

Abstract
Ectopic thyroid tissue along the line of descent of thyroid from foramen caecum along thyroglossal duct to the normal anatomic location in neck has been reported. Ectopic thyroid tissue in adrenal gland (ETTAG) is rarely encountered and very few cases have been reported in literature. The most common differential diagnosis to be considered when thyroid follicles are noted in adrenal gland are metastasis from a thyroid malignancy or a teratoma or an ectopic thyroid tissue in adrenal gland. We present a case of an adrenal incidentaloma in a young pregnant female which was diagnosed to be ectopic thyroid tissue in adrenal gland. The review of literature of similar cases of this rare embryological aberrance is discussed. To our knowledge, only 16 such cases have been documented in literature and our case is the first one from Indian subcontinent and the largest documented with respect to size.
Keywords: Thyroid, ETTAG, Ectopic thyroid, Adrenal gland, Incidentaloma, Teratoma, Metastasis, Pregnancy
Introduction
Ectopic thyroid tissue along the line of descent of thyroid from foramen caecum along thyroglossal duct to the normal anatomic location has been reported, in the so called Wölffer’s area [1]. The are reports of ectopic thyroid tissue in areas above the diaphragm and seldom reported in areas below diaphragm like in duodenum, pancreas and liver [2]. Ectopic thyroid tissue in adrenal gland is a very rare presentation and is mostly asymptomatic and diagnosed only by post-surgery histopathological examination. Ectopic thyroid tissue can have all the conditions that involve normal thyroid, like thyroiditis, thyrotoxicosis, as well as malignancy. ETTAG must always be distinguished from a metastasis originating from a thyroid carcinoma. It is extremely difficult to explain the reason for occurrence of ectopic thyroid in adrenal gland but this need to be considered as a differential diagnosis when evaluating cystic adrenal incidentalomas.
Case presentation
A 32-year-old female was incidentally found to have right adrenal mass during her routine ultrasound during first trimester antenatal checkup. She underwent evaluation with serum catecholamines which was normal. She underwent MRI abdomen which showed a 12 cm x 10 cm T2 hyperintense solid cystic lesion in right suprarenal region in hepatorenal space She was diagnosed to have a Non-functional adrenal tumor, and was observed during pregnancy. Patient was advised surgery for the adrenal tumor during the third trimester but she defaulted. She presented 6 months after delivery with complaints of abdominal distention and increase in size of swelling associated with dull aching abdominal pain. In view of the size of tumor and increase in size, she underwent re-evaluation with CECT abdomen and a whole-body PET CT which showed a 13 × 10 cm right adrenal mass with low FDG avidity (Fig. 1). She was also found to have a 3 × 3 cm left thyroid nodule. She had a past history of right hemithyroidectomy, at some other hospital 10 years back for a benign thyroid nodule and the histopathology was reported as benign colloid nodule. USG neck revealed TIRADS 2 nodule in left lobe of thyroid with no cervical lymph nodes. FNAC of left thyroid nodule was done and was reported as benign colloid nodule (Fig. 2). Her thyroid function test was normal. She underwent Right adrenalectomy. Post operative period and recovery were uneventful.
Fig. 1.

A) CECT abdomen showing a right adrenal mass B) PET CT showing adrenal mass with low FDG avidity
Fig. 2.

Fine needle aspiration cytology of left thyroid nodule- benign colloid nodule (high and low power view)
Histopathology
Histopathology revealed a single globular mass of size 14 × 13 × 5 cm weighing 1045gms. External surface- grey white, globular, smooth and Cut surface extruded gelatinous material with capsule. (Fig. 3) Well circumscribed lesion with solid and cystic components were noted. Microscopy revealed a well circumscribed lesion showing thyroid follicles of varying sizes, filled with colloid and overlying area of thin rim of compressed normal adrenal tissue (Fig. 4). No evidence of overt atypia noted in the thyroid follicular cells. Immunohistochemistry for thyroglobulin and TTF-1 were positive (Fig. 5) confirming thyroid origin. Further Immunohistochemistry was done to check for an adrenal metastasis from thyroid malignancy. Immunohistochemistry for CK 19, Galectin 3 and HBME 1 were negative (Fig. 6). The tumour blocks were sent for BRAFV600 mutation analysis and No V600 mutation was detected in the given specimen.
