

Abstract
Six years ago, we published a paper describing the Society of Behavioral Medicine’s (SBM) health policy organizational leadership structure and policy initiatives. The purpose of the current paper is to provide an update on changes in the infrastructure and new policy initiatives that have been developed since 2017. We review each of the policy leadership arms of SBM including details of the work of each and goals for the future. The SBM engages in several health policy advocacy efforts through their Advocacy Council and Position Statements Committee. The Advocacy Council launched the Health Policy Ambassador Program in 2020. The Ambassador Program serves to train members to develop longer-term relationships with legislative staff around key policy priority areas. The Position Statements Committee is responsible for overseeing the development and dissemination of health policy position statements. Both groups work together and with partner organizations to increase the impact of our science. Over the last 6 years, developing a stronger infrastructure and implementing metrics for progress such as tracking social media engagement has helped to move SBM’s policy agenda forward. The work of the policy-related leadership teams can serve as a model for other organizations who are interested in further developing their policy advocacy efforts.
Keywords: Policy advocacy, Health policy
Over the past 6 years, Society of Behavioral Medicine has significantly expanded its policy advocacy work through the development and dissemination of position statements and through the implementation of our Health Policy Ambassador Program.
Implications.
Practice: Policy efforts can substantially improve the implementation of evidence-based interventions into systems of care and SBM’s health policy advocacy efforts can help to support these efforts.
Policy: SBM has built a policy advocacy infrastructure that trains members to build relationships with legislative staffers and write position statements for policymakers.
Research: Future research should be aimed at better measuring the impact of health policy advocacy efforts.
INTRODUCTION
Federal policies influence social determinants of health, including healthcare access, access to healthy food, and opportunities for physical activity, all of which affect health behavior and health inequities [1]. Given the connections between health behavior, policy, and social determinants of health, the Society of Behavioral Medicine (SBM) developed a training and policy advocacy infrastructure to increase the degree to which behavioral science informs health policy over the past decade [2]. Six years ago, members of SBM published a paper providing an update on the Society’s health policy activities and initiatives [3]. At that time, SBM’s advocacy efforts were in a nascent stage and the focus was on developing an infrastructure to develop and disseminate health policy position statements [3]. Since then, SBM has created additional structures to expand our policy advocacy efforts. In this paper, we provide an update on the activities of our Advocacy Council (formerly the Health Policy Council) and our Position Statements Committee (formerly the Health Policy Committee) and describe our leadership structures and models that have increased our impact. Our overarching goal is to have a roadmap for other organizations who envision future work in health policy advocacy.
METHOD
The following section outlines recent changes to SBM’s overall organizational structure and then describes updates to our main policy advocacy groups within SBM: the Advocacy Council and the Position Statements Committee.
Changes to SBM’s overall organizational structure
When the 2017 paper was published [3], the Health Policy Council primarily oversaw the policy-related work of other SBM committees/councils, whereas the Health Policy Committee led the development and dissemination of SBM’s position statements. The Civic and Public Engagement Committee led responses to public comments about these position statements and facilitated dissemination via social media while the Scientific and Professional Liaison Council (SPLC) focused on developing partnerships with other organizations to increase the impact of SBM’s policy objectives. As part of strategic planning in April 2022, SBM members voted on a new leadership structure (see Fig. 1). We now have the Advocacy Council (previously the Health Policy Council), which is primarily responsible for overseeing our newly organized Health Policy Ambassador Program. The Advocacy Council has nested within it the Position Statements Committee (previously the Health Policy Committee), which is responsible for developing and disseminating our health policy position statements, and the Organizational Partnerships Committee (previously the SPLC), which oversees our relationships with partner organizations (see Fig. 2). The new structure provides a central location to streamline the advocacy process and enhance advocacy collaboration.
Fig 1.
