulnerability to depression in children and adolescents. A developmental psychopathology perspective. In: Abela JRZ, and Hankin BL, editors. Handbook of depression in children and adolescents. New York: The Guilford Press; 2008. p. 35–78. [Google Scholar]
- [9].Beck AT, Shaw BF. Cognitive approaches to depression. In: Handbook of rational emotive theory and practice. New York (NY): Springer; 1977. p. 119–134. [Google Scholar]
- [10].Garnefski N, Kraaij V. Relationships between cognitive emotion regulation strategies and depression: a comparative study of five specific samples. Pers Individ Dif. 2006;40(8):1659–1669. doi: 10.1016/j.paid.2005.12.009 [DOI] [Google Scholar]
- [11].Chachamovich E, Kirmayer LJ, Haggarty JM, et al. Suicide among Inuit: results from a large, epidemiologically representative follow-back study in Nunavut. Can J Psychiatry. 2015;60(6):268–275. doi: 10.1177/070674371506000605 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Egeni CC. Suicide–Eminaq: ethnic case study, theories, application and solutions: socioeconomic and environmental effects on public behavior: the case of Inuit suicide. UK: AuthorHouse; 2011. [Google Scholar]
- [13].Brooker AL. Counselling within Inuit systems in Canada’s north. Can J Counselling Psychother. 2018;52(1):1–15. Available from: https://cjc-rcc.ucalgary.ca/article/view/61182/pdf [Google Scholar]
- [14].Elias B, Mignone J, Hall M, et al. Trauma and suicide behaviour histories among a Canadian indigenous population: an empirical exploration of the potential role of Canada’s residential school system. Soc Sci Med. 2012;74(10):1560–1569. doi: 10.1016/j.socscimed.2012.01.026 [DOI] [PubMed] [Google Scholar]
- [15].Morris M, Crooks C. Structural and cultural factors in suicide prevention: the contrast between mainstream and Inuit approaches to understanding and preventing suicide. J Soc Work Pract. 2015;29(3):321–338. doi: 10.1080/02650533.2015.1050655 [DOI] [Google Scholar]
- [16].Akande VO, Fawehinmi TO, Ruiter RAC, et al. Healthy dietary choices and physical activity participation in the Canadian Arctic: understanding Nunavut Inuit perspectives on the barriers and enablers. Int J Environ Res Public Health. 2021;18(3):940. doi: 10.3390/ijerph18030940 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Muckle G, Laflamme D, Gagnon J, et al. Alcohol, smoking, and drug use among Inuit women of childbearing age during pregnancy and the risk to children. Alcohol Clin Exp Res. 2011;35(6):1081–1091. doi: 10.1111/j.1530-0277.2011.01441.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Roshanafshar S, Hawkins E. Health at a glance: food insecurity in Canada. Catalogue no.82-624-X. 2015. Available from: https://foodsecurecanada.org/sites/foodsecurecanada.org/files/foodinsecurityincanada-march2015.pdf
- [19].Statistics Canada . Inuit: fact sheet for Nunavut. Statistics Canada catalogue No. 89-656-X2016017. Ottawa (ON); 2016. Available from: https://www150.statcan.gc.ca/n1/en/pub/89-656-x/89-656-x2016017-eng.pdf?st=W2WVMI2I [Google Scholar]
- [20].Bradette-Laplante M, Courtemanche Y, Desrochers-Couture M, et al. Food insecurity and psychological distress in Inuit adolescents of Nunavik. Public Health Nutr. 2020;23(14):2615–2625. doi: 10.1017/S1368980020000117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Gray AP, Richer F, Harper S. Individual- and community-level determinants of Inuit youth mental wellness. Can J Public Health. 2016;107(3):e251–e257. doi: 10.17269/cjph.107.5342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Tester FJ. Iglutaq (in my room): the implications of homelessness for Inuit. A case study of housing and homelessness in Kinngait, Nunavut territory. Kinngait: The Harvest Society; 2006. Available from: https://www.tunngavik.com/documents/publications/2006-04-00-Iglutaq-The-Implications-of-Homelessness-for-Inuit.pdf [Google Scholar]
