

Abstract
Background
The Depression Anxiety Stress Scale-21 Items (DASS-21) is commonly used to assess the mental health of students, but there is a need for further clarification regarding its equivalence, structure, and core items.
Methods
We conducted a confirmatory factor analysis (CFA) on a sample of 7943 Chinese students to examine the performance of the DASS-21 and assess measurement invariance. Additionally, we utilized network analysis to investigate the structure and centrality of students’ mental health.
Results
Our findings revealed a stable three-factor structure for the DASS-21, characterized by high correlations among depression, anxiety, and stress. The DASS-21 demonstrated strict invariance across genders and weak invariance across levels of education. Network analysis indicated that symptoms of depression, anxiety, and stress form clusters, with some symptoms exhibiting strong correlations with each other.
Conclusion
Our study highlights a substantial interrelation among depression, anxiety, and stress, revealing a structurally clustered pattern. Network analysis underscores the interconnectedness and centrality of these symptoms, recommending a shorter version of the DASS, and emphasizing the imperative for targeted interventions aimed at improving the psychological well-being of students.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12889-024-20123-6.
Keywords: Students, Depression, Anxiety, Stress, Factor analysis, Network analysis
Introduction
Depression, anxiety, and stress are the most common emotional problems and psychological disorders across the world [1], and they have become increasingly prominent in recent years [2, 3]. Depression refers to an emotional state of helplessness and powerlessness of the self, accompanied by a variety of physiological symptoms, such as weakness and sleep disturbance [4, 5]; anxiety is a future-oriented emotional state featured by stress and worries, which may also be accompanied by physiological responses [6]; stress refers to the psychological and physiological maladjustment that occurs when the demands of the external environment exceed the limits of an individual’s natural regulation, especially in unpredictable and uncontrollable situations [7]. Mental health problems represented by depression, anxiety and stress have received increasing attention from researchers in a variety of fields, including psychology [8], education [9], and economics [10].
From the perspective of education and development, students, as a physiologically or socially “immature group”, face particularly severe problems of depression, anxiety and stress [9]. A meta-analysis found that the overall prevalence of anxiety and depressive symptoms among Chinese students was 24.0% and 22.0%, respectively [11]. Stress is related to a variety of factors, the most common one being academic pressure. Prior studies have shown that Chinese students are exposed to high levels of stress over a long period of time because education in China tends to focus mainly on examinations or tests [12]. Academic pressure has been identified as an important factor contributing to health-related problems such as depression and anxiety among Chinese adolescents [13, 14]. Financial pressure has also been reported to be associated with mental health issues [15]. The impacts of stress, depression and anxiety on students include declined academic performance, sleep disturbances and even self-harming behaviors. For example, through a systematic review and meta-analysis on psychological correlates of college students’ academic performance, Richardson et al. found that academic stress was significantly and negatively correlated with the students’ academic performance (reflected by their grade point average [GPA]) [16]. Prior studies have found that the more stressed students are, the more likely they are to have sleep disorders [17]. One of our previous studies also found that depressive and anxiety symptoms had a mediating effect on the association of school bullying and academic stress with self-harm behaviors [18]. Although the above studies have found correlations between depression, anxiety and stress among students, they utilized different sample sources and research methodologies, resulting in a lower level of robustness in their evidence.
In clinical studies, depression, anxiety and stress are highly likely to co-exist in an individual [19, 20], and studies have also found that the three conditions are highly correlated [21]. The Depression, Anxiety and Stress Scale − 21 Items (DASS-21), consisting of three subscales (i.e., depression, anxiety, and stress subscales), is a validated measurement tool widely used in studies [22]. The scale also possesses a priori theoretical concepts; therefore, it is necessary to examine its applicability and psychometric properties in diverse populations. For instance, to assess whether measurement invariance exists when applied in groups of different genders and educational levels.
This study aims to select a representative sample of Chinese students to assess the suitability and effectiveness of DASS-21 in different groups. To analyze the underlying factor structure of DASS-21, we will utilize confirmatory factor analysis from a latent variable modeling perspective. Additionally, we will employ network analysis methods to investigate the connections between different symptom nodes. By using network analysis, we can examine the relationships and key symptoms associated with psychological disorders without relying on strong prior assumptions. This approach will enable us to gain a comprehensive understanding of the connections between depression, anxiety, and stress from various perspectives. By identifying the core symptoms of depression, anxiety, and stress in the student population, this study will provide valuable evidence and resources for mental health education in schools, clinical diagnosis and counseling, and medication recommendations.
Methods
Participants and procedure
In this study, participants were Chinese students recruited online or through offline convenience sampling from March to September 2022, and they were from a large number of cities including Beijing, Shanghai, Guangzhou, Shenzhen, Shenyang, Huludao, Jinan, Wuhu, Shijiazhuang, Changzhou, Suzhou, Fuzhou, Linyi, Chengdu, Urumqi, Qiqihaer, Kunming, and Wuhan (in descending order regarding the number of participants). We have directly provided the number of participants for each city along with their corresponding demographic data and have included this information in Supplementary Table 1. The students were either recruited online through the Questionnaire Star platform (https://www.wjx.cn/) or offline from different classes, grades, and school. Written informed consent was obtained from all the participants at the beginning of the survey, and the participants could withdraw from the survey at any time without penalty. The survey was completely anonymous with no personal identifying information required. Ethical approval for this study was obtained from the ethics committee of The Second Xiangya Hospital, Central South University.
