

Abstract
Background
Digital mental health interventions (DMHIs) are capable of closing gaps in the prevention and therapy of common mental disorders. Despite their proven effectiveness and approval for prescription, use rates remain low. The reasons include a lack of familiarity and knowledge as well as lasting concerns. Medical students were shown to have a comparatively higher risk for common mental disorders and are thus an important target group for raising awareness about DMHIs. At best, knowledge is already imparted during medical school using context-sensitive information strategies. Yet, little is known about medical students’ information preferences regarding DMHIs.
Objective
This study aims to explore information preferences for DMHIs for personal use among medical students in Germany.
Methods
A discrete choice experiment was conducted, which was developed using an exploratory sequential mixed methods research approach. In total, 5 attributes (ie, source, delivery mode, timing, recommendation, and quality criteria), each with 3 to 4 levels, were identified using formative research. Data were analyzed using logistic regression models to estimate preference weights and the relative importance of attributes. To identify subgroups of students varying in information preferences, we additionally performed a latent class analysis.
Results
Of 309 participants, 231 (74.8%) with reliable data were included in the main analysis (women: 217/309, 70.2%; age: mean 24.1, SD 4.0 y). Overall, the conditional logit model revealed that medical students preferred to receive information about DMHIs from the student council and favored being informed via social media early (ie, during their preclinic phase or their freshman week). Recommendations from other students or health professionals were preferred over recommendations from other users or no recommendations at all. Information about the scientific evidence base was the preferred quality criterion. Overall, the timing of information was the most relevant attribute (32.6%). Latent class analysis revealed 2 distinct subgroups. Class 1 preferred to receive extensive information about DMHIs in a seminar, while class 2 wanted to be informed digitally (via email or social media) and as early as possible in their studies.
Conclusions
Medical students reported specific needs and preferences regarding DMHI information provided in medical school. Overall, the timing of information (early in medical education) was considered more important than the information source or delivery mode, which should be prioritized by decision makers (eg, members of faculties of medicine, universities, and ministries of education). Study findings suggest general and subgroup-specific information strategies, which could be implemented in a stepped approach. Easily accessible digital information may promote students’ interest in DMHIs in the first step that might lead to further information-seeking behavior and the attendance of seminars about DMHIs in the second step.
Keywords: preferences, digital mental health, medical students, innovation diffusion, technology acceptance, health information
Introduction
Background
Despite the considerable burden attributable to common mental disorders (CMDs), numerous structural obstacles to the use of (face-to-face) psychological interventions, such as waiting times, remain [1]. In addition, individual-level barriers, such as skepticism about helpfulness and safety, self-stigma, or simply a lack of awareness of appropriate services, are well documented [2,3]. Given the need for lowering the threshold to access psychological interventions, digital mental health interventions (DMHIs) can play a key role [4]. They can be differentiated by their application field (eg, prevention vs therapy), technical modality (eg, app and virtual reality), guidance (varying in source, timing, and intensity; eg, via videoconference) or application area (eg, stand-alone vs blended care), and theory base (eg, cognitive behavioral therapy) [5,6]. With the Digital Healthcare Act, German health policy created new regulations for the certification and reimbursement of costs for prevention and health care contexts. Since October 2020, physicians and psychotherapists are allowed to prescribe specific certified medical smartphone apps and browser-based applications (German: Digitale Gesundheitsanwendungen [DiGA]) listed in a repository by the Federal Institute for Drugs and Medical Devices (German: Bundesinstitut für Arzneimittel und Medizinprodukte [BfARM]), including digital therapeutics for different CMDs, on the expense of statutory health insurance companies [7,8]. Nevertheless, the general use of DMHIs across European countries in the past years [4] as well as the uptake of DMHIs in terms of DiGA in Germany in recent times is marginal and appears to be hampered by individual-level barriers, such as doubts and lack of knowledge, among health care professionals (HCPs) and patients [9,10]. In addition, the diffusion process is also affected by health policy barriers, such as adverse regulations and increasing barriers to market entry for potential DiGA providers [11]. The distinction between permanent and temporary listing of DiGA has also been criticized, especially by statutory health insurance companies. Although most DiGA in the field of DMHIs are permanently listed based on their scientific evidence base, the so-called fast-track certification of DiGA has raised concerns about the scientific foundation of temporarily listed DiGA. This means that manufacturers that meet the criteria by the BfArM, except for a high-quality randomized controlled trial during the proposal, can get a listing for their DiGA if the concept is likely to succeed. However, it should be considered that manufacturers have an immense financial risk if they fail to prove the positive care effects with rigorously conducted randomized controlled trials within 1 year or if their DiGA price will be upgraded after the test phase. In addition, no DiGA gets a listing by the BfARM, even not provisionally, if no sufficient data for its efficacy from pilot studies was available or data security standards were not met [8]. However, long-term effects and adherence among various patient groups should be monitored, given that the DiGA concept is rather novel. Particularly, the outbreak of the COVID-19 pandemic and the accompanying need to quickly switch to contactless health care made it clear that lacking acquaintance with DMHIs is a key barrier to their implementation in health care [12]. Therefore, the development of user-centered, context-sensitive information strategies for relevant target groups represents a crucial step during the slow innovation diffusion process [13].
When analyzing preferences regarding information strategies on DMHIs, medical students represent a special population of interest not only because they potentially prescribe DMHIs in their role as future physicians but also belong to a group considered vulnerable in terms of a high prevalence of CMDs and often exhibit poor help-seeking behavior when in need [14-16]. Fear of stigmatization in medical school and expected career disadvantages, if mental health issues are disclosed, appear to be widespread reasons for not seeking support [17].
To inform patients and (future) HCPs about DMHIs, acceptance-facilitating interventions (AFIs) have been suggested as information strategies in earlier stages of innovation diffusion [18]. AFIs typically consist of multiple components, such as narrative messages (eg, experts’ recommendations), information on quality criteria, including the scientific evidence base, as well as the use of different media formats ranging from text-based information to video material [19]. Besides insignificant results in some studies on the effects of AFIs [20-22], different experiments have shown that AFIs can foster the acceptance of DMHIs among individuals with CMDs [23,24], students with or without mental health issues [25], and psychotherapists [18].
However, the optimal composition of multiattribute AFIs for providing DMHI information is difficult to determine with commonly used survey methods that do not require respondents to make trade-offs between the components they prefer the most. Discrete choice experiments (DCEs) offer the possibility to investigate complex hypothetical choices of information strategies [26] by involving combinations of various information attributes, varying in attribute levels, and controlling for interactions.
To our knowledge, only few DCEs examined information preferences on mental health services (eg, the study by Cunningham et al [27]), but none of them focused on DMHIs. Furthermore, while prior DCEs have focused on preferences regarding the delivery of DMHIs in the general population and among HCPs in Germany (refer to the studies by Phillips et al [28,29]), little is known about the specific information preferences regarding DMHIs in medical students.
This Study
This DCE aims to examine information preferences on DMHIs for personal use among medical students in Germany. For this purpose, 3 research questions were formulated: (1) What is the preferred information strategy regarding DMHIs (ie, AFIs) in medical students? (2) What are the most important attributes of information strategies? and (3) Does preference heterogeneity exist regarding information strategies?
Methods
Ethical Considerations
The ethics committee of the Faculty of Medicine at the Heinrich Heine University Düsseldorf approved the DCE in August 2022 (approval number 2022-2102).
The DCE was conducted web-based and anonymously using Lighthouse Studio (Sawtooth Inc). No identifying information, such as personal data or IP addresses, was recorded to ensure anonymity. To access the web survey, participants had to provide informed consent (click-to-agree). Participants were able to quit the assessment whenever they wanted. As an incentive, participants could take part in a lottery (5 × €100 [US $110.5] and 30 × €50 [US $55.3]) upon study completion by saving a randomly created code consisting of numbers (eg, via screenshot). No contact data were thus requested for participation in the lottery. This ensured the anonymity of participation. The winning codes were published on the website of the institute in May 2023. The payment was handled by university staff not involved in the research.
Study Design
The presented DCE was the main study of an exploratory mixed methods research approach. Next, we present the development of the DCE. Both study parts have been preregistered [30,31].
Following a sequential methodological approach and recommendations on the construction of DCEs according to the International Society for Pharmacoeconomics and Outcomes Research [32] and Hollin et al [33], the DCE development was grounded in literature research and formative qualitative research.
The development consisted of the following 6 sequential steps: (1) reviewing the research literature (for the research proposal), (2) conducting semistructured qualitative interviews, (3) conducting co-design workshops with medical and psychology students, (4) cognitive interviewing (concurrent think-aloud technique) and selection of attributes, (5) generating the experimental design, and (6) technical pretesting.