- [23].Mariu KR, Merry SN, Robinson EM, et al. Seeking professional help for mental health problems, among New Zealand secondary school students. Clin Child Psychol Psychiatry. 2012;17(2):284–297. doi: 10.1177/1359104511404176 [DOI] [PubMed] [Google Scholar]
- [24].Rickwood D, Deane FP, Wilson CJ, et al. Young people’s help-seeking for mental health problems. Aust E-J Advancem Ment Health, 4(3). 2005;4(3):218–251. doi: 10.5172/jamh.4.3.218 [DOI] [Google Scholar]
- [25].Bennett N, Lemelin R, Ellis S. Indigenous and local perspectives on the community benefits of conservation: a case study of a proposed Canadian national park and the lutsel K’e dene first nation. Geogr Res Forum. 2010;30:105–134. Available from: http://hdl.handle.net/1828/4466 [Google Scholar]
- [26].Litwin L, Hankey J, Lucassen M, et al. Reflections on SPARX, a self-administered e-intervention for depression, for Inuit youth in Nunavut. J Rural Ment Health. 2023;47(1):41–50. doi: 10.1037/rmh0000218 [DOI] [Google Scholar]
- [27].Bohr Y, Litwin L, Hankey JR, et al. Evaluating the utility of a psychoeducational serious game (SPARX) in protecting Inuit youth from depression: Pilot randomized controlled trial. JMIR Serious Games. 2023;11(1):e38493. doi: 10.2196/38493 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Lindsay T, Healey GK. Perspectives of families working with Nunavut’s foster care system. Iqaluit (NU): Quajigiartiit Health Research Centre; 2012. [Google Scholar]
- [29].Milligan C, Mantle R, Blake G, et al. Health system learning with indigenous communities: a study protocol for a two-eyed seeing review and multiple case study. Health Res Policy Syst. 2022;20(1):65. doi: 10.1186/s12961-022-00873-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Kirmayer LJ, Dandeneau S, Marshall E, et al. Rethinking resilience from indigenous perspectives. Can J Psychiatry. 2011;56(2):84–91. doi: 10.1177/070674371105600203 [DOI] [PubMed] [Google Scholar]
- [31].Korhonen M. Resilience: overcoming challenges and moving on positively. National Aboriginal Health Organization; 2007. Available from: https://ruor.uottawa.ca/bitstream/10393/30325/1/2007_Inuit_Resilience_Book.pdf [Google Scholar]
- [32].Ungar M. Resilience, trauma, context, and culture. Trauma, Violence Abuse. 2013;14(3):255–266. doi: 10.1177/1524838013487805 [DOI] [PubMed] [Google Scholar]
- [33].Healey GK, Noah J, Mearns C. The eight ujarait (rocks) model: supporting Inuit adolescent mental health with an intervention model based on Inuit ways of knowing. Int J Indigenous Health. 2016;11(1):92–110. doi: 10.18357/ijih111201614394 [DOI] [Google Scholar]
- [34].Petrasek MacDonald J, Cunsolo Willox A, Ford JD et al, Protective factors for mental health and well-being in a changing climate: perspectives from Inuit youth in Nunatsiavut, Labrador. Soc Sci Med. 2015;141:133–141. doi: 10.1016/j.socscimed.2015.07.017 [DOI] [PubMed] [Google Scholar]
- [35].Kral MJ, Salusky I, Inuksuk P, et al. Tunngajuq: stress and resilience among Inuit youth in Nunavut, Canada. Transcult Psychiatry. 2014;51(5):673–692. doi: 10.1177/1363461514533001 [DOI] [PubMed] [Google Scholar]
- [36].Healey Akearok G, Cueva K, Stoor JPA, et al. Exploring the term “resilience” in Arctic Health and well-being using a sharing circle as a community-centered approach: insights from a conference workshop. Soc Sci. 2019;8(2):45. doi: 10.3390/socsci8020045 [DOI] [Google Scholar]
- [37].Institute of Aboriginal Peoples’ Health . CIHR institute of aboriginal peoples’ health strategic plan 2014-18: wellness, strength and resilience of first nations, Inuit and métis peoples: moving beyond health equity. Canadian institutes of health research. 2015. Avauilable from: https://publications.gc.ca/collections/collection_2016/irsc-cihr/MR4-41-2015-eng.pdf
- [38].Bartlett C, Marshall M, Marshall A. Two-eyed seeing and other lessons learned within a co-learning journey of bringing together indigenous and mainstream knowledges and ways of knowing. J Environ Stud Sci. 2012;2(4):331–340. doi: 10.1007/s13412-012-0086-8 [DOI] [Google Scholar]
