

Abstract
目的
评估患者上颌窦内衬黏膜上皮,即施耐德膜(SM)增厚的情况及其与上颌后牙区根尖周病变(PAL)的关系,以期为牙源性上颌窦炎的预防和治疗提供参考。
方法
回顾性分析符合纳入标准的301例患者554个上颌窦的锥形束计算机断层扫描(CBCT)影像学资料,以确定上颌后牙PAL与SM增厚的相关性。记录病理性黏膜增厚的病例数,并根据SM增厚的程度与类型进行分类。评估SM增厚与PAL的直径,PAL上缘与上颌窦底的波及关系及有PAL的患牙是否进行根管治疗之间的相关性。
结果
在上颌后牙区,当患者出现PAL时,SM增厚的检出率高于无PAL,并且PAL与SM增厚之间具有相关性。PAL各项检测指标与SM增厚程度相关性分析结果显示,CBCT根尖周指数(CBCT-PAI)PAL直径与SM增厚程度呈现正相关性,而PAL上缘与上颌窦底的3种不同波及关系、有PAL的患牙是否进行根管治疗与SM增厚程度不具有相关性。PAL各项检测指标与SM增厚类型相关性分析结果显示,有PAL的患牙是否进行根管治疗与SM增厚类型之间具有相关性,而PAL直径和PAL上缘与上颌窦底的3种不同波及关系与SM增厚类型不具有相关性。
结论
上颌后牙PAL与SM增厚密切相关,PAL直径与SM增厚程度呈正相关;有PAL且进行过根管治疗的患牙常见出现SM息肉型增厚,PAL上缘与上颌窦底的波及关系不影响SM的发展。
Keywords: 施耐德膜增厚, 根尖周病变, 锥形束计算机断层扫描
Abstract
Objective
This study aimed to evaluate the thickening of sinus membrane, which is also named Schneiderian membrane (SM), in patients and its relationship with periapical lesions (PAL) in the posterior maxillary region to provide reference for the prevention and treatment of odontogenic maxillary sinusitis.
Methods
A retrospective analysis was conducted on 554 cone beam computed tomography (CBCT) imaging data of maxillary sinuses from 301 patients who met the inclusion criteria to determine the correlation between PAL and SM thickening in the posterior maxillary region. Cases of pathological SM were recorded and classified on the basis of the degree and type of SM thickening. The correlation between SM thickening and the diameter of PAL, the relationship between the upper edge of PAL and the maxillary sinus floor, and its relationship with whether affected teeth with PAL undergo root canal treatment were evaluated.
Results
The detection rate of SM thickening in patients with PAL was significantly higher than in those without PAL, so PAL was correlated with SM thickening. Analysis on the correlation between PAL detection indicators and SM thickening degree showed that SM thickening degree was positively correlated with PAL diameter (cone beam computed tomography-periapical index) and not correlated with the three spread effects between the upper edge of PAL and the maxillary sinus floor, as well as whether the teeth with PAL undergo root canal treatment. The correlation analysis between PAL detection indicators and SM thickening types showed that whether the teeth with PAL undergo root canal treatment was not correlated with SM thickening types, and the diameter of PAL, the three spread effects between the upper edge of PAL, and the maxillary sinus floor were not correlated with SM thickening types.
Conclusion
The PAL of posterior maxillary teeth is closely related to SM thickening, and the diameter of PAL is positively correlated with the degree of SM thickening. Patients with PAL who have undergone root canal treatment often exhibit SM polyp thickening. In addition, the relationship between the upper edge of PAL and the maxillary sinus floor does not affect the possibility of SM development.
