

Abstract
The activity of anti-CD19 chimerci antigen receptor (CAR) T-cell therapy in chronic lymphocytic leukemia (CLL) with Richter’s transformation (RT) to aggressive large B-cell lymphoma (LBCL) is largely unknown. In a multicenter retrospective study, we report the safety and efficacy of CAR T-cell therapy in patients with RT (N=30) compared to patients with aggressive B-cell lymphoma (N=283) and patients with transformed indolent non-Hodgkin lymphoma (iNHL) (N=141) between April 2016 and January 2023. Two-thirds of patients received prior therapy for CLL before RT and 89% of them received B-cell receptor and B-cell lymphoma 2 inhibitors. Toxicities of CAR T-cell therapy in RT were similar to other lymphomas, with no fatalities related to cytokine release syndrome or immune effector-cell associated neurotoxicity synderome. The 100-day overall response rate and complete response rates in patients with RT were 57% and 47%, respectively. With a median follow-up of 19 months, the median overall survival (OS) was 9.9 months in patients with RT compared to 18 months in de novo LBCL and not reached in patients with transformed iNHL. The OS at 12 months was 45% in patients with RT compared with 62% and 75% in patients with de novo LBCL and transformed iNHL, respectively. In a multivariate analysis, worse OS was associated with RT histology, elevated lactate dehydrogenase, and more prior lines of therapy. CAR T-cell therapy can salvage a proportion of patients with CLL and RT exposed to prior targeted agents; however, efficacy in RT is inferior compared to de novo LBCL and transformed iNHL.
Introduction
Advancements in drug therapies have greatly improved patient outcomes in chronic lymphocytic leukemia (CLL) in the last decade, and long-term responses are attained, even in those with high-risk disease features.1 Nevertheless, patients with progressive disease that is refractory to both B-cell receptor (BCR) and B-cell lymphoma 2 inhibitors (BCL2i) have limited options. Even more challenging are patients with disease transformation to an aggressive lymphoma, known as Richter transformation (RT). Patients with RT face a particularly grim prognosis, as traditional anthracycline-based combination chemoimmunotherapy yields short-lived responses and overall survival (OS) rates of less than 1 year.2,3 Despite the introduction of novel targeted agents, the outcome for patients previously exposed to Bruton’s tyrosine kinase (BTK) inhibitors remains discouraging.4 Allogeneic hematopoietic cell transplantation (allo-HCT) offers potential cure and long-term survival for some RT patients, with a 40% disease-free survival rate achieved in fit individuals following non-myeloablative allo-HCT.5 However, often due to advanced age, comorbidities and lack of disease control, only a fraction of patients may be eligible for allo-HCT.3,6
The advent of chimeric antigen receptor (CAR) T-cell therapy in B-cell malignancies was first used in patients with CLL more than a decade ago.7 Despite some long-lasting remissions reported, CAR T-cell therapy demonstrated only limited success in CLL, possibly due to intrinsic T-cell exhaustion and dysfunction.8,9 In contrast, CAR T-cell therapy has achieved a 2-year event-free survival (EFS) of 40% in early relapsed or refractory large B-cell lymphoma.10-12 Despite numerous clinical trials, including patients with B-cell lymphoma receiving CAR T-cell therapy, those with RT were excluded from prospective trials and the efficacy and safety of CAR T-cell therapy in RT is based on limited retrospective experience.13-15 Given a paucity of data in this space and in order to provide a potential new benchmark of outcomes in this unique cohort, we studied the outcomes of CAR T-cell therapy in patients with RT and compared the results with cohorts of de novo DLBCL and transformed iNHL.
Methods
Study design
This multi-center retrospective analysis included adult patients (age ≥18 years) with one of the following histologies: CLL with documented RT to DLBCL, DLBCL not otherwise specified (NOS), high-grade B-cell lymphoma (HGBL), and transformed iNHL which included transformed follicular lymphoma (tFL) and transformed marginal zone lymphoma (tMZL). All patients were treated between April 2016 and January 2023 at Memorial Sloan Kettering Cancer Center (MSKCC, New York), Hackensack University Medical Center at Hackensack Meridian Health (HMH, New Jersey), Rambam Health Care Campus (Haifa, Israel) and Sheba Medical Center (Ramat Gan, Israel) with one of the following CD19 CAR T-cell products: axicabtagene ciloleucel (axi-cel), tisagenlecleucel (tisa-cel), lisocabtagene maraleucel (liso-cel), or a point-of-care (POC) CD28-based product (given under a phase Ib/II clinical trial; clinicaltrials gov. identifier: NCT02772198).6,7 The POC CD28-based CAR T is a non-commercial, academic CAR T. The construct has single-chain fragment variable (scFv) derived from the mouse anti-CD19 hybridoma, FMC63, fused to intracellular domains from human CD28 and CD3-z, as previously published.16 Fresh product of 1x106 CAR+ cell/kg was delivered to patients after lymphodepletion with fludarabine and cyclophosphamide with a median turn-around time of 10 days from apheresis to end of manufacturing. In addition to comparable manufacturing efficiency, treatment efficacy, and toxicity profiles, studies have observed adverse events profiles similar to those of the commercial products.16-18 Patient data were captured in REDCap databases. The Institutional Review Boards of the participating institutions approved the study in accordance with the Declaration of Helsinki and all patients signed informed consent for treatment.