Steps of DCE Development
Preliminary Work: Literature Research
Research objectives were defined based on the current literature (using electronic databases and hand searching). In the first step, literature was searched to identify general information needs and preferences regarding DMHIs as well as potential acceptance-facilitating features of information on DMHIs among university students as potential users. This was the basis for the research proposal to be funded by the Research Commission of the Medical Faculty at the Heinrich Heine University Düsseldorf (grant 2020-60). As outlined in the Introduction section, this step led to the decision to focus the study on students of health care–related subjects, and especially medical students. In addition, because of the fragmentary research on the topic, a mixed methods design was chosen. In the second step, findings were used to develop semistructured topic guides for the qualitative interviews.
Qualitative Interviews
To explore the specific needs and preferences of students related to health care across Germany, we conducted 21 semistructured individual web-based interviews until consensus and thematic saturation were achieved (16/21, 76% medicine; 5/21, 24% psychology; female: 16/21, 76%; mean age 25.5, SD 3.9 y) in August and September 2021 using videoconference software (Webex; Cisco Systems). The interviews were saved using a digital recorder device and had an average duration of 31.7 (SD 10.3) minutes. The data were analyzed by applying content analysis according to Mayring [34], using MAXQDA, version 2020 (VERBI GmbH). Students indicated little knowledge and experience with DMHIs but positive attitudes toward their potential use. They were asked about their information preferences regarding design (eg, text or video), content (eg, data protection and costs), and source (eg, university or physician). We deductively derived 4 attributes of an information strategy: information source, delivery format, content preferences, and general design preferences, varying in different attribute levels (for a detailed description, refer to the study by Braun et al [35]). The results were used to develop a preliminary set of choice tasks for the DCE to be tested in co-design workshops for comprehensibility, relevance, completeness, and feasibility in the next step [26,32].
The interviews also addressed the setting in which participants would like to receive information about DMHIs. Medical students had preferred the university context in our prior work, which was therefore chosen as a context in the DCE (for detailed information, refer to studies by Braun et al [35] and Dederichs et al [36,37]).
Co-Design Workshops
To involve the target group in the DCE design and to validate and refine the selection of attributes and levels, 2 participatory co-design workshops with 8 university students (6/8, 75% medicine; 1/8, 12% psychology; and 1/8, 12% public health) were conducted in May and June 2022. The face-to-face workshops lasted approximately 90 to 120 minutes. Participants were asked to evaluate prepared choice tasks with respect to comprehensibility and cognitive effort. Owing to the workshops, we decided to focus on medical students only in the further preparation and realization of the DCE because the 2 (25%; nonmedical) of the 8 students expressed slightly different preferences for attributes and levels than medical students, which was interpreted in terms of their different study background. Furthermore, we made minor changes to the set of attributes, splitting content preferences into recommendation (eg, HCPs and patients) and quality criterion (eg, data security and scientific evidence base) and dropping general design preferences because it was rated least important. Furthermore, we added a new attribute called timing (eg, freshman week and preclinic), which seemed to be of greater importance to participants.
Cognitive Interviews
In July 2022, the preliminary DCE was discussed in cognitive interviews with 5 respondents. Participation required informed consent. Using the concurrent think-aloud method, which is an established approach in usability research [38], respondents were asked to share their thoughts while answering the survey, including DCE tasks and instructions. The piloting lasted approximately 60 minutes per participant and aimed to check again for comprehensibility and to identify difficulties in processing. Gathered information only led to some minor rearrangements.
Experimental Design
The experimental design was based on the decision by the research team to choose a set of attributes and levels following the qualitative research steps as well as plausibility considerations on combinations. The choice sets did not include an opt-out option because we wanted to learn which information strategy is preferred by students, given the university would decide to undertake an information campaign for DMHIs. A fractional factorial experimental design [39] was developed based on the study by Kuhlfeld [40] using the statistical software package SAS (SAS Software 9.4 [TS1M2]; SAS Institute Inc). The design allowed for an estimation of the main effects, with all attributes coded categorically. D-efficiency was 16.029. We used effects variable coding according to Bech and Gyrd-Hansen [41]. In the end, the experimental design consisted of 24 choice tasks, which we divided into 8 choice tasks administered in 3 blocks. Each choice set consisted of 5 attributes varying in 3 to 4 attribute levels.
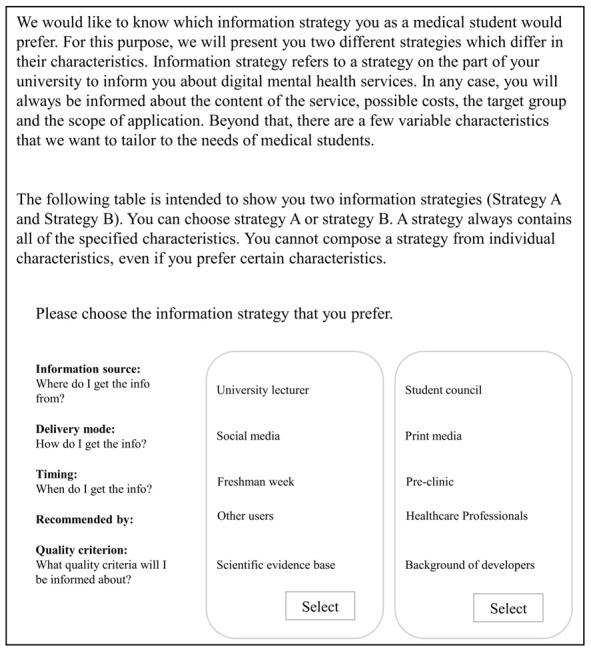
Participants were randomly assigned to 1 of the 3 blocks. In each block, we repeated 1 of the choice tasks to test the internal validity of the experiment as a reliability test. To familiarize respondents with the DCE format, we provided a detailed explanation for each attribute and attribute level (Table 1), followed by a written description of an example information strategy and an example choice task (Figure 1). Respondents were asked to choose the preferred information strategy to receive information about DMHIs. DMHIs were introduced as digital mental health services that can be used anonymously, from any location and at any time, for example, to reduce stress or combat examination anxiety. It was explained that DMHIs refer to smartphone apps (DiGA), browser-based applications, and psychological counseling via videoconferencing. We did not use an attribute for contents in this DCE due to anticipated heterogeneity in needs and knowledge [35].
Table 1.
Final set of attributes and levels of the discrete choice experiment to investigate preferences regarding information strategies for DMHIsa among medical students in Germany.
| Attribute | Level 1 | Level 2 | Level 3 | Level 4 | Description |
| Information source | Student councilb | Student services center | University lecturers | —c | Medical students could be informed on DMHIs by several organizational structures. Instances could be the student council, the student services center, and university lecturers. |
| Delivery mode | Social media | Seminar | Print media | Medical students could receive information on DMHIs via different delivery modes. These include email, the social media accounts of the university, such as Instagram (Meta Platforms, Inc), a seminar that is included in the curriculum, and print media. | |
| Timing | Freshman weekd | Preclinic | Clinic | Practical year | Medical students could be informed about DMHIs by their university at different times. They could be informed right at the beginning of their studies during the freshman week, during the first stage of their studies (preclinic), during the clinical stage of their studies, or at the end of their studies during their practical year. |
| Recommendation | HCPe | Users | Students | No recommendation | Information strategies on DMHIs may contain reviews or recommendations. These could come from HCPs, such as physicians, other users, or students. They also may not contain statements about whether a service is recommended or advertised by other groups of people. |
| Quality criterion | Data security | Scientific evidence base | Background of developers | Quality seal | Medical students could receive information about quality criteria to help them decide whether DMHIs meet a certain standard. These include information on specific measures to safeguard data security, the scientific evidence base, or the professional background of the developers of a specific service. A quality seal informs if, for example, the university or a federal institute has received a quality certificate for its service. |
aDMHI: digital mental health intervention.
bStudent council: members of the student council are students who were elected to represent their perspective and interests in medical school.
cNot applicable.
dFreshman week: in Germany, student councils introduce freshmen to a variety of aspects of campus life over the course of the first week and provide orientation for medical studies. In this welcome week, many workshops and social activities are offered for new students.
eHCP: health care professional.
Figure 1.
Instruction and example choice task of the discrete choice experiment to investigate preferences regarding information strategies for digital mental health interventions among medical students in Germany.
Technical Pretest
Finally, technical pretests of the first version of the programmed DCE with 3 feedback rounds (for iterative improvement) were conducted with 12 respondents from the institute of the principal investigator (eg, master students, doctoral candidates, research associates) and with 2 external medical students (personal contacts) in November and early December 2022. Technical pretesting resulted in several minor formal refinements of the survey interface. On the basis of pretest, the time required to complete the complete questionnaire (including the DCE and the questionnaire) was expected to be 15 to 20 minutes as planned.
Besides the DCE (including instructions), study information, and informed consent, the final survey asked for the background information presented in Textbox 1.
Background information for the final survey.