Keywords: Schneiderian membrane thickening, periapical lesions, cone beam computed tomography
上颌窦是位于上颌骨体内的锥形空腔,衬有一层黏膜,牢固地黏附在骨膜上,称为施耐德膜(Schneiderian membrane,SM)[1]。这是一种假复层纤毛柱状上皮,与呼吸道上皮的黏膜具有相似的特征,正常情况下膜的厚度为(0.30±0.17)mm,当该黏膜受到感染或炎症刺激时,SM厚度会增加[2],SM厚度超过2 mm被认为是病理性的黏膜增厚[3]。牙源性上颌窦炎(odontogenic maxillary sinusitis,OMS)指的是牙相关因素引起的上颌窦炎。由于上颌窦底部与上颌后牙的根部相邻,且二者由同一神经支配,上颌后牙根尖周病变(periapical lesions,PAL)可通过骨髓、血管和淋巴管扩散到上颌窦,从而引起上颌窦黏膜炎,进一步可发展为OMS[4]。PAL是指细菌感染侵入牙髓导致牙根尖周围的炎症性病变,慢性炎症反应通常无症状,绝大部分都会导致根尖周围骨吸收,在影像学中出现PAL[5]–[6]。PAL的炎症反应通常是一种有效的免疫屏障,防止感染从根管蔓延到牙槽骨和其他身体部位。OMS患者常表现为口腔颌面部的持续肿痛,甚至出现头痛,给患者带来了不同程度的痛苦[7]。在临床上OMS常因为诊断不足而被忽视,最终导致患者治疗失败[6]。
目前,锥形束计算机断层扫描(cone beam computed tomography,CBCT)已被证明是鉴定牙髓相关的OMS不可或缺的工具,是准确评估上颌后牙区复杂解剖结构与上颌窦内相关复杂结构相关性的理想方式[8]。近年来,随着CBCT的广泛使用,有研究[9]–[10]发现SM增厚的严重程度与上颌后牙PAL的程度密切相关,虽然人们非常关注PAL对SM增厚的影响,但是至今为止并没有充分重视PAL引起的SM增厚在影像学上的意义以及其后果。此外,在临床实践中也缺乏关于PAL与SM增厚之间确凿相关性的研究。
综上所述,本研究使用CBCT来评估SM增厚等情况及其与上颌后牙区PAL的相关性,分析在PAL存在的情况下SM增厚程度与类型的变化,为OMS的预防和治疗方向提供参考。
1. 材料和方法
1.1. 研究对象
收集2019年1月到2021年12月于大连市口腔医院影像科拍摄CBCT的患者影像资料,随机选择500例患者,得到所有患者的双侧共1 000个上颌窦CBCT图像样本,最终符合纳入标准的有301例患者,共554个上颌窦样本。其中女性160例,男性141例,年龄18~82岁,均值(39.73±15.63)岁。
纳入标准:1)CBCT影像清晰,伪影少,无变形;2)患者年龄≥18岁;3)纳入者至少一侧上颌窦完整且不存在牙齿缺失(第三磨牙缺失除外),能够清楚显示所有上颌第一前磨牙、第二前磨牙、第一磨牙和第二磨牙,牙根发育完整,并排除因第三磨牙阻生引起的SM增厚;4)非手术进行中的患者。
排除标准:1)有一个或多个上颌种植体的患者;2)任何中度、重度牙槽骨吸收,疑似骨内病变;3)被评估为急性创伤性损伤而进行扫描的患者;4)修复体或正畸固位体影响前磨牙和磨牙区图像质量的病例;5)由于急慢性上颌窦炎、上颌窦慢性阻塞性炎症、上颌窦囊肿及肿瘤等非牙源性SM增厚的患者。
1.2. 研究方法
1.2.1. CBCT图像采集
所有患者均使用Kavo 3D eXam扫描仪进行扫描。CBCT图像的采集参数为110 kV和3 mA,切片厚度为0.25 mm,由专业的放射科主治医师进行。图像由横断面重建而来,得到冠状位和矢状位,形成3D图像,以评估上颌窦及其与上颌后牙的关系,同时对研究人员的观测方法及评价标准进行规范。记录每个样本的性别、年龄、是否存在SM增厚、是否存在PAL;对于存在上颌后牙PAL及与病变相关的SM增厚的患者,记录SM增厚的程度与SM的类型、患牙的类型、CBCT根尖周指数(CBCT-periapical index,CBCT-PAI)、PAL上缘与上颌窦底之间的波及关系,同时记录有PAL的患牙是否进行根管治疗。所有测量、评估重复两次,间隔1个月。计算两次测量值的平均值,并进行统计分析。
1.2.2. 评估SM增厚的程度与类型
有无SM增厚:只要存在一个牙根根尖区对应的SM厚度值大于2 mm,则记为该样本存在SM增厚,反之记为无SM增厚。
SM增厚程度:根据Aksoy等[11]的分级标准,对各样本的SM增厚情况进行分级[12]。正常SM厚度:0~2 mm;轻度SM增厚:2~5 mm;中度SM增厚:5~10 mm;重度SM增厚:>10 mm。
SM增厚类型:根据Aksoy等[11]的研究,将SM增厚的类型分为三型。1)扁平型:窦底黏膜水平增厚(图1A、B);2)息肉型:窦底黏膜圆顶状增厚(图1C、D);3)混浊型:完全上颌窦混浊(图1E、F)。
图 1. 施耐德膜的增厚类型.