- [39].Roher SI, Yu Z, Martin DH, et al. How is Etuaptmumk/Two-eyed seeing characterized in indigenous health research? A scoping review. PLOS ONE. 2021;16(7):e0254612. doi: 10.1371/journal.pone.0254612 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].McKivett A, Hudson JN, McDermott D, et al. Two‐eyed seeing: a useful gaze in indigenous medical education research. Med Educ. 2020;54(3):217–224. doi: 10.1111/medu.14026 [DOI] [PubMed] [Google Scholar]
- [41].Peltier C. An application of two-eyed seeing: indigenous research methods with participatory action research. Int J Qual Methods. 2018;17(1):1609406918812346. doi: 10.1177/1609406918812346 [DOI] [Google Scholar]
- [42].National Aboriginal Health Organization [NAHO] . Midwifery and aboriginal midwifery in Canada. 2004. Available from: http://archives.algomau.ca/main/sites/default/files/2012-25_003_006.pdf
- [43].National Aboriginal Health Organization [NAHO] . Ikajurniq–basic counselling skills: Inuit voices, modern methods. 2009. Available from: http://archives.algomau.ca/main/sites/default/files/2012-25_001_027.pdf
- [44].Karetak J, Tester F, Tagalik S. Inuit qaujimajatuqangit: what Inuit have always known to be true. Halifax: Fernwood Publishing; 2017. [Google Scholar]
- [45].Broadhead LA, Howard S. Confronting the contradictions between Western and indigenous science: a critical perspective on two-eyed seeing. AlterNative: Int J Indigenous Peoples. 2021;17(1):111–119. doi: 10.1177/1177180121996326 [DOI] [Google Scholar]
- [46].Wright AL, Gabel C, Ballantyne M, et al. Using two-eyed seeing in research with indigenous people: an integrative review. Int J Qual Methods. 2019;18:1609406919869695. doi: 10.1177/1609406919869695 [DOI] [Google Scholar]
- [47].Government of Nunavut . Inuit societal values. Culture, language, heritage and art. n.d. Available from: https://www.gov.nu.ca/en/culture-language-heritage-and-art/inuit-societal-values
- [48].Pederson C, Otokiak M, Koonoo I, et al. ScIQ: an invitation and recommendations to combine science and Inuit qaujimajatuqangit for meaningful engagement of Inuit communities in research. Arct Sci. 2020;6(3):326–339. doi: 10.1139/as-2020-0015 [DOI] [Google Scholar]
- [49].Williamson LJ. Inuit gender parity and why it was not accepted in the Nunavut legislature. Études/Inuit/Studies. 2006;30(1):51–68. doi: 10.7202/016149ar [DOI] [Google Scholar]
- [50].Tagalik S. Inutsiaqpagutit – that which enables you to have a good life: supporting Inuit early life health. National Collaborating Centre for Aboriginal Health; 2010. Available from: https://www.nccih.ca/docs/health/FS-InutsiaqpagutitInuitHealth-Tagalik-EN.pdf [Google Scholar]
- [51].Thomas A, Bohr Y, Hankey J, et al. How did nunavummiut youth cope during the COVID-19 pandemic? A qualitative exploration of the resilience of Inuit youth leaders involved in the I-SPARX project. Int J Circumpolar Health. 2022;81(1):2043577. doi: 10.1080/22423982.2022.2043577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Butler AC, Chapman JE, Forman EM, et al. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev. 2006;26(1):17–31. doi: 10.1016/j.cpr.2005.07.003 [DOI] [PubMed] [Google Scholar]
- [53].Tolin DF. Is cognitive-behavioral therapy more effective than other therapies? A meta-analytic review. Clin Psychol Rev. 2010;30(6):710–720. doi: 10.1016/j.cpr.2010.05.003 [DOI] [PubMed] [Google Scholar]
- [54].Beck JS. Cognitive behavior therapy: basics and beyond. 2nd ed. New York (NY): Guilford Press; 2011. [Google Scholar]
- [55].Rupke SJ, Blecke D, Renfrow M. Cognitive therapy for depression. Am Fam Physician. 2006;73(1):83–86. [PubMed] [Google Scholar]
- [56].Lewinsohn PM, Clarke GN. Psychosocial treatments for adolescent depression. Clin Psychol Rev. 1999;19(3):329–342. doi: 10.1016/S0272-7358(98)00055-5 [DOI] [PubMed] [Google Scholar]
- [57].Huey SJ Jr, Park AL, Galán CA, et al. Culturally responsive cognitive behavioral therapy for ethnically diverse populations. Annu Rev Clin Psychol. 2023;19(1):51–78. doi: 10.1146/annurev-clinpsy-080921-072750 [DOI] [PubMed] [Google Scholar]