Tools and assessments
The depression anxiety stress scale-21 items (DASS-21)
The DASS-21 is a three-factor model developed by Lovibond et al. [23] to examine common mood disorders such as depression, anxiety, and stress, and to provide auxiliary psychometric indicators for clinical diagnosis. In this study, we used the Chinese version of DASS-21 [24] to examine depression, anxiety and stress of the participants, with seven items for each condition. For instance, the subscale for depression included “I felt sad and depressed”, the subscale for anxiety included “I was aware of dryness of my mouth”, and the subscale for stress included “I found myself getting upset rather easily”. For all the subscales, higher scores indicated higher levels of depression, anxiety and stress. The scale is culturally appropriate, has been widely used in China, has shown high reliability and validity [24], and is suitable for use among primary school [25], secondary school [26], and university students [27]. In this study, the McDonald’s ω coefficients for the three factors, i.e., depression, anxiety and stress, were 0.89, 0.87 and 0.86, respectively.
Demographic variables
The demographic variables used in this study included level of education (upper primary, secondary, undergraduate, and postgraduate students), gender (male and female), and age (continuous variable). The demographic variables considered in this study encompassed educational attainment (ranging from upper primary to postgraduate levels), gender (male and female), and age.
Statistical analysis
Due to the configuration of the online platform, we required participants to complete all questions before submitting the questionnaire, ensuring the completeness of the data from the online sample. Additionally, we used an attention-check question, i.e., “Please choose strongly agree,” and data from participants who selected other options were removed. For offline participants, data were directly entered by the class teachers using an Excel template provided by the researchers, and any missing data were supplemented within a week through re-interviews with the students.We acknowledge the differences in data collection methods between the online and offline samples and have therefore implemented different quality control measures. For the online sample, lacking the contextual oversight of an in-person administrator, we employed attention-check questions and lie detectors to enhance data quality control. In the offline sample, since the data collection was supervised by class teachers who were familiar with and held authority over the students, the process was conducted under serious conditions with the principal investigator’s guidance. The subsequent data entry process included manual verification of handwriting and response patterns, making the attention-check question unnecessary in the offline sample. Therefore, these questions were omitted from the offline data collection. SPSS 21.0 was used to organize the data, and participants with missing values were excluded. JASP 16.0 was used for descriptive statistics, ANOVA, correlation analysis, validation factor analysis, measurement invariance and network analysis based on EBICglasso [28, 29].
It should be noted that in the multi-group validation factor analysis, in order to simplify the model and to avoid the effect of an unbalanced sample size on the model fit, we modified the grouping of education level by combining middle school and high school students to form a group of secondary school students and combining college, undergraduate, and graduate students to form a group of university students. Additionally, in the measurement invariance analysis, according to the criteria of the invariance test indicated by Chen et al. [30], although the sample size of this study was more than sufficient, the number of participants was not balanced between groups, which led to the use of a more lenient criteria (ΔCFI ≤ 0.01; ΔRMSEA ≤ 0.01; ΔSRMR ≤ 0.025). When multiple criteria conflicted, the amount of change in CFI was used as the primary criterion. The network analysis functionality integrated in JASP is based on the R language, with R packages used in this study including bootnet, glasso, huge, and mgm. In the depression-anxiety-stress network, different centrality metrics can be used to explain different symptoms. Closeness centrality measures the average distance from a node to other nodes, indicating the speed and efficiency of symptom propagation for that node. Strength centrality measures the strength of connections between a node and other nodes, indicating the importance and influence of the node in symptom transmission. Betweenness centrality measures the ability of a node to act as a mediator in the network, quantifying the extent to which a node serves as a bridge in symptom transmission. Expected influence measures the influence of a node on other nodes, specifically the degree to which a node affects other nodes in symptom transmission. This study primarily focuses on exploring the comprehensive impact of symptoms. Therefore, the centrality of strength has been selected to illustrate the significance of a single symptom in the network. To prevent potential non-invariance between networks, we utilized the Network Comparison Test (NCT) package in R to conduct network comparison tests for the subgroups (primary school, middle school, and college groups).
Results
Descriptive statistics and analysis of variance
A total of 7934 students were enrolled in this study. They were aged 10–57 years, with a mean age of 19.08 ± 6.76 years. Among them, 4133 were male and 3801 were female. There were 1520 primary school students, 2282 secondary school students, 4132 university students.
The mean scores and ANOVA results of different groups of participants on each scale are shown in Table 1. The post hoc test based on the LSD method showed that: (1) in terms of gender, males had significantly higher levels of depression, anxiety, and stress than females; (2) with regard to the level of education, university students had the highest levels of depression, anxiety, and stress; secondary and primary school students had relatively lower levels of depression, anxiety and stress.
Table 1.
Descriptive statistics and ANOVA for depression, anxiety and stress (N = 7934)
| Male | Female | F | Cohen’s f | Primary | Secondary | University | F | Cohen’s f | |
|---|---|---|---|---|---|---|---|---|---|
| Depression | 0.77 ± 0.71 | 0.66 ± 0.66 | 50.83*** | 0.08 | 0.46 ± 0.58 | 0.64 ± 0.63 | 0.87 ± 0.72 | 152.04*** | 0.24 |
| Anxiety | 0.87 ± 0.71 | 0.73 ± 0.64 | 85.59*** | 0.10 | 0.65 ± 0.57 | 0.76 ± 0.59 | 0.90 ± 0.75 | 53.06*** | 0.14 |
| Stress | 0.91 ± 0.68 | 0.83 ± 0.65 | 30.68*** | 0.06 | 0.76 ± 0.59 | 0.88 ± 0.61 | 0.91 ± 0.72 | 18.83*** | 0.08 |
Note: Scores of depression, anxiety, and stress are the mean scores of the items; *** p < 0.001. Cohen’s f-value indicates the effect size, and the thresholds for differentiation of small, medium, and large effect sizes are 0.1, 0.25, and 0.40, respectively
Correlation analysis
Depression, anxiety and stress were significantly and positively correlated. Among them, anxiety was positively correlated with depression (r = 0.78, p < 0.001), and stress was positively correlated with both depression (r = 0.76, p < 0.001) and anxiety (r = 0.80, p < 0.001).