Fig 1 Type of SM thickening
A:矢状面SM扁平型增厚;B:冠状面SM扁平型增厚;C:矢状面SM息肉型增厚;D:冠状面SM息肉型增厚;E:矢状面SM混浊型增厚;F:冠状面SM混浊型增厚。箭头示增厚的SM。
1.2.3. 评估PAL及PAL存在的各项检测指标
有无PAL:当至少一颗上颌后牙在根尖周围显示存在低密度影像时,记录到有“PAL”即根尖周病变,反之记为无PAL。
PAL直径:采用Estrela等[12]提出的方法,应用CBCT-PAI进行PAL直径的测量。CBCT-PAI分值分别在轴位、冠状位和矢状位3个角度评估,评分由最大病灶范围决定,以mm为单位测量PAL的最大直径,精确度为0.01 mm,并使用以下内容进行评级:0级,完整的根尖周骨结构;1级,根尖周射线透光直径0.5~1 mm;2级,根尖周射线透光直径1~2 mm;3级,根尖周射线透光直径2~4 mm;4级,根尖周射线透光直径4~8 mm;5级,根尖周射线透光直径>8 mm。
PAL上缘与上颌窦底之间的波及关系:采用Lu等[13]的3级评分法评估PAL的最上边界与上颌窦底之间的距离。在矢状位及冠状位测量上颌后牙PAL与上颌窦底的波及关系,分为3个类型。OS型:PAL上缘与上颌窦底存在一定距离;CO型:PAL上缘仅接触上颌窦底但未突破;IS型:PAL上缘突入上颌窦底,上颌窦底影像不连续。当多个牙根均存在PAL时,测量与上颌窦底距离更近的PAL病变(图2)。
图 2. PAL上缘与上颌窦底之间的波及关系.

Fig 2 The relationship between the upper edge of PAL and the maxillary sinus floor
A:矢状面OS型;B:冠状面OS型;C:矢状面CO型;D:冠状面CO型;E:矢状面IS型;F:冠状面IS型。箭头示PAL上缘。
有PAL的患牙是否进行根管治疗:1)未经根管治疗存在PAL(原发性牙髓感染来源的根尖周病变):根管内未见高密度影像;2)根管治疗后存在PAL(继发性牙髓感染来源的根尖周病变):根管内可见高密度影像(图3)。此研究为横断面研究,根管治疗后的患牙仍存在PAL,无法确定是否为根管治疗失败,有可能此时的骨质尚处于修复阶段,但根尖周病变尚存。
图 3. 有PAL的患牙是否进行根管治疗.