- [58].Shepherd M, Fleming T, Lucassen M, et al. The design and relevance of a computerized gamified depression therapy program for indigenous Māori adolescents. JMIR Serious Games. 2015;3(1):e3804. doi: 10.2196/games.3804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [59].Pina AA, Polo AJ, Huey SJ. Evidence-based psychosocial interventions for ethnic minority youth: the 10-year update. J Clin Child Adolesc Phychol. 2019;48(2):179–202. doi: 10.1080/15374416.2019.1567350 [DOI] [PubMed] [Google Scholar]
- [60].Inuit Tapiriit Kanatami [ITK] . The digital divide: broadband connectivity in Inuit Nunangat. 2021. Available from: https://www.itk.ca/wp-content/uploads/2021/08/ITK_Telecomms_English_08.pdf
- [61].Canadian Radio-television and Telecommunications Commission [CRTC] . Telecom regulatory policy CRTC 2016-496. 2016. Available from: https://crtc.gc.ca/eng/archive/2016/2016-496.pdf
- [62].Canadian Radio-television and Telecommunications Commission [CRTC] . Broadband fund: about the fund. 2023. Available from: https://crtc.gc.ca/eng/internet/fnds.htm
- [63].Canadian Radio-television and Telecommunications Commission [CRTC] . Telecom decision CRTC 2023-418. 2023. Available from: https://crtc.gc.ca/eng/archive/2023/2023-418.pdf
- [64].Canadian Radio-television and Telecommunications Commission [CRTC] . Telecom decision CRTC 2024-149. 2024. Available from: https://crtc.gc.ca/eng/archive/2024/2024-149.pdf
- [65].Rabouam C. Satellite dependency in Nunavut: a barrier to the territory’s political realization. 2023 Arctic Yearbook. 2023. p. 1–15. Available from: https://arcticyearbook.com/images/yearbook/2023/Scholarly_Papers/11_Rabouam_AY2023.pdf
- [66].Lochead D. In Nunavut, starlink stands up to cold but service, speeds vary, users say. Arctic Today. 2023. Jan 24. Available from: https://www.arctictoday.com/in-nunavut-starlink-stands-up-to-cold-but-service-speeds-vary-users-say/
- [67].Granic I, Lobel A, Engels RCME. The benefits of playing video games. Am Psychologist. 2014;69(1):66–78. doi: 10.1037/a0034857 [DOI] [PubMed] [Google Scholar]
- [68].Halldorsson B, Hill C, Waite P, et al. Annual research review: immersive virtual reality and digital applied gaming interventions for the treatment of mental health problems in children and young people: the need for rigorous treatment development and clinical evaluation. J Child Psychol Psychiatry. 2021;62(5):584–605. doi: 10.1111/jcpp.13400 [DOI] [PubMed] [Google Scholar]
- [69].Merry SN, Stasiak K, Shepherd M, et al. The effectiveness of SPARX, a computerised self help intervention for adolescents seeking help for depression: randomised controlled non-inferiority trial. BMJ. 2012;344(apr18 3):e2598–e2598. doi: 10.1136/bmj.e2598 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [70].Xie H. A scoping review of gamification for mental health in children: uncovering its key features and impact. Arch Psychiatr Nurs. 2022;41:132–143. doi: 10.1016/j.apnu.2022.07.003 [DOI] [PubMed] [Google Scholar]
- [71].Fleming TM, Bavin L, Stasiak K, et al. Serious games and gamification for mental health: current status and promising directions. Front Psychol. 2017;7:215. doi: 10.3389/fpsyt.2016.00215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].Freeman D, Reeve S, Robinson A, et al. Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol Med. 2017;47(14):2393–2400. doi: 10.1017/S003329171700040X [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Gentry SV, Gauthier A, L’Estrade Ehrstrom B, et al. Serious gaming and gamification education in health professions: systematic review. J Med Internet Res. 2019;21(3):e12994. doi: 10.2196/12994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [74].Fleming T, Poppelaars M, Thabrew H. The role of gamification in digital mental health. World Psychiatry. 