

Abstract
Objective:
This study aimed to identify the clinical and growth parameters associated with retinopathy of prematurity (ROP) in infants with necrotizing enterocolitis (NEC) and spontaneous ileal perforation (SIP).
Methods:
We conducted a retrospective cohort study that compared clinical data before and after NEC/SIP onset in neonates, categorizing by any ROP and severe ROP (Type 1/2) status.
Results:
The analysis included one hundred and nine infants (n=109) with surgical necrotizing enterocolitis/SIP. Sixty infants (60/109, 55%) were diagnosed with any ROP, 32/109 (29.3%) infants (22% Types 1 and 7.3% Type 2) with severe ROP.
On univariate analysis, those with severe ROP(32/109, 39.5%) were of lower median gestational age (23.8 weeks [23.4;24.6] vs. 27.3 [26.3;29.], p=<0.001), lower median birth weight (625 grams [512;710] vs.935 [700;1180]; p<0.001) and experienced higher exposure to clinical chorioamnionitis (22.6% vs. 2.13%; p=<0.006), and later median onset of ROP diagnosis (63.0 days [47.0;77.2] vs. 29.0 [19.0;41.0]; p=<0.001), received Penrose drain placement more commonly (19 (59.4%) vs.16 (34.0%); p=0.04), retained less residual small bowel (70.0 cm [63.1;90.8] vs.90.8 [72.0;101]; p=0.007) following surgery, were exposed to higher FiO2 seven days after birth (p=0.001), received ventilation longer and exposed to higher FiO2 at two weeks (p <0.05) following NEC and developed acute kidney injury (AKI) more often (25 (86.2%) vs.20 (46.5%); p= 0.002) than those without ROP. Those with severe ROP had lower length, weight for length, and head circumference z scores. In an adjusted Firth’s logistic regression, GA (aOR=0.51, 95% CI: [0.35, 0.76]) and diagnosis at later age (aOR=1.08, 95% CI: [1.03, 1.13]) was shown to be significantly associated with any ROP.
Conclusion:
Infants who develop severe ROP following surgical NEC/SIP are likely to be younger, smaller, have been exposed to more O2, develop AKI, and grow poorly compared to those did not develop severe ROP.
Introduction:
Necrotizing enterocolitis (NEC) is the most common acute gastrointestinal illness affecting preterm neonates, injuring 5–10% with a birth weight ≤1500 grams [1, 2]. NEC remains a leading cause of morbidity due to triggering a systemic inflammatory response that induces multiorgan dysfunction and increases the risk of in-hospital mortality leading to an increased annual healthcare burden [3].
Necrotizing enterocolitis is associated with necrosis, inflammation, hemorrhage, and reparative changes on intestinal histopathological examination [4]. The hemorrhagic necrosis seen in infants with NEC is likely due to abnormal vasculature and neoangiogenesis in the intestine [5, 6]. The retinopathy of prematurity is also associated with abnormal vascularization secondary to insulin-like growth factor 1 (IGF-1) and vascular endothelial growth factor (VEGF) mediated effects on retinal angiogenesis [7]. In the Early Treatment for Retinopathy of Prematurity study, ROP developed in 68% of preterm infants <1251 g, and severe retinopathy of prematurity developed in almost 37% of those cases [8]. A recent multicenter study reported that 12.8% of infants born < 28 weeks were diagnosed with severe ROP [9], and 2.5% developed bilateral blindness upon the long-term follow-up. Published reports note that the presence of surgical NEC and the timing of NEC onset are significant risk factors for ROP [10, 11]. Additionally, the established association of surgical NEC with dysbiosis and poor growth outcomes [12, 13] is strikingly similar to the reported association between the altered gut microbiome and the development of ROP [14] and the known heightened risk of severe ROP with poor postnatal weight gain [15, 16]. Accordingly, infants with surgical NEC may be at greater risk for the development of severe ROP secondary to a gastrointestinal-triggered inflammatory surge which influences retinal angio- and vasculogenesis.
Given the paucity of data associating surgical NEC/SIP with severe ROP, we conducted a single-center, retrospective cohort study to determine the clinical risk factors associated with severe ROP in preterm infants with surgical NEC. In addition, we investigated the growth characteristics (weight, length, weight for length, and head circumference) associated with ROP before and after the surgical NEC onset in preterm infants. We hypothesized to identify the clinical risk factors associated with any ROP and severe ROP in preterm infants with surgical NEC.
Methods:
Population and Study Design:
The study was conducted at the University of Mississippi Medical Center after institutional review board approval in a level 4 neonatal intensive care unit, which is a regional referral center for neonates with surgical NEC in the entire state. All neonates admitted between January 1, 2013, and June 2018, diagnosed with NEC (Bell stage III), were included in the study [17]. Neonates diagnosed with medical NEC only were excluded and summarized in Figure 1.
Figure 1:
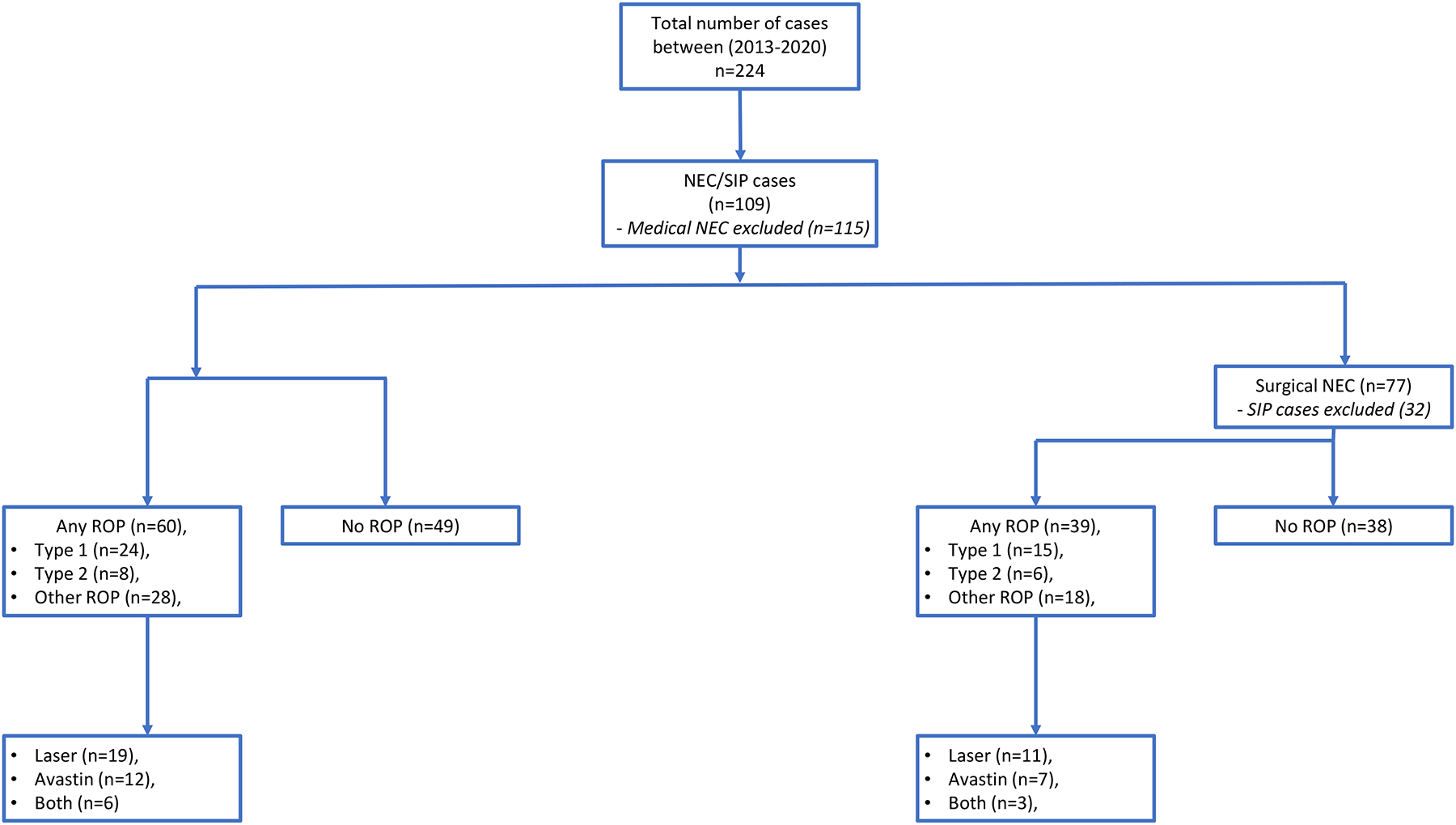
The flowchart showing infants included in the study.
Demographic data:
The data was collected retrospectively from the electronic medical records by the research team members. We collected demographic data, including gestational age (GA), birth weight (BW), sex, appropriate for gestational age (AGA) status, race, out born status, mode of delivery, and Apgar scores ≤ 6 at 5 minutes. We also collected maternal variables, including maternal pregnancy-induced hypertension (PIH), chorioamnionitis, and antenatal steroids.