Definitions and endpoints
Response was assessed at the individual institutions according to the Lugano criteria using positron emission tomography-computed tomography (PET-CT) relative to the disease response before leukapheresis.19 Bulky disease was considered to be a tumor mass of more than 10 cm in diameter. The overall response rate (ORR) was defined as the proportion of patients who achieved a complete or partial response. Progression-free survival (PFS) was defined as the time from CAR T-cell infusion to either first documented progression or death. OS was defined as the time from cell infusion to the date of death. Cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) were graded according to the American Society for Transplantation and Cellular Therapy Consensus Grading.20 The primary end point was the rate of objective response, calculated as the combined rates of complete response and partial response. Secondary end points included the duration of response, PFS, OS and incidence of adverse events.
Statistical analysis
Categorical and continuous variables were described by frequency and percentage or median and range, respectively. Fisher’s exact and Kruskal-Wallis tests were used to study categorical and continuous variables, respectively. The median follow-up was calculated by the reverse Kaplan-Meier method. The Kaplan-Meier method was used for survival description. Univariable Cox regression models clustered by center were created to study clinical factors associated with OS and PFS. Relapse was evaluated using cumulative incidence analysis with a competing risk of death, as well as with univariable cause-specific Cox regression clustered by center. Univariable logistic regression was utilized to determine predictors of CR. The multivariable regression model included variables presenting P<0.1 in the univariable analysis. All P values were 2-sided, and P<0.05 was considered statistically significant. Data were analyzed using R (version 4.1.2).
Results
Patients and disease characteristics
A total of 454 patients with aggressive B-cell lymphoma (DLBCL NOS [85%], HGBL [13%]) were analyzed: 283 with de novo LBCL (62%), 141 with transformed iNHL (31%), and 30 with RT (7%). Among 270 patients with available cytogenetic data, 20% had double-hit or triple-hit LBCL. Patients with transformed iNHL included 105 patients (74%) with tFL and 36 patients (26%) with tMZL. When comparing patients with RT versus all other histologies, baseline patient characteristics were similar (Table 1). Among all patients, median age was 64 years (range, 20-86) and 63% were males. CAR T products used included axi-cel in 45% (N=206), tisa-cel in 24% (N=110), lliso-cel in 13% (N=58), and POC CD19 CAR T cell in 18% (N=80). Most patients with de novo DLBCL (N=124, 44%) and transformed iNHL (N=78, 55%) were treated with axi-cel and most patients with RT (N=16, 53%) were treated with POC CAR T-cell therapy. Most patients (N=308, 77%) had advanced-stage diseases and elevated lactate dehydrogenase (LDH) (N=233,55%), 16% (N=69) had bulky disease and 8% (N=35) had active central nervous system (CNS) involvement at apheresis. Sixty-eight percent of the patients (N=303) received up to three lines of therapy before apheresis, 21% (N=95) received four or five lines of therapy and 11% of patients (N=48) received more than six lines of therapy. Bridging therapy was administered to 266 (59%) patients. The median time from apheresis to CAR T infusion was 36 days (range, 10-377). Lymphodepletion included cyclophosphamide and fludarabine or bendamustine in 405 (89%) and 49 (11%) patients, respectively.
Chronic lymphocytic leukemia characteristics pretransformation
Thirty patients with CLL and RT from four medical centers were evaluated (Sheba N=16 [53%], MSKCC N=11 [37%], HMH N=2 [7%], Rambam N=1 [3%]). Patient characteristics are shown in Table 2. CLL adverse prognostic factors were available in a subset of patients and included: unmutated IGHV in four of seven (57%), complex karyotype in four of 12 (33%), del17p by fluorescence in situ hybridization in seven of 17 (41%), and TP53 mutation five of 12 (42%). Prior to RT, six of 16 patients (37%) had advanced-stage CLL (RAI stage 3/4), and 22 of 26 (85%) had hypogammaglobulinemia. In nine of 28 patients (32%), RT occurred without prior CLL-directed therapy. One patient (4%) presented with de novo RT. Eight of 28 patients (29%) were treated with three or more prior lines of therapy for CLL before RT. Among patients that were treated for CLL prior to RT 68% (19/28), pretransformation therapies included chemoimmunotherapy with fludarabine, cyclophosphamide, rituximab/ obinutuzumab (FCR/O) or bendamustine, rituximab (BR) in 58% (11/19), other chemotherapies 21% (4/19) and targeted therapies 89% (17/19) with BTKi 74% (14/19), phosphoinositide 3 kinase inhibitors (PI3Ki) 16% (3/19) and BCL2i 47% (9/19). Two patients (7%) received prior autologous-SCT and five of the patients (17%) consolidated with allo-HCT for CLL prior to transformation.
The Richter transformation cohort before CAR T-cell therapy (N=30)
The median age of the RT cohort before CAR T-cell therapy was 66 years; range, 44-78. Most patients were male 80% (24/30) and 43% (13/30) had Karnofsky performance status (KPS) ≥90. Most patients (80%; 22/27) had stage 3-4 disease at apheresis, and 32% (9/28) had primary refractory disease. Prior CNS involvement and active CNS involvement at apheresis were documented in 11% (3/28) and 7% (2/28), respectively, and 11% of patients (3/28) had bulky disease. The time from RT diagnosis to CAR T-cell therapy was 9 months (range, 2-13) compared to 15 months (range, 0-219) in patients with de novo LBCL and 14 months (range, 1-247) for patients with transformed iNHL. The median time from apheresis to CAR T-cell infusion was 30 days (range, 10-76) in patients with RT, 35 days (range, 10-377) in patients with de novo LBCL, and 39 days (range, 10-278) in patients with transformed iNHL. Patients with RT received a median of four lines of therapy (range, 2-15) before apheresis, including one (range, 0-8) for CLL before transformation and two (range, 0-7) after transformation directed to RT. Most patients were exposed to targeted therapies with BTKi 75% (21/28), PI3Ki 18% (5/28) and BCL2i 61% (17/28). Prior to CAR T-cell therapy, 17% (5/29) had allo-HCT, and 7% (2/29) had autologous-HCT. Eighteen patients with RT (60%) received bridging therapy, seven (23%) with local radiotherapy and 11 (37%) with systemic therapy including platinum-based chemotherpay (N=2), other systemic chemotherapy (N=1), BTKi (N=3), polatuzumab (N=2), lenalidomide (N=1) and two unknown. No patients received Pi3Ki or BCL2i-based therapy as bridging therapy. Bridging therapies administered to patients with RT were largely comparable to those administered in de novo LBCL and transformed iNHL, though exact comparisons were not feasible due to the low numbers and wide variety of therapeutic options. .