Fig. 3.

Right adrenal cystic mass of size 14 × 13 × 5 cm weighing 1045GMS
Fig. 4.
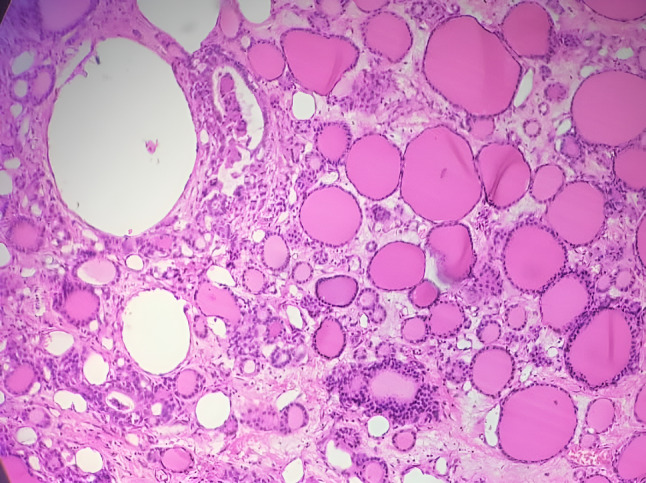
Well circumscribed lesion showing thyroid follicles of varying sizes, filled with colloid
Fig. 5.

Immunohistochemistry to confirm thyroid origin- thyroglobulin and TTF-1 are positive. A) TTF1 positive B) thyroglobulin positive
Fig. 6.

Immunohistochemistry to rule out metastasis from thyroid malignancy- CK 19, galectin 3 and HBME 1 were negative. A) CK 19 negative B) galectin 3 negative C) HBME 1 negative
Discussion
The thyroid tissue develops during the fourth embryonic week as thyroid primordium from endoderm at foramen caecum and by the seventh week, penetrates the underlying mesoderm, descends to the adult position in the neck anterior to trachea. During its descent it is attached to foramen caecum by thyroglossal duct. Ectopic thyroid gland along this pathway of thyroglossal duct can be seen in neck, the mediastinum, the pharynx or the larynx. Outside the route of embryonal descent, intra-abdominal thyroid tissues have been reported in sites like gallbladder, the mesentery of the small intestine, the pancreas, and the space posterior to the spleen and stomach [2–4].
Thyroid develops from endoderm and most ectopic thyroid deposits are also found in endodermal derivatives whereas adrenal cortex is derived from Intermediate mesoderm and medulla is derived from ectodermal neural crest cells. So, the possible explanation for ETTAG could be due to the presence of adrenal stem cells with propensity to develop thyroid tissue [5]. To our knowledge this case is just the 17th case of ETTAG reported in literature in 15 publications (Table 1) and is the first one to be reported in a pregnant female in Indian subcontinent. A review of literature of previous cases shows that ETTAG is more common in female (16:1) and usually cystic in nature and most commonly presents as an adrenal incidentaloma diagnosed with either CT or MRI with normal Thyroid function tests and normal serum catecholamine levels. The initial few cases were reported mainly from Japan [8–13] and the age of presentation is from 29 to 67 years. There is no right or left predominance in presentation. Lesions were 8 mm to 8 cm in size and compared to the previous cases, this is the largest reported in size and weight measuring around 14 cm and weighing around 1 kg.
Table 1.