Collected clinical information for each infant included number of days of mechanical ventilation exposure, presence of patent ductus arteriosus (PDA) and indomethacin/ibuprofen therapy for PDA treatment (before NEC), and inotrope (dopamine) use 24 hours after NEC onset. In addition, we collected information on duration, FiO2 requirement, and mode of ventilation (invasive/non-invasive) before (birth until the day of NEC onset) and following NEC. We also collected data on the blood culture-proven sepsis at NEC onset, length of stay, and mortality. The length of stay was defined as the total duration of hospitalization from the day of admission until discharge or death due to any cause before hospital discharge.
NEC data:
We recorded information on the age (in days) at the time of NEC diagnosis. The diagnosis of NEC was made based on radiographic findings, including pneumatosis, portal venous gas, and pneumoperitoneum on abdominal X-ray. The frequency of surgical NEC (Bell stage III) was also collected [17]. Neonates who died within 48 hours after NEC onset and massive bowel necrosis found during laparotomy or autopsy were classified as having fulminant NEC. At our center, preterm infants with pneumoperitoneum who weigh less than 1 kg at NEC/SIP diagnosis and are hemodynamically unstable are treated first with a Penrose drain at the bedside but may later receive laparotomy. The timing of laparotomy after placement of the Penrose drain was based on clinical deterioration.
NEC Histopathological Evaluation:
Hematoxylin and eosin-stained surgical resected intestinal tissue sections were evaluated for necrosis, inflammation, hemorrhage, and reparative changes. A score of 0 was assigned when the exam appeared normal, 1 for 1–25% necrosis/ inflammation, 2 when 25–50% area involved, 3 when 50–75% area was affected, and 4 when >75% changes were seen[18].
Postoperative information such as postoperative ileus days (defined as infants being NPO after bowel surgery), time to reach full feeds (≥ 120 ml/kg/day), and total parenteral nutrition days were also gathered. The surgical morbidity was classified as strictures, fistulas, wound dehiscence, surgical site infections (including abscesses), adhesions, and perforations.
Retinopathy of Prematurity Data:
ROP testing was indicated if the infant was born before 31 weeks of gestational age, birth weight less than 1500 grams or after 31 weeks if considered high risk. ROP was grouped into three categories: Type 1 ROP, type 2 ROP, and other ROP [11, 19]. Type 1 and type 2 ROP are the most severe and require treatment. Any infant with plus disease was categorized as having type 1 ROP. Plus disease indicates dilated veins and tortuous arteries in the posterior pole of the eye. Type 2 ROP is any infant having stage 3 disease. The infants having eye exam findings other than Type 1 and 2 were classified as other ROP. We recorded data of infants with type 1 and type 2 ROP treated with laser photocoagulation or Avastin(bevacizumab)®.
Kidney Function Data:
We collected all serum creatinine measurements and daily urine output data starting the day before NEC diagnosis, at NEC onset, and up to 1 week after NEC diagnosis.
We defined AKI using the modified neonatal AKI staging criteria previously described in the kidney disease: Improving Global Outcomes (KDIGO) Clinical Practice Guideline [20–24].
Bronchopulmonary dysplasia (BPD) data:
BPD at 36 weeks corrected gestational age was classified as mild, moderate, and severe based on the oxygen requirement at assessment [25]. We collected data on the type of steroid (hydrocortisone/dexamethasone) used during the clinical course following the NEC onset.
Growth Outcome data:
Anthropometric variables collected include weight, height, weight-for-length, head circumference, and respective z-scores [26]. Sex-specific Fenton growth charts were used for infants less than 50 weeks old, and gender-specific World Health Organization (WHO) corrected for gestational age growth charts were used for infants greater than 50 weeks old. Time intervals include prior to developing NEC, during NEC treatment, post-NEC until anastomosis, after anastomosis, at 36 weeks of chronological age, and at discharge.
Brain injury data:
Brain Magnetic Resonance Imaging (MRI) was routinely obtained at term equivalent age or before discharge home for all preterm infants weighing less than 1500 grams at birth. Two pediatric neuroradiologists scored the MRI images independently using the scoring system of eight scales for white and gray matter injury developed by Woodward et al. [27]. The categories of white-matter abnormality were none (a score of 5 to 6), mild (a score of 7 to 9), moderate (a score of 10 to 12), and severe (a score of 13 to 15).
Statistical Methods:
In our study, we analyzed the combined cohort of NEC/SIP and NEC separately. We evaluated all continuous variables utilizing the Mann-Whitney U-test, with the results presented as median values accompanied by the interquartile range (Quartile 1; Quartile 3). In contrast, categorical variables were reported as count (n) and relative frequencies as percentages. To assess the differences among categorical variables, we employed the Chi-squared test. However, when cell counts were under 5, Fisher’s exact test was utilized instead. From the bivariate analyses, statistically significant variables were incorporated into Firth’s logistic regression model. In addressing missing data within our dataset, we employed listwise deletion as our primary method of missing data handling. This approach entailed excluding any preterm infants from the multivariate analysis that had missing values for any variable included in the model. By implementing listwise deletion, we ensured that analyses were conducted on complete cases only. Adjusted odds ratios were reported as effect size along with 95% confidence interval and P value. A two-sided P values less than 0.05 were considered as significant. Statistical analyses were performed in R Statistical Software (version 4.2.1; The R Foundation for Statistical Computing).
Results:
Combined Cohort NEC+SIP:
Any ROP:
In the combined cohort of NEC and SIP, of the 109 infants included in the analysis, 55% (60/109) were diagnosed with any form of ROP and 29.3% (32/109) had severe ROP, including (22% (24/109) with Type 1 and 7.3% (8/109) with Type 2. 28/60 infants were in other ROP category. Forty-nine infants (49/109,45%) did not show any ROP on the eye exam. Among the 60 cases with any ROP, 40% (24/60) were Type 1, 13.3% (8/60) were Type 2 and 28/60 were Other ROP. Regarding management, 31.1% (19/60) treated with laser therapy, 20% (12/60) received Avastin(bevacizumab)®, and 10% (6/60) were treated with both laser and Avastin(bevacizumab)®.
Infants with any ROP (60/109, Type 1, 2 & Other ROP) had significantly lower gestational age (24.4 weeks [23.5;25.4] vs. 27.3 weeks [26.3;29.3), p=<0.001) and lower median birth weight (665 grams [556;776] vs. 935 grams [700;1180], p=<0.001) than those infants with surgical NEC/SIP without ROP. Those with any ROP had a lower frequency of portal venous gas (1/60 (1.7%) vs. 6 /40 (12.2%), p=0.045) on the abdominal x-ray, received Penrose drain therapy more often (35/60 (59 %) vs. 16/49 (34%), p=0.017) and experienced AKI by serum creatinine criteria more often (44 (78.6%) vs. 20 (46.5%),p=0.002) than those infants with surgical NEC without any ROP (49/109).
Furthermore, infants with any ROP had significantly higher exposure to pregnancy-induced hypertension (11 (19 %) vs. 20 (41.7%), p=0.019) and chorioamnionitis (11/60 (19 %) vs.1/49 (2.1%), p=0.017) and PDA more frequently (75% vs. 55%), p=0.048) and received indomethacin more frequently (22% vs.6.2%), p=0.045) than those without any ROP. The data are shown in Table 1 and 2.