Outcomes
Efficacy
Response data were evaluable at day 100 for 440 patients, 271 of them with de novo LBCL, 139 with transformed iNHL, and 30 patients with RT. Patients with transformed iNHL had the highest ORR of 78% (N=110) followed by 68% (N=189) in patients with de novo LBCL and lowest response rate 57% (N=17) in patients with RT. Patients with transformed iNHL also had the highest proportion of CR with 62% (N=87) CR followed by 50% (N=140) in de novo LBCL and 40% (N=14) in RT (Figure 1). The median follow-up was 19.0 months (interquartile range [IQR], 7.2-32.9). The median PFS and OS for the entire cohort were 6.6 (95% confidence interval [CI]: 5.3-8.8) and 23 (95% CI: 17-not reached [NR]) months (Figure 2A, C), PFS and OS at 12 months were 40% (95% CI: 35-45) and 65% (95% CI: 60-70), respectively. At 24 months, PFS and OS were 33% (95% CI: 28-39) and 49% (95% CI: 43-55), respectively (Table 3). The median OS was NR in patients with transformed iNHL (95% CI: 26-NR), 18 months in de novo DLBCL (95% CI: 18-27), and 9.9 months (95% CI: 6.2-NR) in patients with RT (Figure 2B). OS rates at 12 and 24 months, respectively, for patients with transformed iNHL were 75% and 61% for patients with de novo LBCL, 62% and 44%, and for patients with RT 45% and 31% (Figure 2C). Thirty-five patients (8%) had active CNS involvement at time of lymphodepletion. Twenty four of them (69%) had de novo LBCL, nine patients (26%) had transformed iNHL and two patients (6%) had RT. Toxicity profile was similar to patients without CNS involvement, with severe CRS in 3% and severe neurotoxicity (ICANS ≥3) in six patients (17%). At 12 months of follow-up (IRQ, 5.62-127.55), median OS was 9.9 months (95% CI: 6.2-NR) and OS at 24 months was 31% 95% CI: 16-62).
Table 1.
Base line characteristics.

Table 2.
Characteristics of patients with chronic lymphocytic leukemia pretransformation.
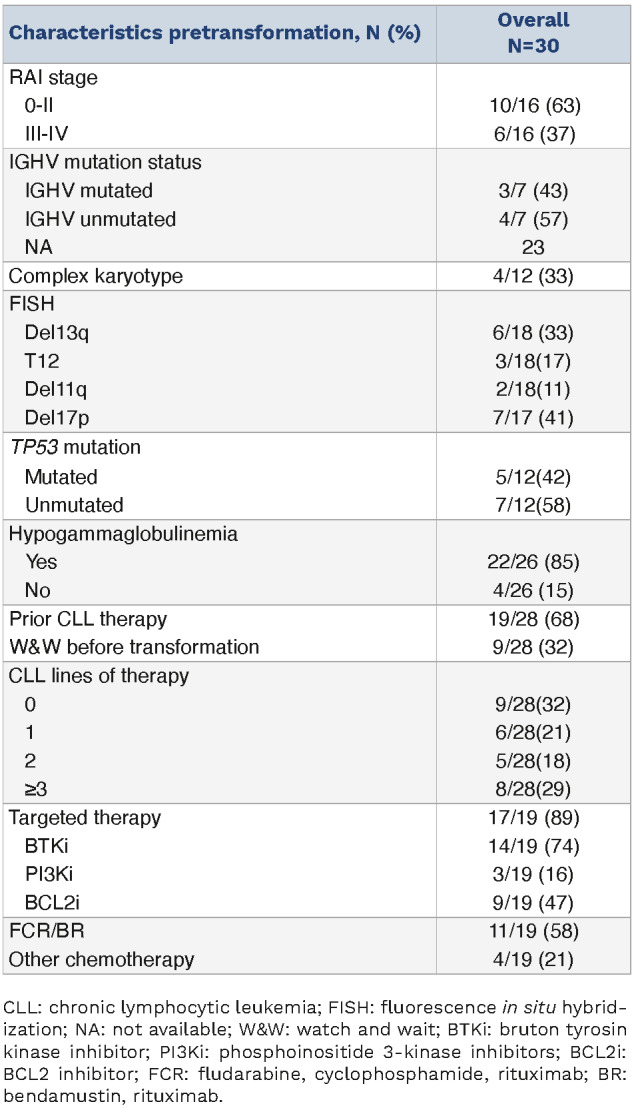
Figure 1.
