

Abstract
Context: Overhead activities such as throwing, tennis, or volleyball place athletes at considerable risk for overuse injuries. A relationship between scapulothoracic muscle imbalance and shoulder pain has been suggested.
Objective: To compare the isokinetic muscle performance of the scapular muscles between overhead athletes with impingement symptoms and uninjured overhead athletes and to identify strength deficits in the patient population.
Design: A repeated-measures analysis of variance with 1 within-subjects factor (side) and 1 between-subjects factor (group) was used to compare strength values and agonist:antagonist ratios across sides and across groups.
Setting: University laboratory.
Patients or Other Participants: Thirty overhead athletes with chronic shoulder impingement symptoms and 30 overhead athletes without a history of shoulder pain.
Intervention(s): A linear protraction-retraction movement in the scapular plane at 2 velocities (12.2 cm/s and 36.6 cm/s).
Main Outcome Measure(s): Isokinetic strength values and protraction:retraction ratios for both velocities.
Results: Overhead athletes with impingement symptoms showed decreased force output:body weight at both velocities in the protractor muscles on the injured side compared with the uninjured side (−13.7% at slow velocity, −15.5% at high velocity) and compared with the control group at high velocity (−20.7%). On both sides, the patient group had significantly lower protraction:retraction ratios than the control group, measured at slow velocity (nondominant = −11%, dominant = −13.7%).
Conclusions: Overhead athletes with impingement symptoms demonstrated strength deficits and muscular imbalance in the scapular muscles compared with uninjured athletes.
Keywords: shoulder, glenohumeral joint
Athletes involved in repetitive overhead activities place unique demands on the shoulder girdle.1 Overhead activities such as throwing, tennis, or volleyball place the athlete at considerable risk of overuse injuries.2,3 The glenohumeral joint is inherently unstable, and stability is provided predominantly by the ligamentous, capsular, and muscular structures and by the relative position of the glenoid and the arm through all arm motions.4 These dynamic constraints include not only the dynamic musculotendinous units of the rotator cuff but also the force couples provided by the scapulothoracic muscles.4,5 The quality of neuromuscular control around the scapula depends on several factors that determine scapular muscle balance. Balanced force production between protractors and retractors is a primary necessity but not the sole condition for muscle balance. In addition, balanced muscle activity among the 3 trapezius parts is necessary for scapular stability. Moreover, balanced timing of muscle recruitment among the scapular muscles is a crucial component of dynamic stability of the scapula throughout arm motion.4–8 In the clinical literature, a relationship of scapulothoracic muscle imbalance to shoulder pain has often been suggested.4–7 These imbalances result in scapular instability, potentially increasing the risk of shoulder problems, and would be present in timing properties as well as in force output and proportional electromyographic activity. Recently, Cools et al9 examined isokinetic muscle performance in the scapular rotators in a population of overhead athletes with impingement symptoms. The injured side showed a significant decrease in force output of the protractors measured at high velocity, suggesting decreased muscle performance in the serratus anterior muscle. In addition, a significantly lower protraction:retraction ratio was present on the injured side than on the uninjured side. However, only side-to-side comparisons were performed because comparative data from a control group consisting of healthy overhead athletes were not available. Therefore, our main objective was to examine the force output and muscle balance of the scapulothoracic muscles in overhead athletes with impingement symptoms in their dominant shoulders and to compare these results with a healthy control group active in overhead sports.
METHODS
Subjects
Both shoulders from a total of 60 subjects were tested. The patient group consisted of 30 overhead athletes in various overhead sports (21 males, 9 females) with unilateral shoulder pain on the dominant side. The average age was 23.6 years (range, 18–35 years). Subjects consisted of 19 volleyball players, 6 tennis players, and 5 athletes in other overhead sports. Thirty healthy overhead athletes with no history of shoulder injuries (18 males, 12 females) served as the control group. The average age was 23.2 years (range, 18–31 years). Subjects consisted of 15 volleyball players, 8 tennis players, and 7 athletes in other overhead sports.
All subjects completed questionnaires regarding their shoulder pain, training, and athletic activities. The demographic characteristics of both groups of subjects are presented in Table 1.