Multi-group validation factor analysis
A validation factor analysis was conducted to confirm the structural validity and fit metrics of the DASS-21 (see Table 2). Factor loadings for individual items were also reported for comparison with the indicators in the network analysis. The results indicated that DASS-21 met the psychometric criteria for all students overall and all groups of students. The unconstrained validation factor analysis suggests that the fit indexes of both male and female groups are acceptable. Meanwhile, the fitted indexes for the groups of primary school students, secondary school students and university students are all acceptable. This was also a prerequisite step for the measurement invariance test.
Table 2.
Indicators and criteria for each DASS-21 fit
| Fit indicator | CFI | TLI | NFI | IFI | GFI | RMSEA | SRMR |
|---|---|---|---|---|---|---|---|
| Total | 0.934 | 0.925 | 0.932 | 0.934 | 0.915 | 0.065 | 0.038 |
| Male | 0.935 | 0.926 | 0.932 | 0.935 | 0.933 | 0.066 | 0.036 |
| Female | 0.928 | 0.918 | 0.924 | 0.928 | 0.913 | 0.066 | 0.039 |
| Primary School Students | 0.927 | 0.917 | 0.916 | 0.927 | 0.941 | 0.063 | 0.035 |
| Secondary School Students | 0.919 | 0.908 | 0.912 | 0.919 | 0.939 | 0.067 | 0.039 |
| University Students | 0.926 | 0.917 | 0.923 | 0.926 | 0.877 | 0.075 | 0.045 |
| Standard | >0.90 | >0.90 | >0.90 | >0.90 | >0.90 | <0.08 | <0.05 |
Abbreviations: CFI = Comparative goodness-of-fit index, TLI = Tucker-Lewis index, NFI = Normative fit index, IFI = Value-added fit index, GFI = Goodness-of-fit index, RMSEA = Root mean square error of approximation, SRMR = Standardized root mean square error
Measurement invariance
We analyzed the measurement invariance of gender and education level (see Table 3). As shown by each model fit indicator, DASS-21 satisfied the metric invariance test (ΔCFI = 0.002), the scalar invariance test (ΔCFI < 0.001), and the strict invariance test (ΔCFI = 0.002) between the male and female groups. Meanwhile, DASS-21 was only able to satisfy the metric invariance test (ΔCFI = 0.010) between the primary, secondary and university student groups. This result indicates that the DASS-21 satisfies weak invariance between levels of education.
Table 3.
Measurement invariance of gender and level of education (N = 7934)
| χ²(df) | CFI | RMSEA | SRMR | ΔCFI | ΔRMSEA | ΔSRMR | Decision | ||
|---|---|---|---|---|---|---|---|---|---|
| Gender | Configural invariance |
6487.556 (372) |
0.931 | 0.066 | 0.039 | ||||
| Metric invariance |
6599.126 (390) |
0.929 | 0.065 | 0.043 | 0.002 | 0.001 | -0.004 | Accepted | |
| Scalar invariance |
6698.416 (408) |
0.929 | 0.064 | 0.042 | < 0.001 | 0.001 | 0.001 | Accepted | |
| Strict invariance |
6823.257 (429) |
0.927 | 0.063 | 0.042 | 0.002 | 0.001 | < 0.001 | Accepted | |
| Level of education | Configural invariance |
7822.668 (668) |
0.924 | 0.070 | 0.042 | ||||
| Metric invariance |
8825.433 (594) |
0.914 | 0.072 | 0.061 | 0.010 | -0.002 | 0.019 | Accepted | |
| Scalar invariance |
11645.511 (630) |
0.885 | 0.081 | 0.077 | 0.029 | -0.009 | -0.016 | Rejected | |
| Strict invariance |
13526.844 (915) |
0.867 | 0.085 | 0.082 | 0.018 | -0.004 | -0.005 | Rejected |
Abbreviations: CFI = Comparative goodness-of-fit index, RMSEA = Root mean square error of approximation, SRMR = Standardized root mean square error. Configural Invariance: Confirms that the factor structure is the same across groups, with consistent factor loadings, without involving cross-group comparisons of parameters.Metric Invariance: Builds on configural invariance by requiring that factor loadings are equivalent across groups, assessing the cross-group measurement equivalence of the tool.Scalar Invariance: Adds the requirement of equal intercepts to metric invariance, indicating that both factor loadings and intercepts are the same across groups.Strict Invariance: Extends scalar invariance by also demanding that error variances or residuals are equal across groups, representing the most rigorous test for complete measurement equivalence
Network analysis
We used all the items of DASS-21 as nodes. The number of non-zero edges in the network was 171/210 with a sparsity of 0.19. The items for depression, anxiety and stress were relatively concentrated in clusters, and items self-depreciation and meaninglessness (0.36), breathing difficulty and trembling (0.25), scare and uneasy (0.24), and arrhythmia and fear (0.21) had the greatest strength of association (see Fig. 1).
Fig. 1.