2023;22(1):46. doi: 10.1002/wps.21041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Ferrari M, Sabetti J, McIlwaine SV, et al. Gaming my way to recovery: a systematic scoping review of digital game interventions for young people’s mental health treatment and promotion. Front Digit Health. 2022;4:814248. doi: 10.3389/fdgth.2022.814248 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [76].Cheek C, Bridgman H, Fleming T, et al. Views of young people in rural Australia on SPARX, a fantasy world developed for New Zealand youth with depression. JMIR Serious Games. 2014;2(1):e3183. doi: 10.2196/games.3183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [77].Oskalns M. A two-eyed seeing approach to evaluating an e-intervention for Inuit youth using Inuit qaujimajatuqangit [Unpublished masters thesis]. York University, Toronto; 2023. [Google Scholar]
- [78].Wabano MJ, Young NL. Aaniish Na Gegii? (the aboriginal children’s health and well-being measure - ACHWM). Sudbury, ON: Wikwemikong Health Centre, Laurentian University; 2012. [Google Scholar]
- [79].Padgett J, McCague H, Bohr Y, et al. Psychometric properties of a community-designed measure to assess wellbeing in Inuit youth: the I-SPARX wellness questionnaire [manuscript in preparation]. Department of Psychology, York University; Forthcoming. [Google Scholar]
- [80].Gelman A, Hill J. Data analysis using regression and multilevel/hierarchical models. Cambridge: Cambridge University Press; 2006. [Google Scholar]
- [81].Singer JD, Willett JB. Applied longitudinal data analysis: modeling change and event occurrence. New York: Oxford University Press; 2003. [Google Scholar]
- [82].Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Phychol. 2006;3(2):77–101. doi: 10.1191/1478088706qp063oa [DOI] [Google Scholar]
- [83].Dedoose . Software for managing, analyzing, and presenting qualitative and mixed methods research data (version 8.0.35) [computer software]. 2018. Available from: www.dedoose.com
- [84].Government of Canada . TCPS 2 (2022) - chapter 9: research involving the first nations, Inuit, and métis peoples of canada. 2023. Available from: https://ethics.gc.ca/eng/tcps2-eptc2_2022_chapter9-chapitre9.html
- [85].Kim J. Youth involvement in participatory action research (PAR): challenges and barriers. Crit Soc Work. 2016;17(1). doi: 10.22329/csw.v17i1.5891 [DOI] [Google Scholar]
- [86].Kral MJ. The return of the sun: suicide and reclamation among Inuit of Arctic Canada. New York: Oxford University Press; 2019. [Google Scholar]
- [87].Ljubicic GJ, Mearns R, Okpakok S, et al. Nunami iliharniq (learning from the land): reflecting on relational accountability in land-based learning and cross-cultural research in Uqšuqtuuq (Gjoa Haven, Nunavut). Arct Sci. 2021;8(1):252–291. doi: 10.1139/as-2020-0059 [DOI] [Google Scholar]
- [88].Sadowsky H, Brunet ND, Anaviapik A, et al. Inuit youth and environmental research: exploring engagement barriers, strategies, and impacts. Facets. 2022;7(1):45–70. doi: 10.1139/facets-2021-0035 [DOI] [Google Scholar]
- [89].Aust F, Diedenhofen B, Ullrich S, et al. Seriousness checks are useful to improve data validity in online research. Behav Res Methods. 2013;45(2):527–535. doi: 10.3758/s13428-012-0265-2 [DOI] [PubMed] [Google Scholar]
- [90].Buchanan EM, Scofield JE. Methods to detect low quality data and its implication for psychological research. Behav Res Methods. 2018;50(6):2586–2596. doi: 10.3758/s13428-018-1035-6 [DOI] [PubMed] [Google Scholar]
- [91].Ihme JM, Lemke F, Lieder K, et al. Comparison of ability tests administered online and in the laboratory. Behav Res Methods. 2009;41(4):1183–1189. doi: 10.3758/BRM.41.4.1183 [DOI] [PubMed] [Google Scholar]
- [92].Greszki R, Meyer M, Schoen H. Exploring the effects of removing “too fast” responses and respondents from web surveys. Public Opin Q. 2015;79(2):471–503. doi: 10.1093/poq/nfu058 [DOI] [Google Scholar]
- [93].Abdelmaseh M, Bohr Y, Muir N. Is playing Inuit-sparx helpful? Examining the usefulness and cultural appropriateness of a cbt-based serious game. 2024. [Forthcoming].