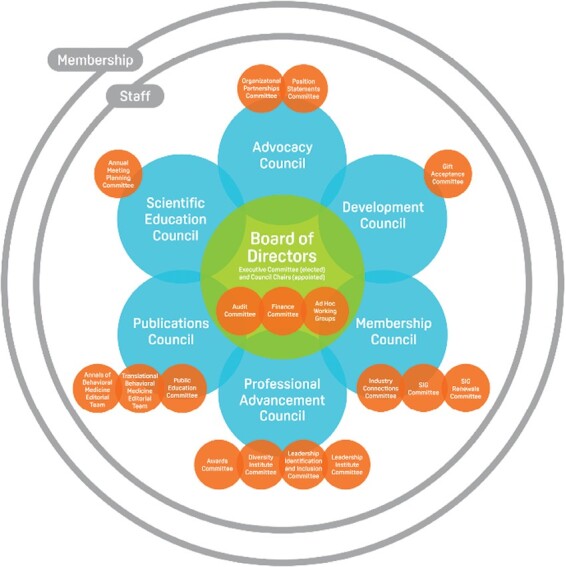
SBM’s organizational leadership structure.
Fig 2.
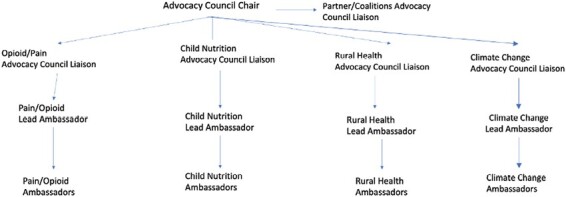
Organization structure of the Advocacy Council.
Advocacy Council: creation of the Health Policy Ambassador Program
During Dr. Sherry Pagoto’s presidency and Dr. Marian Fitzgibbon’s tenure as Health Policy Council (now Advocacy Council) Chair, SBM consulted a health policy specialist to analyze our policy work and provide feedback for developing a strategic plan. This strategic plan was implemented via the creation of the Health Policy Ambassador Program when Dr. Joanna Buscemi became chair of the Advocacy Council in 2019. The main goal of the strategic plan was to develop an advocacy arm of SBM by building long-term relationships with legislative staffers on issues aligned with SBM’s mission.
Prior to the Health Policy Ambassador Program, SBM Board of Directors members traveled annually to Capitol Hill for a 1-day visit and introduced issues to many legislative offices. While these Hill visits were undoubtedly meaningful for Board members, the meetings were too infrequent to build longer-term relationships with policymakers. The purpose of the newly formed Health Policy Ambassadors’ Program was to help SBM—and our members’ evidence-based science—move from being a visitor in lawmakers’ offices to becoming an integral part of lawmakers’ decision-making through ongoing contact and relationship building. Ambassadors are SBM members and experts on a specific topic, and/or live in the relevant policymaker’s district. Ambassadors build relationships with policymakers and their staff, engaging them to make evidence-based decisions on specific health policies. Interactions between ambassadors and legislative staff may include emails, inviting the policymaker to their institutions, and visiting the policymaker at their district or DC office. Ambassadors facilitate two-way education with lawmakers: They educate lawmakers on relevant scientific evidence from the field of behavioral medicine. Likewise, lawmakers educate ambassadors on specific policy issues and the policymaking process. The strategic plan included identifying policy priority areas, matching members to legislators across the country, and developing training materials. These steps were completed before the official launch of the Health Policy Ambassador Program in June 2020.