Table 1. Anthropometric and Demographic Characteristics of the Patient (n = 30) and Control Groups (n = 30).

Patients were included in the impingement group if they had at least 2 of the following 5 criteria9–14:
Positive Neer sign: reproduction of pain when the examiner passively flexes the humerus to end range with overpressure
Positive Hawkins sign: reproduction of pain when the shoulder is passively placed in 90° of forward flexion and internally rotated to end range
Positive Jobe sign: reproduction of pain and lack of force production with isometric elevation in the scapular plane in internal rotation (empty can)
Pain with apprehension: reproduction of pain when an anteriorly directed force is applied to the proximal humerus in the position of 90° of abduction and 90° of external rotation
Positive relocation test: reduction in pain after a positive apprehension test when a posteriorly directed force is applied to the proximal humerus in the position of 90°/90°
For inclusion, at least 1 impingement sign needed to be positive, along with a second positive impingement test or a painful apprehension or positive relocation test. Patients with minor instability and secondary impingement are thought to experience pain but not apprehension with these tests.15,16
Subjects were excluded from the patient group if they had a history of shoulder dislocation, shoulder surgery, current symptoms related to the cervical spine, or documented structural injuries to the shoulder complex. All subjects gave their written informed consent to participate in this study. The study was approved by the Ethical Committee of the Ghent University.
Testing Procedure
All isokinetic tests were performed using a Biodex System 3 isokinetic dynamometer (Biodex Medical Systems, Inc, Shirley, NY). The testing session started with a warm-up procedure, consisting of shoulder movements in all directions, push-up exercises against the wall, and stretching exercises for the rotator cuff and scapular muscles. The uninjured shoulder was tested first, followed by the injured shoulder. In the control group, the nondominant shoulder was tested first, followed by the dominant shoulder.
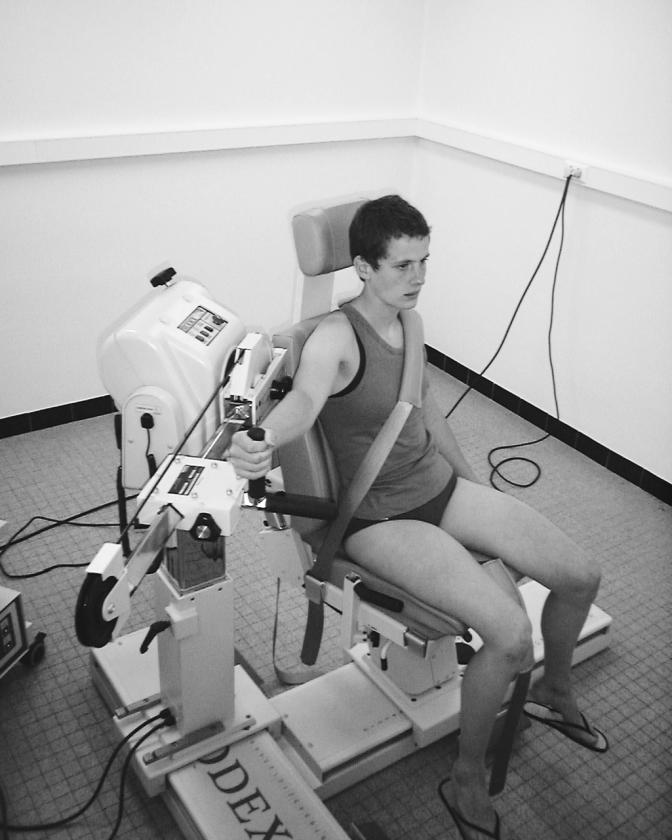
For the testing procedure, the closed chain attachment was fixed to the isokinetic dynamometer in a horizontal position. The handgrip was inserted into the attachment receiving tube with the neutral handle facing up in order to keep the glenohumeral joint in a neutral rotational position. The chair was rotated to 15° and the dynamometer to 45° (Figure). The subject was assessed in the seated position with the arm horizontal in the scapular plane (30° anterior to the frontal plane). The subject was instructed to keep the elbows extended. Stabilization of the trunk was obtained using a strap diagonally from the contralateral shoulder across the chest. Each subject was first tested at 12.2 cm/s (angular velocity of 60°/s), followed by the second test at 36.6 cm/s (angular velocity of 180°/s). Range of motion was assessed by asking subjects to perform a maximal protraction and a maximal retraction movement. Gravity correction was not performed because the movement occurred in a horizontal plane. The test started in a maximal retracted position, and the subjects were instructed to perform maximal protraction and retraction movements over the total range of motion. Five repetitions were performed at the linear velocity of 12.2 cm/s and, after a resting period of 10 seconds, 10 repetitions at a linear velocity of 36.6 cm/s. All movements were performed in the concentric-concentric mode: protraction and retraction movements were performed with concentric muscle activity. Subjects performed 5 familiarization trials before data collection, and they all benefited from verbal encouragement. Visual feedback from the computer screen was not allowed. In a previous study,17 the test-retest reproducibility of this procedure was good to excellent for the peak force values (intraclass correlation coefficient = .88–.96).
