

Abstract
Introduction
Nasal myiasis refers to the presence of the larvae (maggots) within the nasal cavity. This rare condition occurs when the larval stage of certain dipteran flies invades the nose.
Case presentation
We report a case of Nasal myiasis with Angioedema in a 7-year-old girl from rural Ethiopia. The patient presented with worsening facial swelling and expulsion of worms from both nostrils for three days, preceded by foul-smelling nasal discharge for three years. Examination revealed bilateral periorbital edema, upper lip edema, and bilateral nasal cavities filled with maggots and blood‑tinged discharge. After investigations including blood tests and a head CT scan, the patient was diagnosed with nasal myiasis. She was treated with broad-spectrum antibiotics, dexamethasone, endoscopic maggot removal, and debridement. She was discharged with improvement and scheduled for a follow-up. On follow there was no recurrence, the posterior septal perforation was asymptomatic and did not require surgical intervention. This case report adheres to SCARE criteria.
Clinical discussion
Nasal myiasis with angioedema is a rare clinical condition. Diagnosis relies on clinical examination to identify the larvae. Endoscopic larvae extraction combined with over-nasal saline irrigation and systemic broad-spectrum antibiotic was considered appropriate and effective management of nasal myiasis.
Conclusion
Nasal myiasis, an infestation of the nasal passages by fly larvae, is a rare clinical condition, particularly in pediatric populations. Prompt and complete eradication of myiasis minimizes damage to intranasal tissues and reduces the risk of complications. Maintaining good hygiene practices is crucial in preventing this condition.
Keywords: Nasal myiasis, Maggot, Myiasis, Pediatrics nasal myiasis, Endoscopic debridement, Case report
Highlights
-
•
Nasal myiasis refers to the presence of the larvae (maggots) within the nasal cavity.
-
•
Angioedema is a reaction to a trigger that causes swelling in the tissue below the inner layer of your skin or below a mucous membrane.
-
•
Nasal myiasis with Angioedema is a rare clinical condition treatment depending on the symptoms' severity.
1. Introduction
Myiasis is an infestation caused by dipterous larvae in living human and vertebral animals [1,2]. It is an opportunistic parasitic infestation in humans and animals caused by house fly larvae and is commonly found in tropical and subtropical areas of the world [3,13]. The term myiasis comes from the Greek word “muia” or “mya” meaning fly and “iasis” meaning disease [4,7]. Myiasis can occur in any tissues, organs, and body cavities of human beings or animals when it is invaded and infested by the larval of nonbiting flies of the order Diptera [5]. Nasal Myiasis is a rare embarrassing condition defined as the presence of larvae (maggots) within the nasal cavity [4,7]. Diagnosis in most cases can be easily performed by clinical examination, Nasal endoscopy will reveal crawling maggots inside the nasal cavity, combined with alterations in the mucous membrane, secretions, and necrotic tissue [12,13]. CT scans of the nose and sinus are useful to indicate the extent of the infestation and whether maggots have spread beyond the sinonasal area [11]. Nasal maggot infestation presents a serious threat due to the potential for intracranial and intraorbital penetration. Additionally, the larvae can trigger angioedema as a result of the body's reaction [13,15,16]. Treatment for nasal myiasis typically includes a combination of local and systemic measures, such as removing the maggots, administering broad-spectrum antibiotics, and a semisynthetic broad-spectrum antibiotic [13,14]. This case report adheres to SCARE criteria [17].
2. Case report
We present a case of a 7-year-old female child from a rural part of Ethiopia brought by her family with a complaint of worsening facial swelling and expression of worms from the both nostrils of three days duration associated with this she had a history of intermittent expression of worms from the nostrils for the past two weeks, and foul-smelling nasal discharge for the past three years. Her past medical history was insignificant. On physical examination, it was noticed that the bilateral periorbital area and upper lip were edematous, bilateral nasal cavity was filled with maggots and thin blood mixed nasal discharge from the bilateral nostril (Fig. 1). Her Pulse rate was 96 beats per minute, her Blood pressure was 90/60 mmHg, her Respiratory rate was 22 breaths per minute, and normal eye examination.
Fig. 1.

Preoperative examination revealed the bilateral nostrils filled with larvae and facial swelling.