Table 1:
Demographics, Prenatal Information, ROP Features and Clinical Outcomes in infant with and without any ROP in NEC/SIP cohort
| n | All n=109 | No ROP n=49 | Any ROP n=60 | P value | |
|---|---|---|---|---|---|
| Prenatal Information | |||||
| Pregnancy Induced Hypertension, n (%) | 106 | 31 (29.2) | 20 (41.7) | 11 (19.0) | 0.019 |
| Chronic Hypertension, n (%) | 95 | 15 (15.8) | 7 (15.9) | 8 (15.7) | 0.99 |
| Chorioamnionitis, n (%) | 105 | 12 (11.4) | 1 (2.13) | 11 (19.0) | 0.017 |
| Antenatal Steroids, n (%) | 100 | 71 (71.0) | 30 (66.7) | 41 (74.5) | 0.52 |
| Infant Demographics | |||||
| Gestational Age (weeks, median [IQR]) | 109 | 25.4 [24.0;27.3] | 27.3 [26.3;29.3] | 24.4 [23.5;25.4] | <0.001 |
| Birth weight (g, median [IQR]) | 109 | 730 [620;940] | 935 [700;1180] | 665 [556;776] | <0.001 |
| Small for gestational Age, n (%) | 106 | 37 (34.9) | 18 (37.5) | 19 (32.8) | 0.76 |
| Male, n (%) | 109 | 67 (61.5) | 34 (69.4) | 33 (55.0) | 0.18 |
| Ethnicity, n (%) | 107 | 0.32 | |||
| African American | 84 (78.5) | 40 (83.3) | 44 (74.6) | ||
| Caucasian | 20 (18.7) | 8 (16.7) | 12 (20.3) | ||
| Other | 3 (2.80) | 0 (0.00) | 3 (5.08) | ||
| Vaginal Delivery, n (%) | 109 | 34 (31.2) | 16 (32.7) | 18 (30.0) | 0.93 |
| Apgar score <6 at 5 min, n (%) | 107 | 30 (28.0) | 4 (8.33) | 26 (44.1) | <0.001 |
| Out born, n (%) | 109 | 69 (63.3) | 28 (57.1) | 41 (68.3) | 0.31 |
| Infant Medical Information Prior to NEC | |||||
| Patent Ductus Arteriosis, n (%) | 109 | 72 (66.1) | 27 (55.1) | 45 (75.0) | 0.048 |
| PDA Surgical Ligation, n (%) | 106 | 7 (6.60) | 3 (6.25) | 4 (6.90) | 0.99 |
| Indomethacin Use, n (%) | 107 | 16 (15.0) | 3 (6.25) | 13 (22.0) | 0.045 |
| Blood Culture Prior to Onset of NEC, n (%) | 109 | 36 (33.0) | 16 (32.7) | 20 (33.3) | 0.99 |
| Postoperative Systemic Course | |||||
| 24 h Ionotropic support, n (%) | 104 | 76 (73.1) | 30 (63.8) | 46 (80.7) | 0.08 |
| AKI by Serum Creatinine, n (%) | 99 | 64 (64.6) | 20 (46.5) | 44 (78.6) | 0.002 |
| AKI by Urine Output, n (%) | 98 | 44 (44.9) | 17 (42.5) | 27 (46.6) | 0.85 |
| Sepsis Variables | |||||
| Central Line Present (days, median [IQR]) | 95 | 60.0 [38.0;99.0] | 60.0 [43.0;87.0] | 53.5 [36.2;108] | 0.99 |
| Positive Blood Culture Sepsis following NEC, n (%) | 109 | 36 (33.0) | 16 (32.7) | 20 (33.3) | 0.99 |
| Antibiotic Duration (days, median [IQR]) | 75 | 10.0 [7.00;14.0] | 9.50 [6.75;12.5] | 10.0 [7.00;14.0] | 0.65 |
| CRP 24 Hours following NEC (median [IQR]) | 77 | 8.70 [3.20;17.7] | 12.6 [4.40;19.0] | 8.00 [2.98;17.7] | 0.58 |
| CRP 96 Hours following NEC (median [IQR]) | 72 | 8.05 [4.10;17.1] | 15.2 [4.03;22.5] | 6.35 [4.12;9.00] | 0.05 |
| CRP 1 week following NEC (median [IQR]) | 76 | 4.60 [2.50;7.70] | 5.80 [3.00;13.4] | 4.45 [2.45;6.62] | 0.17 |
| CRP 2 weeks following NEC (median [IQR]) | 72 | 3.35 [1.67;5.73] | 3.40 [1.70;7.20] | 3.30 [1.65;5.25] | 0.58 |
| Hematologic Variables | |||||
| Any packed red cell transfusion before NEC, n (%) | 90 | 85 (94.4) | 39 (92.9) | 46 (95.8) | 0.66 |
| Hematocrit before NEC (median [IQR]) | 71 | 34.0 [30.2;38.2] | 34.4 [29.9;39.0] | 33.8 [30.6;37.9] | 0.66 |
| Packed red cell transfusion 48 hours after NEC onset, n (%) | 98 | 77 (78.6) | 37 (78.7) | 40 (78.4) | 0.99 |
| Any Platelet transfusion before NEC, n (%) | 102 | 78 (76.5) | 36 (75.0) | 42 (77.8) | 0.92 |
| Platelet transfusion 48 hours after NEC, n (%) | 91 | 41 (45.1) | 20 (44.4) | 21 (45.7) | 0.99 |
| ROP | |||||
| Day of Life at no ROP (g, median [IQR]) | 109 | 47.0 [42.0;57.0] | 44.0 [40.0;56.0] | 52.0 [43.0;57.2] | 0.017 |
| Day of Life of Severe ROP Diagnosis (g, median [IQR]) | 109 | 60.0 [44.0;75.0] | 44.0 [40.0;56.0] | 70.5 [60.8;87.0] | <0.001 |
| Corrected Gestational Age of Severe ROP Diagnosis (g, median [IQR]) | 109 | 34.4 [33.1;36.1] | 33.7 [32.6;35.2] | 34.8 [33.7;37.0] | 0.015 |
| Type 1 ROP, n (%) | 109 | 24 (22.0) | 0 (0.00) | 24 (40.0) | <0.001 |
| Type 2 ROP, n (%) | 109 | 8 (7.34) | 0 (0.00) | 8 (13.3) | 0.008 |
| No ROP | 109 | 49 (45.0) | 49 (100) | 0 (0.00) | <0.001 |
| Laser, n (%) | 109 | 19 (17.4) | 0 (0.00) | 19 (31.7) | <0.001 |
| Avastin(bevacizumab)®, n (%) | 109 | 12 (11.0) | 0 (0.00) | 12 (20.0) | 0.003 |
| Both, n (%) | 109 | 6 (5.50) | 0 (0.00) | 6 (10.0) | 0.032 |
| Outcomes | |||||
| Brain MRI Corrected Gestational Age (weeks, median [IQR]) | 54 | 40.8 [38.3;46.4] | 41.1 [36.3;45.3] | 40.5 [39.0;48.4] | 0.39 |
| White Matter Abnormality, n (%) | 51 | 26 (51.0) | 9 (42.9) | 17 (56.7) | 0.49 |
| Grey Matter Abnormality, n (%) | 50 | 5 (10.0) | 1 (5.00) | 4 (13.3) | 0.64 |
| Length of Stay (days, median [IQR]) | 109 | 117 [72.0;171] | 138 [47.0;171] | 116 [75.8;172] | 0.95 |
| Death, n (%) | 109 | 37 (33.9) | 21 (42.9) | 16 (26.7) | 0.12 |
Notes: Continuous data was represented as median (Interquartile range, IQR) and categorical data was represented as frequency (percentages). P values were based on Chi-squared test (or Fisher’s exact test when cell counts below 5) and Mann-Whitney U-test. IQR represented as (Quartile 1; Quartile 3)
Table 2:
NEC features, and postoperative information in preterm infants with any ROP in NEC/SIP cohort.