Experimental setup for the isokinetic protraction-retraction movement in the scapular plane using a Biodex isokinetic dynamometer.
Statistical Analysis
After data collection, we determined peak force values using Biodex software. Peak force is the maximal value on the force-angle-curve over 5 or 10 repetitions. Consistency of peak force across trials was acceptable because for both groups and on both sides, the coefficient of variance never exceeded 9.5 (SD = 4.7) for the tests at slow velocity and 11.2 (SD = 4.9) for the tests at high velocity. For this specific testing protocol, coefficients of variance up to 14.8 (SD = 8.6) provide reliable peak force data.17 The absolute data were normalized to body weight (N/kg). In addition, the agonist:antagonist muscle ratio was calculated by hand for both sides, with the protraction force as the agonist value and the retraction force as the antagonist value.
Means and standard deviations were calculated for the dependent variables, namely, isokinetic peak force for protraction and retraction, measured at 2 velocities (12.2 and 36.6 cm/s), and the protraction:retraction ratio, calculated for both test velocities.
Because all data were normally distributed with equal variances, we used parametric tests for statistical analysis. Differences in isokinetic peak force/body weight were analyzed with a general linear model analysis of variance in which the within-subjects factor was side (2 levels) and the between-subjects factor was group (2 levels). Multiple analyses of variance were performed for each dependent variable. We first tested interaction effects to determine any potential influence of group effects. Interaction effects of group and side were of interest. In the presence of an interaction, group differences and side differences were tested at each level of the interacting variable, using a Bonferroni procedure. In the absence of interactions, main effects of group and side were analyzed. All patients were injured on their dominant sides, so side comparisons were performed comparing the injured (dominant) shoulder of the patient group with the dominant shoulder of the control group and the uninjured (nondominant) shoulder of the patient group with the nondominant shoulder of the control group. All statistical analysis was performed with the Statistical Package for Social Sciences (version 11.0; SPSS Inc, Chicago, IL). Power was calculated at 85%. Computations regarding effect size were based on the results from our previous study on healthy subjects.17
RESULTS
The normalized values for the peak force/body weight (N/ kg) and agonist:antagonist ratios for both sides and both groups are presented in Table 2. Statistical analysis was performed on the normalized data. The general linear model 2-way analysis of variance with repeated-measures design revealed a significant group × side interaction effect for protraction at both velocities (P = .004 at slow velocity, P < .001 at high velocity) and retraction at high velocity (P = .01). Subsequently, we investigated the effects of groups for each side and the effects of side for each group. The percentage of side differences in each group and the P values of the Bonferroni tests for these side differences are also presented in Table 2. The percentages of group differences for each side with the P values of the post hoc tests are summarized in Table 3.
Table 2. Normalized Peak Force/Body Weight (N/kg) of Shoulder Girdle Protraction, Retraction, and Agonist/Antagonist Ratio as Mean (SD).

Table 3. Mean Group Differences for Peak Force/Body Weight (N/kg) and Protraction:Retraction Ratio.