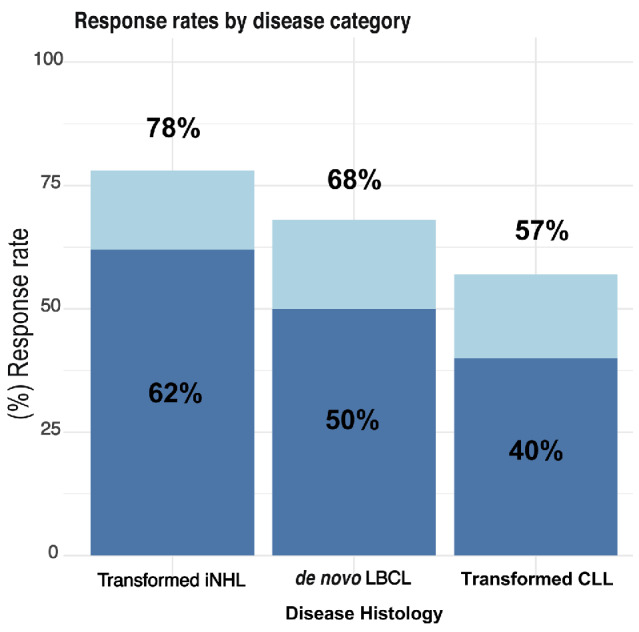
Overall response according to histology achieved at day 100. Overall response rate (ORR) P=0.071; complete response (CR) P=0.046. LBCL: large B-cell lymphoma; iNHL: low grade non-Hodgkin lymphoma; CLL: chronic lymphocytic leukemia.
In a multivariate analysis, more prior lines of therapy, high LDH, and the presence of RT were associated with shorter OS rates whereas, age and the CAR T-cell co-stimulatory domain were not associated with survival (Table 4). Compared to patients with de novo LBCL, relapse rates were lowest for transformed iNHL (hazard ratio [HR]=0.75, 95% CI: 0.71-0.8) and highest in patients with RT (HR=1.38, 95% CI: 1.17-1.61; P<0.001) (Figure 3). At 12 months and 24 months after administration of CAR T, 68% and 77% of patients with RT experienced disease relapse. Age and the number of lines of therapy before apheresis were not associated with the risk of relapse (Online Supplementary Table SA2) However, an elevated LDH before lymphodepletion was associated with a higher relapse rate (HR=1.73, 95% CI: 1.05-2.83; P=0.012) and use of a product with CD28 co-stimulatory domain was associated with a lower relapse rate (HR=0.71, 95% CI: 0.55-0.910; P=0.038). (Online Supplementary Table SA2) The only predictor of the failure to achieve CR by day 100 in multivariable analysis was elevated LDH (HR=0.32, 95% CI: 0.21-0.47; P<0.001) prior to lymphodepletion. An exploratory univariate analysis performed to identify factors for OS in patients with RT included age at CAR T-cell infusion, elevated LDH before apheresis, bridging BTKi exposure therapy, performance status, disease stage, and number of prior lines of therapy. The only factor associated with shorter OS was the receipt of ≥6 prior lines of therapy (HR=2.00, 95% CI: 1.25-3.19; P=0.002) (Online Supplementary Table S A3).
Figure 2.

Survival outcomes according to histology. (A) Overall survival (OS) of the cohort. (B) OS according to histology. (C) Progression-free survival (PFS) of the cohort. (D) PFS according to histology. De novo large B-cell lymphoma (LBCL): transformed low grade non-Hodgkin lymphoma (iNHL) and transformed chronic lymphocytic leukemia (CLL). CAR: chimeric antigen receptor; NR: not reached.
At the time of last follow-up, the disease statuses of 24 patients with RT were as follows: nine patients remained in remission, 15 relapsed with RT, two of them relapsed with CLL as well. Fifteen patients (50%) received further therapy, 12 for relapsed or residual disease, and five patients (17%) underwent allo-HCT. Of the five patients who underwent allo-HCT, two patients (7%) underwent consolidation in CR after CAR T-cell therapy. Of these two patients, one had disease progression after 25 months, and the other died from non-relapse mortality 2 months post allo-HCT. Three patients with progression of disease after CAR T received salvage therapy for relapse with bispecific antibodies and underwent allo-HCT in remission.
Nine of 26 evaluable patients with RT had CLL at apheresis (35%) based on non-active lymphadenopathy per positron-emission tomography/computed tomography (PET/CT) scan, of whom only one had lymphocytosis. All patients with CLL component responded, three with CR and five with PR, one was not evaluable. Though measurable residual disease was not tested, all patients had lymphopenia.
Table 3.
Safety and efficacy.

Only six patients (20%) with RT had clonality assessed. Five patients (80%) had clonally related RT. Three of them had progression of disease within 1-4.5 months after CAR T-cell infusion and two patients were alive and free of disease after 10 and 42 months.
Safety
Safety analysis was performed on 453 patients who received CD19 CAR T-cell therapy infusion (Table 3). CRS occurred in 76% (N=345) of patients, with severe CRS (grade ≥3) or in 9% (N=40). The median duration of CRS was 5 days (range, 0-356). ICANS was diagnosed in 28% (N=129) of patients and severe ICANS (grade ≥3) in 13% (N=48). There was one fatality related to ICANS. The median duration of ICANS was 5 days (range, 0-114). Steroids were administered to 31% (N=141) of the patients for ICANS and tocilizumab was administered to 31% (N=139) of patients with CRS. Prolonged neutropenia, at day 60 from apheresis, was higher in patients with RT (80%) compared to 66% in transformed iNHL and 58% in de novo LBCL. Twenty percent of patients with RT had thrombocytopenia at day 60 compared to 15% of patients with transfomed iNHL and de novo LBCL (Online Supplementary Figure S1). Thirty-eight patients (9%) were admitted to intensive care unit. Among patients with RT, toxicity grades were largely similar with no fatalities and one intensive care unit admission (3%) as shown in Table 3.