| n | All, n=109 | No ROP n=49 | Any ROP n=60 | P value | |
|---|---|---|---|---|---|
| NEC Disease Features | |||||
| Clinical Presentation of NEC, n (%) | 107 | 0.004 | |||
| Abdominal Distension | 98 (91.6) | 41 (83.7) | 57 (98.3) | ||
| Bloody Stools | 6 (5.61) | 6 (12.2) | 0 (0.00) | ||
| Feeding Intolerance | 3 (2.80) | 2 (4.08) | 1 (1.72) | ||
| Radiological Findings, n (%) | 108 | ||||
| Pneumatosis | 42 (38.9) | 22 (44.9) | 20 (33.9) | 0.33 | |
| Portal Venous Gas | 7 (6.48) | 6 (12.2) | 1 (1.69) | 0.045 | |
| Pneumoperitoneum | 62 (57.4) | 25 (51.0) | 37 (62.7) | 0.3 | |
| Penrose Drain, n(%) | 106 | 51 (48.1) | 16 (34.0) | 35 (59.3) | 0.017 |
| Fulminant NEC, n (%) | 108 | 10 (9.26) | 4 (8.16) | 6 (10.2) | 0.99 |
| Length and Region of Bowel (cm, median [IQR]) | 104 | 10.7 [4.27;27.4] | 15.0 [5.35;36.6] | 9.70 [3.50;21.5] | 0.05 |
| Length of Jejunum Lost (cm, median [IQR]) | 97 | 0.00 [0.00;8.10] | 1.00 [0.00;14.4] | 0.00 [0.00;3.55] | 0.16 |
| Length of Ileum Lost (cm, median [IQR]) | 101 | 3.20 [0.00;9.00] | 3.80 [0.00;12.2] | 3.20 [0.00;8.75] | 0.52 |
| Length of Colon Lost (cm, median [IQR]) | 101 | 0.00 [0.00;1.70] | 0.00 [0.00;1.05] | 0.00 [0.00;2.00] | 0.79 |
| Region of Bowel Resected, n (%) | 100 | 0.74 | |||
| Large Bowel or Both | 31 (31.0) | 13 (28.3) | 18 (33.3) | ||
| Small bowel | 69 (69.0) | 33 (71.7) | 36 (66.7) | ||
| Presence of Ileocecal Valve, n (%) | 105 | 76 (72.4) | 32 (66.7) | 44 (77.2) | 0.33 |
| Type of Stoma | |||||
| Jejunostomy, n (%) | 109 | 34 (31.2) | 19 (38.8) | 15 (25.0) | 0.18 |
| Ileostomy, n (%) | 109 | 62 (56.9) | 23 (46.9) | 39 (65.0) | 0.09 |
| Colostomy, n (%) | 109 | 11 (10.1) | 2 (4.08) | 9 (15.0) | 0.11 |
| Total small bowel Lost, (cm, median [IQR]) | 109 | 8.00 [3.20;22.3] | 10.0 [4.20;31.2] | 6.20 [1.98;12.7] | 0.024 |
| Residual small bowel, (cm, median [IQR]) | 109 | 77.7 [65.0;98.0] | 90.8 [72.0;101] | 70.0 [63.5;94.0] | 0.004 |
| Residual Colon, (cm, median [IQR]) | 109 | 24.4 [22.7;27.8] | 24.4 [22.7;36.0] | 22.7 [22.7;24.4] | 0.001 |
| Histopathological Factors | |||||
| Necrosis (≥50 vs <50%, median [IQR]) | 76 | 1.50 [0.00;3.00] | 2.00 [0.00;3.00] | 1.00 [0.00;2.00] | 0.42 |
| Inflammation (≥50 vs <50%, median [IQR]) | 76 | 2.00 [1.00;2.00] | 2.00 [1.00;3.00] | 2.00 [1.00;2.00] | 0.38 |
| Hemorrhage (≥ 50 vs <50%, median [IQR]) | 76 | 2.00 [2.00;3.00] | 3.00 [2.00;4.00] | 2.00 [1.50;3.00] | 0.2 |
| Reparative Change, n (%) | 76 | 32 (42.1) | 12 (36.4) | 20 (46.5) | 0.51 |
| Post Operative Intestinal Features | |||||
| Post Operative Ileus (days, median [IQR]) | 83 | 13.0 [11.0;17.5] | 12.5 [11.0;17.2] | 13.0 [10.5;17.0] | 0.69 |
| Duration of Parenteral Nutrition (days, median [IQR]) | 105 | 81.0 [38.0;118] | 76.5 [36.2;120] | 86.0 [39.0;118] | 0.6 |
| Postoperative Day at Starting Enteral Feedings (days), n (%) | 82 | 14.0 [12.0;18.0] | 14.0 [12.0;18.0] | 14.0 [11.8;18.8] | 0.78 |
| Time to reach full feeds, (days) (median [IQR]) | 70 | 65.5 [32.0;92.2] | 62.0 [41.0;93.0] | 69.0 [29.0;89.0] | 0.8 |
| Wound Dehiscence, n (%) | 109 | 28 (25.7) | 11 (22.4) | 17 (28.3) | 0.63 |
| Wound Infection, n (%) | 109 | 14 (12.8) | 10 (20.4) | 4 (6.67) | 0.07 |
| Stricture, n (%) | 109 | 12 (11.0) | 5 (10.2) | 7 (11.7) | 0.99 |
| Adhesions, n (%) | 109 | 56 (51.4) | 22 (44.9) | 34 (56.7) | 0.3 |
Notes: Continuous data was represented as median (Interquartile range, IQR) and categorical data was represented as frequency (percentages). P values were based on Chi-squared test (or Fisher’s exact test when cell counts below 5) and Mann-Whitney U-test. IQR was represented as (Quartile 1; Quartile 3)
ROP Type 1 and 2:
Out of the 81 infants included in the analysis, 39.5% (32/81) were diagnosed with Type 1 or 2 ROP. 28 cases were excluded due to other ROP diagnosis. Infants with severe ROP (32/81) exhibited lower median gestational age (23.8 weeks [23.4;24.6] vs. 27.3 weeks [26.3; 29.0], p<0.001) and birth weight (625 grams [512;710] vs.935 grams [700; 1180]; p<0.001) compared to those without severe ROP. Furthermore, a higher exposure to clinical chorioamnionitis was observed in infants with severe ROP (22.6% vs. 2.13%; p<0.006). Infants with severe ROP also had later median onset of ROP diagnosis (63.0 days [47.0;77.2] vs. 29.0 [19.0;41.0]; p=<0.001), received Penrose drain therapy (19 [59.4%] vs. 16 [34.0%]; p=0.046) more frequently, and had a higher incidence of AKI (25 [86.2%] vs.20 [46.5%]; p= 0.002) than those without ROP. Those with severe ROP had lower residual small bowel (70.0 cm [63.1;90.8] vs.90.8 [72.0;101]; p=0.007), lower residual colon (22.7 cm [22.7;24.4] vs. 24.4 cm [22.7;36.0]; p=0.003) than the other group (See Supplemental Table 1).
Oxygen exposure and ROP:
Infants with severe ROP were exposed to higher FiO2 at seven days after birth (44 [30;57] vs. 25[21;35]; p=0.001) and were intubated longer (12.5 days [7.75;17.8] vs. 3.5 days [1.00;4.75]; p<0.001) before NEC and were exposed to a longer duration of invasive (47.0 days [33.0;70.0] vs. 16.0 days [8.50;45.8];p0.001), non-invasive ventilation (60.5 days [37.5;83.0]vs. 24 days [9.00;42.5];p=0.005) and higher FiO2 at two weeks (30 [25.0;38.0] vs. 25 [21.0;30.5];p=0.007) following NEC diagnosis compared to those without severe ROP.
There were no statistically significant differences in the intestinal histopathology, postoperative features such as time to reach feeds and parenteral nutrition dependence, BPD, white matter and grey matter injury on brain MRI, length of stay, and mortality between infants with severe ROP and those without. The data are shown in Table 3.
Table 3:
Oxygen and Ventilation data
| All, N=109 | No ROP, N=49 | Any ROP, N=60 | P Value | |
|---|---|---|---|---|
| Day 7 Fio2 (median [IQR]) | 30.0 [21.5;39.0] | 21.0 [21.0;30.0] | 35.0 [29.0;46.5] | 0.001 |
| Fio2 Admission Out born (median [IQR]) | 44.5 [29.0;68.8] | 32.0 [27.5;43.8] | 51.0 [30.0;75.8] | 0.09 |
| Invasive ventilation duration before NEC (median [IQR]) | 7.00 [4.00;13.8] | 3.50 [1.00;4.75] | 8.50 [6.50;15.0] | <0.001 |
| Non-invasive duration before NEC (median [IQR]) | 8.00 [3.25;15.5] | 9.50 [6.25;16.2] | 3.50 [2.75;10.0] | 0.19 |
| Fio2 7 days before NEC (median [IQR]) | 25.5 [21.0;39.5] | 23.0 [21.0;33.2] | 28.0 [22.8;39.5] | 0.28 |
| Invasive vent duration after NEC (days) (median [IQR]) | 39.0 [12.0;57.0] | 16.0 [8.50;45.8] | 45.0 [18.0;65.0] | 0.001 |
| Non-invasive duration after NEC (median [IQR]) | 46.0 [22.0;73.0] | 24.0 [9.00;42.5] | 62.0 [38.5;99.5] | 0.001 |
| Fio2 after 2 weeks NEC (median [IQR]) | 29.0 [23.0;36.0] | 25.0 [21.0;30.5] | 30.0 [25.0;38.0] | 0.002 |
| BPD, n (%) | 0.05 | |||
| No BPD | 12 (15.0) | 8 (23.5) | 4 (8.70) | |
| Mild | 9 (11.2) | 1 (2.94) | 8 (17.4) | |
| Moderate | 19 (23.8) | 10 (29.4) | 9 (19.6) | |
| Severe | 40 (50.0) | 15 (44.1) | 25 (54.3) | |
| Postnatal use of steroids, n (%) | 68 (63.0) | 29 (59.2) | 39 (66.1) | 0.58 |
| Type of Steroid Used, n (%) | 0.99 | |||
| Hydrocortisone | 58 (85.3) | 26 (86.7) | 32 (84.2) | |
| Dexamethasone | 10 (14.7) | 4 (13.3) | 6 (15.8) |
Notes: Continuous data was represented as median (Interquartile range, IQR) and categorical data was represented as frequency (percentages).
P values were based on Chi-squared test (or Fisher’s exact test when cell counts below 5) and Mann-Whitney U-test
IQR represented as (Quartile 1; Quartile 3)
Growth outcomes and Severe ROP:
The preterm infants with severe (type 1 and type 2) ROP had significantly lower length and head circumference z scores before and following NEC. However, weight for length Z scores were significantly lower for infants with severe ROP than the other group. The data has been summarized in Figure 2 and Table 4.
Figure 2.