Overhead athletes with impingement symptoms showed decreased force output/body weight at both velocities in the protractor muscles on the injured side compared with the uninjured side (−13.7% at slow velocity, −15.5% at high velocity; see Table 2) and compared with the control group, measured at high velocity (−20.7%; see Table 3). For retraction at slow velocity, no interaction effect of group × side (P = .12) or main side (P = .40) or group (P = .56) effects were noted. Post hoc tests were not performed for this variable.
Analysis of the protraction:retraction ratio at slow velocity revealed main side effects (P = .001) and group effects (P = .001) but no significant interaction of group × side (P = .74). This means that side differences are collapsed across groups and group differences are equally present on both sides. In both groups, significant side differences were seen in the protraction:retraction ratio (control group = −7.6%, patient group = −10.5%; see Table 2). On both sides, the patient group showed significantly lower protraction:retraction ratios compared with the control group (nondominant = −11%, dominant = −13.7%; see Table 3). At high velocity, statistical analysis of the ratios showed no interaction of group × side (P = .63) or main effects for side (P = .51) or group (P = .41). We did not perform post hoc tests for this variable.
DISCUSSION
Our purpose was to analyze isokinetic muscle performance variables of the scapular protraction and retraction muscles in athletes with and without chronic shoulder pain and to identify any deficits in overhead athletes with impingement symptoms compared with a healthy athletic population.
Our results revealed a significant decrease in force output in the scapular protractors in the injured shoulder of the patient group compared with the dominant side of a healthy control group when measured at slow velocity. These values suggest a lack of muscle strength in the serratus anterior muscle, the major scapular protractor. In addition to the group differences, side differences were found in the patient group in scapular protraction strength at both velocities, with a decrease in the injured shoulder compared with the uninjured side. In a previous study,9 statistically significant side differences were found in the protraction force at high but not low velocity between the injured and uninjured sides in a patient group of volleyball players with chronic impingement symptoms. However, in that study, the protractors were concluded to lack muscle power rather than absolute muscle strength. In addition, strength values were not compared with a healthy control group. Our present investigation revealed valuable additional information: not only side differences but also group differences were apparent, and decreased muscle strength was demonstrated not only at high but also at low velocity, indicating dysfunction in more than 1 variable of muscle performance.
The question arises whether the side differences found in our patient group are the result of muscle adaptation to overhead sport activity rather than an indication of muscle imbalance and related to shoulder injury. In the healthy athletes, protraction peak force/body weight was slightly higher on the dominant than the nondominant side at both velocities. However, side differences were not statistically significant. Wilk et al4 documented the isometric scapular muscle strength values of professional baseball players. Some side differences in scapular muscle strength in this population were noted in favor of the dominant side, but the lack of statistical analysis of these anecdotal data does not allow us to draw conclusions. In addition, whereas the athletes examined by Wilk et al4 were baseball players, our patients were active in tennis and volleyball, which makes comparisons between these groups somewhat inappropriate. In view of our control-group results, in which no significant side differences were present, the decreased protractor muscle strength in the patient group may be considered abnormal.