Discussion
Our study describes a cohort of 454 patients who underwent CAR T-cell therapy and focuses on 30 patients with RT in comparison with 283 patients with de novo LBCL and 141 patients with transformed iNHL.
CD19‐CAR T cells have revolutionized the treatment of B-cell lymphoid malignancies with a growing number of approved indications.21-26 Successful results of pivotal trials paved the way to utilize CAR T-cell therapy in earlier lines of therapy for LBCL and expanded the inclusions of patients with other entities, such as high-grade B cell lymphoma, mantle cell and Burkitt’s lymphomas. Histologic transformation of indolent lymphomas to aggressive subtypes were included in CAR T-cell trials but subgroup-specific data are limited. Given that for the same histology RT patients were excluded from initial pivotal CAR T-cell trials our study contributes to an area of unmet need.
Table 4.
Univariate and multivariate analysis to identify prognostic factors for overall survival.

Perhaps most significant, while rates of CRS and ICANS were similar, the response rates were smaller, and PFS and OS were shorter for patients with RT than those with transformed iNHL and de novo LBCL. Interestingly, among all patients, those with transformed iNHL had the best overall outcomes. The response rate for patients with de novo LBCL was lower than most other prospective CD19 CAR T-cell trials; however, in the current trial the LBCL cohort also included patients with high-risk disease (20% DHT). By comparison, a designated trial of axi-cel as part of first-line treatment in patients with high-risk LBCL with either double- or triple-hit lymphomas, those with positive interim PET or high-risk international prognostic index (IPI) demonstrated 80% CR. In addition, efficacy varies among published trials and no direct comparison is available between commercially available products.27,28
The information of CAR T-cell therapy in relapsed/refractory (R/R) transformed iNHL is available based on patients who participated in trials of R/R FL or LBCL; however, subgroup-specific data are limited.21,29 In a single-arm trial of CD19 CAR T in FL, six of 13 patients (46%) with heavily pretreated tFL achieved CR, and a median duration of response of 10.2 months. No relapses occurred after 15 months, with durable remissions observed for up to 39 months after CAR T infusion.26 A multicenter study (TRANSCEND NHL 001) of patients with R/R LBCL treated with lisocabtagene maraleucel included 78 patients (29%) with transformed iNHL, 60 patients with tFL and 18 patients with other transformed iNHL (10 with MZL and others with CLL/SLL). The ORR and CR in patients with tFL were 84% and 63%, respectively, and in patients with other transformed iNHL 61% and 39%, respectively. Patients with tFL achieved long duration of responses, but in other transformed iNHL histologies, the median duration of response lasted less than 3 months and OS 6.5 months.29
The rare occurrence and aggressive nature of RT also contribute to the limited data available on CD19 CAR T in RT. The potential use of CAR T-cell therapy in RT patients was initially reported in case reports and pilot studies of patients with R/R CLL that included limited number of patients with history of RT treated with commercial and POC CAR T-cell products.13,16,30-32 Recently, Kittai et al. reported on the largest cohort of patients with RT who received CD19-targeted CAR T in a retrospective international multicenter trial. Their trial included 69 patients that were treated with one of five commercial CAR T-cell products. Despite the limitation of intertrial comparison, our study share many similarities with their report having patient population with median age 64 years at CAR T-cell infusion, same proportion of major risk factors including Del17p/ TP53 mutation, high LDH, CNS involvement and SUVmax pre apheresis. In addition, in both trials patients were treated with four lines of therapy for CLL and RT, including the high proportion of patients that had received BTKi and BCL2i. The ORR was 63% compared to 57% in our RT cohort and CR was 46% versus 47%. Over longer median of follow-up of 24 months versus 19 months they found a median PFS of 4.7 months versus 6.6 months in our cohort and OS of 8.45 months versus 9.9 months. An estimated 2-year PFS was 29% versus 33%. In multivariate analysis, higher risk for disease progression increased with higher number lines of therapy and high LDH in both trials. Higher proliferative index, Ki67 and intensive care unit level were also risk factors for disease progression in their cohort. Despite these similarities, our trial has smaller number of patients and a proportion of patients recived POC non-commercial CAR T-cell product. Our study reinforces the efficacy and safety results and provides further information by comparing the outcomes of CAR T-cell therapy in patients with de novo LBCL and transformed iNHL.15
