

Abstract
Introduction
Advances in diagnostic technologies have resulted in an increase in patients with synchronous cancers. We report robotic hemicolectomy and robotic partial nephrectomy via a posterior approach.
Case presentation
A 72‐year‐old woman presented with synchronous ascending colon and right kidney cancers. We performed simultaneous robotic right hemicolectomy and robotic right partial nephrectomy. The renal tumor was located in a posterior and mid‐lower pole of the kidney, we positioned the ports similar to the retroperitoneal approach and to gain a confronting approach to the tumor.
Conclusion
Considering preoperative evaluations and intraoperative conditions comprehensively, it is essential to flexibly adapt to the appropriate surgical position and port arrangement to perform the surgery with consideration for oncological principles.
Keywords: colorectal cancer, hemicolectomy, heminephrectomy, renal cancers, robotic‐assisted surgery
Abbreviations & Acronyms
- RAPN
robotic‐assisted partial nephrectomy
- RCC
renal cell carcinoma
- RRC
robotic right hemicolectomy
Keynote message.
Simultaneous robotic surgery was performed for ascending colon cancer and right kidney cancer. The right hemicolectomy was performed via a transperitoneal approach, followed by the right partial nephrectomy was performed in the left lateral decubitus position which enabled to gain confronting approach to the tumor.
Introduction
When multiple cancers are found simultaneously, if possible, they are excised concurrently. However, it is necessary for specialized physicians to consider each case individually, determining the type of cancer, the appropriate approach for each, and whether minimally invasive surgery is feasible. We experienced a case of concurrent cancer involving ascending colon and right kidney. Since there are still few reports on performing minimally invasive robotic surgery for these cancers, we report RRC and RAPN via a posterior approach.
Case presentation
A 72‐year‐old woman, 149 cm in height and 64.5 kg in weight was presented with anemia. The colonoscopy revealed a tumor of the ascending colon pathologically diagnosed as adenocarcinoma. Staging chest and abdominal CT scan did not show any distant metastasis except a 45‐mm mass on the posterior and medial side and mid‐lower pole of the right kidney (Fig. 1). The renal mass showed heterogeneous contrast enhancement, consistent with clear cell RCC. We made a clinical diagnosis of ascending colon cancer cT3N0M0 and clear cell RCC cT1bN0M0 (RENAL nephrometry score: 2 + 2 + 3 + 2 = 9p).
Fig. 1.
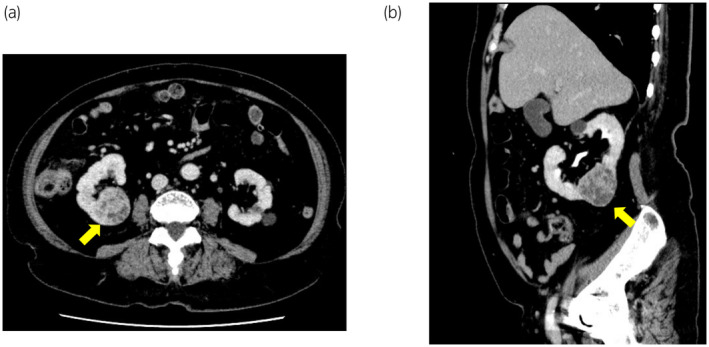
CT view of 45 mm mass on the posterior and medial side and mid‐lower pole of the right kidney: (a) axial view and (b) sagittal view.
The patient underwent simultaneous RRC and RAPN using da Vinci® Xi (Intuitive Surgical Inc., Sunnyvale, CA, USA). The patient was placed in lithotomy position with 15‐degree Trendelenburg and with 15‐degree left tilt. Port placements are shown in Fig. 2a. The robot was docked from the patient's right side (Fig. 2b) and a standard RRC was performed.
Fig. 2.