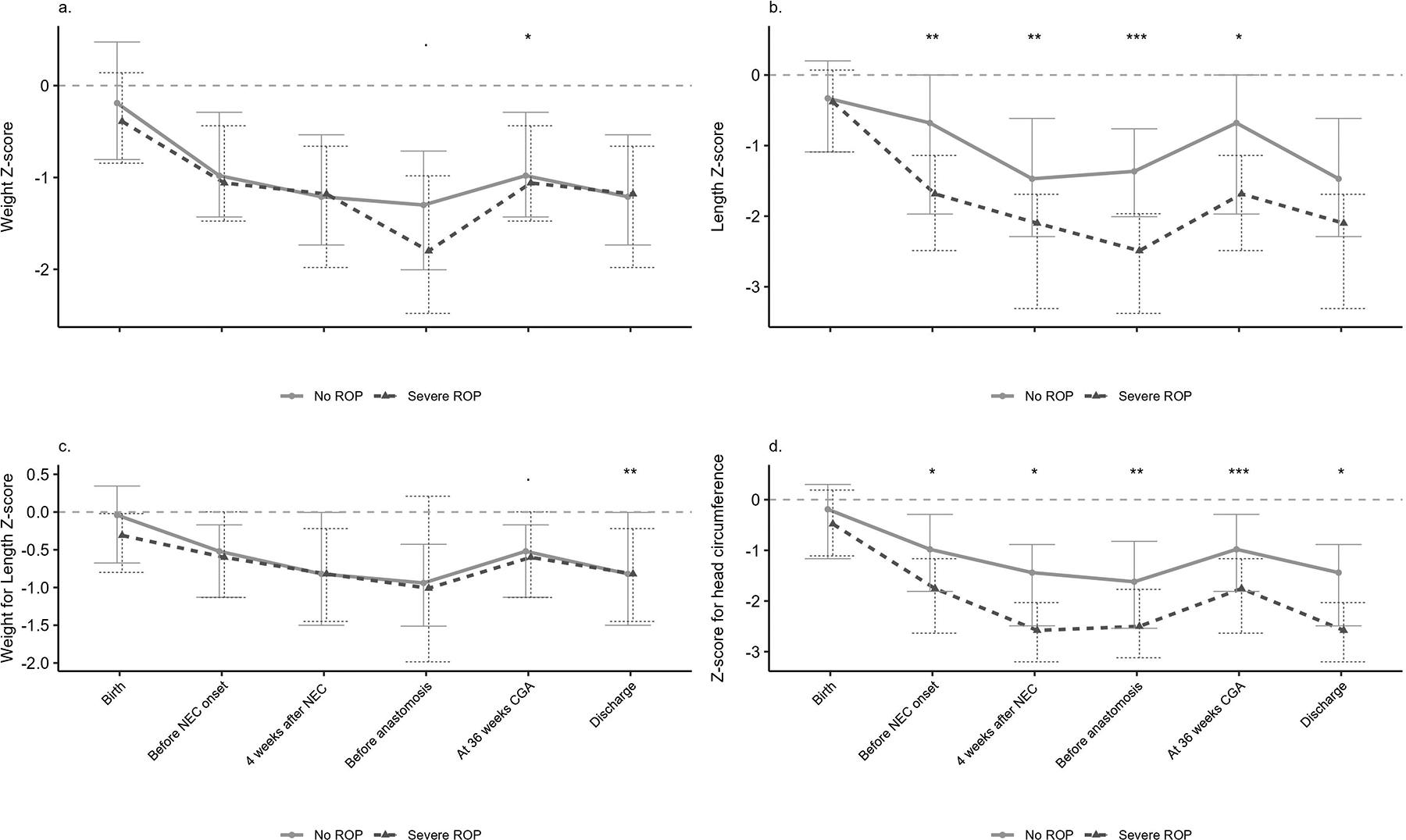
Growth trajectory of weight z-score, length z-score, weight for length z-score and z-score for head circumference by severe ROP. (Note. symbols are represented as ranges of P values i.e. 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ‘ 1)
Table 4:
Growth Parameters in infants with and without severe ROP
| NEC + SIP | NEC Cohort | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | No ROP | Type 1 or 2 ROP | No ROP | Type 1 or 2 ROP | ||||||
| At birth | n | n=66 | n=39 | n=27 | p | n | n=46 | n=28 | n=18 | p |
| Weight (z score) | 66 | −0.32 [−0.82;0.41] | −0.19 [−0.80;0.48] | −0.39 [−0.84;0.14] | 0.49 | 46 | −0.36 [−0.96;0.28] | −0.24 [−0.96;0.34] | −0.44 [−1.24;0.08] | 0.73 |
| Total length (cm, median [IQR]) | 66 | 31.6 [30.4;34.5] | 34.0 [31.6;38.2] | 30.5 [28.8;31.2] | <0.001 | 46 | 31.6 [30.1;34.5] | 34.1 [30.9;39.2] | 30.5 [28.8;31.5] | 0.001 |
| Total length (z score) | 66 | −0.37 [−1.11;0.17] | −0.33 [−1.09;0.20] | −0.38 [−1.09;0.07] | 0.56 | 46 | −0.40 [−1.43;0.14] | −0.50 [−1.77;0.14] | −0.32 [−1.21;−0.04] | 0.99 |
| Weight for total length (percentile) | 66 | 41.6 [24.3;61.9] | 50.3 [25.7;63.6] | 36.1 [18.5;45.1] | 0.05 | 46 | 41.7 [22.7;62.4] | 49.3 [26.0;66.0] | 35.1 [15.8;45.3] | 0.09 |
| Weight and total length (z score) | 66 | −0.21 [−0.70;0.33] | −0.04 [−0.68;0.34] | −0.31 [−0.80;−0.02] | 0.24 | 46 | −0.18 [−0.73;0.35] | −0.01 [−0.65;0.42] | −0.31 [−0.88;0.03] | 0.3 |
| Head circumference (cm, median [IQR]) | 66 | 22.5 [21.5;24.0] | 24.0 [22.5;26.8] | 21.5 [21.0;22.2] | <0.001 | 46 | 23.0 [21.5;24.5] | 24.0 [22.4;27.5] | 21.5 [21.5;22.9] | 0.002 |
| Head circumference (z score) | 66 | −0.30 [−1.14;0.30] | −0.19 [−1.17;0.30] | −0.48 [−1.11;0.19] | 0.94 | 46 | −0.36 [−1.24;0.30] | −0.19 [−1.96;0.32] | −0.49 [−1.13;0.00] | 0.89 |
| Before NEC | n=71 | n=41 | n=30 | n=50 | n=30 | n=20 | ||||
| Weight (z score) | 71 | −1.00 [−1.43;−0.36] | −0.98 [−1.43;−0.29] | −1.06 [−1.47;−0.44] | 0.35 | 50 | −1.02 [−1.59;−0.50] | −0.98 [−1.43;−0.28] | −1.31 [−1.68;−0.71] | 0.1 |
| Total length (cm, median [IQR]) | 71 | 35.3 [33.0;39.1] | 37.5 [34.2;41.0] | 33.5 [30.6;35.2] | <0.001 | 50 | 35.4 [33.4;39.5] | 37.5 [34.3;40.8] | 33.8 [30.8;35.1] | 0.001 |
| Total length (z score) | 71 | −1.28 [−2.20;−0.36] | −0.68 [−1.97;0.00] | −1.69 [−2.49;−1.14] | 0.007 | 50 | −1.41 [−2.33;−0.51] | −1.00 [−2.19;−0.05] | −1.72 [−2.80;−1.14] | 0.033 |
| Weight and total length (percentile) | 71 | 28.4 [12.5;45.8] | 29.8 [12.3;43.3] | 27.4 [12.9;50.3] | 0.68 | 50 | 29.0 [12.7;46.4] | 30.1 [13.4;47.8] | 20.8 [11.8;41.9] | 0.44 |
| Weight and total length (z score) | 71 | −0.53 [−1.14;−0.11] | −0.52 [−1.13;−0.17] | −0.60 [−1.13;0.00] | 0.79 | 50 | −0.55 [−1.14;−0.09] | −0.52 [−1.10;−0.06] | −0.82 [−1.19;−0.21] | 0.43 |
| Head circumference (cm, median [IQR]) | 71 | 25.0 [23.0;28.7] | 26.5 [24.2;30.3] | 24.0 [21.5;26.4] | 0.003 | 50 | 25.2 [23.6;28.4] | 26.5 [24.5;30.0] | 24.0 [21.9;26.1] | 0.010 |
| Head circumference (z score) | 71 | −1.43 [−1.98;−0.41] | −0.98 [−1.81;−0.29] | −1.75 [−2.64;−1.17] | 0.014 | 50 | −1.52 [−2.55;−0.41] | −0.99 [−1.77;−0.31] | −1.95 [−2.94;−1.33] | 0.038 |
| 4 weeks after NEC | n=68 | n=39 | n=29 | n=47 | n=28 | n=19 | ||||
| Weight (z score) | 68 | −1.19 [−1.89;−0.64] | −1.21 [−1.74;−0.54] | −1.18 [−1.98;−0.66] | 0.55 | 47 | −1.26 [−1.90;−0.64] | −1.23 [−1.66;−0.55] | −1.37 [−2.03;−0.65] | 0.48 |
| Total length (cm, median [IQR]) | 68 | 40.0 [35.3;43.1] | 42.0 [38.8;44.5] | 36.0 [33.5;40.0] | <0.001 | 47 | 40.0 [35.7;44.0] | 42.1 [40.0;44.6] | 36.0 [34.0;39.2] | <0.001 |
| Total length (z score) | 68 | −1.77 [−2.59;−1.01] | −1.47 [−2.29;−0.62] | −2.10 [−3.31;−1.69] | 0.003 | 47 | −2.04 [−2.64;−1.04] | −1.65 [−2.32;−0.62] | −2.51 [−3.46;−1.73] | 0.012 |
| Weight and total length (percentile) | 68 | 20.3 [6.24;42.7] | 20.7 [6.66;49.9] | 20.1 [5.50;40.4] | 0.88 | 47 | 19.2 [6.66;43.2] | 19.8 [7.48;49.4] | 19.2 [5.44;37.4] | 0.57 |
| Weight and total length (z score) | 68 | −0.82 [−1.49;−0.07] | −0.82 [−1.50;0.00] | −0.82 [−1.45;−0.22] | 0.74 | 47 | −0.84 [−1.47;−0.05] | −0.85 [−1.45;−0.02] | −0.84 [−1.52;−0.13] | 0.96 |
| Head circumference (cm, median [IQR]) | 68 | 28.0 [25.4;30.0] | 29.5 [27.5;32.1] | 26.2 [23.8;28.5] | 0.001 | 47 | 28.0 [26.3;30.6] | 29.5 [27.6;32.3] | 26.9 [24.2;28.4] | 0.005 |
| Head circumference (z score) | 68 | −2.08 [−3.04;−1.05] | −1.44 [−2.49;−0.88] | −2.58 [−3.20;−2.03] | 0.013 | 47 | −2.00 [−2.83;−1.04] | −1.47 [−2.34;−0.98] | −2.44 [−3.27;−1.92] | 0.06 |
| Before reanastomosis | n=56 | n=30 | n=26 | n=37 | n=21 | n=16 | ||||