White blood cell count was 9.49 ∗ 103/mm3 (Normal range: 4.0 ∗ 103/mm3–10.0 ∗ 103/mm3), Hemoglobin was 12.1 g/dl (Normal range: 11.9 g/dl–15.9 g/dl), platelet count 284 ∗ 103/mm3 (normal range 100 ∗ 103/mm3–300 ∗ 103/mm3), Fasting blood glucose 92 mg/dl (normal range 70–100 mg/dl), and creatinine 0.37 (normal range 0.32–0.59). A Head CT scan without contrast revealed opacification of bilateral maxillary and ethmoid sinuses, bilaterally atrophied inferior and middle turbinates, and defect in the posterior nasal septum (Fig. 2).
Fig. 2.

Head CT scan, opacification of bilateral maxillary and ethmoid sinuses, bilaterally atrophied inferior and middle turbinate and defect in the posterior nasal septum.
The final diagnosis was Nasal myiasis with Angioedema. She was admitted to the ward with broad-spectrum antibiotics (ceftriaxone 50 mg/kg/day into two divided doses), Dexamethasone (0.5 mg/kg/day in three divided doses for 48 h), and analgesics (Acetaminophen 10 mg/kg three times per day) were started. Endoscopic removal of the maggot and debridement of the necrotic tissue are done under general anesthesia, intraoperative findings include maggot in the nasal vestibule and nasal cavity proper, nasal septum perforated, necrotic tissue over the lateral nasal wall, and edematous maxillary and ethimoidal sinus mucosa bilaterally (Fig. 3). She was kept in the ward for 07 days with antibiotics and nasal saline irrigation to remove blood encrustations four times per day. Upon discharge, the nasal cavity was clean (Fig. 4), and the family was advised on the prevention and appointed to a follow-up clinic. On follow there was no recurrence, the posterior septal perforation was asymptomatic and did not require surgical intervention.
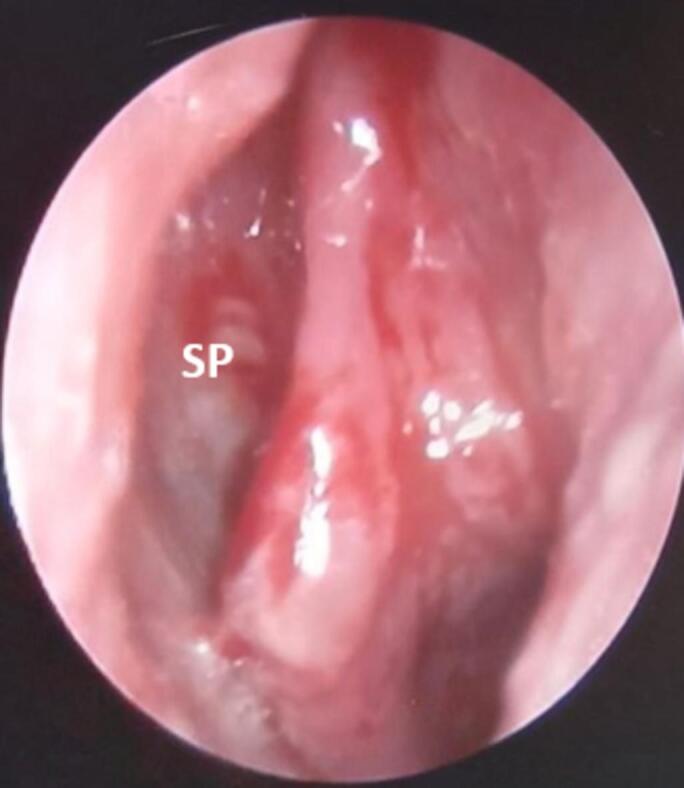
Fig. 3.

Intraoperative images include maggot in the cavity proper, nasal septum perforated (SP), and necrotic tissue over the lateral nasal wall.
Fig. 4.
After treatment clean nasal cavity with a perforated posterior nasal septum (SP).
3. Discussion
Myiasis, the infestation of living tissue by fly larvae, is classified within the ICD-10 into various categories, including Cutaneous myiasis, Wound myiasis, Ocular myiasis, Nasopharyngeal myiasis (nose, sinus, larynx, and pharynx), Aural myiasis, Myiasis of other sites, and Myiasis, unspecified [6]. While myiasis can affect various bodily locations, otorhinolaryngological myiasis (affecting the nose, ears, trachea, and mouth) is particularly rare, with only a handful of studies, primarily case reports, documenting its occurrence [2]. The limited research is due in part to incomplete registries and a lack of follow-up with patients [2]. The nose, ears, and eyes are the most common sites of invasion in the head and neck region [8]. Although infrequent, myiasis is more prevalent in developing, low-income tropical countries, particularly among impoverished adults and elderly villagers who may neglect hidden nasal conditions and live in unhygienic environments [9].