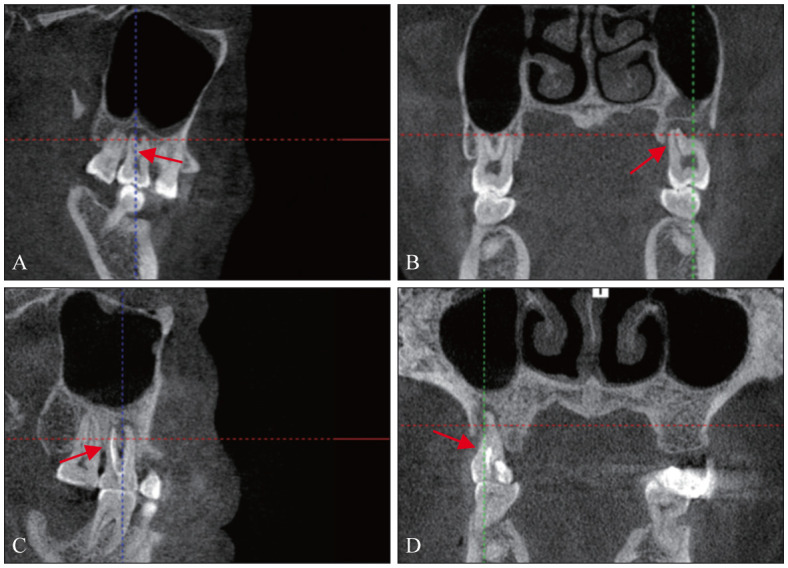
Fig 3 Teeth with PAL undergo root canal treatment were evaluated
A:矢状面未经根管治疗存在PAL;B:冠状面未经根管治疗存在PAL;C:矢状面根管治疗后存在PAL;D:冠状面根管治疗后存在PAL。箭头示根管内影像。
1.3. 统计学分析
使用Excel建立数据库,采用SPSS 26.0统计学软件进行分析,对数据进行描述性分析,并使用卡方检验或者Fisher确切概率法,等级资料相关性分析采用Spearman相关系数。所有分析均采用显著性水平α=0.05,P<0.05为差异有统计学意义。
2. 结果
2.1. SM增厚与PAL
在301例患者中,平均SM的厚度为3.12 mm,有179例患者(59.5%)中出现单侧或双侧上颌窦SM增厚。其中52例(17.3%)出现双侧上颌窦SM增厚,127例(42.2%)出现单侧SM增厚。122例(40.5%)双侧上颌窦均未出现SM增厚。在554个上颌窦样本中,有231个(41.7%)样本出现SM增厚。所有样本中SM平均厚度为3.12 mm,在SM增厚样本中,平均SM的厚度为6.34 mm。当上颌后牙存在PAL时,SM增厚的检出率达60.6%(132/218);而无PAL时,SM增厚的检出率仅为29.5%(99/336),差异有统计学意义(P<0.05)(表1),说明PAL与SM增厚之间具有相关性。
表 1. SM增厚与PAL的关系.
Tab 1 Relationship between SM thickening and PAL
| 有无PAL | 有无SM增厚/n(%) |
合计 | χ2值 | P值 | |
| 无增厚 | 有增厚 | ||||
| 无PAL | 237(70.5) | 99(29.5) | 336 | 7.606 | 0.000 |
| 有PAL | 86(39.4) | 132(60.6) | 218 | ||
|
| |||||
| 合计 | 323 | 231 | 554 | ||
2.2. PAL各项检测指标与SM增厚程度
本研究共收集554个上颌窦样本,其中与PAL相关的SM增厚132个,按其SM增厚程度进行分级,轻度SM增厚74个(56.1%),中度SM增厚40个(30.3%),重度SM增厚18个(13.6%)。分别分析PAL直径(CBCT-PAI)、PAL上缘与上颌窦底的波及关系、有PAL的患牙是否进行根管治疗与SM增厚程度的关系。
CBCT-PAI 1/2/3分级患者中,轻度SM增厚程度占比较高,CBCT-PAI 4分级患者中,中度和重度SM增厚程度占比较高(表2)。研究显示,CBCT-PAI分级在不同SM增厚程度组之间的分布具有统计学意义(表2)。进一步采用Spearman相关性检验,发现二者呈正相关(表2,r=0.470,P=0.000),表明CBCT-PAI分级与不同SM增厚程度有关,且呈正相关关系。
表 2. PAL各项检测指标与SM增厚程度的关系.