The most important prognostic factor in RT is clonal relationship to the underlying CLL. Other poor prognostic factors are TP53 mutations, poor patient performance status, elevated LDH, multiple prior lines of therapy, and failure to achieve CR to initial induction therapy for RT.33,34 Patients with CLL and prior exposure and/or refractoriness to novel agents have the shortest survival.35,36 Prior BTKi failure in RT patients may also adversely affect prognosis. In our study, 58% among those with information available (N=12) had TP53 mutations, and most patients were exposed to targeted therapies: 75% to BTKi and 69% to BCL2i. A significant predictor of inferior survival was exposure to six or more prior lines of therapy. Age, performance status, LDH prior to apheresis, and the type of CAR T co-stimulatory domain of the product did not affect survival. Notably, the response rate of our RT cohort was lower than reported in other cohorts of elderly patients with LBCL treated with CAR T cells.37,38
Our study is limited by its retrospective design and its heterogeneity related to the different programs of each center, including commercial with different co-stimulatory molecules versus POC CAR T with different co-stimulatory molecules and non-uniform construct production. In order to minimize the limitation of including POC non-comercial CAR T, we performed sensitivity analysis excluding patients that were treated with that construct and found no difference in safety or efficacy (Online Supplementary Tables S4, S5; Online Supplementary Figure S2). The relatively small number of patients in the RT cohort needs to be interpreted with great caution and requires confirmation in larger trials. Importantly, clonality studies were not available for most patients in the cohort. However, given a paucity of published data for patients with RT, our multicenter effort may provide a benchmark for future studies, and uniquely compared to the outcomes after CD19 CAR T cells with other more common histologies such as transformed iNHL and de novo DLBCL. Additionally, most patients were previously exposed to targeted therapies representing current standards of care. Response rates after CAR T-cell therapy in RT are modest and ultimately the disease relapses in most patients. Nonetheless, the response rates that we observed far exceed previous publications with chemoimmunotherapy (CIT) that generally result in lower response rates with CR rates of 20% and median survival of 6 to 12 months.39-43 Efforts to improve on the outcomes of CAR T-cell therapy in RT involve understanding why the poorer results in these patients. Efforts should focus on better understanding the disease biology and the reasons for the CAR T failures. One cause is the immune system dysfunction and T-cell exhaustion related to the course of pretransformation CLL and prior therapies. Additionally, better understanding of specific factors that affect the individual patient as TP53 and other molecular disruptions. Importantly, our work and others emphasize that CAR T-cell efficacy improves when used earlier in the course of the disease. Further work should be done on the effect of combining BTKi and other novel agents. Novel approaches with small cohorts are ongoing, some of which show promising short-term results, including CIT combined with targeted agents, non-covalent BTKi, checkpoint inhibitors, antibody-drug conjugates and bi-specific antibodies.44-49 Until more mature results and clinical evidence of these trials will be available, our data suggest that CAR T-cell therapy is valid therapeutic option for patients with RT. As CR in RT is essential but not sufficient for long term remission, even at the era of appealing new biologic agents efforts should be made to consolidate response with allo-HCT when feasible. Moreover, it is imperative to design unique clinical trials aimed at treating this patient population.
Figure 3.
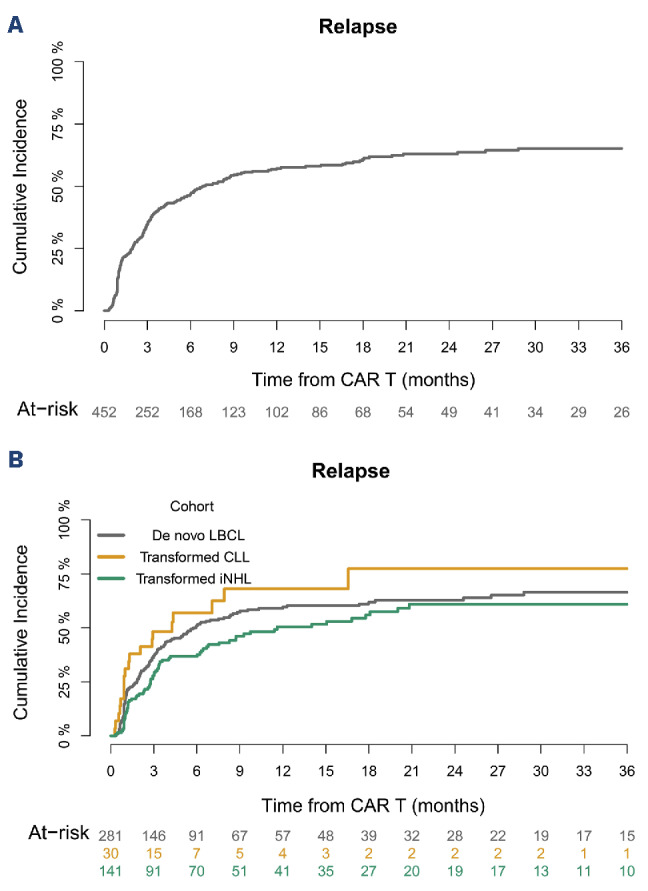
Cumulative relapse. Cumulative relapse (A) in the entire cohort and (B) according to histology. CAR: chimeric antigen receptor; LBCL: large B-cell lymphoma; iNHL: low grade non-Hodgkin lymphoma; CLL: chronic lymphocytic leukemia.
In conclusion, we observed objective responses to CAR T-cell therapy in more than half of patients with RT, higher than reported in previous CIT trials. Despite favorable initial responses in some, most patients with RT had early progression of disease. This suggests a potential window of opportunity to consider consolidative allo-HCT, though this strategy remains an open question. Earlier referral to specialized centers and rapid availability of CAR T cells are key factors in allowing for these treatment possibilities. Interestingly, the efficacy of CAR T-cell therapy in RT patients is not dependent of age, and it significantly decreases when given after multiple lines of therapy, suggesting that it should be considered earlier in these patients. Moreover, we await the results of prospective studies to further clarify the role of CD19 CAR T-cell therapy in this historically difficult-to-treat population.
Supplementary Material
Funding Statement
Funding: This research was supported in part by NIH/NCI Cancer Center Support Grant P30 CA008748. RS reports grant support from the NIH/NCI (K08CA282987). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Data-sharing statement
Research datasets for the present study are available from the corresponding author upon reasonable request.