When the Ambassador Program was launched, the key policy priorities included (i) to educate lawmakers about evidence-based research to ensure that children have access to healthy foods, (ii) to educate lawmakers about evidence-based interventions to best manage pain and combat opioid misuse, and (iii) to educate lawmakers about the unique healthcare needs of rural populations and evidence-based strategies to improve their health outcomes and quality of life. During the 2022 SBM annual meeting, a fourth priority area was added to educate lawmakers about evidence-based interventions to mitigate climate change and its adverse effects on health outcomes, particularly for vulnerable populations. When the Ambassador Program began in 2020, we initiated efforts with our first three priority areas and activated a dozen Ambassadors in nine states across the country. Now, we have more than doubled this number of Ambassadors (n = 25) across 17 states and have added the climate change priority area to our advocacy efforts. To date, we have had 293 contacts (e.g., email, videoconferences, and social media tags) with legislative staff across all priority areas. Over the past 2 years, we expanded our advocacy efforts through the Ambassador Program by identifying an organizational structure within the Advocacy Council that will provide long-term growth. For example, we identified a liaison for each priority area group who serves as a member of the council. Their job is to monitor the activity of the Ambassador subgroups and to encourage monthly email contact and quarterly video/in-person contact. They also provide monthly feedback to the Council. We also identified a Lead Ambassador for each health policy priority area who is responsible for sending monthly email content on each area to the larger group to facilitate the monthly email touch point. The Ambassadors are responsible for sending the monthly email and for contributing to the development of the talking points for the next quarterly meetings. Also, Ambassadors have developed and published position statements through the Position Statements Committee (see Fig. 1) pipeline. Once approved, position statements are used as talking points for future meetings with legislative staffers. We have also expanded our work by partnering with similarly oriented organizations (e.g., Center for Science in the Public Interest, Rural Policy Research Institute, APA Society for Health Psychology, American Physical Therapy Association, and Voice for Non-Opioid Choices) and by joining coalitions (e.g., National Alliance for Nutrition and Activity, HER-NOPREN COVID-19 School Nutrition Working Group, MAT Act Campaign, and ecoAmerica) that are working on similar key priority issues. A liaison from the Organizational Partnerships Committee attends the monthly Advocacy Council meeting to share relevant partner updates; the liaison also sends emails to Ambassadors with partner content that is useful for creating talking points and email touch points. Our partners frequently sign on to our position statements. As a relatively small organization, these partnerships and coalitions help to amplify our messages to a wider audience, and can provide additional content expertise and advocacy training (e.g., The climate change Ambassadors completed training provided by ecoAmerica). We have also signed onto or endorsed over 30 statements/letters developed by partner organizations that have been sent to members of Congress and other government officials.
COVID-19 response
Over the course of our advocacy work, we learned that it is helpful to develop talking points that link to issues that are most pressing to legislative staff. Certainly, no issue has been more pressing over the last 3 years than the COVID-19 pandemic. The Ambassador Program was set to launch in March 2020, but we decided to put the launch on hold “until the pandemic was over.” In May 2020, it became clear that the pandemic was here to stay for the foreseeable future. While our priority areas were already set, we quickly realized that each of these areas was immediately impacted, such that already existing problems were exacerbated by the pandemic. The Advocacy Council and Ambassador groups had to be nimble and align their talking points to how the pandemic was impacting their specific priority areas. For example, the child nutrition group focused on how the pandemic was impacting child food insecurity and expanding government funding nutrition programs to mitigate the harm caused by disruptions in the school meal program. The opioid/pain management and rural health groups worked on talking points on expanding telehealth access and coverage for providers so that services were not interrupted by pandemic-related disruptions. These links to COVID-19 allowed us to appeal to timely issues that aligned with legislative priorities and helped us to connect to their policy agendas. See all COVID-19-related position statements here.
Challenges and success stories of the Ambassador Program
While the Ambassador Program has been feasible and productive, we have faced some challenges. One challenge is finding the correct contact information for the health policy staff for each Senator or Representative and making initial contact with the correct person. While all constituents can email their Senators or Representatives or complete an online form from their website, these types of contacts typically generate automated responses that do not facilitate a long-term relationship. We find that having direct contact information for health policy staffers is necessary for relationship building. Another challenge is maintaining regular monthly contact with our legislators. We hope that the structure of the Council and the role of the Lead Ambassador will continue to facilitate our volunteers in maintaining this regular contact.
Another limitation is that it is difficult to measure the impact of our work. While measuring impact is challenging with policy work, we have had some promising early successful outcomes. First, SBM has been sought out by members of Congress to endorse proposed bills that are relevant to our mission. For example, SBM endorsed Senator Elizabeth Warren’s Research Funding and NIH Funding Acts, Senator Kristen Gillibrand’s Ensuring Nutrition for America’s Students Act, and Senator Pat Toomy’s IMPROVE Addiction Care Act. As previously mentioned, we also track each contact our Ambassadors have with their staffers and have had over 293 contacts since the program began in 2020. Finally, we measure success from our Ambassadors’ stories. For example, as one rural health Ambassador commented, “The legislative staffer asked for some evidence about telehealth, which I found and shared with them. A month later, the legislator’s e-newsletter described a new telehealth bill they had introduced, and it included my recommendation. It was satisfying to see my efforts pay off.” Another Ambassador for the pain/opioid health policy priority area commented, “I had a call with the 2 congressional aides. They were extremely helpful and passionate about our work. For my state, coverage for telehealth will end 12/31/2020. They will work to develop a bill to provide for telehealth coverage (video and phone) at a reimbursement rate similar to in person visits.” These are examples of the many success stories we hear from our Ambassadors. Many of our Ambassador’s legislative staff initiate contact to ask questions about our science base to inform the development of Bills, which is further evidence that our relationship building is supporting the science-to-policy translation that is key to the overall goals of the program. Prior to the development of the Ambassador Program, we did not have two-way communication and success stories like this, which speaks to the potential impact of the program.