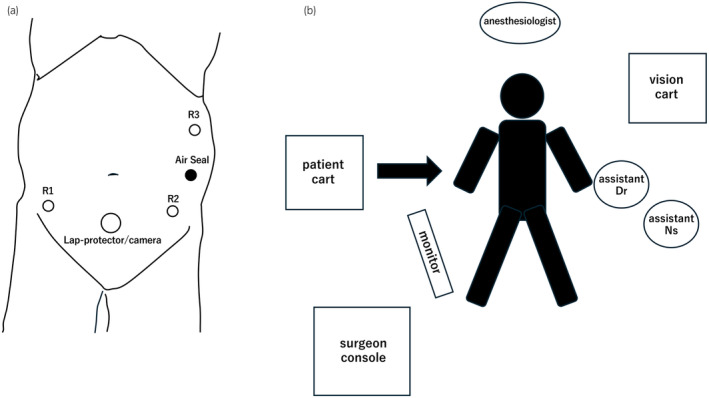
(a) Port placement for robotic right hemicolectomy with the patient in the lithotomy position. (b) Operating room setup and patient positioning for robotic right hemicolectomy.
The robot was undocked and the patient was placed in the complete left lateral decubitus position. Camera port was placed just below the costal margin in the mid axillary line and the retro‐renal surgical space was created using PDB Balloon dissector (Covidien Ltd., Mansfield, MA). The other ports were placed as shown in Fig. 3a. The robot was docked again from the patient's right side more cephalad than before (Fig. 3b). There were two renal arteries and two renal veins, all of which were taped off with vessel loop. The tumor location was confirmed with L43K drop‐in ultrasound probe (Fujifilm, Tokyo, Japan) and the surrounding Gerota's fascia was incised. All renal arteries and veins were clamped, the renal tumor was excised, and renorrhaphy was performed. The warm ischemic time was 22 min and 40 s. After confirming adequate hemostasis, the robot was undocked. A drain tube was placed below the liver and all the incisions were closed.
Fig. 3.
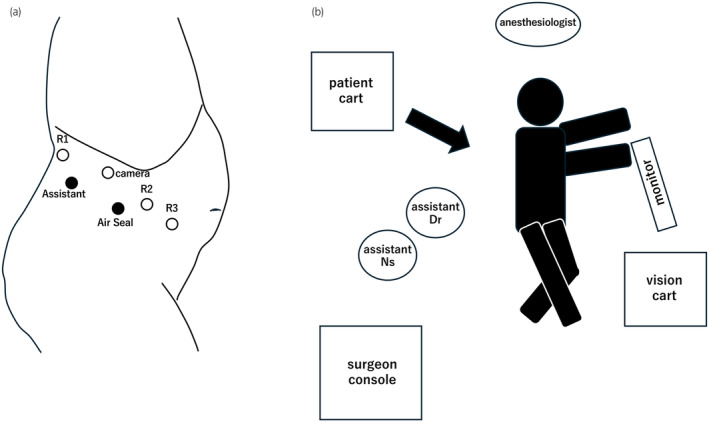
(a) Port placement for robotic partial nephrectomy with the patient in the left decubitus position. (b) Operating room setup and patient positioning for robotic right partial nephrectomy.
The total operative time was 539 min including docking and team switching: 221 min for right hemicolectomy and 235 min for partial nephrectomy. RRC and RAPN console times were 161 and 151 min, respectively. The estimated blood loss was 213 mL. No intraoperative complications were registered and the postoperative course was uneventful.
Discussion
Synchronous primary malignancies reported to represent 1% of cancer cases, 4% of which were concomitant colorectal cancer and renal cancer. 1 According to other report, among 103 patients who underwent colorectal surgery during that period, five cases of synchronous colorectal and renal carcinomas were detected (4.85%). 2 There are a few reports of simultaneous hemicolectomy and partial nephrectomy treated with full robotic surgery. 3 , 4 , 5 In this case, as the tumor was located on the same side as the ascending colon and right kidney, concerns about adhesions making subsequent surgery difficult arose during sequential surgery. Moreover, due to the urgency of both surgeries, simultaneous surgery was chosen.