The significant decline in force output for the protractors at both velocities reflects a decrease in muscle performance of the serratus anterior muscle and/or the other scapular protractors. This muscle is generally accepted to be of tremendous importance in optimal shoulder function, especially in overhead motions, when demands on muscle function are extremely high in strength as well as in power.1,3 Diminished force in this muscle may result in a lack of powerful protraction during the throwing motion. A scapula that is unable to move in smooth coordination with the humerus during the acceleration phase may increase the stresses on the glenohumeral joint and, hence, jeopardize shoulder stability.1,18
Our patient group demonstrated lower strength ratios on both sides than the healthy control group. On the injured side, the value is smaller than 1. The uninjured athletes also showed significant side differences in the protraction:retraction ratios: significantly lower on the dominant side (1.09) than the nondominant side (1.18). It is generally believed that the agonist: antagonist muscle ratios are important values when considering how the scapula provides stability, mobility, and symptom-free function.4 Our data show that, in spite of a lack of difference in absolute muscle strength in the healthy group's protractors, the balance between agonists and antagonists differs between sides. Because in this study the protractors are suggested to be the agonists, higher ratios indicate higher strength values for the protractors in relation to the retractors. Our healthy athletes showed a protraction:retraction ratio of about 1 on the dominant side. Protractors and retractors seemed to be equal in strength. In a study of nonathletic healthy subjects, ratios were calculated to be 1.18 on the nondominant and 1.11 on the dominant sides.17 No significant side differences were apparent for absolute muscle strength data or for the calculated ratios. The ratio on the nondominant side in the athletic population is similar to the values found in a nonathletic population. This suggests that in subjects not active in overhead sports and in the nondominant shoulder in overhead athletes, protraction force is slightly greater than retraction force. The lower ratio on the dominant side of the overhead athletes and, subsequently, the assumption that protractors and retractors are equal in strength may be the expression of sport-specific adaptation of muscle performance in this population. These results are similar to previous observations demonstrating altered neuromuscular control mechanisms in competitive overhead athletes compared with normal subjects not participating in overhead sports and compared with the nonthrowing extremity.10,19,20 The strength ratios of the injured shoulder (smaller than 1) indicate that the protractors are weaker than the retractors. These results possibly reflect a muscular imbalance in the scapular muscles at the expense of protraction force. We noted no significant side or group differences at high velocity. An interesting finding in this study is that both the injured and the uninjured sides of the patient group displayed differences from the control group. Bilateral deficits in unilaterally injured patients are also demonstrated in the timing properties of the scapular muscles.10 It is unclear whether this muscle pattern is a primary phenomenon, which may predispose the athlete to injury, or secondary as a result of the pain. The causative relationship between shoulder injury and scapulothoracic dysfunction is unclear and remains a topic of controversy in the literature.7,18
Our results regarding retraction force at high velocity are somewhat confounding. Although a significant group × side interaction effect was found, post hoc tests did not reveal any significant side or group differences. In both groups, we observed some side differences in this variable, a decrease on the injured side within the patient group and a higher value on the dominant side in the control group. Although retraction force on the injured side was decreased compared with the uninjured side and with both sides of the healthy athletes, none of these differences reached statistical significance. Because the standard deviations of these variables were rather high, we believe that future research on a larger or a more homogeneous group of patients might confirm these tendencies.
A possible explanation for the differences between sides and between groups established in this investigation may be the presence of pain during the test. Pain-related inhibition of muscle activity is a well-known phenomenon. Muscle inhibition is described in the literature as a diminished ability to recruit all motor units to their full extent during a maximal voluntary contraction.21 It has been suggested that scapular dyskinesis may be a nonspecific response to shoulder dysfunction. These abnormal scapular movements possibly are the result of the inhibition or disorganization of activation patterns in the scapula-stabilizing muscles.22 In our investigation, patients were questioned regarding the occurrence of pain during the test. None reported experiencing pain during the procedure, possibly because of the relatively safe position of the shoulder in the scapular plane and because most of the athletes experienced pain only during their overhead sports. However, this factor was not confirmed by a written questionnaire, which should be acknowledged as a limitation to the study.
The question arises as to the clinical implications of our results. The main question in view of designing an appropriate rehabilitation program for overhead athletes is whether the deficiencies found in our investigation are reversible. In other words, is it possible to influence these imbalances by an adequate exercise program, and which exercises are the most appropriate?
In recently published rehabilitation protocols for shoulder pain in overhead athletes, much attention has been paid to the restoration of normal scapulothoracic function.3–5,7,23–25 Strengthening of the scapular muscles is often the major treatment goal. Our results regarding isokinetic protraction strength confirm previous hypotheses of decreased muscle force in patients with shoulder pain3,7 and, hence, provide additional arguments for protraction strengthening as a treatment goal in overhead athletes with shoulder pain.