Background information
Demographic characteristics (gender, age, and German state of the university)
Studies (number of semesters, passed examinations—up to 3 in Germany until approbation)
Familiarity with digital mental health interventions (DMHIs; if they have heard of DMHIs before)
Attitudes toward potential use (how often they would like to use DMHIs: minutes a day and days a week)
Willingness to pay for DMHIs (preferred mode of payment and amount of money willing to pay)
Self-assessed stress in the previous and current semester using a visual analog scale (VAS) [42] ranging from 0 (minimum) to 10 (maximum)
Recruitment and Data Collection
Medical students who stated that they were aged ≥18 years and enrolled at a medical school in Germany were able to participate in the anonymous web study by accessing a link to the survey website (eg, via QR code). We followed a convenience sampling strategy, which means participants were recruited via social media and email (via student councils), personal contacts (eg, face-to-face, WhatsApp [Meta Platforms, Inc] personal chat, and chat groups), printed flyers, and posters at different universities across Germany. We also involved lecturers to promote the study (showing slides with a QR code and link to the DCE in their presentation slides). We were also supported by the Study Dean of our Faculty of Medicine, including survey invitations sent via email to different semesters in April 2023.
Data collection took place from December 10, 2022, to May 2, 2023, once the required number of participants was reached. A sample size of >125 medical students was targeted to provide sufficient statistical power for the main analysis and several subgroup analyses based on a rule-of-thumb formula proposed by Johnson and Orme [43].
Statistical Analysis
On the basis of the technical pretests of the web survey, it was assumed that a minimum processing time of 5 minutes was required to read the instructions and complete the DCE tasks properly; 5 minutes was a rather conservative estimation of the minimum processing time, as no participant in the pretest was able to complete the DCE in <5 minutes. For participants with lower processing time, we expected an insufficient engagement with the DCE (eg, choosing randomly and thereby increasing the error term of the analytical model) and excluded them from the analysis (ie, hard cutoff criterion). Moreover, participants who answered less than half of the choice sets (<4) were also excluded. Furthermore, the main analysis was based on respondents who passed the reliability test exclusively. The reliability test was passed if a repeated ninth control choice set was answered identically (ie, 1 choice set with strategy A and B swapped was repeated). Descriptive analysis for individual characteristics of the complete sample and participants that passed and did not pass the reliability test, respectively, were performed.
DCE data were analyzed using logistic regression models. In particular, we ran a conditional logit model clustered at the individual level to receive preference weights of levels as well as the relative importance of attributes. As the scale of coefficients is arbitrary, attributes are only comparable in relation to each other [44] using the relative importance of attributes.
In the second step, we considered possible preference heterogeneity by using a latent class analysis (LCA) model. The optimal class size was determined by the Bayesian information criterion and consistent Akaike information criterion. Classes were described by their preference weights and the relative importance of attributes. We also calculated posterior probabilities for being a member of a class for each participant. Respondents were assigned to the class with the higher posterior probability, and we compared individual characteristics of the assigned participants across classes descriptively. The analysis was performed with Stata 15 (StataCorp LLC). The significance level for statistical tests was an α error probability of <.05.
Results
Descriptive and Preliminary Analysis
The web survey was accessed 749 times. Of the 428 participants who gave informed consent, 97 (22.7%) needed a processing time of <5 minutes to complete the survey and were thus excluded from the analysis. Of those 97 participants who showed a processing time below 5 minutes, 66 (68%) participants did not complete at least 1 choice set, and another 5 (5%) respondents did complete <4 choice sets. Of the remaining 331 individuals, 309 (93%) respondents answered ≥4 choice sets of the DCE. In detail, those respondents who answered more than half of the choice sets completed all choice sets. Of those 22 individuals who answered <4 choice sets, 2 (9%) participants answered 2 choice sets, 1 (5%) participant answered one choice set, and 19 (86%) participants answered no choice set at all. The reliability test was passed by 231 (74.8%) of 309 participants (ie, complete samples). To describe choice-making behavior in the DCE in greater detail, we provide a lexicographic score analysis similar to Phillips et al [28], as shown in Multimedia Appendix 1 [28].
Characteristics of the sample are provided in Table 2 for the complete sample (N=309) as well as for participants who passed and did not pass the reliability test, respectively (n=231, 74.8 and n=78, 25.2%).
Table 2.
Individual characteristics of the full study sample, a sample with participants who passed, and a sample with participants who did not pass the reliability test (passed if a repeated ninth control choice set was answered identically in the discrete choice experiment; N=309)a.
| Variables | Full sample (N=309) | Passed reliability test (n=231) | Did not pass the reliability test (n=78) | Testb (P value) | ||
| Gender, n (%) | >.99c | |||||
|
|
Women | 217 (70.2) | 162 (70.1) | 55 (70.5) |
|
|
|
|
Men | 91 (29.4) | 68 (29.4) | 23 (29.5) |
|
|
|
|
Nonbinary | 1 (0.3) | 1 (0.4) | 0 (0) |
|
|
| Age (y), mean (SD) | 24.1 (4.0) | 24.1 (3.9) | 24.0 (4.1) | .88d | ||
| Semesters, mean (SD) | 7.1 (3.4) | 7.2 (3.4) | 7.0 (3.5) | .75d | ||
| Passed examinations, n (%)e | .95c | |||||
|
|
No passed examination | 113 (36.6) | 85 (36.8) | 28 (35.9) |
|
|
|
|
M1 examination | 151 (48.9) | 113 (48.9) | 38 (48.7) |
|
|
|
|
M2 examination | 43 (13.9) | 31 (13.4) | 12 (15.4) |
|
|
|
|
M3 examination | 2 (0.6) | 2 (0.9) | 0 (0) |
|
|
| Self-assessed stress (previous semester), n (%) | .32c | |||||
|
|
0=“no stress at all” | 0 (0) | 0 (0) | 0 (0) |
|
|
|
|
1 | 11 (3.6) | 10 (4.3) | 1 (1.3) |
|
|
|
|
2 | 8 (2.6) | 7 (3) | 1 (1.3) |
|
|
|
|
3 | 33 (10.7) | 24 (10.4) | 9 (11.5) |
|
|
|
|
4 | 25 (8.1) | 15 (6.5) | 10 (12.8) |
|
|
|
|
5 | 21 (6.8) | 18 (7.8) | 3 (3.8) |
|
|
|
|
6 | 31 (10) | 19 (8.2) | 12 (15.4) |
|
|
|
|
7 | 61 (19.7) | 46 (19.9) | 15 (19.2) |
|
|
|
|
8 | 62 (20.1) | 48 (20.8) | 14 (17.9) |
|
|
|
|
9 | 34 (11) | 28 (12.1) | 6 (7.7) |
|
|
|
|
10=“very stressed” | 23 (7.4) | 16 (6.9) | 7 (9) |
|
|
| Self-assessed stress (currently), n (%) | .33c | |||||
|
|
0=“no stress at all” | 23 (7.4) | 17 (7.4) | 6 (7.7) |
|
|
|
|
1 | 24 (7.8) | 20 (8.7) | 4 (5.1) |
|
|
|
|
2 | 47 (15.2) | 36 (15.6) | 11 (14.1) |
|
|
|
|
3 | 37 (12) | 23 (10) | 14 (17.9) |
|
|
|
|
4 | 25 (8.1) | 16 (6.9) | 9 (11.5) |
|
|
|
|
5 | 26 (8.4) | 19 (8.2) | 7 (9) |
|
|
|
|
6 | 27 (8.7) | 19 (8.2) | 8 (10.3) |
|
|
|
|
7 | 39 (12.6) | 32 (13.9) | 7 (9) |
|
|
|
|
8 | 31 (10) | 22 (9.5) | 9 (11.5) |
|
|
|
|
9 | 13 (4.2) | 11 (4.8) | 2 (2.6) |
|
|
|
|
10=“very stressed” | 17 (5.5) | 16 (6.9) | 1 (1.3) |
|
|
| Being aware of DMHIsf, n (%) | 98 (31.7) | 75 (32.5) | 23 (29.5) | .68d | ||
| Expected frequency of use (days per week), mean (SD) | 2.2 (1.6) | 2.2 (1.6) | 2.3 (1.5) | .61d | ||
| Expected frequency of use (minutes per day), mean (SD) | 21.4 (16.5) | 21.2 (15.5) | 22.1 (19.2) | .60d | ||
| Price participants were willing to pay (€g), mean (SD) | 25.7 (60.4) | 22.8 (22.0) | 34.5 (114.2) | 0.5d | ||
aNo missing data in individual characteristics.
bTest for differences in individual characteristics for participants who passed the reliability test and those who did not pass the reliability test.
cFisher exact test.
dMann-Whitney U test.
eM1-M3: first to third state examination in medical schools in Germany.
fDMHI: digital mental health intervention.
gExchange rate: 1€=US $1.11.