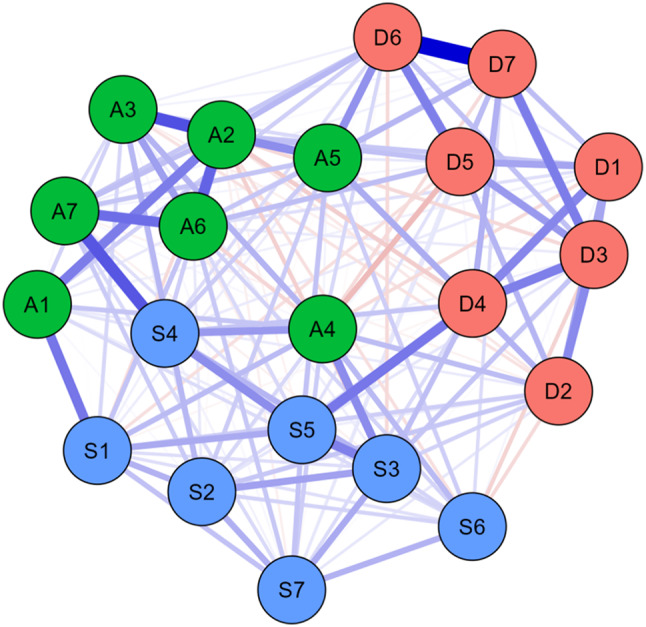
Network estimates of depression, anxiety and stress symptoms. Notes: D represents depression items, A represents anxiety items, and S represents stress items. Blue lines represent positive correlations and red lines represent negative correlations, with thicker lines indicating stronger correlations. The value in the middle of the line represents the strength of the correlation between two nodes
We also reported the centrality of individual nodes, which measures the influence of a node within in a network. Changes in nodes with higher centrality could affect, to a greater extent, the nodes that connected to them. The results showed that breathing difficulty and nervous had higher betweenness centrality and closeness centrality, while breathing difficulty had higher degree centrality (see Fig. 2).
Fig. 2.

Centrality graph of the network. Notes: Betweenness implies how often a node is on the shortest path between any two other nodes; closeness is the inverse of the sum of the shortest path distances from all other nodes in the network to a particular node; degree represents the number of other nodes that are directly connected to a particular node. Expected influence refers to the influence of one node on other nodes compared to the previous centrality metrics, with the edge weight directionality taken into account
To further examine the differences and associations between the latent variable model and the theoretical perspective of the psychopathological network, we compared the factor loadings and expected impacts of the scale items (see Table 4). In this study, panic, arrhythmia, self-depreciation, meaninglessness, uneasiness, and nervousness had high expected impact. Factors of stress and anxiety were found to share core symptoms. Panic and arrhythmia had high explanatory power and importance in the anxiety factor, while uneasiness and nervousness played a more central role in the stress factor. In the depression factor, the two analytical methods found inconsistent key symptoms, with hopelessness and enthusiasm having higher factor loadings in the traditional latent variable model. Self-depreciation and meaninglessness showed higher expected impacts in the network analysis. Based on this, we recommend using self-depreciation, meaninglessness, panic, arrhythmia, blue, and nervousness as a shortened version of the DASS-6. Confirmatory factor analysis results indicated that the fit indices for the DASS-6 meet psychometric standards: GFI = 0.998; RMSEA = 0.034; CFI = 0.998; NFI = 0.924; NNFI = 0.994; TLI = 0.994; IFI = 0.998. The McDonald’s ω coefficients for the three factors of depression, anxiety, and stress were 0.816, 0.769, and 0.750, respectively, with a total McDonald’s ω of 0.905.
Table 4.
Factor loadings and expected impact of symptoms (N = 7934)
| Code | Symptom | Factor loading | Expected impact |
|---|---|---|---|
| D1 | No positive | 0.66 | -0.55 |
| D2 | Initiation | 0.57 | -1.21 |
| D3 | Hopelessness | 0.70 | 0.09 |
| D4 | Blue | 0.65 | 0.82 |
| D5 | Enthusiasm | 0.67 | -0.38 |
| D6 | Self-depreciation | 0.65 | 1.15 |
| D7 | Meaninglessness | 0.65 | 0.92 |
| A1 | Dry mouth | 0.58 | -0.76 |
| A2 | Breathing difficulty | 0.68 | -0.38 |
| A3 | Trembling | 0.61 | -0.16 |
| A4 | Social anxiety | 0.54 | -1.08 |
| A5 | Panic | 0.69 | 1.60 |
| A6 | Arrhythmia | 0.71 | 1.34 |
| A7 | Scare | 0.67 | 0.03 |
| S1 | Restlessness | 0.56 | -0.55 |
| S2 | Allergy | 0.64 | 0.26 |
| S3 | Consumption | 0.64 | 0.17 |
| S4 | Uneasiness | 0.70 | 1.01 |
| S5 | Nervousness | 0.69 | 0.62 |
| S6 | Low patience | 0.45 | -2.67 |
| S7 | Irritability | 0.64 | -0.29 |
Note: Bold numbers indicate that the item has a high Factor loading or Expected impact in that factor
Subgroup network analysis
The density ratios for the primary school group, middle school group, and university group were 159/210, 154/210, and 171/210, respectively. To better understand the core symptoms and structure of symptom networks among different age groups of students, we divided the student population into three groups for analysis (Fig. 3). In the network of primary school students, the highest edge weights were observed between self-depreciation and meaninglessness (0.31), arrhythmia and scare (0.26), and nervousness and blue (0.24). In the network of middle school students, the highest edge weights were observed between self-depreciation and meaninglessness (0.39), dry mouth and restlessness (0.27), no positive and blue (0.25), and hopelessness and meaninglessness (0.25). Although self-depreciation and meaninglessness still maintained a high level of connectivity, there were shifts and changes in the other major edge weights, especially with close associations among other depressive symptoms. Additionally, a negative correlation was observed between arrhythmia and social anxiety, indicating an inverse relationship between social anxiety and arrhythmia. In the network of university students, the highest edge weight remained between self-depreciation and meaninglessness (0.36). There were further changes in the other major edge weights, such as breathing difficulty and trembling (0.28), hopelessness and blue (0.28), and scare and uneasiness (0.27). Furthermore, there were some symptoms that showed negative associations, such as consumption and breathing difficulty (-0.13) and blue and breathing difficulty (-0.11).