Tab 2 Relationship between various indicators of PAL and the degree of SM thickening
| 各项检测指标 | SM增厚程度/n |
卡方检验/Fisher确切概率法 |
Spearman相关分析 |
||||||
| 轻度 | 中度 | 重度 | 合计 | χ2值 | P值 | r值 | P值 | ||
| CBCT-PAI分级 | 1 | 5 | 0 | 2 | 7 | / | 0.000 | 0.470 | 0.000 |
| 2 | 22 | 1 | 1 | 24 | |||||
| 3 | 38 | 14 | 5 | 57 | |||||
| 4 | 9 | 25 | 10 | 44 | |||||
| PAL上缘与上颌窦底之间的波及关系 | OS型 | 18 | 5 | 0 | 23 | / | 0.110 | / | / |
| CO型 | 39 | 24 | 12 | 75 | |||||
| IS型 | 17 | 11 | 6 | 34 | |||||
| 有PAL的患牙是否进行根管治疗 | 未经根管治疗的PAL | 43 | 14 | 10 | 67 | 5.739 | 0.057 | / | / |
| 根管治疗后的PAL | 31 | 26 | 8 | 65 | |||||
PAL上缘与上颌窦底之间的波及关系、有PAL的患牙是否进行根管治疗与SM增厚程度详见表2,研究显示PAL上缘与上颌窦底的3种不同波及关系、有PAL的患牙是否进行根管治疗与SM增厚程度之间的分布均无统计学意义(表2)。
2.3. PAL各项检测指标与SM增厚类型
本研究共收集554个上颌窦样本,其中与PAL相关的SM增厚132个,按其SM增厚类型进行分类,扁平型有91个(68.9%),息肉型有32个(24.2%),混浊型有9个(6.8%)。分别分析CBCT-PAI、PAL上缘与上颌窦底的波及关系、有PAL的患牙是否进行根管治疗与SM增厚类型之间的关系。
CBCT-PAI分级和PAL上缘与上颌窦底的3种不同波及关系与SM增厚类型的结果详见表3,研究显示二者与SM增厚类型之间的分布无统计学意义(表3),说明CBCT-PAI分级和PAL上缘与上颌窦底的3种不同波及关系与SM增厚类型无关。
表 3. PAL各项检测指标与SM增厚类型的关系.
Tab 3 Relationship between various indicators of PAL and the type of SM thickening
| 各项检测指标 | SM增厚类型/n |
卡方检验/Fisher确切概率法 |
|||||
| 扁平型 | 息肉型 | 混浊型 | 合计 | χ2值 | P值 | ||
| CBCT-PAI分级 | 1 | 3 | 2 | 2 | 7 | / | 0.238 |
| 2 | 19 | 5 | 0 | 24 | |||
| 3 | 41 | 13 | 3 | 57 | |||
| 4 | 28 | 12 | 4 | 44 | |||
| PAL上缘与上颌窦底之间的波及关系 | OS型 | 21 | 2 | 0 | 23 | / | 0.141 |
| CO型 | 48 | 21 | 6 | 75 | |||
| IS型 | 22 | 9 | 3 | 34 | |||
| 有PAL的患牙是否进行根管治疗 | 未经根管治疗的PAL | 50 | 9 | 8 | 67 | / | 0.002 |
| 根管治疗后的PAL | 41 | 23 | 1 | 65 | |||
未经根管治疗和根管治疗后的PAL患者与SM增厚类型结果详见表3,研究显示未经根管治疗的PAL与根管治疗后的PAL所导致的SM增厚类型之间有统计学差异(表3),表明SM增厚类型与有PAL的患牙是否进行根管治疗相关,根管治疗后的PAL组中SM息肉型增生多于未经根管治疗的PAL组,未经根管治疗的PAL组扁平型和混浊型多于根管治疗后PAL组。
3. 讨论
SM是一种位于鼻腔的呼吸道上皮内膜,它是由外胚层发展而来的,具有假复层纤毛柱状上皮的特征,在鼻腔和鼻旁窦中有重要功能。研究[2]认为,正常的上颌窦中SM的厚度约为1 mm,但厚度不恒定,并且存在个体差异。Pokorny等[14]发现64%的OMS病例在CT成像上显示出明显的根尖周感染。由于上颌后牙与上颌窦底的解剖关系紧密,如果上颌后牙出现PAL但没有及时治疗,那么可能会导致感染扩散到上颌窦,增加上颌窦炎发生的风险[4]。而且,如果情况严重,还可能出现与颅脑和眼睛相关的并发症。Zhang等[15]提出了“上颌牙-骨-窦复合体”的概念,指出上颌后牙、牙槽骨和上颌窦紧密相连,它们构成了一个复杂的解剖结构,在血液供应、感觉和空间定位等方面相互关联,一旦发生疾病,这些结构就极易相互影响。OMS是一种涉及上颌牙齿、牙槽骨和鼻窦病变的疾病,调查SM增厚与PAL的关系可能有助于确定最佳的治疗方式。近年来,OMS的发病率不断上升,在慢性上颌窦炎中占5%~40%[1],呈上升趋势。然而,尽管OMS在上颌窦感染中起着重要作用,但它的重要性常常被忽视,延误诊断,从而导致治疗不当甚至失败。临床上往往很难区分鼻源性上颌窦炎和OMS的真正原因,在影像学上亦存在部分难点。影像学是诊疗过程中的重要一环,本研究使用CBCT来探究SM增厚及其类型与PAL的关系,旨在为临床提供参考依据。