Most participants (217/309, 70.2%) in the full sample were women aged, on average, approximately 24 years (SD 4.0) and studying in their seventh semester (mean 7.1, SD 3.4). The mean age of men (mean 25.7, SD 4.4 years) was significantly higher than that of women (mean 23.3, SD 3.5 years) in the full sample (Mann-Whitney U test: P<.001), which also corresponds to a significantly higher mean semester for men than for women (mean 7.9, SD 3.1 vs mean 6.8, SD 3.5 semesters, Mann-Whitney U test: P=.006). Approximately one-third (113/309, 36.6%) of the university students in the complete sample passed no major examination to date, while nearly one-half (151/309, 48.9%) passed the M1 examination, which is the first state examination in medical studies and takes place after completion of the preclinical phase. The distribution of self-assessed stress during the previous semester was left-tailed, with a majority (211/309, 68.3%) of students indicating 6 to 10 on the 10-point rating scale, which might be interpreted as feeling moderately to severely stressed. In comparison to stress in the previous semester, the current self-assessed stress shifted to a lower level (only 127/309, 41.1% indicated a 6-10).
Of the 309 participants, 98 (31.7%) indicated being aware of DMHIs. On average, participants were willing to use DMHIs 2 days per week (mean 2.2, SD 1.6 days) and 21 minutes per day (mean 21.4, SD 16.5 min). As the most preferred payment mode, 93.2% (288/309) of students agreed on free offers. Nonetheless, the mean willingness to make a one-time payment for DMHI service was mean €25.7 (SD €60.4; 1€=US $1.11). A detailed analysis of the willingness to pay is provided in Multimedia Appendix 2.
Comparing individuals with a reliable versus a nonreliable response pattern according to their characteristics, no significant differences were detected (all with P>.05). In the following analysis, only participants who passed the reliability test were included. Yet, the results of the complete sample analysis are similar to the results based on the sample of respondents who passed the reliability test (Multimedia Appendix 3). Also, a Swait-Louviere test [45] indicated that while preferences were not significantly different for people who passed and did not pass the reliability test at the 5% significance level (H0a: P=.18), it also showed that the scale parameter differed significantly (H0b: P=.003).
Main Findings
Table 3 presents the conditional logit regression results for respondents who passed the reliability test (n=231).
Table 3.
Conditional logit regression results of the discrete choice experiment, showing significant attributes and levels as well as the relative importance of attributes in comparison.
| Attributes and levels | Coefficient (SE; 95% CIa) | Relative importance (%) | |||
| Information source | 9.22 | ||||
|
|
Student service center | –0.04 (0.05; –0.13 to 0.06) |
|
||
|
|
Student council | 0.17 (0.05; 0.07 to 0.28) |
|
||
|
|
University lecturers | –0.14 (0.04; –0.22 to –0.05) |
|
||
| Delivery mode | 24.44 | ||||
|
|
Social media | 0.27 (0.06; 0.15 to 0.39) |
|
||
|
|
0.16 (0.06; 0.05 to 0.27) |
|
|||
|
|
Seminar | 0.12 (0.07; –0.02 to 0.25) |
|
||
|
|
Print media | –0.55 (0.07; –0.68 to –0.42) |
|
||
| Timing | 32.59 | ||||
|
|
Freshman week | 0.31 (0.06; 0.19 to 0.42) |
|
||
|
|
Preclinic | 0.50 (0.06; 0.38 to 0.62) |
|
||
|
|
Clinic | –0.20 (0.05; –0.31 to –0.10) |
|
||
|
|
Practical year | –0.60 (0.07; –0.73 to –0.47) |
|
||
| Recommendation | 19.09 | ||||
|
|
HCPb | 0.14 (0.05; 0.04 to 0.24) |
|
||
|
|
Students | 0.29 (0.05; 0.18 to 0.39) |
|
||
|
|
Users | –0.07 (0.05; –0.16 to 0.02) |
|
||
|
|
No review | –0.35 (0.06; –0.47 to –0.24) |
|
||
| Quality criterion | 14.66 | ||||
|
|
Data security | –0.12 (0.06; –0.24 to –0.01) |
|
||
|
|
Evidence based | 0.30 (0.06; 0.18 to 0.41) |
|
||
|
|
Quality seal | 0.02 (0.05; –0.08 to 0.12) |
|
||
|
|
Background of developers | –0.20 (0.06; –0.31 to –0.08) |
|
||
aCI significance is assumed if the CI does not include the number 0 (no different signs).
bHCP: health care professional.
Medical students significantly (P=.001) preferred to receive information about DMHIs from the student council and significantly refused to receive information from university lecturers (P=.002). As delivery mode, participants wanted to get the information delivered via social media (P<.001) and email (P=.006) and did not want to receive the information via print-based media (P<.001). Students had significant positive preference weights for receiving the information about DMHIs during their preclinic phase or in the freshman week and significant negative preference weights for the practical year (all with P<.001).
The recommendation should be given by other students (P<.001) or HCPs (P=.007), while no recommendation was rated negatively (P<.001).
As a quality criterion, medical students significantly preferred information about the evidence-based background of DMHIs (P<.001). Data security (P=.04) and background of developers (P=.001) showed significant negative preference weights.
With a relative importance of 32.6%, the most relevant attribute for medical students was timing (ie, time point in their studies when the information is shared). In addition, the attributes delivery mode (relative importance 24.4%) and recommendation (relative importance 19.1%) showed a high relative importance as well. The attributes of quality criterion (relative importance 14.7%) and information source (relative importance 9.2%) were less important for medical students.
To account for preference heterogeneity, we used an LCA. The results for respondents who passed the reliability test (n=231) are presented in Table 4. The optimal number of classes was determined by the Bayesian information criterion and consistent Akaike information criterion, which were minimized at 2 classes (Multimedia Appendix 4).
Table 4.
Latent class model regression results of the discrete choice experiment, showing significant attributes and levels as well as the relative importance of attributes in comparison for 2 identified groups varying in information preferences (N=231).
| Attributes and levels | Class 1 (n=147) | Class 2 (n=84) | ||||||
|
|
Coefficient (SE; 95% CI) | Relative importance (%) | Coefficient (SE; 95% CI) | Relative importance (%) | ||||
| Information source | 1.49 |
|
24.21 | |||||
|
|
Student service center | –0.03 (0.07; –0.18 to 0.11) |
|
–0.07 (0.13; –0.32 to 0.18) |
|
|||
|
|
Student council | 0.03 (0.07; –0.12 to 0.18) |
|
0.56 (0.25; 0.07 to 1.04) |
|
|||
|
|
University Lecturers | 0.00 (0.07; –0.14 to 0.14) |
|
–0.49 (0.26; –0.99 to 0.02) |
|
|||
| Delivery mode | 35.49 |
|
42.86 | |||||
|
|
Social media | 0.09 (0.10; –0.10 to 0.29) |
|
0.67 (0.19; 0.29 to 1.05) |
|
|||
|
|
–0.09 (0.09; –0.27 to 0.08) |
|
0.74 (0.29; 0.17 to 1.31) |
|
||||
|
|
Seminar | 0.76 (0.13; 0.51 to 1.01) |
|
–1.11 (0.38; –1.85 to –0.36) |
|
|||
|
|
Print media | –0.77 (0.11; –0.98 to –0.55) |
|
–0.31 (0.49; –1.27 to 0.65) |
|
|||
| Timing | 21.27 |
|
46.11 | |||||
|
|
Freshman week | 0.14 (0.08; –0.02 to 0.29) |
|
0.86 (0.32; 0.24 to 1.48) |
|
|||
|
|
Preclinic | 0.48 (0.11; 0.27 to 0.69) |
|
0.71 (0.31; 0.09 to 1.32) |
|
|||
|
|
Clinic | –0.18 (0.09; –0.36 to –0.003) |
|
–0.43 (0.18; –0.78 to –0.09) |
|
|||
|
|
Practical year | –0.44 (0.10; –0.63 to –0.24) |
|
–1.13 (0.46; –2.02 to –0.24) |
|
|||
| Recommendation | 19.73 |
|
4.02 | |||||
|
|
HCPa | 0.22 (0.09; 0.04 to 0.40) |
|
–0.03 (0.33; –0.68 to 0.62) |
|
|||
|
|
Students | 0.35 (0.09; 0.17 to 0.54) |
|
0.04 (0.18; –0.32 to 0.39) |
|
|||
|
|
Users | –0.07 (0.08; –0.23 to 0.09) |
|
0.08 (0.32; –0.55 to 0.72) |
|
|||
|
|
No review | –0.50 (0.06; –0.61 to –0.38) |
|
–0.09 (0.45; –0.97 to 0.79) |
|
|||
| Quality criterion | 22.02 |
|
19.10 | |||||
|
|
Data security | –0.39 (0.09; –0.56 to –0.22) |
|
0.37 (0.26; –0.15 to 0.88) |
|
|||
|
|
Evidence based | 0.56 (0.10; 0.35 to 0.76) |
|
0.00 (0.18; –0.37 to 0.36) |
|
|||
|
|
Quality seal | –0.04 (0.08; –0.20 to 0.13) |
|
0.09 (0.14; –0.19 to 0.38) |
|
|||
|
|
Background of developers | –0.13 (0.05; –0.23 to –0.03) |
|
–0.46 (0.28; –1.00 to 0.08) |
|
|||
aHCP: health care professional.