Various authors24,26–30 have investigated electromyographic muscle activity of the scapular muscles during exercises commonly used in shoulder rehabilitation. Based on the results of these studies, several exercises are promoted to enhance the strength of the scapular muscles. From a biomechanical point of view, the push-up exercise shows the closest resemblance to the protraction movement investigated in our study. However, it must be noted that although protraction in our testing procedure was performed with the elbow extended in the scapular plane, the push-up exercise allows elbow movements and results in a movement of the scapula from a frontal-plane orientation when the elbow is flexed to a more sagittal-plane orientation at full arm extension. Based on our results, we feel that this exercise should be implemented into a shoulder-girdle rehabilitation program. However, it is often suggested that in patients with scapulothoracic muscle dysfunction, a lack of muscle activity in the serratus anterior is accompanied by hyperactivity in the upper trapezius,11,24,31 indicating imbalances of muscle activity rather than global weakness of the scapulothoracic muscles. In view of this possibility, patients should perform exercises that promote serratus anterior activity while suppressing upper trapezius activity. In a recent investigation, Ludewig et al24 examined the relative balance of serratus anterior and upper trapezius muscle activity during several push-up exercises. They concluded that the standard push-up is an optimal exercise to promote activity in the serratus anterior while keeping the upper trapezius:serratus anterior ratio low. A patient who is unable to perform this exercise may benefit from a progression of exercises, starting with the plus phase of wall push-ups, followed by elbow push-ups and knee push-ups. However, we did not investigate other exercises that are often promoted to enhance scapular muscle strength, such as elevation in the scapular plane.
The limitations of our study should be noted. Although the serratus anterior and the trapezius are considered to be the major protractor and retractor, respectively, we should take into account that other muscles also contribute to both movement directions, such as the pectoralis and the rhomboid muscles. However, individual muscle activity of the scapular muscles was not measured in this study. Therefore, even though the results were interpreted in relation to serratus anterior and trapezius muscle strength, extrapolation of our results to the strength of these muscles should be performed with caution.
For the purpose of this study, protraction-retraction movements were performed in the scapular plane, which is 30° anterior of the frontal plane, instead of in the frontal plane. Researchers32,33 have suggested that the isokinetic assessment of muscle performance in patients with shoulder pain should be performed in the scapular plane rather than in the frontal plane. This arm position reduces the stress placed on the anterior capsuloligamentous structures and prevents impingement of the rotator cuff under the acromion. It also provides better congruency between the articular surfaces of the glenohumeral joint and offers more comfort to the injured subject. However, performing the movement in this particular plane possibly limits the global range of motion of the scapula on the thoracic wall and influences performance of the scapular muscles. Future investigators should examine scapular muscle performance in other planes of movement, particularly the frontal plane.
The testing position, in which the patient is sitting with the arm elevated horizontally in the scapular plane, lacks some functional relevance in relation to overhead throwing because gravity is eliminated and force-dependent muscle activation patterns of the trunk are not facilitated. In addition, only concentric force values were obtained. However, eccentric force output is a relevant muscle performance variable, especially in the overhead throwing motion.7,34 Moreover, movement velocities performed in this isokinetic protocol do not approximate true movement speeds during overhead throwing and should be interpreted with caution. Future research should emphasize these functional muscle performance considerations.
CONCLUSIONS
Our aim was to compare the isokinetic force output of the scapular muscles between overhead athletes with chronic impingement symptoms and overhead athletes without shoulder pain. The injured athletes showed decreased muscle peak force/body weight in the protractors on the injured side compared with the uninjured side and with healthy athletes. In addition, the patients demonstrated decreased agonist:antagonist ratios on both sides, suggesting a muscular imbalance in the scapular force coupled with relative weakness of the protractors.
These findings support the hypothesis that shoulder impingement may be related to scapulothoracic muscle dysfunction and may have implications for the conservative treatment of impingement syndrome.
Acknowledgments
We thank Julie De Spiegelaere and Natalie Vermeire for their assistance in the collection of the data.
