

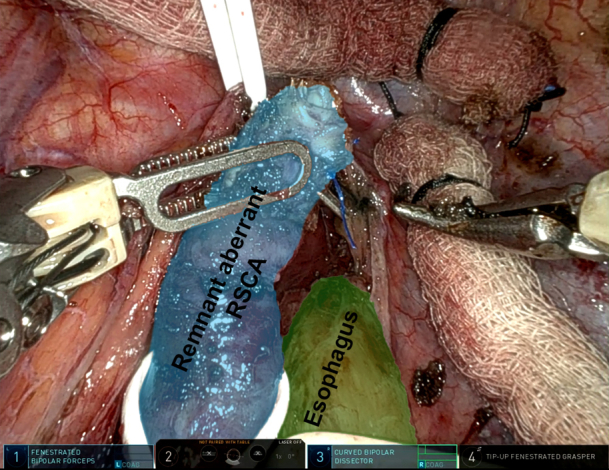
Robot-assisted thoracoscopic view of the remnant aberrant right subclavian artery.
Central Message.
Treatment of symptomatic dysphagia lusoria from an aberrant right subclavian artery was safely achieved using a multidisciplinary 3-staged minimally invasive approach.
Dysphagia lusoria is the rare phenomenon of extrinsic compression of the esophagus caused by an aberrant right subclavian artery. Treatment is indicated for symptomatic relief and to prevent aneurysmal dilation. Surgical treatment traditionally involves ligation of the aberrant subclavian artery at its origin via thoracotomy and revascularization of the subclavian artery.1 We describe a multidisciplinary 3-staged minimally invasive treatment approach. Institutional review board approval and consent was not required for this case report.
Clinical Report
Two similarly aged male patients (ages 57 and 51 years) presented with dysphagia secondary to extrinsic compression of the esophagus by an aberrant right subclavian artery originating from the descending aorta and taking a retroesophageal course (Figure 1).
Figure 1.
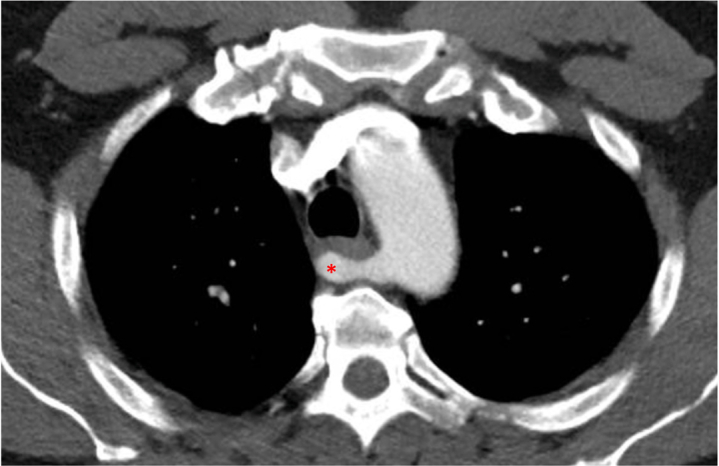
Computed tomography image showing the aberrant right subclavian originating from the descending aorta and taking a retroesophageal course (red star).
Both patients were treated in a staged fashion starting with transposition of the aberrant right subclavian artery to the right common carotid artery via a neck incision. This was followed by endovascular placement of a thoracic aortic stent graft (ie, thoracic endovascular aortic repair) to cover the orifice of the aberrant right subclavian artery. Using a right robotic video-assisted thoracoscopic surgery approach, the remnant aberrant artery was dissected free from surrounding structures (Figure 2) to its previously transected distal extent, ligated at its origin using a robotic stapler, and extracted. The arterial stump was oversewn and pexied away from the esophagus to minimize risk of erosion or fistulization to the esophagus (Video 1).
Figure 2.

Robot-assisted right thoracoscopic view of the remnant aberrant right subclavian artery. RSCA, Right subclavian artery.
The 57-year-old patient had persistent dysphagia following carotid-subclavian transposition and only experienced symptom relief after the remnant aberrant artery was resected. Following resection of their remnant aberrant subclavian artery, patients were discharged on postoperative days 3 and 2, respectively, recovered well without any short-term complications, and achieved complete symptom resolution. Although both patients reported no symptom recurrence via informal telephone follow-up, they were lost to long-term imaging follow-up.
Conclusions
Effective treatment of dysphagia lusoria may require resection of the remnant aberrant subclavian artery after carotid-subclavian transposition. A transthoracic robotic approach to dividing and removing the aberrant artery has been reported.2, 3, 4 When transposition is performed as the initial step, thrombosis of the remnant artery can occur. Unique to our strategy, we deployed endovascular stent graft coverage of the remnant orifice to mitigate potential thromboembolic events secondary to manipulation of the thrombosed remnant, thereby improving the safety of minimally invasive resection of the remnant artery. However, longer-term consequences of endovascular stent graft use in this specific setting are unknown.
Webcast
You can watch a Webcast of this AATS meeting presentation by going to: https://www.aats.org/resources/staged-robotic-video-assisted-7224.
Conflict of Interest Statement
Dr Altorki has received grants or contracts from AstraZeneca and Roche/Genentech and has ownership interest in Angiocrine Bioscience, TMRW, and Viewpoint Medical. Dr Port has leadership and ownership interest in Angiocrine Bioscience, TMRW, and Viewpoint Medical. Dr Lee receives speaker fees from AstraZeneca. All other authors reported no conflicts of interest.
The Journal policy requires editors and reviewers to disclose conflicts of interest and to decline handling or reviewing manuscripts for which they may have a conflict of interest. The editors and reviewers of this article have no conflicts of interest.
Footnotes
Read at the 104th Annual Meeting of The American Association for Thoracic Surgery, Toronto, Ontario, Canada, April 27-30, 2024.
IRB: This was a case report that did not require review or approval by the Institutional Review Board as it did not involve human subjects research.
Informed consent: Patient written consent for the publication of the study was not obtained as all unique patient information is de-identified.
Supplementary Data
Robotic-assisted right thoracoscopic technique for division of the remnant aberrant right subclavian artery after subclavian-carotid transposition and TEVAR. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00341-9/fulltext.
{kind=link}
References
- 1.Levitt B., Richter J.E. Dysphagia lusoria: a comprehensive review. Dis Esophagus. 2007;20:455–460. doi: 10.1111/j.1442-2050.2007.00787.x. [DOI] [PubMed] [Google Scholar]
- 2.Kimble Jett G., Tran A., Hafen L., Shutze W. Robotic-assisted treatment of aberrant retroesophageal right subclavian artery. 2021. https://ctsnet.figshare.com/articles/media/Robotic-Assisted_Treatment_of_Aberrant_Retroesophageal_Right_Subclavian_Artery/14465859?file=27687279
- 3.Meredith L., Nooromid M., Okusanya O. Robotic resection of aberrant right subclavian artery for dysphagia lusoria. 2023. https://www.ctsnet.org/article/robotic-resection-aberrant-right-subclavian-artery-dysphagia-lusoria [DOI] [PMC free article] [PubMed]
- 4.La Regina D., Prouse G., Mongeli F., Pini R. Two-step treatment of dysphagia lusoria: robotic-assisted resection of aberrant right subclavian artery following aortic debranching. Eur J Cardiothorac Surg. 2020;58(5):1093–1094. doi: 10.1093/ejcts/ezaa182. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Robotic-assisted right thoracoscopic technique for division of the remnant aberrant right subclavian artery after subclavian-carotid transposition and TEVAR. Video available at: https://www.jtcvs.org/article/S2666-2507(24)00341-9/fulltext.