When assigning participants based on their posterior probabilities, we found that nearly two-thirds (147/231, 63.6%) could be allocated to class 1 (labeled “seminar-based information strategy”) and one-third (84/231, 36.4%) to class 2 (referred to as “early digital information strategy”). The 2 classes differed considerably in their preference patterns as well as in their relative importance of attributes. For class 1, the most important attribute was the delivery mode (approximately 36%) with seminar as the most preferred level. The attributes quality criterion, timing, and recommendation had similar shares of relative importance, approximately 20% each. In particular, preferences of class 1 showed that information about the evidence base of DMHIs should be used as a quality criterion, information should be provided during the preclinic phase, and recommendations for DMHIs should be given by students or HCPs. Information source was the least important attribute of class 1 (approximately 1%). According to the relative importance of attributes for class 2, timing (approximately 46%) and, with comparable relative importance, delivery mode (approximately 43%) were the most important attributes. Class 2 showed a strong preference for receiving the information about DMHIs early during their studies (preclinic phase or freshman week) and preferred receiving information via email or social media. The attribute information source showed a relative importance of approximately 24%, with student council as the preferred level. Regarding the attribute quality criterion (approximately 19%), data security was preferred by class 2 (not significant). The attribute recommendation was the least relevant attribute for class 2 (approximately 4%).
We compared the individual characteristics of members of class 1 and class 2, respectively, and found no significant differences (all with P<.05), except for being familiar with DMHIs (Multimedia Appendix 4). In detail, members of class 1 were significantly more familiar with DMHIs than members of class 2 (37.4% vs 23.8%).
Discussion
Principal Findings
In this study, we conducted a DCE to investigate information preferences regarding DMHIs for personal use among medical students in Germany. We aimed to derive a preferred information strategy and aimed to identify its most important features. In addition, we investigated whether there are latent classes among medical students that differ in information strategy preferences.
Preferred Information Strategy and Relative Importance of Features
Overview
In the subsequent sections, the results regarding the various features of the preferred information strategy are discussed one by one. It is important to consider that participants thought about self-use, as indicated in the Introduction section. When addressing them as future physicians, results may be different.
Medical Students Preferred to Be Informed Early in the Freshman Week or the Preclinical Phase of Their Studies
Potentially, medical students (mean semester was 7, SD 3.4) had already experienced study-related mental health issues themselves or had seen such issues in their peers, which might lead to a preference for early information. Indeed, a meta-analysis indicated increased prevalence rates of mental health problems, especially in younger and preclinical students [16]. At best, the timing for information should be chosen when students feel mentally healthy or when academic distress has not already contributed to manifested health issues requiring interventions.
Information via Social Media and Email Was Favored Compared With Print-Based Media
Potentially, this reflects the habits and preferences of younger adults and digital natives included in our study. However, the research literature on the digital resource preferences of health care students belonging to the so-called Generation Z is interestingly limited and inconsistent [46]. In addition, in our study, participants even clearly refused to receive information via print media (eg, flyers). A possible explanation for this is the immense amount of printed information in medical schools. Students have to read and learn a great deal of complex content, mainly from textbooks, in a very short time for examination preparation. Possibly, they do not want the same modality of delivery that is regularly associated with study, work, or even stress for obtaining information concerning the promotion of their mental health. Another disadvantage of print media could be that it is visible to others when someone receives information via, for example, flyer or brochure. In contrast, brief information delivered digitally could be perceived as more pleasant (eg, a short video) and is easy to access whenever needed in daily life. Furthermore, the DCE was conducted about 3 years after the beginning of the COVID-19 pandemic, which led to the extension of e-learning in medical education. Elevated familiarity with digitally provided, approved health information in recent years may have increased the acceptance of digital information channels for other contexts [47]. Of course, students generally vary in learning preferences and learning styles [48] while research on learning styles in particular has been subject to controversy in terms of its evidence base and practical usefulness in medical education [49]. Therefore, we focused on stated preferences as well-researched constructs in the investigation of user-centered information strategies. However, we could only consider previously identified attributes and levels that may alter over time regarding their relevance for the target group with changing consumer habits and experiences. Future DCEs should explore which channel of social media (eg, Instagram [Meta Platforms, Inc] or TikTok [ByteDance]) and which presentation format (eg, video or participatory) should be used to disseminate information on DMHIs.
Participants Liked to Receive Recommendations From Other Students and HCPs
Both students and HCPs appeared suitable as role models (refer to social cognitive theory [50]) and trusted sources. Possibly, students preferred these sources as they are similar to themselves now (ie, as students) and hypothetically in the future (ie, as physicians), as different empirical investigations on the impact of narratives from individuals with a similar background on decision-making in health care contexts indicated [51,52]. Nonetheless, influences of recommendations are highly context sensitive.
For instance, in a DCE with young adults conducted by Cunningham et al [27], those who wanted to be informed digitally preferred recommendations by other young adults with previous experiences of depression and anxiety, while those who wanted to be informed conventionally via traditional media channels liked to receive recommendations from physicians. Hence, information features should be tailored to the preferences of the target group, including subgroups differing in information preferences (refer to LCA results mentioned subsequently). Although testimonials are commonly used in DMHI advertisements, it remains unclear how useful recipients view such recommendations as features of information or if the advertisements have an influence on the uptake of DMHIs [22]. Therefore, the integration of recommendations should be carefully chosen in dialog with the key target group for the information distribution. In future studies, it would be interesting to investigate the characteristics of recommendations that students perceive as trustworthy (eg, those with own experience with mental health issues).
Regarding Quality Criteria, Medical Students Significantly Preferred Information About the Evidence-Based Background of DMHIs
Data security and background of developers showed significant negative preference weights. Students expected the information to be provided by the university (as stated in the DCE’s instructions), and possibly assumed that the offerings were already quality tested and therefore focused on other quality criteria than they would be interested in another setting. Addressed in their role as future professionals, preferences might differ, and participants may place more emphasis on information on the evidence base or data security for professional use (eg, refer to studies by Braun et al [35] and Dederichs et al [36]).
Medical Students Preferred to Receive Information About DMHIs From Their Student Council
Medical students even refused to receive information from university lecturers. With respect to mental health topics, students may have a higher trust in students’ representatives as peers and may worry about stigmatization by lecturers if they disclose their need for support.
Subgroup-Specific Information Strategies
LCA identified 2 distinct groups of students who differed considerably in their information preferences. Class 1, which we classified as “seminar-based information strategy,” preferred to receive information about DMHIs in a face-to-face seminar in the preclinic phase. Moreover, they preferred to obtain recommendations from other students, while information about the evidence base of DMHIs should serve as a key quality criterion. Except for the delivery mode (seminar), preferences of class 1 were similar to the overall preferences of participants regarding DMHI information strategies, which can be well explained by the fact that the majority (ie, 147/231, 63.6%) could be classified as members of class 1.
In contrast, the ideal information strategy of class 2 (“early digital information strategy”) would be to provide information by the student council via social media or by email. Regarding the timing of information, class 2 preferred to receive them as early as possible, that is, during the freshman week (before the actual start of studies). The attributes quality criteria and recommendation were less important for class 2 than for class 1, and the findings were insignificant. Members of class 2 were significantly less familiar with DMHIs than members of class 1. Hence, they may want to be initially informed at a low threshold. In prior qualitative studies with medical students, they expressed the wish to get quick support by interventions that are easy to access in times of study-related distress, for example, services targeting stress and time management [36,53]. Furthermore, we did not find any significant differences (eg, in stress levels) in the individual characteristics of members of class 1 and class 2.
However, preferences of classes 1 and 2 should be not viewed as divergent strategies but may help to develop complementary stepped or matched approaches. For instance, digitally provided information could be the first step that might lead to further information-seeking behavior and the attendance of seminars on DMHIs. A combination of both strategies should be used to reach a higher number of medical students throughout Germany. Specifically, the digital strategy, which is in line with the overall preference, represents a way to reach a broad range of medical students, especially those with little knowledge or no currently perceived need for DHMIs.
Besides the DCE, our study provided new insights into the willingness to pay for DMHIs, which should also be considered by universities when informing about interventions. In particular, medical students stated being willing to pay €22.7 (US $ 25.25) as a unique fee on average to use DMHIs.