References
- 1.Woyach JA, Barr PM, Kipps TJ, et al. Characteristics and clinical outcomes of patients with chronic lymphocytic leukemia/small lymphocytic lymphoma receiving Ibrutinib for >/=5 years in the RESONATE-2 study. Cancers (Basel). 2023;15(2):507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tsimberidou AM, O’Brien S, Khouri I, et al. Clinical outcomes and prognostic factors in patients with Richter’s syndrome treated with chemotherapy or chemoimmunotherapy with or without stem-cell transplantation. J Clin Oncol. 2006;24(15):2343-2351. [DOI] [PubMed] [Google Scholar]
- 3.Al-Sawaf O, Robrecht S, Bahlo J, et al. Richter transformation in chronic lymphocytic leukemia (CLL)-a pooled analysis of German CLL Study Group (GCLLSG) front line treatment trials. Leukemia. 2021;35(1):169-176. [DOI] [PubMed] [Google Scholar]
- 4.Elnair R, Ellithi M, Kallam A, Shostrom V, Bociek RG. Outcomes of Richter’s transformation of chronic lymphocytic leukemia/ small lymphocytic lymphoma (CLL/SLL): an analysis of the SEER database. Ann Hematol. 2021;100(10):2513-2519. [DOI] [PubMed] [Google Scholar]
- 5.Lahoud OB, Devlin SM, Maloy MA, et al. Reduced-intensity conditioning hematopoietic stem cell transplantation for chronic lymphocytic leukemia and Richter’s transformation. Blood Adv. 2021;5(14):2879-2889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Aulakh S, Reljic T, Yassine F, et al. Allogeneic hematopoietic cell transplantation is an effective treatment for patients with Richter syndrome: a systematic review and meta-analysis. Hematol Oncol Stem Cell Ther. 2021;14(1):33-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Porter DL, Levine BL, Kalos M, Bagg A, June CH. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia. N Engl J Med. 2011;365(8):725-733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Melenhorst JJ, Chen GM, Wang M, et al. Decade-long leukaemia remissions with persistence of CD4(+) CAR T cells. Nature. 2022;602(7897):503-509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Frey NV, Gill S, Hexner EO, et al. Long-term outcomes from a randomized dose optimization study of chimeric antigen receptor modified T cells in relapsed chronic lymphocytic leukemia. J Clin Oncol. 2020;38(25):2862-2871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med. 2022;386(7):640-654. [DOI] [PubMed] [Google Scholar]
- 11.Abramson JS, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel as second-line therapy for large B-cell lymphoma: primary analysis of the phase 3 TRANSFORM study. Blood. 2023;141(14):1675-1684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Perales MA, Anderson LD, Jain T, et al. Role of CD19 chimeric antigen receptor T cells in second-line large B cell lymphoma: lessons from phase 3 trials. An expert panel opinion from the American Society for Transplantation and Cellular Therapy. Transplant Cell Ther. 2022;28(9):546-559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kittai AS, Bond DA, William B, et al. Clinical activity of axicabtagene ciloleucel in adult patients with Richter syndrome. Blood Adv. 2020;4(19):4648-4652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Benjamini O, Shimoni A, Besser M, et al. Safety and efficacy of CD19-CAR T cells in Richter’s transformation after targeted therapy for chronic lymphocytic leukemia. Blood. 2020;136(Suppl 1):40. [Google Scholar]
- 15.Kittai AS, Bond D, Huang Y, et al. Anti-CD19 chimeric antigen receptor T-cell therapy for Richter transformation: an international, multicenter, retrospective study. J Clin Oncol. 2024;42(17):2071-2079. [DOI] [PubMed] [Google Scholar]
- 16.Kedmi M, Shouval R, Fried S, et al. Point-of-care anti-CD19 CAR T-cells for treatment of relapsed and refractory aggressive B-cell lymphoma. Transplant Cell Ther. 2022;28(5):251-257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fried S, Shkury E, Itzhaki O, et al. Point-of-care anti-CD19 chimeric antigen receptor T-cell therapy for relapsed/refractory follicular lymphoma. Leuk Lymphoma. 2023;64(12):1956-1963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fried S, Shouval R, Varda-Bloom N, et al. Point-of-care CAR T-cell therapy as salvage strategy for out-of-specification tisagenlecleucel. Leuk Lymphoma. 2022;63(14):3385-3393. [DOI] [PubMed] [Google Scholar]
- 19.Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059-3068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lee DW, Santomasso BD, Locke FL, et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. 2019;25(4):625-638. [DOI] [PubMed] [Google Scholar]
- 21.Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N Engl J Med. 2017;377(26):2531-2544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor T cells in refractory B-cell lymphomas. N Engl J Med. 2017;377(26):2545-2554. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Westin JR, Oluwole OO, Kersten MJ, et al. Survival with axicabtagene ciloleucel in large B-cell lymphoma. N Engl J Med. 2023;389(2):148-157. [DOI] [PubMed] [Google Scholar]
- 24.Kamdar M, Solomon SR, Arnason J, et al. Lisocabtagene maraleucel versus standard of care with salvage chemotherapy followed by autologous stem cell transplantation as second-line treatment in patients with relapsed or refractory large B-cell lymphoma (TRANSFORM): results from an interim analysis of an open-label, randomised, phase 3 trial. Lancet. 2022;399(10343):2294-2308. [DOI] [PubMed] [Google Scholar]
- 25.Fowler NH, Dickinson M, Dreyling M, et al. Tisagenlecleucel in adult relapsed or refractory follicular lymphoma: the phase 2 ELARA trial. Nat Med. 2022;28(2):325-332. [DOI] [PubMed] [Google Scholar]