Nasal Myiasis is defined as the presence of larvae (maggots) within the nasal cavity, it is a rare embarrassing situation for the child, parents, and family, which creates a social stigma still in this time [4,7,10]. The process begins when a fly enters the nasal cavity and deposits its eggs. These eggs hatch into larvae within 24 h. The larvae mature fully within 2–3 days and then migrate in search of dry environments to complete their life cycle [15]. It is commonly seen among low-socioeconomic status, mentally retarded persons, immunocompromised patients, chronic sinonasal diseases, intubated patients, tropical weather, and unhygienic living status [4,13,16]. Associated factors grossly related to nasal myiasis are Sinonasal neglected or untreated mass, atrophic rhinitis, chronic infections like tuberculosis, leprosy, or Hansen's disease, mentally retarded, and prolonged bed-ridden patient [2,11].
The manifestations of nasal myiasis are usually related to the presence and movement of the larvae and include nasal and/or facial pain, bloody or mucopurulent nasal secretion, epistaxis, foul smell, and anosmia [12]. Diagnosis in most cases can be easily performed by clinical examination [13]. Nasal endoscopy will reveal crawling maggots inside the nasal cavity, combined with alterations in the mucous membrane, secretions, and necrotic tissue. CT scans of the nose and sinus are useful to indicate the extent of the infestation and whether maggots have spread beyond the nasosinusal area [11]. Nasal maggot infestation poses a serious threat due to the potential for intracranial and intraorbital penetration [13]. Treatment for nasal myiasis typically includes a combination of local and systemic measures, such as removing the maggots, administering broad-spectrum antibiotics, and oral ivermectin, a semisynthetic broad-spectrum antibiotic [13,14]. Maintaining good hygiene practices is crucial in preventing this condition [4,12]. In our case the patient was admitted prophylactic broad-spectrum antibiotics were given, endoscopic maggot removal and debridement were done under general anesthesia, and postoperatively the nasal cavity was cleaned to remove blood encrustations with normal saline and discharge improved. On follow there was no recurrence, the posterior septal perforation was asymptomatic and did not require surgical intervention.
4. Conclusion
Nasal myiasis, an infestation of the nasal passages by fly larvae, is a rare clinical condition, particularly in pediatric populations. However, it remains a concern in developing and underdeveloped countries. Diagnosis is often straightforward, relying on clinical examination to identify the larvae. Endoscopic larvae extraction combined with nasal saline irrigation and systemic broad-spectrum antibiotic was considered appropriate and effective management of nasal myiasis. Prompt and complete eradication of myiasis minimizes damage to intranasal tissues and reduces the risk of complications. Maintaining good hygiene practices is crucial in preventing this condition.
Author contribution
Hailemariam Kassaye Alebie, Department of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Writing the paper, and Corresponding author
Phone: +251928548595
Email: mariamhk21@gmail.com
Bisrat Getachew Yihun, Assistant Professor of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Phone: +251913672185
Email: schbisrat@gmail.com
Waltenigus Birhanu Demsie, Department of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Phone: +251921126315
Email: waltebirh@gmail.com
Hikma Amin Aliye, Department of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Phone: +251911226335
Email: hikamin2025@gmail.com
Alebachew Melkamu Aschenkew, Department of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Phone: +251911226335
Email: alebiekas@gmail.com
Consent
Written informed consent was obtained from the patient's father to publish this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Our institution's policy exempts reporting individual cases from ethical review, as we rigorously uphold patient anonymity and confidentiality in all case presentations.
Guarantor
-
1.
Hailemariam Kassaye Alebie, Department of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
-
2.
Bisrat Getachew Yhunie, Assistant professor of Otolaryngology-Head and Neck Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Provenance and peer review
Not published.
Research registration number
On processes.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
All authors declare no conflicts of interest in this article.
Data availability
All data are included within the article.