Limitations
A key limitation was that we recruited medical students mainly via one channel, namely, personal invitations (eg, chat groups and emails from student councils), as postings in social media groups (eg, on Facebook [Meta Platforms, Inc]), as well as flyers on campus across different universities, were much less effective in terms of recruitment success. Nonetheless, the sample seems to be similar to the overall population of medical students in Germany regarding their individual characteristics, such as age and gender (eg, study by Groene et al [54]).
Another limitation was that students could participate during the semester and during the semester break. Information preferences regarding mental health services might differ depending on the time of participation and related needs and stress levels (eg, in times of examinations and semester appointments). Specifically, increased perceived stress may indicate personal need or relevance of mental health information and thereby foster the motivation to seek information on coping strategies, which may be related to more interest in easily accessible support services, such as DMHIs.
However, our study can only provide very limited information on whether or how emotional distress may have influenced DMHI information preferences. Due to ethical aspects and to keep the (emotional) response burden as low as possible, we refrained from using clinical screening measures on CMDs in this study. A future DCE could put a greater emphasis on information preference on DMHIs for self-help and adjunctive treatment, which could include the assessment of different mental health conditions.
A further limitation was that most participants had not heard of DMHIs before, which is similar to prior studies with students from our work group [25,36,55,56] but may have resulted in difficulties in decision-making and thus contributed to heuristic decisions (eg, finding student councils more appealing than lectures and thus wanting them as information source).
It should be noted that there was no opt-out option given to respondents, which corresponds to the real-world setting of students receiving information by a university information campaign. However, our results may be biased to some extent as students not wanting to receive information may differ in their preferences from those wanting to receive information.
Finally, we will discuss a few thoughts on the selected attributes and levels. Concerning the level “seminar,” belonging to the attribute “delivery mode,” further information on the organization of a seminar (eg, block seminar, face-to-face seminar, and web seminar) would be desirable. Further research should clarify the preferences of medical students regarding the design of seminars about DMHIs (eg, mode, duration, and topic).
Finally, there might be a lack of selectivity in the attribute levels “students” and “users” regarding the attribute “recommendation” because students can also be users at the same time. However, due to the different assessments (with other students being a significant recommendation source), it seems that the participants viewed those attributes differently, and therefore, this limitation may not be severe. Future DCEs could use additional qualitative methods to prevent such potential sources of bias (eg, by more detailed descriptions of prototypical users or personas to be developed with the target group).
Conclusions
Overall, the study findings suggest distinct general and subgroup-specific information strategies on DMHIs that are potentially suitable for medical students in Germany. Designing information strategies according to the stated preferences could help to increase DMHI use. This DCE offers a variety of possible features to be tested in practice. As the first step, AFI strategies could start to promote the awareness of or basic knowledge of DMHIs for health promotion purposes with a social media campaign related to the university setting aimed at students early in their studies. The campaign could be provided by the student council, combining recommendations and information about scientific evidence as complementary features. This low-threshold offer could lead to students attending seminars on DMHIs involving more detailed knowledge in a second step. Seminars should be firmly anchored in the curricula of the medical faculties in accordance with the mandatory German National Competency-Based Learning Objective Catalogue of Medicine; digital competencies have not been listed for very long in this catalogue [57], but are now, albeit to a limited extent.
Acknowledgments
This discrete choice experiment (DCE) was funded as main part of a mixed methods study (subproject: “eMent-In-form-DCE”) by internal funds for Young Investigators of the Research Commission (German: “Forschungskommission”; FoKo) of the Faculty of Medicine at the Heinrich Heine University Düsseldorf (proposal 2020-60; granted for the project lead JA-H). The authors thank the Open Access Funds of the Heinrich Heine University Düsseldorf and the Faculty of Medicine for providing the open-access publication fees. The authors also cordially thank Sawtooth Inc for supporting their DCE with a PhD grant (PH MSc) with a free license to their software program Lighthouse Studio to program, host, and administer the DCE. The authors also thank the staff of the study dean of the Faculty of Medicine at the Heinrich Heine University Düsseldorf; Fatma Sahan, BSc; Lisa Guthardt, MA; Dr Thomas Muth; Fiona Kohl, MPH; Susan Gritzka, MSc; Anna Siegel-Kianer; and several student councils (eg, Düsseldorf, Jena, Essen, and Münster) for their support with the recruitment of the sample. The authors also thank Dr Ann-Kathrin Schwientek, MPH, for her substantial contribution to the interview study (planning, conduction, and analysis), which served as the basis for the DCE.
Abbreviations
- AFI
acceptance-facilitating intervention
- BfARM
Bundesinstitut für Arzneimittel und Medizinprodukte
- CMD
common mental disorder
- DCE
discrete choice experiment
- DiGA
Digitale Gesundheitsanwendungen
- DMHI
digital mental health intervention
- HCP
health care professional
- LCA
latent class analysis
Choice-making behavior–lexicographic scores.
Willingness to pay for digital mental health interventions.
Results of the complete sample analysis.
Further information on latent class analysis.
Data Availability
The data sets generated during and analyzed during this study are available from the corresponding author on reasonable request.
Footnotes
Authors' Contributions: MV contributed to conceptualization, formal analysis, methodology, visualization, and writing and preparing the original draft. JTB contributed to formal analysis, investigation, visualization, and writing and preparing the original draft. PH contributed to conceptualization, investigation, software use, visualization, and writing, reviewing, and editing the manuscript. SS contributed to investigation, software, and writing, reviewing, and editing the manuscript. BH contributed to methodology and writing, reviewing, and editing the manuscript. AL contributed to conceptualization, methodology, and writing, reviewing, and editing the manuscript. AI and CRP contributed to conceptualization and writing, reviewing, and editing the manuscript. STC and LS contributed to investigation and writing, reviewing, and editing the manuscript. NK-S contributed to methodology and writing, reviewing, and editing the manuscript. PA contributed to conceptualization, resources, and writing, reviewing, and editing the manuscript. JA-H contributed to conceptualization, funding acquisition, methodology, project administration, validation, and writing and preparing the original draft.
Conflicts of Interest: None declared.
References
- 1.Borghouts J, Eikey E, Mark G, De Leon C, Schueller SM, Schneider M, Stadnick N, Zheng K, Mukamel D, Sorkin DH. Barriers to and facilitators of user engagement with digital mental health interventions: systematic review. J Med Internet Res. 2021 Mar 24;23(3):e24387. doi: 10.2196/24387. https://www.jmir.org/2021/3/e24387/ v23i3e24387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Heinig I, Wittchen HU, Knappe S. Help-seeking behavior and treatment barriers in anxiety disorders: results from a representative german community survey. Community Ment Health J. 2021 Nov;57(8):1505–17. doi: 10.1007/s10597-020-00767-5. https://europepmc.org/abstract/MED/33471256 .10.1007/s10597-020-00767-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tomczyk S, Schmidt S, Muehlan H, Stolzenburg S, Schomerus G. A prospective study on structural and attitudinal barriers to professional help-seeking for currently untreated mental health problems in the community. J Behav Health Serv Res. 2020 Jan;47(1):54–69. doi: 10.1007/s11414-019-09662-8.10.1007/s11414-019-09662-8 [DOI] [PubMed] [Google Scholar]
- 4.Gaebel W, Lukies R, Kerst A, Stricker J, Zielasek J, Diekmann S, Trost N, Gouzoulis-Mayfrank E, Bonroy B, Cullen K, Desie K, Ewalds Mulliez AP, Gerlinger G, Günther K, Hiemstra HJ, McDaid S, Murphy C, Sander J, Sebbane D, Roelandt JL, Thorpe L, Topolska D, Van Assche E, Van Daele T, Van den Broeck L, Versluis C, Vlijter O. Upscaling e-mental health in Europe: a six-country qualitative analysis and policy recommendations from the eMEN project. Eur Arch Psychiatry Clin Neurosci. 2021 Sep;271(6):1005–16. doi: 10.1007/s00406-020-01133-y.10.1007/s00406-020-01133-y [DOI] [PubMed] [Google Scholar]