Fig. 3.

Edge structure of mental health network of students at different educational levels. Note: (1) (2) (3) respectively represent the primary school group, the middle school group and the university group
Afterwards, we utilized the NCT R package to conduct pairwise comparisons and found that there was no significant difference in overall strength between the primary and middle school groups (9.29 vs. 9.65, p = 0.07), nor in edge weights (p > 0.05). However, there was a significant difference in overall strength between the primary and college groups (9.29 vs. 11.04, p < 0.01), and in edge weights (p < 0.01). At the same time, there was a significant difference in overall strength between the middle and college groups (9.65 vs. 11.04, p < 0.01), and in edge weights (p < 0.01).
In the centrality section (Fig. 4), based on considerations of statistical procedures, we decided to use strength centrality to explain the dynamics and differences in core symptoms of psychological health among students in different grade levels. The red line represented primary school students, the green line represented secondary school students, and the blue line represented university students and above.
Fig. 4.

Mental health network centrality map of students at different educational stages
Among primary school students, the three nodes with the highest centrality were meaninglessness (1.527), blue (1.312), and arrhythmia (1.128). For middle school students, it was social anxiety (1.717), meaninglessness (1.597), and arrhythmia (1.524). And for university students, it was breathing difficulty (3.337), self-depreciation (1.163), and consumption (0.954). In primary school students, the primary symptoms observed were depression. In middle school students, the symptoms were predominantly anxiety. However, in university students, the symptoms exhibited greater complexity.
In terms of changes across grade levels, as age increased, the importance of low patience gradually rose, approaching a central position within the symptom network. In contrast, the importance of blue declined year by year.
Discussion
This study explored the internal associations and structure of depression, anxiety and stress among Chinese students based on the latent variable model and psychopathological network theory [31]. Greater depression, anxiety, and stress have been found among males than females, and prior studies [32] also suggested that this might be because Chinese males tended to take on more social responsibility and project a strong image, and this cultural pressure may affect the mental health of Chinese males. Chinese males also have a lower level of collateral social support, which may lead to their difficulty in relieving stress through the social system. The mental health of students is also getting worse with increased level of education. This may be due to the gradual increase in academic pressure, the increasing social responsibilities, and increased self-awareness and awareness of emotions [11]. Prior studies also found that depression, anxiety and stress are highly likely to co-exist [19, 20] and the importance of different symptoms or symptom clusters varies [33]. The correlation and network analyses in the present study showed that depression, anxiety and stress were positively and strongly correlated not only at the variable level but also at the symptom level.
The confirmatory factor analysis indicated excellent fit of the three-factor structure for depression, anxiety and stress, which has been supported by existing studies [24]. The multi-group confirmatory factor analysis found measurement invariance of the DASS-21, which was in line with prior studies [34, 35], and the DASS-21 met strict equivalence in gender. However, the DASS-21 only satisfies weak equivalence in the level of education, which might be due to the fact that the studied population covered primary, secondary, and tertiary school students, and that there were differences in the understanding of scale items between the groups [34]. Therefore, it is not recommended to use the same set of scales on the whole student population. Subsequent research can focus on the revise of a version specifically for primary school students, which should be more relevant to their daily life.
The network analyses indicated that self-depreciation was most strongly associated with meaninglessness in the network of depressive symptoms. Studies based on a phenomenological hermeneutic approach suggest that the association of these two symptoms may be related to an imbalance between the real and ideal selves [36]. Within the anxiety symptom network, breathing difficulty and trembling had the strongest association, followed by arrhythmia and scare. The above four symptoms tend to co-occur in one individual, as neurotransmitters such as norepinephrine, a key factor for anxiety, may simultaneously affect the heart rate, respiration and sympathetic nervous system [37]. We also found a strong association between scare and uneasiness, which has been reported in prior clinical studies [38]. Although it was assumed that they belonged to different factors in the latent variable model, the network analysis showed a stronger association. With regard to centrality, breathing difficulty, nervousness, panic, arrhythmia, self-depreciation, meaninglessness, and uneasiness played a more important role in their symptom clusters. Therefore, we believe that these core symptoms can constitute the items of a shorter version of the DASS, which is further supported by psychometric testing. We are confident that the DASS-6 can serve as a quicker and more convenient screening tool within the Chinese student population. The advantage of network analyses is that more information can be obtained from cross-sectional data than from latent variable models. A better understanding of the interplay between all the symptoms and the identification of key symptom nodes in the network structure [39, 40], may help us find ways to improve the mental health of students.
In our study, we used the NetworkComparisonTest to analyze the characteristics of depression, anxiety, and stress symptom networks among students at different educational stages (elementary, middle, and college) [41]. The results showed that while there were no significant differences in the overall intensity and edge weights of symptoms between elementary and middle school students, both groups exhibited significantly lower levels compared to college students. This may reflect the increasing academic pressures and social responsibilities that come with age, thereby leading to higher levels of mental health symptoms [42]. These findings provide an important perspective for understanding changes in the mental health status of students across different educational stages, and also highlight potential psychological health issues that may need attention during the educational process.