Future directions for Advocacy Council
Behavioral scientists do not usually receive any formal training on legislative outreach or how to translate their work for legislators [4, 5]. Such training is critical to influence and advance policies that can help maximize the effect of behavioral programs and interventions. It is also a point of leverage to reduce research to policy translation gaps in behavioral medicine. In an effort to conceptualize future council efforts, Figueroa and Verma developed a framework (see Fig. 3) that can be leveraged as a tool of thought for constituent driven, evidence-based health policy advocacy [6]. The Constituent-driven Policy Advocacy Model (CPAM) comprises three primary domains for policymakers, scientists, and/or community advocates. Within the research domain, an emphasis on advocacy and community engagement, combined with evidence synthesis and scientific communication is critical to inform policy changes, lest behavioral medicine research remains trapped in scientific journals. Within the policymaking domain, a new model for “engaged” policymaking is needed and should involve more engagement between lawmakers and constituents, ensuring more sensitive, targeted, and equitable results. Within the advocacy domain, the emphasis is on building the capacity to assess needs, form collaborations and coalitions with assertive leadership, as well as identify a policy champion invested in a shared policy priority area with strong constituent support [6]. Through this lens, council leaders would be able to advocate for policies centering equity, evidence, and nonpartisanship stances, as well as engage SBM members in a standardized fashion to maximize collective impact. Given SBM’s growing advocacy presence, this framework serves as a guide for the SBM Advocacy Council and Ambassadors as constituents advocating for key health policy priorities and contributing to rigorous research in these areas concurrently.
Fig 3.
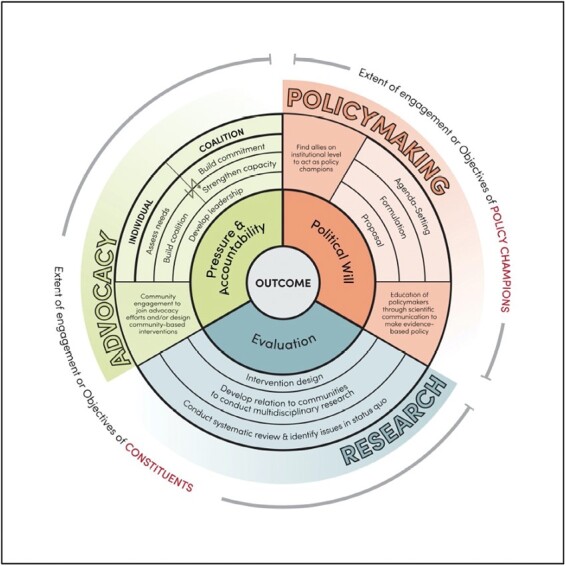
Constituent-driven Policy Advocacy Model [6].
Position Statements Committee updates
At the time of our update 6 years ago, we had published 15 health policy position statements. Since then, our total number has increased to 58, 33 of which were published in the past 6 years (January 2018–January 2023). Position statements published during this time included relevant and timely topics such as anti-racism, COVID-19, cardiovascular disease, and substance misuse.
Proposal and composition processes
The current model for review and publication of position statements within the Position Statements Committee includes multiple phases of review. This helps ensure that authorship teams receive detailed feedback and expert advising as they craft their position statements. During the proposal phase, which is the initial phase of submission for SBM position statements, authors submit a preliminary position statement proposal that outlines a brief summary statement, the problem being addressed, the current policy or policies in this space, and specific policy recommendations. This proposal is reviewed by the committee, which gives detailed feedback on the proposal. If the committee approves the proposal, it moves forward to the composition model phase where authors are paired with a liaison as summarized in the subsequent section. During the composition phase, authorship teams work closely with their liaison to draft a position statement that is focused on behavioral medicine and a specific set of policy recommendations to improve its effectiveness at reaching legislators. Once authors go through these two phases, their position statement moves to the final stage of review and approval by the SBM Executive Committee and then on to dissemination. During the dissemination phase, SBM authors partner with SBM staff to distribute this position statement widely through social media (Twitter and Facebook) and in partnerships and co-endorsements with other societies and organizations to expand reach.