- 5.Ebert DD, Harrer M, Apolinário-Hagen J, Baumeister H. Digital interventions for mental disorders: key features, efficacy, and potential for artificial intelligence applications. Adv Exp Med Biol. 2019;1192:583–627. doi: 10.1007/978-981-32-9721-0_29. [DOI] [PubMed] [Google Scholar]
- 6.Gagnon MP, Sasseville M, Leblanc A. Classification of digital mental health interventions: a rapid review and framework proposal. Stud Health Technol Inform. 2022 May 25;294:629–33. doi: 10.3233/SHTI220545.SHTI220545 [DOI] [PubMed] [Google Scholar]
- 7.Gerlinger G, Mangiapane N, Sander J. [Digital health applications (DiGA) in medical and psychotherapeutic care. Opportunities and challenges from the perspective of the healthcare providers] Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2021 Oct;64(10):1213–9. doi: 10.1007/s00103-021-03408-8.10.1007/s00103-021-03408-8 [DOI] [PubMed] [Google Scholar]
- 8.Heimann P, Lorenz N, Blum N, Schifferings C. [Experiences of digital health care applications (DIGA) manufacturers with the BfArM Fast-Track procedure] Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2021 Oct;64(10):1249–53. doi: 10.1007/s00103-021-03422-w.10.1007/s00103-021-03422-w [DOI] [PubMed] [Google Scholar]
- 9.Wangler J, Jansky M. Digitale gesundheitsanwendungen (DiGA) in der primärversorgung – erfahrungen und beobachtungen von hausärzt*innen hinsichtlich der anwendung von DiGA. Präv Gesundheitsf. 2022 Oct 25;18(4):483–91. doi: 10.1007/s11553-022-00988-4. [DOI] [Google Scholar]
- 10.Dahlhausen F, Zinner M, Bieske L, Ehlers JP, Boehme P, Fehring L. Physicians' attitudes toward prescribable mHealth apps and implications for adoption in Germany: mixed methods study. JMIR Mhealth Uhealth. 2021 Nov 23;9(11):e33012. doi: 10.2196/33012. https://mhealth.jmir.org/2021/11/e33012/ v9i11e33012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Schlieter H, Kählig M, Hickmann E, Fürstenau D, Sunyaev A, Richter P, Breitschwerdt R, Thielscher C, Gersch M, Maaß W, Reuter-Oppermann M, Wiese L. [Digital health applications (DiGA) in the area of tension between progress and criticism : discussion paper from the "digital health" specialist group of the German Informatics Society] Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2024 Jan;67(1):107–14. doi: 10.1007/s00103-023-03804-2. https://europepmc.org/abstract/MED/38086924 .10.1007/s00103-023-03804-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Torous J, Jän Myrick K, Rauseo-Ricupero N, Firth J. Digital mental health and COVID-19: using technology today to accelerate the curve on access and quality tomorrow. JMIR Ment Health. 2020 Mar 26;7(3):e18848. doi: 10.2196/18848. https://mental.jmir.org/2020/3/e18848/ v7i3e18848 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rogers EM. Diffusion of preventive innovations. Addict Behav. 2002;27(6):989–93. doi: 10.1016/s0306-4603(02)00300-3.S0306-4603(02)00300-3 [DOI] [PubMed] [Google Scholar]
- 14.Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, Sen S, Mata DA. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. 2016 Dec 06;316(21):2214–36. doi: 10.1001/jama.2016.17324. https://europepmc.org/abstract/MED/27923088 .2589340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Quek TT, Tam WW, Tran BX, Zhang M, Zhang Z, Ho CS, Ho RC. The global prevalence of anxiety among medical students: a meta-analysis. Int J Environ Res Public Health. 2019 Jul 31;16(15):2735. doi: 10.3390/ijerph16152735. https://www.mdpi.com/resolver?pii=ijerph16152735 .ijerph16152735 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peng P, Hao Y, Liu Y, Chen S, Wang Y, Yang Q, Wang X, Li M, Wang Y, He L, Wang Q, Ma Y, He H, Zhou Y, Wu Q, Liu T. The prevalence and risk factors of mental problems in medical students during COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2023 Jan 15;321:167–81. doi: 10.1016/j.jad.2022.10.040. https://linkinghub.elsevier.com/retrieve/pii/S0165-0327(22)01231-9 .S0165-0327(22)01231-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shahaf-Oren B, Madan I, Henderson C. "A lot of medical students, their biggest fear is failing at being seen to be a functional human": disclosure and help-seeking decisions by medical students with health problems. BMC Med Educ. 2021 Dec 05;21(1):599. doi: 10.1186/s12909-021-03032-9. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-021-03032-9 .10.1186/s12909-021-03032-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Baumeister H, Terhorst Y, Grässle C, Freudenstein M, Nübling R, Ebert DD. Impact of an acceptance facilitating intervention on psychotherapists' acceptance of blended therapy. PLoS One. 2020;15(8):e0236995. doi: 10.1371/journal.pone.0236995. https://dx.plos.org/10.1371/journal.pone.0236995 .PONE-D-20-00142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hein HJ, Glombiewski JA, Rief W, Riecke J. Effects of a video intervention on physicians' acceptance of pain apps: a randomised controlled trial. BMJ Open. 2022 Apr 25;12(4):e060020. doi: 10.1136/bmjopen-2021-060020. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=35470200 .bmjopen-2021-060020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Baumeister H, Seifferth H, Lin J, Nowoczin L, Lüking M, Ebert D. Impact of an acceptance facilitating intervention on patients' acceptance of internet-based pain interventions: a randomized controlled trial. Clin J Pain. 2015 Jun;31(6):528–35. doi: 10.1097/AJP.0000000000000118. [DOI] [PubMed] [Google Scholar]
- 21.Lin J, Faust B, Ebert DD, Krämer L, Baumeister H. A web-based acceptance-facilitating intervention for identifying patients' acceptance, uptake, and adherence of internet- and mobile-based pain interventions: randomized controlled trial. J Med Internet Res. 2018 Aug 21;20(8):e244. doi: 10.2196/jmir.9925. https://www.jmir.org/2018/8/e244/ v20i8e244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Healey BJ, Griffiths KM, Bennett K. The effect of programme testimonials on registrations for an online cognitive behaviour therapy intervention: a randomised trial. Digit Health. 2017 Sep 12;3:2055207617729937. doi: 10.1177/2055207617729937. https://journals.sagepub.com/doi/abs/10.1177/2055207617729937?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_2055207617729937 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Soucy JN, Owens VA, Hadjistavropoulos HD, Dirkse DA, Dear BF. Educating patients about internet-delivered cognitive behaviour therapy: perceptions among treatment seekers and non-treatment seekers before and after viewing an educational video. Internet Interv. 2016 Nov;6:57–63. doi: 10.1016/j.invent.2016.09.003. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(16)30035-5 .S2214-7829(16)30035-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ebert DD, Berking M, Cuijpers P, Lehr D, Pörtner M, Baumeister H. Increasing the acceptance of internet-based mental health interventions in primary care patients with depressive symptoms. A randomized controlled trial. J Affect Disord. 2015 May 01;176:9–17. doi: 10.1016/j.jad.2015.01.056.S0165-0327(15)00069-5 [DOI] [PubMed] [Google Scholar]
- 25.Apolinário-Hagen J, Fritsche L, Wopperer J, Wals F, Harrer M, Lehr D, Ebert DD, Salewski C. Investigating the persuasive effects of testimonials on the acceptance of digital stress management trainings among university students and underlying mechanisms: a randomized controlled trial. Front Psychol. 2021;12:738950. doi: 10.3389/fpsyg.2021.738950. https://europepmc.org/abstract/MED/34721212 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Reed Johnson F, Lancsar E, Marshall D, Kilambi V, Mühlbacher A, Regier DA, Bresnahan BW, Kanninen B, Bridges JF. Constructing experimental designs for discrete-choice experiments: report of the ISPOR Conjoint Analysis Experimental Design Good Research Practices Task Force. Value Health. 2013;16(1):3–13. doi: 10.1016/j.jval.2012.08.2223. https://linkinghub.elsevier.com/retrieve/pii/S1098-3015(12)04162-9 .S1098-3015(12)04162-9 [DOI] [PubMed] [Google Scholar]
- 27.Cunningham CE, Walker JR, Eastwood JD, Westra H, Rimas H, Chen Y, Marcus M, Swinson RP, Bracken K. Modeling mental health information preferences during the early adult years: a discrete choice conjoint experiment. J Health Commun. 2014 Apr;19(4):413–40. doi: 10.1080/10810730.2013.811324. https://europepmc.org/abstract/MED/24266450 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Phillips EA, Himmler SF, Schreyögg J. Preferences for e-mental health interventions in Germany: a discrete choice experiment. Value Health. 2021 Mar;24(3):421–30. doi: 10.1016/j.jval.2020.09.018. https://linkinghub.elsevier.com/retrieve/pii/S1098-3015(20)34465-X .S1098-3015(20)34465-X [DOI] [PubMed] [Google Scholar]
- 29.Phillips EA, Himmler S, Schreyögg J. Preferences of psychotherapists for blended care in Germany: a discrete choice experiment. BMC Psychiatry. 2022 Feb 12;22(1):112. doi: 10.1186/s12888-022-03765-x. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/s12888-022-03765-x .10.1186/s12888-022-03765-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schwientek AK, Braun P, Apolinário-Hagen J, Loerbroks A, Guthardt L. Formative qualitative research on the development of a discrete choice experiment on e-mental-health information preferences and needs among prospect healthcare providers. OSF Registries. 2021. Aug 19, [2024-09-10]. https://osf.io/kemw8 .