- 26.Hirayama AV, Gauthier J, Hay KA, et al. High rate of durable complete remission in follicular lymphoma after CD19 CAR-T cell immunotherapy. Blood. 2019;134(7):636-640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Riedell PA, Hwang WT, Nastoupil LJ, et al. Patterns of use, outcomes, and resource utilization among recipients of commercial axicabtagene ciloleucel and tisagenlecleucel for relapsed/refractory aggressive B cell lymphomas. Transplant Cell Ther. 2022;28(10):669-676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bachy E, Le Gouill S, Di Blasi R, et al. A real-world comparison of tisagenlecleucel and axicabtagene ciloleucel CAR T cells in relapsed or refractory diffuse large B cell lymphoma. Nat Med. 2022;28(10):2145-2154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Abramson JS, Palomba ML, Gordon LI, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396(10254):839-852. [DOI] [PubMed] [Google Scholar]
- 30.Xia L, Wang Y, Li T, et al. The clinical study on treatment of CD19-directed chimeric antigen receptor-modified T cells in a case of refractory Richter syndrome. Cancer Med. 2019;8(6):2930-2941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Turtle CJ, Hay KA, Hanafi LA, et al. Durable molecular remissions in chronic lymphocytic leukemia treated with CD19-specific chimeric antigen receptor-modified T cells after failure of ibrutinib. J Clin Oncol. 2017;35(26):3010-3020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gauthier J, Hirayama AV, Purushe J, et al. Feasibility and efficacy of CD19-targeted CAR T cells with concurrent ibrutinib for CLL after ibrutinib failure. Blood. 2020;135(19):1650-1660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Rossi D, Spina V, Deambrogi C, et al. The genetics of Richter syndrome reveals disease heterogeneity and predicts survival after transformation. Blood. 2011;117(12):3391-3401. [DOI] [PubMed] [Google Scholar]
- 34.Wang Y, Tschautscher MA, Rabe KG, et al. Clinical characteristics and outcomes of Richter transformation: experience of 204 patients from a single center. Haematologica. 2020;105(3):765-773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Maddocks KJ, Ruppert AS, Lozanski G, et al. Etiology of ibrutinib therapy discontinuation and outcomes in patients with chronic lymphocytic leukemia. JAMA Oncol. 2015;1(1):80-87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Woyach JA, Ruppert AS, Guinn D, et al. BTKC481S-mediated resistance to ibrutinib in chronic lymphocytic leukemia. J Clin Oncol. 2017;35(13):1437-1443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Neelapu SS, Jacobson CA, Oluwole OO, et al. Outcomes of older patients in ZUMA-1, a pivotal study of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood. 2020;135(23):2106-2109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Zhang H, Liu M, Li Q, et al. Evaluation of the safety and efficacy of humanized anti-CD19 chimeric antigen receptor T-cell therapy in older patients with relapsed/refractory diffuse large B-cell lymphoma based on the comprehensive geriatric assessment system. Leuk Lymphoma. 2022;63(2):353-361. [DOI] [PubMed] [Google Scholar]
- 39.Langerbeins P, Busch R, Anheier N, et al. Poor efficacy and tolerability of R-CHOP in relapsed/refractory chronic lymphocytic leukemia and Richter transformation. Am J Hematol. 2014;89(12):E239-243. [DOI] [PubMed] [Google Scholar]
- 40.Dabaja BS, O’Brien SM, Kantarjian HM, et al. Fractionated cyclophosphamide, vincristine, liposomal daunorubicin (daunoXome), and dexamethasone (hyperCVXD) regimen in Richter’s syndrome. Leuk Lymphoma. 2001;42(3):329-337. [DOI] [PubMed] [Google Scholar]
- 41.Tsimberidou AM, Kantarjian HM, Cortes J, et al. Fractionated cyclophosphamide, vincristine, liposomal daunorubicin, and dexamethasone plus rituximab and granulocyte-macrophage-colony stimulating factor (GM-CSF) alternating with methotrexate and cytarabine plus rituximab and GM-CSF in patients with Richter syndrome or fludarabine-refractory chronic lymphocytic leukemia. Cancer. 2003;97(7):1711-1720. [DOI] [PubMed] [Google Scholar]
- 42.Rogers KA, Huang Y, Ruppert AS, et al. A single-institution retrospective cohort study of first-line R-EPOCH chemoimmunotherapy for Richter syndrome demonstrating complex chronic lymphocytic leukaemia karyotype as an adverse prognostic factor. Br J Haematol. 2018;180(2):259-266. [DOI] [PubMed] [Google Scholar]
- 43.Tsimberidou AM, Wierda WG, Wen S, et al. Phase I-II clinical trial of oxaliplatin, fludarabine, cytarabine, and rituximab therapy in aggressive relapsed/refractory chronic lymphocytic leukemia or Richter syndrome. Clin Lymphoma Myeloma Leuk. 2013;13(5):568-574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Jain N, Senapati J, Thakral B, et al. A phase 2 study of nivolumab combined with ibrutinib in patients with diffuse large B-cell Richter transformation of CLL. Blood Adv. 2023;7(10):1958-1966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Davids MS, Rogers KA, Tyekucheva S, et al. Venetoclax plus dose-adjusted R-EPOCH for Richter syndrome. Blood. 2022;139(5):686-689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Thompson PA, Jiang X, Banerjee P, et al. A phase two study of high dose blinatumomab in Richter’s syndrome. Leukemia. 2022;36(9):2228-2232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Vaisitti T, Arruga F, Vitale N, et al. ROR1 targeting with the antibody-drug conjugate VLS-101 is effective in Richter syndrome patient-derived xenograft mouse models. Blood. 2021;137(24):3365-3377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Wierda WG, Lewis DJ, Ghia P, et al. Efficacy of pirtobrutinib, a highly selective, non-covalent (reversible) BTK inhibitor in Richter transformation: results from the phase 1/2 BRUIN study. Blood. 2022;140(Supplement 1):846-849. [Google Scholar]
- 49.Kater AP, Ye JC, Sandoval-Sus J, et al. Subcutaneous epcoritamab in patients with Richter’s syndrome: early results from phase 1b/2 trial (EPCORE CLL-1). Blood. 2022;140(Suppl 1):850-851. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Research datasets for the present study are available from the corresponding author upon reasonable request.