Liaison model
A key feature integrated into the Position Statements Committee structure is the use of liaisons. The Position Statements Committee now pairs each authorship team of an approved position statement proposal with a liaison who serves as a standing or ad hoc member of the committee. This pairing ensures that each authorship team is working alongside someone on the committee with the expertise to guide them in writing their position statement, both in terms of content and policy expertise. The liaison provides feedback on the structure, content, and policy recommendations of the position statement to make sure it is optimally formatted to target the intended audience: policymakers. This model has led to the successful drafting and publishing of position statements across a number of policy topic areas with SBM and has supported authors who have little to no prior experience with policy work or writing position statements.
COVID-19 response
Given the need to devise specific social and behavioral health policies to mitigate COVID-19’s impacts on population health, the Position Statements Committee streamlined its policy position statement process for COVID-19-related statements and devised a new outreach approach to recruit more position statement authorship teams. First, we omitted the proposal step from the policy position statement process. Second, we sped up position statement review times (e.g., 1-month review time). Last, we conducted strategic outreach (e.g., targeted emails to the SBM’s Special Interest Group leadership with invitations to draft relevant, topical position statements, and meet with Position Statements Committee leadership) to draft position statements about time-sensitive COVID-19 topics. Before implementing these strategies, we piloted our efforts with the Health Equity Special Interest Group. After the successes of the pilot and release of two position statements (COVID-19 and Health Equity and COVID-19 and Rural Health) with the Health Equity Special Interest Group, we rolled out our streamlined process and outreach efforts. Specifically, we reached out to the larger list of Special Interest Groups leadership and the Ambassadors so that we could create and release more COVID-19-related position statements. The Position Statements Committee liaisons were instrumental in supporting these initiatives. These efforts serve as a model for future time-sensitive public health issues of importance.
These COVID-19-specific streamlined Position Statements Committee processes and outreach efforts resulted in 11f COVID-19-related position statements published between 2020 and 2021. Many of these statements applied a health equity lens to underscore existing social inequities that were exacerbated by the COVID-19 pandemic and included health-equity-specific policy recommendations. For example, position statements addressed food insecurity and federal food assistance programs, racial and ethnic and rural healthcare disparities, mental health, intimate partner violence, and telehealth for people with existing chronic conditions. All COVID-19-related health policy position statements can be found here. During this specific focus on COVID-19-related position statements, many SBM members delayed the release of their non-COVID-19 position statements so that we could prioritize the release of statements related to the COVID-19 pandemic. This “all-hands on deck” approach led by our Position Statements Committee, Special Interest Group leadership, and SBM membership at large led to the release of highly impactful, relevant, and timely COVID-19 position statements.
Updated dissemination strategies
The Position Statements Committee is focused on increasing the reach and impact of SBM’s position statements, in accordance with SBM’s Board of Director’s strategic visioning and planning activities. Prior dissemination efforts included disseminating position statements and infographics on social media, asking co-endorsing partners and authorship teams to post on social media (with prewritten examples of tweets), and including the position statement links in the SBM newsletter. They also included publishing position statements on the SBM website and emailing select position statements to congressional staff. While these prior efforts yielded some successes, they did not achieve sufficient reach and impact for this critically important policy work. Thus, we created a three-member dissemination strategy planning committee who worked to identify new dissemination strategies to complement existing ones.
Our new dissemination strategies have focused on maximizing existing resources and more strategic use of social media. Specifically, we swapped out infographics with optimized graphics with less text and one-sentence summaries and found that these optimized graphics have greater reach than our prior infographics. We now ask the lead author of the position statements to provide us with their university’s Twitter handles so that we can tag their institutions in tweets. We also encourage authors to share their position statements with institutional media contacts and to publish press releases if possible. We also are leveraging SBM’s Special Interest Groups to assist in dissemination efforts. For instance, during our monthly Position Statement Committee meetings, we map position statement topics onto the Special Interest Group areas of expertise, and upon release of the position statements, we invite relevant Special Interest Group leadership to disseminate the statements via their listservs and social media handles. We also are more intentional about leveraging the resources of our co-endorsing partners. Specifically, when developing example tweets, we add the co-endorsing partner Twitter handles to the sample tweets so that authorship teams can tag the organizations. We have revised our co-endorsement invitation emails to include language that the co-endorsers agree to disseminate the position statements via social media.