- 31.Braun P, Apolinário-Hagen J, Vomhof M, Stehl S, Icks A, Angerer P, Loerbroks A. Informing future healthcare providers about eMental health services: a discrete choice experiment on preferences regarding information strategies among German-speaking medical students (preregistration) Internet Archive. 2022. Oct 22, [2024-09-01]. https://archive.org/details/osf-registrations-2s9u8-v1 .
- 32.Bridges JF, Hauber AB, Marshall D, Lloyd A, Prosser LA, Regier DA, Johnson FR, Mauskopf J. Conjoint analysis applications in health--a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011 Jun;14(4):403–13. doi: 10.1016/j.jval.2010.11.013. https://linkinghub.elsevier.com/retrieve/pii/S1098-3015(10)00083-5 .S1098-3015(10)00083-5 [DOI] [PubMed] [Google Scholar]
- 33.Hollin IL, Craig BM, Coast J, Beusterien K, Vass C, DiSantostefano R, Peay H. Reporting formative qualitative research to support the development of quantitative preference study protocols and corresponding survey instruments: guidelines for authors and reviewers. Patient. 2020 Feb;13(1):121–36. doi: 10.1007/s40271-019-00401-x.10.1007/s40271-019-00401-x [DOI] [PubMed] [Google Scholar]
- 34.Mayring P. Qualitative Inhaltsanalyse: Grundlagen und Techniken. Langensalza, Germany: Beltz Publishing; 2015. [Google Scholar]
- 35.Braun P, Schwientek AK, Angerer P, Guthardt L, Icks A, Loerbroks A, Apolinário-Hagen J. Investigating information needs and preferences regarding digital mental health services among medical and psychology students in Germany: a qualitative study. Digit Health. 2023 May 25;9:20552076231173568. doi: 10.1177/20552076231173568. https://journals.sagepub.com/doi/10.1177/20552076231173568?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub0pubmed .10.1177_20552076231173568 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Dederichs M, Weber J, Pischke CR, Angerer P, Apolinário-Hagen J. Exploring medical students' views on digital mental health interventions: a qualitative study. Internet Interv. 2021 Sep;25:100398. doi: 10.1016/j.invent.2021.100398. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(21)00038-5 .S2214-7829(21)00038-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dederichs M, Nitsch FJ, Apolinário-Hagen J. Piloting an innovative concept of e-mental health and mHealth workshops with medical students using a participatory co-design approach and app prototyping: case study. JMIR Med Educ. 2022 Jan 10;8(1):e32017. doi: 10.2196/32017. https://mededu.jmir.org/2022/1/e32017/ v8i1e32017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Wolcott MD, Lobczowski NG. Using cognitive interviews and think-aloud protocols to understand thought processes. Curr Pharm Teach Learn. 2021 Feb;13(2):181–8. doi: 10.1016/j.cptl.2020.09.005.S1877-1297(20)30302-6 [DOI] [PubMed] [Google Scholar]
- 39.Collins LM, Dziak JJ, Li R. Design of experiments with multiple independent variables: a resource management perspective on complete and reduced factorial designs. Psychol Methods. 2009 Sep;14(3):202–24. doi: 10.1037/a0015826. https://europepmc.org/abstract/MED/19719358 .2009-12975-002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kuhlfeld WF. Marketing research methods in SAS: experimental design, choice, conjoint, and graphical techniques. SAS Institute Inc. 2010. Oct 1, [2023-08-27]. https://support.sas.com/techsup/technote/mr2010.pdf .
- 41.Bech M, Gyrd-Hansen D. Effects coding in discrete choice experiments. Health Econ. 2005 Oct;14(10):1079–83. doi: 10.1002/hec.984. [DOI] [PubMed] [Google Scholar]
- 42.Dutheil F, Pereira B, Moustafa F, Naughton G, Lesage FX, Lambert C. At-risk and intervention thresholds of occupational stress using a visual analogue scale. PLoS One. 2017;12(6):e0178948. doi: 10.1371/journal.pone.0178948. https://dx.plos.org/10.1371/journal.pone.0178948 .PONE-D-15-02672 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Johnson R, Orme B. Getting the most from CBC. Sawtooth Software, Inc. 2003. [2023-08-27]. https://sawtoothsoftware.com/resources/technical-papers/getting-the-most-from-cbc .
- 44.Mühlbacher A, Johnson FR. Choice experiments to quantify preferences for health and healthcare: state of the practice. Appl Health Econ Health Policy. 2016 Jun;14(3):253–66. doi: 10.1007/s40258-016-0232-7.10.1007/s40258-016-0232-7 [DOI] [PubMed] [Google Scholar]
- 45.Swait J, Louviere J. The role of the scale parameter in the estimation and comparison of multinomial logit models. J Mark Res. 2018 Dec 20;30(3):305–14. doi: 10.1177/002224379303000303. [DOI] [Google Scholar]
- 46.Shorey S, Chan V, Rajendran P, Ang E. Learning styles, preferences and needs of generation Z healthcare students: scoping review. Nurse Educ Pract. 2021 Nov;57:103247. doi: 10.1016/j.nepr.2021.103247.S1471-5953(21)00283-3 [DOI] [PubMed] [Google Scholar]
- 47.Hertling SF, Back DA, Eckhart N, Kaiser M, Graul I. How far has the digitization of medical teaching progressed in times of COVID-19? A multinational survey among medical students and lecturers in German-speaking central Europe. BMC Med Educ. 2022 May 20;22(1):387. doi: 10.1186/s12909-022-03470-z. https://bmcmededuc.biomedcentral.com/articles/10.1186/s12909-022-03470-z .10.1186/s12909-022-03470-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ogut E, Senol Y, Yildirim FB. Do learning styles affect study duration and academic success? Eur J Anat. 2017;21(3):235–40. http://www.eurjanat.com/web/paper.php?id=170006eo . [Google Scholar]
- 49.Newton PM, Najabat-Lattif HF, Santiago G, Salvi A. The learning styles neuromyth is still thriving in medical education. Front Hum Neurosci. 2021;15:708540. doi: 10.3389/fnhum.2021.708540. https://europepmc.org/abstract/MED/34456698 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. London, UK: Pearson; 1985. [Google Scholar]
- 51.Shaffer VA, Zikmund-Fisher BJ. Narratives in decision aids: a controversy. In: Lucius-Hoene G, Holmberg C, Meyer T, editors. Illness Narratives in Practice: Potentials and Challenges of Using Narratives in Health-Related Contexts. Oxford, UK: Oxford University Press; 2018. [Google Scholar]
- 52.Shaffer VA, Focella ES, Hathaway A, Scherer LD, Zikmund-Fisher BJ. On the usefulness of narratives: an interdisciplinary review and theoretical model. Ann Behav Med. 2018 Apr 19;52(5):429–42. doi: 10.1093/abm/kax008. https://europepmc.org/abstract/MED/29684135 .4921125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Dederichs M, Weber J, Muth T, Angerer P, Loerbroks A. Students' perspectives on interventions to reduce stress in medical school: a qualitative study. PLoS One. 2020;15(10):e0240587. doi: 10.1371/journal.pone.0240587. https://dx.plos.org/10.1371/journal.pone.0240587 .PONE-D-20-12633 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Groene OR, Huelmann T, Hampe W, Emami P. German physicians and medical students do not represent the population they serve. Healthcare (Basel) 2023 Jun 06;11(12):1662. doi: 10.3390/healthcare11121662. https://www.mdpi.com/resolver?pii=healthcare11121662 .healthcare11121662 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Apolinário-Hagen J, Harrer M, Dederichs M, Fritsche L, Wopperer J, Wals F, Loerbroks A, Lehr D, Salewski C, Angerer P, Ebert DD. Exploring the influence of testimonial source on attitudes towards e-mental health interventions among university students: four-group randomized controlled trial. PLoS One. 2021;16(5):e0252012. doi: 10.1371/journal.pone.0252012. https://dx.plos.org/10.1371/journal.pone.0252012 .PONE-D-20-22489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Paganin G, Apolinário-Hagen J, Simbula S. Introducing mobile apps to promote the well-being of German and Italian university students. A cross-national application of the Technology Acceptance Model. Curr Psychol. 2022 Oct 27;:1–12. doi: 10.1007/s12144-022-03856-8. https://europepmc.org/abstract/MED/36320558 .3856 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Aulenkamp J, Mikuteit M, Löffler T, Schmidt J. Overview of digital health teaching courses in medical education in Germany in 2020. GMS J Med Educ. 2021;38(4):Doc80. doi: 10.3205/zma001476. https://europepmc.org/abstract/MED/34056069 .zma001476 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Choice-making behavior–lexicographic scores.
Willingness to pay for digital mental health interventions.
Results of the complete sample analysis.
Further information on latent class analysis.
Data Availability Statement
The data sets generated during and analyzed during this study are available from the corresponding author on reasonable request.