Reported cases of ETTAG in literature
| Case no | Year of publication | Author | Country | Age/Sex | Presentation | Pathology finding | Thyroid evaluation |
|---|---|---|---|---|---|---|---|
| 1 | 1996 | Tsujimura [8] | Japan | 61/F | Incidental finding | Unilocular /Right adrenal /cystic/ 3.5 cm | No evidence of cancer |
| 2 | 1999 | Shiraisi [9] | Japan | 50/F | Right hypochondrial pain | Multilocular/ Right adrenal/ cystic 3 cm | USG thyroid normal- no evidence of cancer |
| 3 | 1999 | Shiraisi [9] | Japan | 50/M | Incidental finding | Multilocular/Right adrenal/ cystic/ ruptured cyst | USG and Iodine scintigraphy normal – no evidence of cancer |
| 4 | 2006 | Shuno [10] | Japan | 50/F | Incidental finding on Preoperative CT for gastric cancer | Multilocular/ left adrenal/ cystic/ 5 cm | Iodine scintigraphy normal- no evidence of cancer |
| 5 | 2006 | Hagiuda [11] | Japan | 54/F | Hypertension evaluation | Unilocular/ Left adrenal/ cystic/ 8 mm | MRI and thyroid scintigraphy normal- no evidence of cancer |
| 6 | 2006 | Takao [12] | Japan | 67/F | Incidental finding on Preoperative CT for gastric cancer | Multilocular/ left adrenal/ cystic/ 3 cm | USG and Iodine scintigraphy normal – no evidence of cancer |
| 7 | 2011 | Bohinc [13] | USA | 61/F | Hypertension evaluation | Solid nodule/ left adrenal/8 mm | USG thyroid nodule FNAC hurthle cells, thyroidectomy HPE- Micropapillary thyroid carcinoma |
| 8 | 2013 | Romero- Rojas [14] | Colombia | 38/F | Back pain | Unilocular/ Left adrenal/ cystic/ 5.2 cm | Thyroid USG normal- no evidence of cancer |
| 9 | 2013 | Romero- Rojas [14] | Spain | 59/F | Incidental finding | Unilocular/ left adrenal/ cystic/ 4 cm | Thyroid USG normal- no evidence of cancer |
| 10 | 2014 | Gourmaud [15] | Switzerland | 51/F | Incidental finding | Multilocular/ Left adrenal/ cystic / 3.3 cm | Thyroid USG normal- no evidence of cancer |
| 11 | 2015 | Casadei [16] | Italy | 32/F | Low back ache | Unilocular/ Right adrenal/ cystic/ 4 cm | Thyroid USG and CT- no evidence of cancer |
| 12 | 2016 | Yilmaz [17] | Turkey | 57/F | Incidentaloma | Solid cystic/ Right adrenal/ 6 mm | MNG- total thyroidectomy – no evidence of cancer |
| 13 | 2017 | LI [18] | China | 49/F | Incidentaloma | Unilocular/ Left adrenal/ Cystic/ 2 cm | USG thyroid normal- no evidence of cancer |
| 14 | 2019 | Rawitzer [19] | Germany | 39/F | Back pain | Unilocular/Right adrenal/ cystic/8 cm | Thyroid USG normal |
| 15 | 2020 | Zhang [20] | China | 33/F | Incidentaloma | Unilocular/ left adrenal/ cystic / 7 cm | USG thyroid normal- no evidence of cancer |
| 16 | 2020 | Paunovic [21] | Serbia | 29/F | Incidentaloma | Unilocular/ left adrenal/ cystic/ 2.8 cm | USG thyroid normal- no evidence of cancer |
| 17 | 2022 | Our case | India | 32/F | Pregnancy Incidentaloma | Multilocular/ Right adrenal/ solid cystic/ 14 cm | USG colloid nodule FNAC no evidence of cancer |
It is important to distinguish this condition from metastatic thyroid cancer. Adrenal metastasis from thyroid cancers though rare have been reported and should be the first differential to be considered in case of histopathology showing thyroid follicles in adrenal gland [6]. Hence all these patients need to undergo clinical radiological and FNAC to rule out a thyroid malignancy. In a few cases, patients underwent total thyroidectomy to rule out malignancy. Our patient too had an Ultrasound which showed colloid nodules and no evidence of malignancy in thyroid. Metastasis from thyroid cancer can be extremely well differentiated and difficult to distinguish from ectopic benign thyroid deposit. Meyer and Steinberg’s proposed criteria for the differential diagnosis of non-neoplastic thyroid tissue from metastatic thyroid cancer; microscopic size, round or oval follicles, nonpapillary pattern, uncrowded nuclei, and the absence of stromal proliferation or psammoma bodies indicate a nonneoplastic lesion [7]. IHC for CK19, galectin-3 or HBME 1, molecular analysis for BRAF or RAS mutations might be helpful to diagnose metastasis from thyroid carcinomas. The other differential diagnosis to be considered is that of a teratoma. But in none of the previous cases reported, the histopathology had any evidence of any other tissue components to suggest the ectopic thyroid is a teratoma/choriostoma.