本研究按SM增厚的严重程度进行分级,其中轻度SM增厚占56.1%,中度SM增厚占30.3%,重度SM增厚占13.6%。本研究最常见到的SM增厚程度为轻度SM增厚,即SM增厚程度为2~5 mm,此结果与Shanbhag等[16]的一致。然而,Gurhan等[17]的研究中最常检测到的是重度SM增厚。这些研究结果的差异可能在于不同的研究使用了不同的影像学方法来评估牙齿的根尖周状态以及纳入病例的人群不同。本研究显示CBCT-PAI分级在不同SM增厚程度呈正相关性,即随着PAL程度的增加,SM增厚的程度也在增加。这与许多研究[13],[18]–[19]所得的结果相同。相反的,Lu等[13]发现PAL在微小病变、轻度病变、较大范围病变3组之间,SM增厚程度变化无差异。这两个结果之间的不同可能是对PAL的分级程度不同造成的。此外,本研究发现PAL上缘与上颌窦底之间的3种波及关系对SM增厚未发现统计学关联,这与之前的研究[20]认为上颌窦炎的严重程度可能更大程度上取决于根尖周炎症边缘距上颌窦底的远近不一致。尽管先前的研究认为黏膜刺激可能受到PAL和上颌窦底之间距离的潜在影响[21]。原因之一可能是上颌骨小梁具有多孔结构,在放射学上可检测到的PAL病变形成或扩大之前,细菌毒素可以通过疏松的上颌骨及血管、淋巴管等结构扩散,直接渗入上颌窦;但是即使根尖周病灶上缘与上颌窦底存在一定距离,根尖炎症的细菌与毒素也能侵入上颌窦,并造成上颌窦底SM增厚程度的增加。因此,在临床工作中要警惕慢性根尖周病变的病灶,即使病变上缘远离上颌窦底这种波及关系,也会影响SM增厚。研究[22]发现,有PAL的患牙是否进行根管治疗对SM增厚程度无影响,与本研究结果一致。
本研究分析了PAL各项检测指标与SM增厚类型之间的相关性,发现根管治疗后存在PAL组SM息肉型增生多于未经根管治疗PAL组,未经根管治疗的PAL组扁平型和混浊型多于根管治疗后存在PAL组。该结果可能是由于未经治疗的PAL与根管治疗后PAL组中根管菌群的组成存在差异[23]。Hong等[24]的研究表明,根管微生物的组成在未经根管治疗的PAL和根管治疗后的PAL组中是不同的。未经根管治疗的PAL感染特点是多种微生物混合并且普遍存在厌氧菌,最常发现的菌属为革兰阴性菌群。相比之下,根管治疗后仍存在的PAL感染,与革兰阳性细菌(如肠球菌和链球菌)的高流行率有关。随着现代分子科技的不断精进,传统的单一取样方法已显现出其局限性,无法充分揭示根管内细菌的全貌,而多元化的取样与检测策略的联合应用则有望显著提升细菌种类的识别能力[25]。然而,根管治疗前后PAL中细菌微生物构成的差异是否对SM的增厚类型产生影响,目前尚不清楚。因此,针对这一问题,将来需要进一步的深入探究。
综上,超过半数的病例在影像学研究中显示SM增厚现象,而且这种现象与PAL直径呈明显的正向关联。随着PAL病变程度的加重,SM增厚的程度也会增加。不管PAL侵犯上颌窦底的具体位置如何,都应该高度重视上颌后牙区域的SM异常。由于患者可能没有明显的症状,临床上更需要密切关注并及时诊治PAL,以防止其引发OMS的可能性。本研究的主要局限是为横断面研究,患者的临床症状和病史没有包括在本研究中。因为影像数据的回顾性评估无法完全提供关于根尖周围病变的炎症状态或性质的进一步信息。因此,需要进一步的影像学结合临床症状的追踪或溯源研究来探究这种关系。对于上颌后牙区存在PAL引起的SM增厚应引起注意,以实现早期诊断和有效治疗。口腔科医生和耳鼻喉科医生合作诊断和治疗疑似的OMS可能是一种有效的以患者为中心的策略。
Footnotes
利益冲突声明:作者声明本文无利益冲突。
References
- 1.Whyte A, Boeddinghaus R. Imaging of odontogenic sinusitis[J] Clin Radiol. 2019;74(7):503–516. doi: 10.1016/j.crad.2019.02.012. [DOI] [PubMed] [Google Scholar]
- 2.Insua A, Monje A, Chan HL, et al. Accuracy of Schneiderian membrane thickness: a cone-beam computed tomography analysis with histological validation[J] Clin Oral Implants Res. 2017;28(6):654–661. doi: 10.1111/clr.12856. [DOI] [PubMed] [Google Scholar]
- 3.Kuligowski P, Jaroń A, Preuss O, et al. Association between odontogenic and maxillary sinus conditions: a retrospective cone-beam computed tomographic study[J] J Clin Med. 2021;10(13):2849. doi: 10.3390/jcm10132849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.戢 晓, 张 岚, 黄 定明. 牙源性与非牙源性上颌窦炎鉴别诊断及其治疗方案的研究进展[J] 国际口腔医学杂志. 2023;50(5):566–572. [Google Scholar]; Ji X, Zhang L, Huang DM. Diagnosis and treatment of odontogenic and non-odontogenic maxillary sinusitis[J] Int J Stomatol. 2023;50(5):566–572. [Google Scholar]
- 5.Marian-Vladimir C. Essential endodontology: prevention and treatment of apical periodontitis[J] Stomatol Edu J. 2020;7(4):302–308. [Google Scholar]