There is debate about whether to perform colon or renal surgery first. In this case, we chose to perform right hemicolectomy first followed by partial nephrectomy. Similar to the report by Espín‐Basany et al., 5 who performed RRC and right transperitoneal RAPN for anterior lower pole tumor sharing same ports without changing position, we planned to assess the surgical field around the kidney after colon surgery without changing position to determine the optimal position, port arrangement, and approach for partial resection of the cT1b renal tumor. Upon assessment of the surgical field around the kidney after colon surgery, we decided to perform renal partial resection in the complete left lateral decubitus position.
In the standard transperitoneal anterior approach, the tumor was located in a dorsal and median portion, which was thought to make tumor resection and renorrhaphy difficult. Therefore, for the following reasons, we decided to position the ports similar to the retroperitoneal approach and to gain confronting approach to the tumor.
Due to the location of tumor, approaching the right kidney from posterior aspect allows to directly face the tumor, resulting in optimal visibility of the overall view during the resection and renorrhaphy.
Despite the disruption of right posterior retroperitoneum during colon resection, the remaining Gerota's fascia and connective tissues prevent the kidney from collapsing medially in the lateral position.
While there is concern about the kidney collapsing inward compared to the standard retroperitoneal approach, this is mitigated by the use of an extra arm to support the kidney.
Despite the posterior approach in this case, there was no limitation in the mobility of the forceps, and with the assistance of the extra arm, the kidney remained stable, allowing for the successful excision of the tumor and renal renorrhaphy. Additionally, the isolation of the renal arteries and veins performed prior to tumor excision could also be carried out in the same manner as the standard retroperitoneal approach.
The patient cart was undocked and rolled out once, but upon repositioning, it was rolled back in from the same side. When performing a right partial nephrectomy via a retroperitoneal approach, the patient cart usually docks from the left side of the patient. However, by effectively utilizing the boom function of the da Vinci Xi, docking can be performed from the right side of the patient in this case. Although the port configuration changed from colon resection, docking was possible by rotating the boom, allowing us to resume the surgery without rearranging the equipments within the operating room.
Conclusion
Depending on the patient's stature and tumor location, renal partial resection can be performed using the same position or ports as colon resection. However, considering preoperative evaluations and intraoperative conditions comprehensively, it is essential to flexibly adapt to the appropriate surgical position and port arrangement to perform the surgery with consideration for oncological principles.
Author contributions
Masaru Ishida: Writing – original draft. Toru Yamada: Writing – review and editing. Rei Takeuchi: Writing – review and editing. Yuta Jin: Writing – review and editing. Kaori Katsumata: Writing – review and editing. Takafumi Saito: Writing – review and editing. Masashi Arai: Writing – review and editing. Tansei Sanjo: Writing – review and editing. Tadatsugu Anno: Writing – review and editing. Tomohisa Egawa: Writing – review and editing.
Conflict of interest
The authors declare that they have no conflict of interest.
Approval of the research protocol by an Institutional Reviewer Board
Not applicable.
Informed consent
Informed consent was obtained from the patient for the publication of this case report.
Registry and the Registration No. of the study/trial
Not applicable.
Acknowledgments
None.
References
- 1. Aydiner A, Karadeniz A, Uygun K et al. Multiple primary neoplasms at asingle institution: differences between synchronous and metachronousneoplasms. Am J Clin Oncol 2000; 23: 364–370. [DOI] [PubMed] [Google Scholar]
- 2. Halak M, Hazzan D, Kovacs Z, Shiloni E. Synchronous colorectal and renal carcinomas: a noteworthy clinical entity. Report of five cases. Dis Colon Rectum 2000; 43: 1314–1315. [DOI] [PubMed] [Google Scholar]
- 3. Piccoli M, Pecchini F, Esposito S et al. First cases of combined full robotic partial nephrectomy and colorectal resections: results and new perspectives. Int J Med Robot 2020; 16: 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Sanmoto Y, Hosoi T, Kinuta S. Simultaneous total robotic right hemicolectomy and right partial nephrectomy. J Surg Case Rep 2023; 7: 1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Espín‐Basany E, Pellino G, Lorente GD. Robotic right hemicolectomy and partial nephrectomy for synchronous malignancies—a video vignette. Color Dis 2020; 22: 1770–1771. [DOI] [PubMed] [Google Scholar]