References
- 1.Sayyahfar, S., Zare Mahmoudabadi, R., Mahdavynia, S., Esteghamati, A., Salemi, B., & Khanaliha, K. (n.d.). First report of nasal myiasis caused by Lucilia sericata in the pediatric age group from Tehran, Iran. 2021; (17):7 https://creativecommons.org/licenses/by-nc/4.0/. [DOI] [PMC free article] [PubMed]
- 2.Rana A.K., Sharma R., Sharma V.K., Mehrotra A., Singh R. Otorhinolaryngological myiasis: the problem and its presentations in the weak and forgotten. Ghana Med. J. 2020;54(3):173–178. doi: 10.4314/gmj.v54i3.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bosmia A.N., Zimmermann T.M., Griessenauer C.J., Shane Tubbs R., Rosenthal E.L. Nasal myiasis in Hinduism and contemporary otorhinolaryngology. J. Relig. Health. 2017;56(4):1263–1281. doi: 10.1007/s10943-013-9817-8. [DOI] [PubMed] [Google Scholar]
- 4.Swain S., Sarangi R., Mohanty J. Nasal myiasis among pediatric patients: our experiences. Med. J. Dr. D.Y. Patil Vidyapeeth. 2020;(1):48–52. doi: 10.4103/mjdrdypu.mjdrdypu_110_19. [DOI] [Google Scholar]
- 5.Professor of Medical Entomology at the Liverpool School of Tropical Medicine. 1997;(1):78.
- 6.World Health Organization . Vol. 1. World Health Organization; 2011. International Statistical Classification of Diseases and Related Health Problems; p. 1. [Google Scholar]
- 7.Singh K., Prepageran N., Mohd Nor K. Nasal cavity myiasis presenting with preseptal cellulitis. Acta Oto-Laryngol. Case Rep. 2017;2(1):26–28. doi: 10.1080/23772484.2017.1291278. [DOI] [Google Scholar]
- 8.Arora S., Sharma J.K., Pippal S.K., Sethi Y., Yadav A. Clinical etiology of myiasis in ENT: a retrograde period - interval study. Braz. J. Otorhinolaryngol. 2009;75(3):356–361. doi: 10.1016/s1808-8694(15)30651-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ahm D., Delwar A., Professor A. Medical & Clinical Research Med Clin Res. Vol. 1. 2021. Corresponding author nasal myiasis: a neglect state; p. 4.www.medclinres.org [Google Scholar]
- 10.White Z.L., Chu M.W., Hood R.J., White Z. Nasal myiasis: a case report online exclusive. 2015;1(1):3. doi: 10.1177/014556131509400719. www.entjournal.com [DOI] [PubMed] [Google Scholar]
- 11.Serafim R.A., do Espírito Santo R.B., de Mello R.A.F., Collin S.M., Deps P.D. Case report: nasal myiasis in an elderly patient with atrophic rhinitis and facial sequelae of leprosy. Am. J. Trop. Med. Hyg. 2020;102(2):448–450. doi: 10.4269/ajtmh.19-0708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Francesconia F., Lupi O. Clinical Microbiology Reviews. 1(25) 2012. Myiasis; pp. 79–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Swain S., Sahu M., Baisakh M. Nasal myiasis in clinical practice. Apollo Med. 2018;15(3):128. doi: 10.4103/am.am_53_17. [DOI] [Google Scholar]
- 14.Neves Abdo, E., César Sette-Dias, A., Rômulo Comunian, C., Eduardo Assis Dutra, C., & Guimarães de Aguiar, E. (n.d.). Oral myiasis: a case report. 2006; 1(1): 3. [PubMed]
- 15.Katabi A., Aguirre M., Obeidat Y., Al-Ourani M., Assad S., Zeid F. Nasal myiasis in myasthenic crisis, a case report and literature review. Respir. Med. Case. Rep. 2020;1:31. doi: 10.1016/j.rmcr.2020.101212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lee Y.T., Chen T.L., Lin Y.C., Fung C.P., Cho W.L. Nosocomial nasal myiasis in an intubated patient. J. Chin. Med. Assoc. 2011;74(8):369–371. doi: 10.1016/j.jcma.2011.06.001. [DOI] [PubMed] [Google Scholar]
- 17.Sohrabi C., Mathew G., Maria N., Kerwan A., Franchi T., Agha R.A. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. Lond. Engl. 2023;109(5):1136. doi: 10.1097/JS9.0000000000000373. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data are included within the article.