| Weight (z score) | 56 | −1.48 [−2.19;−0.85] | −1.30 [−2.00;−0.71] | −1.80 [−2.48;−0.98] | 0.1 | 37 | −1.49 [−2.18;−0.87] | −1.30 [−2.16;−0.58] | −1.75 [−2.59;−1.07] | 0.27 |
| Total length (cm, median [IQR]) | 56 | 44.2 [41.5;47.1] | 45.0 [42.0;47.9] | 43.0 [41.1;46.4] | 0.1 | 37 | 44.0 [41.0;47.0] | 46.0 [42.0;48.0] | 41.8 [38.9;44.5] | 0.032 |
| Total length (z score) | 56 | −1.94 [−3.01;−1.13] | −1.36 [−2.01;−0.76] | −2.49 [−3.38;−1.96] | <0.001 | 37 | −2.10 [−3.06;−1.05] | −1.44 [−2.18;−0.75] | −2.91 [−3.48;−2.33] | <0.001 |
| Weight and total length (percentile) | 56 | 17.4 [3.69;42.0] | 17.4 [6.52;33.5] | 15.8 [2.35;58.1] | 0.83 | 37 | 16.9 [2.59;42.7] | 16.9 [3.01;35.2] | 15.8 [2.51;52.6] | 0.76 |
| Weight and total length (z score) | 56 | −0.94 [−1.79;−0.20] | −0.94 [−1.51;−0.43] | −1.01 [−1.98;0.21] | 0.82 | 37 | −0.96 [−1.94;−0.18] | −0.96 [−1.88;−0.38] | −1.01 [−1.96;0.07] | 0.77 |
| Head circumference (cm, median [IQR]) | 56 | 30.6 [28.6;32.6] | 30.8 [30.0;33.5] | 30.1 [28.5;31.7] | 0.27 | 37 | 30.5 [28.7;31.8] | 30.5 [30.0;33.5] | 29.7 [27.6;31.6] | 0.3 |
| Head circumference (z score) | 56 | −2.19 [−2.79;−1.21] | −1.62 [−2.54;−0.82] | −2.50 [−3.12;−1.77] | 0.008 | 37 | −2.26 [−2.92;−1.52] | −1.90 [−2.86;−0.98] | −2.41 [−3.23;−1.95] | 0.1 |
| At 36 weeks | n=65 | n=35 | n=30 | n=46 | n=26 | n=20 | ||||
| Weight (z score) | 65 | −1.43 [−2.00;−0.76] | −1.05 [−1.71;−0.62] | −1.73 [−2.31;−1.07] | 0.027 | 46 | −1.50 [−2.11;−0.68] | −1.12 [−1.84;−0.47] | −1.86 [−2.55;−1.13] | 0.037 |
| Total length (cm, median [IQR]) | 65 | 42.3 [40.0;44.5] | 43.0 [41.5;45.0] | 41.3 [40.0;43.0] | 0.008 | 46 | 42.0 [40.0;44.9] | 43.1 [41.2;45.0] | 41.3 [39.8;43.0] | 0.040 |
| Total length (z score) | 65 | −1.67 [−2.60;−1.09] | −1.50 [−2.21;−0.76] | −2.21 [−3.21;−1.34] | 0.035 | 46 | −1.83 [−3.02;−0.84] | −1.63 [−2.30;−0.63] | −2.35 [−3.34;−1.50] | 0.09 |
| Weight and total length (percentile) | 65 | 16.8 [3.88;37.3] | 23.2 [8.14;43.1] | 10.7 [2.46;33.0] | 0.08 | 46 | 16.2 [2.96;42.0] | 23.2 [4.24;46.9] | 8.02 [2.05;25.6] | 0.049 |
| Weight and total length (z score) | 65 | −0.96 [−1.76;−0.32] | −0.73 [−1.44;−0.17] | −1.25 [−1.97;−0.45] | 0.08 | 46 | −0.98 [−1.89;−0.20] | −0.73 [−1.72;−0.08] | −1.40 [−2.08;−0.66] | 0.05 |
| Head circumference (cm, median [IQR]) | 65 | 29.5 [28.3;31.5] | 31.0 [29.4;31.9] | 28.8 [27.6;29.5] | 0.001 | 46 | 29.5 [28.2;31.7] | 30.5 [29.1;31.8] | 29.0 [27.3;29.6] | 0.029 |
| Head circumference (z score) | 65 | −1.96 [−2.75;−0.85] | −1.32 [−2.24;−0.45] | −2.60 [−3.35;−2.02] | 0.001 | 46 | −2.04 [−2.88;−0.66] | −1.40 [−2.55;−0.45] | −2.52 [−3.63;−1.98] | 0.027 |
| Discharge | n=63 | n=35 | n=28 | n=43 | n=25 | n=18 | ||||
| Weight (z score) | 63 | −1.69 [−2.67;−0.63] | −1.63 [−2.66;−0.66] | −1.90 [−2.66;−0.19] | 0.98 | 43 | −1.87 [−2.98;−0.89] | −1.68 [−2.94;−0.65] | −2.02 [−2.98;−1.61] | 0.48 |
| Total length (cm, median [IQR]) | 63 | 51.5 [49.5;58.9] | 51.5 [48.4;58.9] | 51.6 [49.9;57.5] | 0.63 | 43 | 52.0 [49.5;56.4] | 54.2 [50.0;60.0] | 50.5 [49.5;53.8] | 0.13 |
| Total length (z score) | 63 | −1.74 [−3.46;−0.92] | −1.57 [−3.33;−0.59] | −2.34 [−3.46;−1.53] | 0.14 | 43 | −2.38 [−3.60;−1.50] | −1.71 [−3.66;−0.99] | −2.90 [−3.46;−1.94] | 0.16 |
| Weight and total length (percentile) | 63 | 48.2 [13.6;93.8] | 22.0 [3.18;71.0] | 77.5 [46.7;97.6] | 0.003 | 43 | 59.0 [20.6;95.4] | 28.7 [5.80;94.0] | 76.7 [43.6;97.9] | 0.07 |
| Weight and total length (z score) | 63 | 0.02 [−1.33;1.54] | −0.77 [−1.91;0.55] | 0.76 [0.00;1.97] | 0.002 | 43 | 0.24 [−0.98;1.71] | −0.63 [−2.18;1.56] | 0.74 [0.02;2.05] | 0.06 |
| Head circumference (cm, median [IQR]) | 63 | 35.7 [34.0;38.5] | 35.5 [34.0;38.0] | 36.1 [34.0;38.6] | 0.61 | 43 | 36.0 [34.0;38.0] | 36.5 [34.5;38.5] | 35.0 [33.7;37.0] | 0.23 |
| Head circumference (z score) | 63 | −2.02 [−3.21;−1.06] | −1.64 [−2.63;−0.33] | −2.40 [−3.36;−1.69] | 0.031 | 43 | −2.02 [−3.49;−1.16] | −1.81 [−3.29;−0.51] | −2.57 [−3.66;−1.72] | 0.18 |
Notes: All continuous data was represented as median (Interquartile range, IQR). P values were based on Mann-Whitney U-test. IQR was represented as (Quartile 1; Quartile 3)
Multivariable Analysis:
After adjusting for other covariates using Firth’s logistic regression, gestational age (aOR= 0.51, 95% CI [0.35–0.76], p<0.001) demonstrated a significant inverse association with the occurrence of any ROP. Conversely, the day of diagnosis of severe ROP following NEC (aOR=1.08, 95% CI [1.03 −1.13], p=0.005) was positively associated with the occurrence of any ROP. Acute kidney injury as determined by serum creatinine, FiO2 requirements at 7 days of life, and the duration of invasive ventilation following NEC did not show a statistically significant association with ROP. The data has been summarized in Table 5.