- [94].Anderssen E. Mental health-boosting video game Sparx aims to help indigenous youth. The globe and mail. 2019. Apr 24. Available from: https://www.theglobeandmail.com/canada/article-mental-health-boosting-video-game-sparx-aims-to-help-indigenous-youth/
- [95].Tindall L, Mikocka‐Walus A, McMillan D, et al. Is behavioural activation effective in the treatment of depression in young people? A systematic review and meta‐analysis. Psychol Psychother: Theory, Res Pract. 2017;90(4):770–796. doi: 10.1111/papt.12121 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Stanley B, Brown G, Brent DA, et al. Cognitive-behavioral therapy for suicide prevention (CBT-SP): treatment model, feasibility, and acceptability. J Am Acad Child Adolesc Psychiatry. 2009;48(10):1005–1013. doi: 10.1097/CHI.0b013e3181b5dbfe [DOI] [PMC free article] [PubMed] [Google Scholar]
- [97].Rolston A, Lloyd-Richardson E. What is emotion regulation and how do we do it?. New York: Cornell Research Program on Self-Injury and Recovery, Cornell University; 2020. [Google Scholar]
- [98].Hatkevich C, Penner F, Sharp C. Difficulties in emotion regulation and suicide ideation and attempt in adolescent inpatients. Psychiatry Res. 2019;271:230–238. doi: 10.1016/j.psychres.2018.11.038 [DOI] [PubMed] [Google Scholar]
- [99].Beck AT. Cognitive therapy of depression. New York: Guilford Press; 1979. [Google Scholar]
- [100].McIntosh CN, Fischer DG. Beck’s cognitive triad: one versus three factors. Can J Behavioural Sci/Revue Canadienne des Sci du Comportement. 2000;32(3):153–157. doi: 10.1037/h0087110 [DOI] [Google Scholar]
- [101].Breitborde NJ, Wastler H, Pine JG, et al. Suicidality and social problem solving skills among individuals with first‐episode psychosis participating in coordinated specialty care. Early Interv Psychiatry. 2021;15(3):497–504. doi: 10.1111/eip.12967 [DOI] [PubMed] [Google Scholar]
- [102].Wingate LR, Van Orden KA, Joiner TE Jr., et al. Comparison of compensation and capitalization models when treating suicidality in young adults. J Consult Clin Psychol. 2005;73(4):756–762. doi: 10.1037/0022-006X.73.4.756 [DOI] [PubMed] [Google Scholar]
- [103].Reinecke MA, DuBois DL, Schultz TM. Social problem solving, mood, and suicidality among inpatient adolescents. Cognit Ther Res. 2001;25(6):743–756. doi: 10.1023/A:1012971423547 [DOI] [Google Scholar]
- [104].Zeyrek EY, Gençöz F, Bergman Y, et al. Suicidality, problem-solving skills, attachment style, and hopelessness in Turkish students. Death Stud. 2009;33(9):815–827. doi: 10.1080/07481180903142407 [DOI] [PubMed] [Google Scholar]
- [105].Gulliver A, Griffiths K, Christensen H. Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. Biomed Central Psychiatry. 2010;10(1):113. doi: 10.1186/1471-244X-10-113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [106].Rickwood DJ, Deane FP, Wilson CJ. When and how do young people seek professional help for mental health problems? Med J Aust. 2007;187(7):35–39. doi: 10.5694/j.1326-5377.2007.tb01334.x [DOI] [PubMed] [Google Scholar]
- [107].Robertson A, Mason ECM, Placeres V, et al. Investigating a deep breathing intervention to promote mental health in P‐12 schools. Psychol Schools. 2023;60(8):3056–3072. doi: 10.1002/pits.22908 [DOI] [Google Scholar]