We also piloted collaborations with SBM “influencers” to share position statements. We review the Twitter profiles of SBM members and identify a subset (e.g., 5–10 people who have at least 5,000 followers or people who engage with the behavioral medicine Twitter handle frequently). We ask these “influencers” to share the position statement (depending on the content of the brief so that we are not repeatedly asking the same people to share). Collaborations with SBM “influencers” is strategic to not overburden them with requests to share position statements. We also have several dissemination strategies that will be implemented soon. These upcoming strategies include working with the Position Statement Committee liaison to identify additional legislators who may be interested in the topic, recirculating prior impactful position statements, and creating a calendar of health awareness months and post (or repost) position statements that map onto that particular topic and using health month-specific hashtags.
Success stories
With the addition in recent years of distribution of the position statements through social media, we have had some reported success stories of statements with a wider reach. Some of the highest impact position statements, to date, have included the following: (i) “Protect Abortion Rights,” which received 10,001 impressions on Twitter and 513 on Facebook and (ii) “Expand Telehealth for Bariatric Surgery,” which received 7,633 impressions on Twitter and 770 on Facebook. Another notable position statement, which touched on COVID-19, was “We Call for Equitable Healthcare during COVID-19 Pandemic,” which received 3,420 impressions on Twitter and 1,098 on Facebook. It should be noted these metrics refer to the official SBM account’s tweets, thus reach was likely higher with impressions from SBM members’ tweets.
Student mentorship program
In Fall 2021, the Positions Statements Committee launched a pilot student mentorship program to involve more SBM student members in the position statement writing process and to provide valuable health policy experience to interested students. The committee hosted an informational webinar for interested applicants and created a partnership with the SBM Student Special Interest Group to advertise the webinar and the program application process.
Six student mentees, including undergraduate and graduate students, were selected to participate in the pilot program for the 2021–2022 academic year. Students provided their priority interest areas to the committee using short keywords and attempts were made to match students to authorship teams writing briefs related to at least one of these topic areas. Mentors (lead authors of position statements) were solicited during the statement proposal phase. Mentors could opt-in to the mentorship program on the statement proposal form that is submitted by all lead authors, and in some cases, the chair of the Position Statements Committee also sent an email directly to the lead author asking if they were interested in mentoring a student. We saw a high rate of success with these personalized emails, and we plan to use this approach moving forward. When students were matched to a mentor, the committee chair facilitated introductions between the mentee and mentor, and the student joined the authorship team and assisted with drafting, writing, and revising the position statement; conducting literature reviews; formatting the brief; and taking meeting notes. As part of this program, a detailed guide was developed to lay out the student responsibilities and other author responsibilities and how to manage any conflict. As the pilot year wraps up, we plan to send out program evaluations to both mentees and mentors to explore how we can improve the mentorship program.
Future directions
Future directions of the Position Statements Committee include the following: (i) expanding the impact and reach of position statements and their recommended policy changes through broad dissemination of this work (e.g., op-eds, social media, etc.) and via stronger connections with partners who have substantial advocacy resources, (ii) facilitating a more streamlined connection between publishing position statements and connecting with legislators, (iii) more intentional growing of SBM’s Twitter audience (e.g., through following and interacting with accounts of policymakers, policy influencers, and media and journalist accounts), and (iv) growing the student mentorship program to help mentor students in policy work. To achieve these goals, the Position Statements Committee is undertaking formal partnerships with the Public Education Committee, the Advocacy Council, and utilizing the recently developed SciComm Toolkit developed by SBM.