REFERENCES
- Arroyo JS, Hershon SJ, Bigliani LU. Special considerations in the athletic throwing shoulder. Orthop Clin North Am. 1997;28:69–78. doi: 10.1016/s0030-5898(05)70265-0. [DOI] [PubMed] [Google Scholar]
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology, part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404–420. doi: 10.1053/jars.2003.50128. [DOI] [PubMed] [Google Scholar]
- Pink MM, Tibone JE. The painful shoulder in the swimming athlete. Orthop Clin North Am. 2000;31:247–261. doi: 10.1016/s0030-5898(05)70145-0. [DOI] [PubMed] [Google Scholar]
- Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30:136–151. doi: 10.1177/03635465020300011201. [DOI] [PubMed] [Google Scholar]
- Kamkar A, Irrgang JJ, Whitney SL. Nonoperative management of secondary shoulder impingement syndrome. J Orthop Sports Phys Ther. 1993;17:212–224. doi: 10.2519/jospt.1993.17.5.212. [DOI] [PubMed] [Google Scholar]
- Burkhart SS, Morgan CD, Kibler WB. The disabled shoulder: spectrum of pathology, part III: the SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy. 2003;19:641–661. doi: 10.1016/s0749-8063(03)00389-x. [DOI] [PubMed] [Google Scholar]
- Kibler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998;26:325–337. doi: 10.1177/03635465980260022801. [DOI] [PubMed] [Google Scholar]
- Lephart SM, Pincivero DM, Giraldo JL, Fu FH. The role of proprioception in the management and rehabilitation of athletic injuries. Am J Sports Med. 1997;25:130–137. doi: 10.1177/036354659702500126. [DOI] [PubMed] [Google Scholar]
- Cools AM, Witvrouw EE, Declercq GA, Vanderstraeten GG, Cambier DC. Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during a protraction-retraction movement in overhead athletes with impingement symptoms. Br J Sports Med. 2004;38:64–68. doi: 10.1136/bjsm.2003.004952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment pattern: trapezius muscle latency in overhead athletes with and without impingement symptoms. Am J Sports Med. 2003;31:542–549. doi: 10.1177/03635465030310041101. [DOI] [PubMed] [Google Scholar]
- Lukasiewicz AC, McClure P, Michiner L, Pratt N, Sennet B. Comparison of 3-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. 1999;29:574–586. doi: 10.2519/jospt.1999.29.10.574. [DOI] [PubMed] [Google Scholar]
- Speer KP, Hannafin JA, Altchek DW, Warren RF. An evaluation of the shoulder relocation test. Am J Sports Med. 1994;22:177–183. doi: 10.1177/036354659402200205. [DOI] [PubMed] [Google Scholar]
- Tennent TD, Beach WR, Meyers JF. A review of the special tests associated with shoulder examination, part I: the rotator cuff tests. Am J Sports Med. 2003;31:154–160. doi: 10.1177/03635465030310011101. [DOI] [PubMed] [Google Scholar]
- Tennent TD, Beach WR, Meyers JF. A review of the special tests associated with shoulder examination, part II: laxity, instability, and superior labral anterior and posterior (SLAP) lesions. Am J Sports Med. 2003;31:301–307. doi: 10.1177/03635465030310022601. [DOI] [PubMed] [Google Scholar]
- Cavallo RJ, Speer KP. Shoulder instability and impingement in throwing athletes. Med Sci Sports Exerc. 1998;30:S18–S25. doi: 10.1097/00005768-199804001-00004. (suppl) [DOI] [PubMed] [Google Scholar]
- Sørensen AK, Jørgensen U. Secondary impingement in the shoulder: an improved terminology in impingement. Scand J Med Sci Sports. 2000;10:266–278. doi: 10.1034/j.1600-0838.2000.010005266.x. [DOI] [PubMed] [Google Scholar]
- Cools A, Witvrouw E, Danneels L, Vanderstraeten G, Cambier D. Test-retest reproducibility of concentric strength values for shoulder girdle protraction and retraction using the Biodex isokinetic dynamometer. Isokinet Exerc Sci. 2002;10:129–136. [Google Scholar]