- 6.Wuokko-Landén A, Blomgren K, Suomalainen A, et al. Odontogenic causes complicating the chronic rhinosinusitis diagnosis[J] Clin Oral Investig. 2021;25(3):947–955. doi: 10.1007/s00784-020-03384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Workman AD, Granquist EJ, Adappa ND. Odontogenic sinusitis: developments in diagnosis, microbiology, and treatment[J] Curr Opin Otolaryngol Head Neck Surg. 2018;26(1):27–33. doi: 10.1097/MOO.0000000000000430. [DOI] [PubMed] [Google Scholar]
- 8.Bajoria AA, Sarkar S, Sinha P. Evaluation of odontogenic maxillary sinusitis with cone beam computed tomography: a retrospective study with review of literature[J] J Int Soc Prev Community Dent. 2019;9(2):194–204. doi: 10.4103/jispcd.JISPCD_435_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zadsirjan S, Sheikhi M, Dakhilalian A, et al. Association of inflammatory periapical lesions with maxillary sinus abnormalities: a retrospective cone-beam computed tomography study[J] J Dent(Shiraz) 2021;22(4):273–280. doi: 10.30476/DENTJODS.2021.87286.1254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.齐 建华, 来 卫东, 赵 彦霞, et al. CBCT评估牙源性炎性疾病与上颌窦黏膜增厚相关性的回顾性分析[J] 临床口腔医学杂志. 2021;37(5):292–295. [Google Scholar]; Qi JH, Lai WD, Zhao YX, et al. Evaluation on correlation between odontogenic inflammatory diseases and mucosal thickening of maxillary sinus using CBCT: a retrospective analysis[J] J Clin Stomatol. 2021;37(5):292–295. [Google Scholar]
- 11.Aksoy U, Orhan K. Association between odontogenic conditions and maxillary sinus mucosal thickening: a retrospective CBCT study[J] Clin Oral Investig. 2019;23(1):123–131. doi: 10.1007/s00784-018-2418-x. [DOI] [PubMed] [Google Scholar]
- 12.Estrela C, Bueno MR, Azevedo BC, et al. A new periapical index based on cone beam computed tomography[J] J Endod. 2008;34(11):1325–1331. doi: 10.1016/j.joen.2008.08.013. [DOI] [PubMed] [Google Scholar]
- 13.Lu Y, Liu ZJ, Zhang L, et al. Associations between maxillary sinus mucosal thickening and apical periodontitis using cone-beam computed tomography scanning: a retrospective study[J] J Endod. 2012;38(8):1069–1074. doi: 10.1016/j.joen.2012.04.027. [DOI] [PubMed] [Google Scholar]
- 14.Pokorny A, Tataryn R. Clinical and radiologic findings in a case series of maxillary sinusitis of dental origin[J] Int Forum Allergy Rhinol. 2013;3(12):973–979. doi: 10.1002/alr.21212. [DOI] [PubMed] [Google Scholar]
- 15.Zhang JL, Liu L, Yang L, et al. Diagnosis of odontogenic maxillary sinusitis by cone-beam computed tomography: a critical review[J] J Endod. 2023;49(11):1445–1456. doi: 10.1016/j.joen.2023.08.014. [DOI] [PubMed] [Google Scholar]