- [108].Aktaş GK, İlgin VE. The effect of deep breathing exercise and 4–7-8 breathing techniques applied to patients after bariatric surgery on anxiety and quality of life. Obes Surg. 2023;33(3):920–929. doi: 10.1007/s11695-022-06405-1 [DOI] [PubMed] [Google Scholar]
- [109].Fincham GW, Strauss C, Montero-Marin J, et al. Effect of breathwork on stress and mental health: a meta-analysis of randomised-controlled trials. Sci Rep. 2023;13(1):432. doi: 10.1038/s41598-022-27247-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- [110].Nyer M, Gerbarg PL, Silveri MM, et al. A randomized controlled dosing study of Iyengar yoga and coherent breathing for the treatment of major depressive disorder: impact on suicidal ideation and safety findings. Complement Ther Med. 2018;37:136–142. doi: 10.1016/j.ctim.2018.02.006 [DOI] [PubMed] [Google Scholar]
- [111].Ermine W. First Nations education in Canada: the circle unfolds. Vancouver: UBC Press; 1995. p. 101–112. [Google Scholar]
- [112].Fonda M. On the origins and spread of pan-Indian spirituality in Canada. Stud Religion/Sci Religieuses. 2016;45(3):309–334. doi: 10.1177/0008429816657741 [DOI] [Google Scholar]
- [113].Dudgeon P, Kelly K. Contextual factors for research on psychological therapies for Aboriginal australians. Aust Psychol. 2014;49(1):8–13. doi: 10.1111/ap.12030 [DOI] [Google Scholar]
- [114].Bennett ST, Babbage DR. Cultural adaptation of CBT for aboriginal australians. Aust Psychol. 2014;49(1):19–21. doi: 10.1111/ap.12029 [DOI] [Google Scholar]
- [115].Nelson J, Ryan K, Rotumah D, et al. Aboriginal practitioners offer culturally safe and responsive CBT: response to commentaries. Aust Psychol. 2014;49(1):22–27. doi: 10.1111/ap.12041 [DOI] [Google Scholar]
- [116].Bennett‐Levy J, Wilson S, Nelson J, et al. Can CBT be effective for Aboriginal Australians? Perspectives of Aboriginal practitioners trained in CBT. Aust Psychol. 2014;49(1):1–7. doi: 10.1111/ap.12025 [DOI] [Google Scholar]
- [117].Ishikawa SI, Kikuta K, Sakai M, et al. A randomized controlled trial of a bidirectional cultural adaptation of cognitive behavior therapy for children and adolescents with anxiety disorders. Behav Res Ther. 2019;120:103432. doi: 10.1016/j.brat.2019.103432 [DOI] [PubMed] [Google Scholar]
- [118].Farrand P, Mullan E, Rayson K, et al. Adapting CBT to treat depression in armed forces veterans: qualitative study. Behav Cogn Psychother. 2019;47(5):530–540. doi: 10.1017/S1352465819000171 [DOI] [PubMed] [Google Scholar]
- [119].Kowatch KR, Schmidt F, Mushquash CJ. Review of culturally-adapted cognitive behavioral therapy interventions for North American indigenous children and youth. J Concurrent Disord. 2019;1(3):5. doi: 10.54127/LDMQ1890 [DOI] [Google Scholar]
- [120].Jalal B, Kruger Q, Hinton D. Culturally adapted CBT (CA-CBT) for traumatised indigenous South Africans (Sepedi): a randomised pilot trial comparing CA-CBT to applied muscle relaxation. Intervention. 2020;18(1):61–65. doi: 10.4103/INTV.INTV_68_18 [DOI] [Google Scholar]
- [121].Naeem F, Waheed W, Gobbi M, et al. Preliminary evaluation of culturally sensitive CBT for depression in Pakistan: findings from developing culturally sensitive CBT project (DCCP). Behav Cogn Psychother. 2011;39(2):165–173. doi: 10.1017/S1352465810000822 [DOI] [PubMed] [Google Scholar]