Table 5:
Association between any ROP in infants with NEC/SIP and related factors using Firth’s logistic regression
| Predictors | aOR | 95% CI | P value |
|---|---|---|---|
| Fio2 at day 7 of life | 1.03 | 0.99 – 1.07 | 0.13 |
| Gestational age | 0.51 | 0.35 – 0.76 | <0.001 |
| Day of severe ROP diagnosis after birth | 1.08 | 1.03 – 1.13 | 0.005 |
| Invasive ventilation after birth | 0.99 | 0.97 – 1.01 | 0.436 |
| AKI by serum creatinine | 3.79 | 0.71 – 20.09 | 0.128 |
Reference category was set to no ROP group.
aOR represents adjusted odds ratio and CI represents confidence interval.
NEC cohort:
Out of the 77 infants included in the analysis, 50.6% (39/77) were diagnosed with any form of ROP. Among these, 38.5% (15/39) had Type 1 ROP and 15.4% (6/39) had Type 2 ROP. Regarding the treatment, 28.2% (11/39) of the infants received laser therapy, while 17.9% (7/39) were treated with the Avastin(bevacizumab)® medication. Additionally, 7.69% (3/39) of the infants underwent both laser and Avastin(bevacizumab)® treatments.
Any ROP:
Preterm infants diagnosed with any ROP had a lower median gestational age (24.4 weeks [23.6;25.8] vs. 27.5 weeks [26.4;29.6]; p<0.001) and lower median birth weight (670 grams [585;760] vs. 938 grams [688; 1300]; p<0.001) than those without ROP. The data are shown in Supplemental Table 2.
Severe ROP:
21/59 (35.5%) infants had severe ROP. Those with severe ROP had lower median gestational age (24 weeks [23.5;25.2] vs. 27.5 weeks [26.4;29.6]; p<0.001), lower median birth weight (640 grams [519;710] vs. 938 grams [688;1300], <0.001), were diagnosed at later median of life (81days [69.0;94.0] vs. 43.5 days [40.0;47.8]; p<0.001). The data are summarized in Supplemental Table 3.
The ROP information of infants with and without surgical NEC/SIP has been summarized in Supplemental Table 4.
Growth Outcomes:
In the NEC cohort, the weight z scores and weight for length percentiles were significantly lower at 36 weeks corrected gestational age for the preterm infants with severe ROP. The length z scores were significantly lower before and four weeks following NEC diagnosis and at the time of re-anastomosis. The data has been summarized in Table 4.
Discussion:
In our cohort of infants with surgical NEC/SIP, more than half developed ROP, but 45% did not develop any ROP. One-third of infants were diagnosed with severe ROP, of which type 1 ROP was more common. Nearly a third of the infants with severe ROP received laser treatment, and one-fifth received bevacizumab. Infants with severe ROP were smaller and younger. They were exposed to prenatal risk factors such as PIH, chorioamnionitis, and postnatal risk factors including PDA, indomethacin, AKI, more FiO2, and longer invasive and non-invasive mechanical ventilation duration. Additionally, infants with surgical NEC were diagnosed with severe ROP almost six weeks later than those without severe ROP. Infants with NEC/SIP with severe ROP also grew less well, demonstrated by lower weight z scores and linear growth before and after the NEC onset. These highly suggest systemic inflammatory response triggered by NEC, which has multiorgan system effects.
Published reports show that the prematurity and the percent and duration of oxygen exposure influence the incidence of ROP in preterm infants [7, 28]. The studies have demonstrated the relationship between the oxygen and the ROP with phase I (hyperoxia-induced vasoconstriction and ischemic injury) and phase II (vascular endothelial growth factor–driven Vaso proliferation) of the disease [7].
In our cohort, infants with ROP were exposed to higher FiO2 and ventilated more commonly before and after the NEC onset. In multivariate analysis, however, oxygen exposure was not a significant risk for the development of severe ROP. The possible explanation may be most likely due to three factors. Firstly, it may be due to involvement of clinical factors other than total oxygen exposure; Secondly, we failed to model the in -vivo oxygen saturation accurately and thirdly small sample size in the regression models as noted by Chen et al. [28].
In our cohort, the infants with severe ROP were younger (23.8 weeks vs. 27.3 weeks) and had lower birth weights (625 grams vs.935 grams) than those without severe ROP, as reported in a previously published report [29]. A study of discordant twin pairs reported that gestational age predicts ROP severity more accurately than birth weight [30]. In a prospective study from the Australian and New Zealand Neonatal Network, Darlow et al. reported that prematurity was the dominant risk factor, with infants with GA of <25 weeks having 20 times greater odds of severe ROP than infants with GA of 28 weeks. Birth weight for GA also had a “dose-response” effect placing the more growth-restricted infants at greater risk such that infants ≤ 3rd weight percentile for GA had four times greater odds of developing severe ROP than in the 25th to 75th percentiles. Although we did not identify sex as a contributor to ROP among NEC infants, male sex was identified as a significant risk factor in at least one prior study [31].
Within our cohort, infants with severe ROP experienced poor growth, evidenced by lower length and head circumference z scores before and following the NEC/SIP onset. The infants were also exposed to chorioamnionitis, similar to a recent prospective study reporting that slower length gain and maternal chorioamnionitis were associated with delayed regression and complete retina vascularization in preterm infants [32]. In this cohort, the weight z scores and weight for length percentiles were significantly lower at 36 weeks corrected gestational age for the preterm infants with severe ROP. Poor weight gain postnatally shares a known association with severe ROP [33–35]. Given that poor postnatal weight gain is linked to persistently low serum IGF-1 in preterm infants, it is conceivable that the poor weight experienced in infants with NEC is a marker for retinal IGF-1 insufficiency and the resultant incomplete VEGF signaling aberrant vascular development of ROP [36].
The presence and timing of NEC requiring surgery is a significant risk factor for ROP development in preterm infants [10, 11]. Fundora et al. [11] reported that infants with early surgical NEC (8–28 days) had the highest risk of developing any ROP and severe ROP. In our cohort, infants with severe ROP had a median age of diagnosis of 23 days vs. 11 days for infants with no ROP, although the differences did not reach statistical significance. Several studies have shown that preterm infants with surgical NEC have severe white matter injury on the brain MRI, higher serum pro-inflammatory markers, and poor neurodevelopmental outcome at two years of corrected age [27, 37–40]. Animal studies have reported surgical NEC leads to systemic inflammation and causes neuronal injury via microglial activation, inflammatory pathway activation, and brain barrier disruption [41–44]. The presence of AKI following NEC/SIP onset was most likely associated with the severe ROP on bivariate analysis, which may most likely be explained due to systemic inflammation initiated secondary to NEC/SIP affecting kidneys and retina leading to multiple systemic morbidities Mechanistically, we hypothesize that severe acute kidney injury in neonates with surgical NEC may exacerbate the injury by acting as a catalyst or modifier of retinal inflammation. Further studies are needed to understand the role between severe kidney injury and ROP in preterm infants with surgical NEC.
Our study’s strengths include a broad evaluation of clinical and growth parameters known or hypothesized to be associated with severe ROP. Nonetheless, our study has important limitations. First, this is a single-center experience, potentially limiting the study’s generalizability. Secondly, sample size limits our power to detect associations between clinical factors, NEC, and ROP, which may result in type I errors. Thirdly, in our cohort, three -fourth of the infants with surgical NEC were African American. While this is likely partly due to the demographics of Mississippi, this may also be related to adverse social determinants of health.
In conclusion, our study found that ROP developed in more than half of infants with surgical NEC/SIP, with Type 1 disease being the most common. Affected infants tended to be smaller, younger, and exposed to prenatal and postnatal risk. In addition, those with severe ROP grew poorly before and after the NEC diagnosis. These findings highlight the need to develop risk factor-based strategies such as kidney protective strategies and optimizing the use of Fio2 to identify infants at greater risk of severe ROP to improve short and long-term outcomes. Furthermore, to improve ophthalmologic outcomes, preterm infants at risk need to maintain adequate weight gain, linear growth, and nutrition in accordance with local protocols to help prevent ROP in infants with NEC/SIP.
Supplementary Material
Acknowledgment:
The Mississippi Center for Clinical and Translational Research for supporting NEC research.
Funding:
Dr. Parvesh Mohan Garg is partially supported by the NIGMS of the NIH under Award Number 5U54GM115428. The content is solely the authors’ responsibility and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Conflicts of interest: The authors disclose no conflicts.