Recently, several studies among Chinese populations have validated the DASS-21 scale [43–45]. This study confirms previous research and, with a representative large sample of student data, revealed a stable three-factor structure for the DASS-21, characterized by high correlations among depression, anxiety, and stress. Our research observed differences and variations in core symptoms between different age groups, which helps to better understand the mental health status of students at various age levels. At the same time, we also proposed a brief version of the DASS-6 and assessed its reliability and validity, providing a potentially more efficient tool for mental health assessment, which has not been explored in existing literature.
Integrating the perspectives of latent variable theory and psychopathological network theory, we found that panic and arrhythmia, and uneasy and nervous had superior performances in terms of factor loadings and expected impacts in anxiety and stress networks, suggesting that there is consistency across theoretical perspectives for key symptoms of anxiety and stress. However, in the depression network, there was inconsistency between factor loadings and expected impacts, which might be due to the fact that depressive symptoms are more biased towards internal mechanisms compared to anxiety and stress, with greater discrepancy between outward symptoms and underlying constructs [46]. Intervention for depression, anxiety and stress, such as counselling or medications, may be more effective with the identification of the right targets. At present, the development and selection of medications for depression and anxiety has still been challenging due to unclear pathogenesis of the mental illnesses [47]. Through network analyses, the relationships between individual symptoms can be organized to find the key symptoms in the network [39, 48], which may provide a reference for subsequent empirical interventions and pharmacotherapy.
Our findings should be interpreted in light of certain strengths and limitations. The strengths of the study include the use of consistent measurement tools and the availability of a large sample size of representative data for analysis. Limitations of the study include two aspects. Firstly, network models have drawbacks, such as model overfitting or excessive complexity [49]. Secondly, the present study used cross-sectional data, and despite the introduction of a penalty factor in the network model, the associations we obtained remained correlational rather than causal. Thus, we emphasized the relative importance of a symptom for mental disorders, but such an assumption might be less likely due to “missing in the hypothesis”. Considering the differences in depression, anxiety, and stress between groups of different genders and ages, subsequent studies can focus on the differences in the DASS-21 network using different grouping methods, identification of symptom nodes that are more suitable for interventions based on the differences in the centrality of nodes, and development of intervention strategies that are more relevant to the characteristics of the studied population [50].
Conclusion
Factor and network analyses showed that depression, anxiety and stress were closely related among Chinese students. DASS-21 has varying degrees of measurement invariance across genders and grades. The DASS-6 has a satisfactory reliability and validity. There are also differences and changes in core symptoms among different age groups, which provide reference for subsequent intervention.
List of Abbreviations
| Code | Symptom | Question |
|---|---|---|
| D1 | No positive | I couldn’t seem to experience any positive feeling at all. |
| D2 | Initiation | I found it difficult to work up the initiative to do things. |
| D3 | Hopelessness | I felt that I had nothing to look forward to. |
| D4 | Blue | I felt down-hearted and blue. |
| D5 | Enthusiasm | I was unable to become enthusiastic about anything. |
| D6 | Self-depreciation | I felt I wasn’t worth much as a person. |
| D7 | Meaninglessness | I felt that life was meaningless. |
| A1 | Dry mouth | I experienced dryness of my mouth. |
| A2 | Breathing difficulty | I experienced breathing difficulty (e.g., excessively rapid breathing). |
| A3 | Trembling | I experienced trembling (e.g., in the hands). |
| A4 | Social anxiety | I was worried about situations in which I might panic and make a fool of myself. |
| A5 | Panic | I felt I was close to panic. |
| A6 | Arrhythmia | I was aware of the action of my heart in the absence of physical exertion (e.g., sense of heart rate increase, heart missing a beat). |
| A7 | Scare | I felt scared without any good reason. |
| S1 | Restlessness | I found it hard to wind down. |
| S2 | Allergy | I tended to over-react to situations. |
| S3 | Consumption | I felt that I was using a lot of nervous energy. |
| S4 | Uneasiness | I found myself getting agitated. |
| S5 | Nervousness | I found it difficult to relax. |
| S6 | Low patience | I was intolerant of anything that kept me from getting on with what I was doing. |
| S7 | Irritability | I felt that I was rather touchy. |
Abbreviations
| Abbreviations | Full Name |
|---|---|
| DASS-21 | Depression Anxiety Stress Scale − 21 Items |
| CFA | Confirmatory Factor Analysis |
| NCT | Network Comparison Test |
| CFI | Comparative Goodness-of-Fit Index |
| TLI | Tucker-Lewis Index |
| NFI | Normative Fit Index |
| IFI | Incremental Fit Index |
| GFI | Goodness-of-Fit Index |
| RMSEA | Root Mean Square Error of Approximation |
| SRMR | Standardized Root Mean Square Error |
| GPA | Grade Point Average |
| ω | McDonald’s Omega |
| LSD | Least Significant Difference |
| NNFI | Non-Normed Fit Index |
| EBIC | Extended Bayesian Information Criterion |
| glasso | Graphical Lasso |
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgements
We sincerely thank the participating schools and students for their support, and we are also grateful to the anonymous reviewers for their valuable feedback, which has greatly enhanced this study.
Author contributions
Zheng Zhang and Ruoheng Lin designed the study and wrote the first draft of manuscript. Huifeng Wu and Shuo Wu collected and organized the primary data. Le Zhang conducted the statistical analyses. Zijun Wu and Mengna Li managed the literature searches. Xiangbin Zhang and Jiansong Zhou provided supervision in the implementation of the study. All authors approved the final manuscript.