Conclusions
SBM has made enormous strides in policy work in the last 13 years. Over the past 6 years specifically, SBM has significantly expanded their health policy advocacy work with a particular focus on relationship building with policymakers and their staff. With the implementation of the health policy strategic plan, we built the Ambassador Program which has continued to grow since its initial launch. Because we are an organization that covers a wide breadth of topic areas within behavioral medicine, we were strategic in selecting our key priority areas to keep our advocacy efforts as focused as possible. We also built a training and leadership infrastructure that will allow the program to be sustainable over time. Moving forward, the Advocacy Council will continue to find ways to facilitate the communication and relationship-building efforts between the Ambassadors and policymakers and will apply the CPAM [6] to future work. The Position Statements Committee has also continued to expand and grow over the last 6 years and was extremely nimble and prolific during the COVID-19 pandemic. The student mentorship program, developed during Dr. Akilah Dulin’s tenure, will serve to train and engage the next generation of health policy advocates so that the work can continue moving forward. Additionally, the Position Statements Committee continues to work toward more efficient and effective dissemination efforts so that the position statements reach even more stakeholders. Future work in this space will also involve continuing to partner with like-minded organizations and coalitions to find ways to collaborate and further the impact of our work. We will also work to further identify new methods for measuring the reach and impact of our efforts. Over the last several years, we have developed metrics such as number of position statements developed, social media engagement, and internet click data as well as Ambassador stories and interactions with legislative offices, we will continue to try to quantify our impact as much as possible moving forward. Overall, the policy advocacy work of SBM has grown exponentially over the past decade, and SBM leaders have plans to continue to grow this work in ways that expand the reach of our work to increase our impact on population health.
Call to Action
We ask that the members of SBM consider joining the organization’s policy advocacy efforts through any of the following actions:
1) Submit a position statement proposal on a topic that aligns with SBM’s mission and your own expertise.
2) Consider joining the Position Statements Committee or Advocacy Council.
3) Consider becoming a Health Policy Ambassador.
4) Help disseminate position statements on social media and to your local policymakers.
Given the broad expertise of the organization, SBM can continue to grow its impact in the policy advocacy space across the field of behavioral medicine. SBM has built the infrastructure to support member training and experience in this area, and with increased engagement, can further expand our impact in the policy space.
Contributor Information
Joanna Buscemi, DePaul University, Chicago, IL 60614, USA.
Roger Figueroa, Cornell University, Ithaca, NY 14850, USA.
Brooke M Bell, Tufts University, Princeton, NJ 08544, USA.
Akilah Dulin, Brown University, Providence, RI 02912, USA.
Megan Shen, Fred Hutchinson Cancer Center, Seattle, WA 98109, USA.
Kristin L Schneider, Rosalind Franklin University, North Chicago, IL 60064, USA.
Sherry Pagoto, University of Connecticut, Storrs, CT 06269, USA.
Marian Fitzgibbon, University of Illinois at Chicago, Chicago, IL 60608,USA.
Compliance with Ethical Standards
Conflicts of Interest: Joanna Buscemi, Roger Figueroa, Brooke M. Bell, Akilah Dulin, Megan Shen, Kristin L. Schneider, Sherry Pagoto, and Marian Fitzgibbon have no conflict of interest to report.
Human Rights: This article does not contain any studies with human participants performed by any of the authors.
Informed Consent: This study does not involve human participants and informed consent was therefore not required.
Welfare of Animals: This article does not contain any studies with animals performed by any of the authors.
REFERENCES
- 1. Emmons KM, Chambers DA. Policy implementation science – an unexplored strategy to address social determinants of health. Ethn Dis. 2021;31(1):133–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Estabrooks P, Pagoto S, Otten J, et al. The Society of Behavioral Medicine (SBM) and public policy advocacy: a call to action. Transl Behav Med. 2011;1(3):492–496. doi: 10.1007/s13142-011-0073-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Buscemi J, Bennett GG, Gorin SS, et al. A 6-year update of the health policy and advocacy priorities of the Society of Behavioral Medicine. Transl Behav Med. 2017;7(4):903–911. doi: 10.1007/s13142-017-0507-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Biglan A, Levin ME. Contextual analysis and the success of translational research. Transl Behav Med. 2016;6(1):160–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Dobbins M, Hanna SE, Ciliska D, et al. A randomized controlled trial evaluating the impact of knowledge translation and exchange strategies. Implement Sci. 2009;4(1):1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Figueroa R, Verma R. Constituent-driven health policy informed by policy advocacy literature. Transl Behav Med. 2023;13(5):ibac116. [DOI] [PubMed] [Google Scholar]