- Augé WK, II, Morrison DS. Assessment of the infraspinatus spinal stretch reflex in the normal, athletic, and multidirectionally unstable shoulder. Am J Sports Med. 2000;28:206–213. doi: 10.1177/03635465000280021101. [DOI] [PubMed] [Google Scholar]
- Dover GC, Kaminski TW, Meister K, Powers ME, Horodyski M. Assessment of shoulder proprioception in the female softball athlete. Am J Sports Med. 2003;31:431–437. doi: 10.1177/03635465030310031801. [DOI] [PubMed] [Google Scholar]
- Scovazzo ML, Browne A, Pink M, Jobe FW, Kerrigan J. The painful shoulder during freestyle swimming: an electromyographic and cinematographic analysis of twelve muscles. Am J Sports Med. 1991;19:577–582. doi: 10.1177/036354659101900604. [DOI] [PubMed] [Google Scholar]
- Hopkins JT, Ingersoll CD. Arthrogenic muscle inhibition: a limiting factor in joint rehabilitation. J Sport Rehabil. 2000;9:135–159. [Google Scholar]
- Kibler WB, McMullen J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg. 2003;11:142–151. doi: 10.5435/00124635-200303000-00008. [DOI] [PubMed] [Google Scholar]
- Akuthota V, Chou LH, Drake DF, Nadler SF, Toledo SD. Sports and performing arts medicine, 2: shoulder and elbow overuse injuries in sports. Arch Phys Med Rehabil. 2004;85:S52–S58. doi: 10.1053/j.apmr.2003.11.010. (3 suppl 1) [DOI] [PubMed] [Google Scholar]
- Ludewig PM, Hoff MS, Osowski EE, Meschke SA, Rundquist PJ. Relative balance of serratus anterior and upper trapezius muscle activity during push-up exercises. Am J Sports Med. 2004;32:484–493. doi: 10.1177/0363546503258911. [DOI] [PubMed] [Google Scholar]
- Morrison DS, Greenbaum BS, Einhorn A. Shoulder impingement. Orthop Clin North Am. 2000;31:285–293. doi: 10.1016/s0030-5898(05)70148-6. [DOI] [PubMed] [Google Scholar]
- Ballantyne BT, O'Hare SJ, Paschall JL. Electromyographic activity of selected shoulder muscles in commonly used therapeutic exercises. Phys Ther. 1993;73:668–677. doi: 10.1093/ptj/73.10.668. et al. [DOI] [PubMed] [Google Scholar]
- Decker MJ, Hintermeister RA, Faber KJ, Hawkins RJ. Serratus anterior muscle activity during selected rehabilitation exercises. Am J Sports Med. 1999;27:784–791. doi: 10.1177/03635465990270061601. [DOI] [PubMed] [Google Scholar]
- Hintermeister RA, Lange GW, Schultheis JM, Bey MJ, Hawkins RJ. Electromyographic activity and applied load during shoulder rehabilitation exercises using elastic resistance. Am J Sports Med. 1998;26:210–220. doi: 10.1177/03635465980260021001. [DOI] [PubMed] [Google Scholar]
- Lear LJ, Gross MT. An electromyographical study of the scapular stabilizing synergists during a push-up progression. J Orthop Sports Phys Ther. 1998;28:146–157. doi: 10.2519/jospt.1998.28.3.146. [DOI] [PubMed] [Google Scholar]
- Moseley JB, Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992;20:128–134. doi: 10.1177/036354659202000206. [DOI] [PubMed] [Google Scholar]
- Sahrman S. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis, MO: Mosby; 2002:193–261.
- Durall C, Davies G, Kernozak T, Gibson M, Fater D, Straker J. The reproducibility of assessing arm elevation in the scapular plane on the Cybex 340. Isokinet Exerc Sci. 2000;8:7–11. [Google Scholar]
- Mayer F, Horstmann T, Bäurle W, Grau S, Handel M, Dickhuth H. Diagnostics with isokinetic devices in shoulder measurements: potentials and limits. Isokinet Exerc Sci. 2001;9:19–25. [Google Scholar]
- Noffal GJ. Isokinetic eccentric-to-concentric strength ratios of the shoulder rotator muscles in throwers and nonthrowers. Am J Sports Med. 2003;31:537–541. doi: 10.1177/03635465030310041001. [DOI] [PubMed] [Google Scholar]