Funding
This research was funded by STI2030-Major Projects-2021ZD0200700, Major Science and Technology Projects in Changsha, China (kq2301008) and the Hunan Provincial Natural Science Foundation of China (2023JJ60144).
Data availability
No datasets were generated or analysed during the current study.
Declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee for Research of the Second Xiangya Hospital of Central South University. All participants will provide informed written consent prior to commencing the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Zheng Zhang and Ruoheng Lin share first authorship.
Contributor Information
Xiangbin Zhang, Email: 208102082@csu.edu.cn.
Jiansong Zhou, Email: zhoujs2003@csu.edu.cn.
References
- 1.O’Leary K. Global increase in depression and anxiety. Nat Med. 2021:d41591–021. [DOI] [PubMed]
- 2.Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a Meta-analysis. JAMA Pediatr. 2021;175:1142–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhan H, Zheng C, Zhang X, Yang M, Zhang L, Jia X. Chinese College Students’ stress and anxiety levels under COVID-19. Front Psychiatry. 2021;12. [DOI] [PMC free article] [PubMed]
- 4.Velikova SA. A contemporary view of depressive symptomatology. Revista geintec-gestao Inovacao e Tecnologias. 2021;11:50–60. [Google Scholar]
- 5.Bibring E. The mechanism of depression. 1953.
- 6.Shedletsky R, Endler NS. Anxiety: the state-trait model and the interaction model. J Pers. 1974;42:511–27. [DOI] [PubMed] [Google Scholar]
- 7.Koolhaas JM, Bartolomucci A, Buwalda B, de Boer SF, Flügge G, Korte SM, et al. Stress revisited: a critical evaluation of the stress concept. Neurosci Biobehavioral Reviews. 2011;35:1291–301. [DOI] [PubMed] [Google Scholar]
- 8.Vaughan RS, Edwards EJ, MacIntyre TE. Mental health measurement in a post Covid-19 world: psychometric properties and invariance of the DASS-21 in athletes and non-athletes. Front Psychol. 2020;11:590559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Welford P, O’Brien A. Improving student mental wellbeing. BMJ. 2019;366:l2421. [DOI] [PubMed]
- 10.Knapp M, Wong G. Economics and mental health: the current scenario. World Psychiatry. 2020;19:3–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhang Y, Bao X, Yan J, Miao H, Guo C. Anxiety and depression in Chinese students during the COVID-19 pandemic: a Meta-analysis. Front Public Health. 2021;9:697642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Li J-h, Feng X, -l, Mei SL, Yao DL. Investigation of study pressure effects on mental health of junior high school students in Changchun. Med Soc. 2007;20:56–7. [Google Scholar]
- 13.Giota J, Gustafsson J-E. Perceived academic demands, peer and teacher relationships, stress, anxiety and mental health: changes from grade 6 to 9 as a function of gender and cognitive ability. Scandinavian J Educational Res. 2021;65:956–71. [Google Scholar]
- 14.Zhang C, Shi L, Tian T, Zhou Z, Peng X, Shen Y et al. Associations between academic stress and depressive symptoms mediated by anxiety symptoms and hopelessness among Chinese college students. Psychol Res Behav Manage. 2022;15:547–56. [DOI] [PMC free article] [PubMed]
- 15.Schröpfer K, Schmidt N, Kus S, Koob C, Coenen M. Psychological stress among students in health-related fields during the COVID-19 pandemic: results of a cross-sectional study at selected Munich universities. Int J Environ Res Public Health. 2021;18:6611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Richardson M, Abraham C, Bond R. Psychological correlates of university students’ academic performance: a systematic review and meta-analysis. Psychol Bull. 2012;138:353. [DOI] [PubMed] [Google Scholar]
- 17.Bodys-Cupak I, Czubek K, Grochowska A. Stress and Sleep disorders in Polish nursing students during the SARS-CoV-2 Pandemic—Cross Sectional Study. Front Psychol. 2022;12:814176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chen H, Guo H, Chen H, Cao X, Liu J, Chen X, et al. Influence of academic stress and school bullying on self-harm behaviors among Chinese middle school students: the mediation effect of depression and anxiety. Front Public Health. 2023;10:1049051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kieseppä V, Holm M, Jokela M, Suvisaari J, Gissler M, Lehti V. Depression and anxiety disorders among immigrants living in Finland: Comorbidity and mental health service use. J Affect Disord. 2021;287:334–40. [DOI] [PubMed] [Google Scholar]
- 20.Bystritsky A, Kronemyer D. Stress and anxiety: counterpart elements of the stress/anxiety complex. Psychiatric Clin. 2014;37:489–518. [DOI] [PubMed] [Google Scholar]
- 21.Yalçın İ, Can N, Mançe Çalışır Ö, Yalçın S, Çolak B. Latent profile analysis of COVID-19 fear, depression, anxiety, stress, mindfulness, and resilience. Curr Psychol. 2021;41(1):459–69. [DOI] [PMC free article] [PubMed]
- 22.Mellor D, Vinet EV, Xu X, Mamat NHB, Richardson B, Román F. Factorial invariance of the DASS-21 among adolescents in four countries. Eur J Psychol Assess. 2015;31:138-42.
- 23.Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression anxiety stress scales (DASS) with the Beck Depression and anxiety inventories. Behav Res Ther. 1995;33:335–43. [DOI] [PubMed] [Google Scholar]
- 24.Gong X, Xie X, Xu R, Luo Y. Psychometric properties of the Chinese versions of DASS-21 in Chinese college students. Chin J Clin Psychol. 2010;18:443–6.