Consent: Patient consent is not required as per IRB
References:
- 1.Neu J and Walker WA, Necrotizing enterocolitis. N Engl J Med, 2011. 364(3): p. 255–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sankaran K, et al. , Variations in incidence of necrotizing enterocolitis in Canadian neonatal intensive care units. J Pediatr Gastroenterol Nutr, 2004. 39(4): p. 366–72. [DOI] [PubMed] [Google Scholar]
- 3.Mowitz ME, Dukhovny D, and Zupancic JAF, The cost of necrotizing enterocolitis in premature infants. Semin Fetal Neonatal Med, 2018. 23(6): p. 416–419. [DOI] [PubMed] [Google Scholar]
- 4.Garg PM, et al. , Incomplete resection of necrotic bowel may increase mortality in infants with necrotizing enterocolitis. Pediatr Res, 2021. 89(1): p. 163–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Garg PM, et al. , Clinical determinants and impact of hemorrhagic lesions on intestinal pathology in preterm infants with surgical necrotizing enterocolitis. J Neonatal Perinatal Med, 2023. 16(1): p. 119–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Garg PM, et al. , Clinical and histopathological correlates of intestinal repair in preterm infants following surgical necrotizing enterocolitis. J Matern Fetal Neonatal Med, 2022. 35(26): p. 10565–10576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hartnett ME and Penn JS, Mechanisms and management of retinopathy of prematurity. N Engl J Med, 2012. 367(26): p. 2515–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Good WV, et al. , The incidence and course of retinopathy of prematurity: findings from the early treatment for retinopathy of prematurity study. Pediatrics, 2005. 116(1): p. 15–23. [DOI] [PubMed] [Google Scholar]
- 9.Bell EF, et al. , Mortality, In-Hospital Morbidity, Care Practices, and 2-Year Outcomes for Extremely Preterm Infants in the US, 2013–2018. Jama, 2022. 327(3): p. 248–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yucel OE, et al. , Incidence and risk factors for retinopathy of prematurity in premature, extremely low birth weight and extremely low gestational age infants. BMC Ophthalmol, 2022. 22(1): p. 367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fundora JB, et al. , Association of Surgical Necrotizing Enterocolitis and its Timing with Retinopathy of Prematurity. Am J Perinatol, 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pammi M, et al. , Intestinal dysbiosis in preterm infants preceding necrotizing enterocolitis: a systematic review and meta-analysis. Microbiome, 2017. 5(1): p. 31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bell M, et al. , Neurodevelopmental and Growth Outcomes of Extremely Preterm Infants with Short Bowel Syndrome. J Pediatr, 2021. 230: p. 76–83.e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhang JY, Greenwald MJ, and Rodriguez SH, Gut Microbiome and Retinopathy of Prematurity. Am J Pathol, 2023. [DOI] [PubMed] [Google Scholar]
- 15.Wongnophirun A, et al. , Association between severe retinopathy of prematurity and postnatal weight gain in very low-birthweight infants at Chiang Mai University Hospital, Thailand. Paediatr Int Child Health, 2020. 40(2): p. 85–91. [DOI] [PubMed] [Google Scholar]
- 16.Aydemir O, et al. , Adjusted poor weight gain for birth weight and gestational age as a predictor of severe ROP in VLBW infants. Eye (Lond), 2011. 25(6): p. 725–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bell MJ, et al. , Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg, 1978. 187(1): p. 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Remon JI, et al. , Depth of bacterial invasion in resected intestinal tissue predicts mortality in surgical necrotizing enterocolitis. J Perinatol, 2015. 35(9): p. 755–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Revised indications for the treatment of retinopathy of prematurity: results of the early treatment for retinopathy of prematurity randomized trial. Arch Ophthalmol, 2003. 121(12): p. 1684–94. [DOI] [PubMed] [Google Scholar]
- 20.Selewski DT, et al. , Neonatal Acute Kidney Injury. Pediatrics, 2015. 136(2): p. e463–73. [DOI] [PubMed] [Google Scholar]
- 21.Jetton JG, et al. , Incidence and outcomes of neonatal acute kidney injury (AWAKEN): a multicentre, multinational, observational cohort study. Lancet Child Adolesc Health, 2017. 1(3): p. 184–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Jetton JG, et al. , Assessment of Worldwide Acute Kidney Injury Epidemiology in Neonates: Design of a Retrospective Cohort Study. Front Pediatr, 2016. 4: p. 68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jetton JG and Askenazi DJ, Acute kidney injury in the neonate. Clin Perinatol, 2014. 41(3): p. 487–502. [DOI] [PubMed] [Google Scholar]
- 24.Zappitelli M, et al. , Developing a neonatal acute kidney injury research definition: a report from the NIDDK neonatal AKI workshop. Pediatr Res, 2017. 82(4): p. 569–573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Jobe AH and Bancalari E, Bronchopulmonary dysplasia. Am J Respir Crit Care Med, 2001. 163(7): p. 1723–9. [DOI] [PubMed] [Google Scholar]
- 26.Villar J, et al. , Monitoring the Postnatal Growth of Preterm Infants: A Paradigm Change. Pediatrics, 2018. 141(2). [DOI] [PubMed] [Google Scholar]
- 27.Woodward LJ, et al. , Neonatal MRI to predict neurodevelopmental outcomes in preterm infants. N Engl J Med, 2006. 355(7): p. 685–94. [DOI] [PubMed] [Google Scholar]
- 28.Chen JS, et al. , Quantification of Early Neonatal Oxygen Exposure as a Risk Factor for Retinopathy of Prematurity Requiring Treatment. Ophthalmol Sci, 2021. 1(4): p. 100070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sabri K, et al. , Retinopathy of Prematurity: A Global Perspective and Recent Developments. Pediatrics, 2022. 150(3). [DOI] [PubMed] [Google Scholar]
- 30.Wang ZH, Li YY, and Liu ZM, Birth weight and gestational age on retinopathy of prematurity in discordant twins in China. Int J Ophthalmol, 2014. 7(4): p. 663–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Darlow BA, et al. , Prenatal risk factors for severe retinopathy of prematurity among very preterm infants of the Australian and New Zealand Neonatal Network. Pediatrics, 2005. 115(4): p. 990–6. [DOI] [PubMed] [Google Scholar]
- 32.Schoephoerster J, et al. , Identification of clinical factors associated with timing and duration of spontaneous regression of retinopathy of prematurity not requiring treatment. J Perinatol, 2023. [DOI] [PubMed] [Google Scholar]
- 33.Sethi NK, et al. , Study to evaluate the relation between weight gain in infants and occurrence of retinopathy of prematurity. Indian J Ophthalmol, 2023. 71(3): p. 890–894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wallace DK, et al. , Poor postnatal weight gain: a risk factor for severe retinopathy of prematurity. J aapos, 2000. 4(6): p. 343–7. [DOI] [PubMed] [Google Scholar]
- 35.Lin L and Binenbaum G, Postnatal weight gain and retinopathy of prematurity. Semin Perinatol, 2019. 43(6): p. 352–359. [DOI] [PubMed] [Google Scholar]
- 36.Smith LE, et al. , Regulation of vascular endothelial growth factor-dependent retinal neovascularization by insulin-like growth factor-1 receptor. Nat Med, 1999. 5(12): p. 1390–5. [DOI] [PubMed] [Google Scholar]
- 37.Hintz SR, et al. , Neuroimaging and neurodevelopmental outcome in extremely preterm infants. Pediatrics, 2015. 135(1): p. e32–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Shin SH, et al. , Surgical Necrotizing Enterocolitis versus Spontaneous Intestinal Perforation in White Matter Injury on Brain Magnetic Resonance Imaging. Neonatology, 2016. 110(2): p. 148–54. [DOI] [PubMed] [Google Scholar]
- 39.Merhar SL, et al. , Brain magnetic resonance imaging in infants with surgical necrotizing enterocolitis or spontaneous intestinal perforation versus medical necrotizing enterocolitis. J Pediatr, 2014. 164(2): p. 410–2.e1. [DOI] [PubMed] [Google Scholar]
- 40.Maheshwari A, et al. , Cytokines associated with necrotizing enterocolitis in extremely-low-birth-weight infants. Pediatr Res, 2014. 76(1): p. 100–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Adén U, et al. , Systemic inflammation sensitizes the neonatal brain to excitotoxicity through a pro-/anti-inflammatory imbalance: key role of TNFalpha pathway and protection by etanercept. Brain Behav Immun, 2010. 24(5): p. 747–58. [DOI] [PubMed] [Google Scholar]
- 42.Brunse A, Abbaspour A, and Sangild PT, Brain Barrier Disruption and Region-Specific Neuronal Degeneration during Necrotizing Enterocolitis in Preterm Pigs. Dev Neurosci, 2018. 40(3): p. 198–208. [DOI] [PubMed] [Google Scholar]
- 43.Niño DF, et al. , Cognitive impairments induced by necrotizing enterocolitis can be prevented by inhibiting microglial activation in mouse brain. Sci Transl Med, 2018. 10(471). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Biouss G, et al. , Experimental necrotizing enterocolitis induces neuroinflammation in the neonatal brain. J Neuroinflammation, 2019. 16(1): p. 97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.