- 16.Shanbhag S, Karnik P, Shirke P, et al. Association between periapical lesions and maxillary sinus mucosal thickening: a retrospective cone-beam computed tomographic study[J] J Endod. 2013;39(7):853–857. doi: 10.1016/j.joen.2013.04.010. [DOI] [PubMed] [Google Scholar]
- 17.Gürhan C, Şener E, Mert A, et al. Evaluation of factors affecting the association between thickening of sinus mucosa and the presence of periapical lesions using cone beam CT[J] Int Endod J. 2020;53(10):1339–1347. doi: 10.1111/iej.13362. [DOI] [PubMed] [Google Scholar]
- 18.Ince Yusufoglu S, Hasanoglu Erbasar GN, Gülen O. Evaluation of the effect of periapical lesions and other odontogenic conditions on maxillary sinus mucosal thickness characteristics and mucosal appearance: a CBCT study[J] J Dent Res Dent Clin Dent Prospects. 2021;15(3):163–171. doi: 10.34172/joddd.2021.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Huang YT, Hu SW, Huang JY, et al. Assessment of relationship between maxillary sinus membrane thickening and the adjacent teeth health by cone-beam computed tomography[J] J Dent Sci. 2021;16(1):275–279. doi: 10.1016/j.jds.2020.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.杨 雨楠, 刘 鹏, 王 虎, et al. 上颌窦黏膜增厚的锥形束CT影像分析[J] 国际口腔医学杂志. 2023;50(3):302–307. [Google Scholar]; Yang YN, Liu P, Wang H, et al. Evaluation of maxillary sinusitis with cone beam computed tomography[J] Int J Stomatol. 2023;50(3):302–307. [Google Scholar]
- 21.Nunes CA, Guedes OA, Alencar AH, et al. Evaluation of periapical lesions and their association with maxillary sinus abnormalities on cone-beam computed tomographic images[J] J Endod. 2016;42(1):42–46. doi: 10.1016/j.joen.2015.09.014. [DOI] [PubMed] [Google Scholar]
- 22.Garcia-Font M, Abella F, Patel S, et al. Cone-beam computed tomographic analysis to detect the association between primary and secondary endodontic infections and mucosal thickness of maxillary sinus[J] J Endod. 2020;46(9):1235–1240. doi: 10.1016/j.joen.2020.05.015. [DOI] [PubMed] [Google Scholar]
- 23.Siqueira JF, Rocas IN. Present status and future directions: microbiology of endodontic infections[J] Int Endod J. 2022;55(S3):512–530. doi: 10.1111/iej.13677. [DOI] [PubMed] [Google Scholar]
- 24.Hong BY, Lee TK, Lim SM, et al. Microbial analysis in primary and persistent endodontic infections by using pyrosequencing[J] J Endod. 2013;39(9):1136–1140. doi: 10.1016/j.joen.2013.05.001. [DOI] [PubMed] [Google Scholar]
- 25.朱 嘉妮, 苏 勤. 难治性根尖周炎根管内及根尖外菌群的研究现状[J] 国际口腔医学杂志. 2022;49(3):283–289. [Google Scholar]; Zhu JN, Su Q. Research status of the use of root canal and periapical microflora in refractory periapical periodontitis[J] Int J Stomatol. 2022;49(3):283–289. [Google Scholar]