- 25.Szabó M. The short version of the Depression anxiety stress scales (DASS-21): factor structure in a young adolescent sample. J Adolesc. 2010;33:1–8. [DOI] [PubMed] [Google Scholar]
- 26.Willemsen J, Markey S, Declercq F, Vanheule S. Negative emotionality in a large community sample of adolescents: the factor structure and measurement invariance of the short version of the depression anxiety stress scales (DASS-21). Stress Health. 2011;27:e120–8. [Google Scholar]
- 27.Coker AO, Coker OO, Sanni D. Psychometric properties of the 21-item depression anxiety stress scale (DASS-21). Afr Res Rev. 2018;12:135–42. [Google Scholar]
- 28.JASP TEAM.
- 29.Tang H, Zhang Z, Chen H, Chen H, Chen X, Li S, et al. Core items selection and psychometric properties of the adult attention-deficit hyperactivity disorder self-report scale-chinese short version (ASRS-CSV). Asian J Psychiatry. 2024;99:104136. [DOI] [PubMed] [Google Scholar]
- 30.Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equation Modeling: Multidisciplinary J. 2007;14:464–504. [Google Scholar]
- 31.Borsboom D. A network theory of mental disorders. World Psychiatry. 2017;16:5–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Guo K, Zhang X, Bai S, Minhat HS, Nazan AINM, Feng J, Saliluddin. Assessing social support impact on depression, anxiety, and stress among undergraduate students in Shaanxi province during the COVID-19 pandemic of China. PLoS ONE. 2021;16:e0253891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Van den Bergh N, Marchetti I, Koster EH. Bridges over troubled waters: mapping the interplay between anxiety, depression and stress through network analysis of the DASS-21. Cogn Therapy Res. 2021;45:46–60. [Google Scholar]
- 34.Putnick DL, Bornstein MH. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. 2016;41:71–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lu S, Hu S, Guan Y, Xiao J, Cai D, Gao Z, et al. Measurement invariance of the Depression anxiety stress Scales-21 across gender in a sample of Chinese university students. Front Psychol. 2018;9:2064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Arvidsdotter T, Marklund B, Kylén S, Taft C, Ekman I. Understanding persons with psychological distress in primary health care. Scand J Caring Sci. 2016;30:687–94. [DOI] [PubMed] [Google Scholar]
- 37.Mah L, Szabuniewicz C, Fiocco AJ. Can anxiety damage the brain? Curr Opin Psychiatry. 2016;29:56–63. [DOI] [PubMed] [Google Scholar]
- 38.Midtbust MH, Alnes RE, Gjengedal E, Lykkeslet E. A painful experience of limited understanding: healthcare professionals’ experiences with palliative care of people with severe dementia in Norwegian nursing homes. BMC Palliat Care. 2018;17:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Borsboom D, Deserno MK, Rhemtulla M, Epskamp S, Fried EI, McNally RJ, et al. Network analysis of multivariate data in psychological science. Nat Rev Methods Primers. 2021;1:1–18. [Google Scholar]
- 40.Borsboom D, Deserno MK, Rhemtulla M, Epskamp S, Fried EI, McNally RJ, et al. Reply to ‘Critiques of network analysis of multivariate data in psychological science’. Nat Rev Methods Primers. 2022;2:1–2. [Google Scholar]
- 41.van Borkulo C, Boschloo L, Borsboom D, Penninx BWJH, Waldorp LJ, Schoevers RA. Association of Symptom Network structure with the course of [corrected] Depression. JAMA Psychiatry. 2015;72:1219–26. [DOI] [PubMed] [Google Scholar]
- 42.R RB. N, M M, D R, M L, M C, The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord. 2015;173. [DOI] [PubMed]
- 43.Chen I-H, Chen C-Y, Liao X-L, Chen X-M, Zheng X, Tsai Y-C, et al. Psychometric properties of the Depression, anxiety, and stress scale (DASS-21) among different Chinese populations: a cross-sectional and longitudinal analysis. Acta Psychol (Amst). 2023;240:104042. [DOI] [PubMed] [Google Scholar]
- 44.Cao C-H, Liao X-L, Gamble JH, Li L-L, Jiang X-Y, Li X-D, et al. Evaluating the psychometric properties of the Chinese depression anxiety stress scale for Youth (DASS-Y) and DASS-21. Child Adolesc Psychiatry Ment Health. 2023;17:106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cao C-H, Liao X-L, Jiang X-Y, Li X-D, Chen I-H, Lin C-Y. Psychometric evaluation of the depression, anxiety, and stress scale-21 (DASS-21) among Chinese primary and middle school teachers. BMC Psychol. 2023;11:209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mascaro N, Rosen DH. Existential meaning’s role in the enhancement of hope and prevention of depressive symptoms. J Pers. 2005;73:985–1014. [DOI] [PubMed] [Google Scholar]
- 47.Schafer KM, Lieberman A, Sever AC, Joiner T. Prevalence rates of anxiety, depressive, and eating pathology symptoms between the pre-and peri-COVID-19 eras: a meta-analysis. J Affect Disord. 2022;298:364–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.CAI Y, DONG S. HU C-P. Network analysis and its applications in psychology. Adv Psychol Sci. 2020;28:178. [Google Scholar]
- 49.Neal ZP, Forbes MK, Neal JW, Brusco MJ, Krueger R, Markon K, et al. Critiques of network analysis of multivariate data in psychological science. Nat Reviews Methods Primers. 2022;2:90. [Google Scholar]
- 50.McNally RJ. Can network analysis transform psychopathology? Behav Res Ther. 2016;86:95–104. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
No datasets were generated or analysed during the current study.