Conclusion
Ectopic thyroid tissue is a rare entity and is usually found along the route of embryonal descent and rarely reported in adrenal gland. Aberrant descent of embryological tissue can justify Ectopic thyroid in sites such as the heart, mediastinum, and at mid-subdiaphragmatic locations like the porta hepatis and duodenum but do not explain its presence in adrenal gland. These are mostly cystic adrenal masses detected incidentally and are diagnosed only on histopathological examination. When thyroid tissue is identified in adrenalectomy specimen the differential diagnosis to be considered are ETTAG, teratoma, or metastasis from a thyroid primary. The relevant literature review and the evaluation in our case helps us better understand this rare pathology and has to be considered as a differential diagnosis in case of cystic adrenal incidentalomas. Thorough thyroid evaluation is mandatory in all patients with ETTAG.
Acknowledgements
The Authors would like to thank and acknowledge the efforts of Dr Sandhya Sundaram and Dr Leena Joseph, Professors in Pathology for their help in histopathological diagnosis, Immunohistochemistry studies and Molecular studies in this case.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by VV and BM. The draft of the manuscript was written by VV and all authors commented on the manuscript. Article Review and editing was done by SK and GS Supervision was by JCB. All authors read and approved the final manuscript.
Funding
The authors did not receive support from any organization for the submitted work. No external funding utilised.
Data availability
No datasets were generated or analysed during the current study.
Declarations
Ethical standards and ethics committee approval
The authors certify that the patient care was accordance with the Declaration of Helsinki. All treatment was as per standard treatment guidelines and no deviation was from standard of care. No patient data collection or experimental or novel intervention was done in this patient. This is not a study but a mere reporting of a case findings and hence was hence approved for exemption from ethical committee approval of our institution.
Consent to participate
The authors certify that they have obtained all appropriate patient consent forms. The patient was explained about the treatment option the complications the adverse reactions and the follow up protocol and was explained in detail regarding the same in patient`s own language and patient consented for the procedure.
Consent for publication
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their informed written consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity. Patient was explained that the text and any pictures or videos published in the article will be freely available on the internet and may be seen by the general public. Also, images are entirely unidentifiable and there are no details on individuals reported within this manuscript.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Noussios G, Anagnostis P, Goulis DG, et al. Ectopic thyroid tissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol. 2011;165:375–82. [DOI] [PubMed] [Google Scholar]
- 2.Cassol CA, Noria D, Asa SL. Ectopic thyroid tissue within the gall bladder: case report and brief review of the literature. Endocr Pathol. 2010;21:263–5. [DOI] [PubMed] [Google Scholar]
- 3.Eyüboğlu E, Kapan M, Ipek T, et al. Ectopic thyroid in the abdomen: report of a case. Surg Today. 1999;29:472–4. [DOI] [PubMed] [Google Scholar]