- [122].Hays P. An international perspective on the adaptation of CBT across cultures. Aust Psychol. 2014;49(1):17–18. doi: 10.1111/ap.12027 [DOI] [Google Scholar]
- [123].Christ C, Schouten MJ, Blankers M, et al. Internet and computer-based cognitive behavioral therapy for anxiety and depression in adolescents and young adults: systematic review and meta-analysis. J Med Internet Res. 2020;22(9):e17831. doi: 10.2196/17831 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [124].Do R, Lee S, Kim JS, et al. Effectiveness and dissemination of computer-based cognitive behavioral therapy for depressed adolescents: effective and accessible to whom? J Affect Disord. 2021;282:885–893. doi: 10.1016/j.jad.2020.12.177 [DOI] [PubMed] [Google Scholar]
- [125].Boydell KM, Hodgins M, Pignatiello A, et al. Using technology to deliver mental health services to children and youth: a scoping review. J Can Acad Child Adolesc Psychiatry. 2014;23(2):87. [PMC free article] [PubMed] [Google Scholar]
- [126].Lucassen M, Samra R, Iacovides I, et al. How LGBT+ young people use the internet in relation to their mental health and envisage the use of e-therapy: exploratory study. JMIR Serious Games. 2018;6(4):e11249. doi: 10.2196/11249 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [127].Myers K, Cummings JR, Zima B, et al. Advances in asynchronous telehealth technologies to improve access and quality of mental health care for children and adolescents. J Technol Behavioral Sci. 2018;3(2):87–106. doi: 10.1007/s41347-018-0055-5 [DOI] [Google Scholar]
- [128].Vallury KD, Jones M, Oosterbroek C. Computerized cognitive behavior therapy for anxiety and depression in rural areas: a systematic review. J Med Internet Res. 2015;17(6):e139. doi: 10.2196/jmir.4145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [129].Lucassen MF, Merry SN, Hatcher S, et al. Rainbow SPARX: a novel approach to addressing depression in sexual minority youth. Cognit Behavioral Pract. 2015;22(2):203–216. doi: 10.1016/j.cbpra.2013.12.008 [DOI] [Google Scholar]
- [130].Thabrew H, Stasiak K, Garcia‐Hoyos V, et al. Game for health: how eHealth approaches might address the psychological needs of children and young people with long‐term physical conditions. J Paediatr Child Health. 2016;52(11):1012–1018. doi: 10.1111/jpc.13271 [DOI] [PubMed] [Google Scholar]
- [131].Pickren WE, Taşçı G. Indigenous psychologies: resources for future histories. In: McCallum D, editor. The Palgrave handbook of the history of human sciences. Singapore: Palgrave Macmillan; 2022. doi: 10.1007/978-981-15-4106-3_80-3 [DOI] [Google Scholar]
- [132].Forbes A, Ritchie S, Walker J, et al. Applications of two-eyed seeing in primary research focused on indigenous health: a scoping review. Int J Qual Methods. 2020;19:1609406920929110. doi: 10.1177/1609406920929110 [DOI] [Google Scholar]
- [133].MacGill V. Reframing cognitive behaviour theory from a systems perspective. Systemic Pract Action Res. 2018;31(5):495–507. doi: 10.1007/s11213-017-9440-9 [DOI] [Google Scholar]
- [134].Bornstein MH, Kotler JA, Lansford JE. The future of parenting programs: an introduction. Parent: Sci Pract. 2022;22(3):189–200. doi: 10.1080/15295192.2022.2086808 [DOI] [PMC free article] [PubMed] [Google Scholar]