- 4.Takahashi T, Ishikura H, Kato H, et al. Ectopic thyroid follicles in the submucosa of the duodenum. Virchows Arch Pathol Anat Histopathol. 1991;418:547–50. [DOI] [PubMed] [Google Scholar]
- 5.Bishop E, Eble JN, Cheng L, et al. Adrenal myelolipomas show nonrandom X-chromosome inactivation in hematopoietic elements and fat: support for a clonal origin of myelolipomas. Am J Surg Pathol. 2006;30:838–43. [DOI] [PubMed] [Google Scholar]
- 6.Zhou Zhen-yu, Jun J, et al. Clinical analysis of 9 cases of ectopic thyroid carcinoma[J]. Chin J Clin Res. 2012;25(12):1197–8. [Google Scholar]
- 7.Meyer JS, Steinberg LS. Microscopically benign thyroid follicles in cervical lymph nodes. Serial section study of lymph node inclusions and entire thyroid gland in 5 cases. Cancer. 1969;24(2):302–11. 10.1002/1097-0142(196908)24:2%3C;2820240213%3E;PMID. [DOI] [PubMed]
- 8.Tsujimura A, Takahe M, Takayama H, et al. Ectopic thyroid tissue in a cystic adrenal mass. Br J Urol. 1996;77:605–6. [DOI] [PubMed] [Google Scholar]
- 9.Shiraishi T, Imai H, Fukutome K, Watanabe M, Yatani R. Ectopic thyroid in the adrenal gland. Hum Pathol. 1999;30(1):105-8. 10.1016/s0046-8177(99)90309-x. PMID: 9923936. [DOI] [PubMed]
- 10.Shuno Y, Kobayashi T, Morita K, et al. Ectopic thyroid in the adrenal gland presenting as cystic lesion. Surgery. 2006;139:580–2. [DOI] [PubMed] [Google Scholar]
- 11.Hagiuda J, Kuroda I, Tsukamoto T, Ueno M, Yokota C, Hirose T, Deguchi N. Ectopic thyroid in an adrenal mass: a case report. BMC Urol. 2006;6:18. 10.1186/1471-2490-6-18. PMID: 16899136; PMCID: PMC1555601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Takao H, Doi I, Watanabe T. Ectopic thyroid in the adrenal gland: computed tomography findings. J Comput Assist Tomogr. 2006;30:221–2. [DOI] [PubMed] [Google Scholar]
- 13.Bohinc BN, Parker JC, Hope WW et al. Micropapillary thyroid carcinoma and concomitant ectopic thyroid tissue in the adrenal gland: metastasis or metaplasia? Thyroid. 2011; 21:1033-8. [DOI] [PubMed]
- 14.Romero-Rojas A, Bella-Cueto MR, Meza-Cabrera IA, et al. Ectopic thyroid tissue in the adrenal gland: a report of two cases with pathogenetic implications. Thyroid. 2013;23:1644–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gourmaud J, Bongiovanni M, Triponez F, et al. Ectopic thyroid tissue in the adrenal gland. Endocr Pathol. 2014;25:353–5. [DOI] [PubMed] [Google Scholar]
- 16.Casadei GP, Bertarelli C, Giorgini E, et al. Ectopic thyroid tissue in the adrenal gland: report of a case. Int J Surg Pathol. 2015;23:170–5. [DOI] [PubMed] [Google Scholar]
- 17.Yılmaz BA, Aktürk M, Kan E, et al. Ectopic thyroid in the adrenal presenting as an adrenal incidentaloma. Turk J Endocrinol Metab. 2016;20:4. [Google Scholar]
- 18.Li H, Chen Q, Zhu Y, et al. Ectopic thyroid tissue in the adrenal gland: a case report with clinical and pathogenetic implications. Int J Clin Exp Patho. 2017;10:8761–4. [PMC free article] [PubMed] [Google Scholar]
- 19.Rawitzer J, Kapakoglou A, Walz MK, et al. Ektopes Schild drüsengewebe in Der Nebenniere. Pathologe. 2020;41:177–80. [DOI] [PubMed] [Google Scholar]
- 20.Zhang L-I, Zhai X-Q, Wang Lan-ping, Ji M, Zhou F. Ectopic thyroid tissue in the adrenal gland: a case report and literature review. Volume 21. Human Pathology: Case Reports; 2020. p. 200386. [Google Scholar]
- 21.Paunovic I, Rovcanin B, Jovanovic M, Buzejic M, Dundjerovic D, Zivaljevic V. Ectopic thyroid tissue in adrenal gland, case report and review of literature. Gland Surg. 2020;9(5):1573–8. 10.21037/gs-20-471. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No datasets were generated or analysed during the current study.