

Abstract
Background
It is important to assess the quality of fundamental movements, to discover deficits, evaluate mobility, balance, and stability, and identify movement dysfunction and asymmetries. However, little research has been performed on the assessment of fundamental movements with bodybuilders.
Purpose
The purpose of this research was to examine the quality of professional and amateur bodybuilders’ functional movements and the quality of the back squat performance. A secondary purpose was to discern whether greater experience in bodybuilding was associated with better scores on the back squat assessement (BSA).
Study design
Cross-Sectional Cohort
Methods
Twenty-six athletes were recruited to participate. The group of professional bodybuilders consisted of five men and six women, a total of 11 athletes. The group of amateur bodybuilders consisted of seven men and eight women, a total of 15 athletes. The Functional Movement Screen™ (FMS™) was used to assess the seven included fundamental patterns that evaluate an individual’s neuromuscular control, mobility, balance, and stability. The BSA was used to assess the quality of movement, dysfunction, deficit, or compensation during the squat exercise. Statistical analyses applied non-parametric tests (Wilcoxon, Mann-Whitney U, and Friedman’s) for dependent and independent samples, with significance set at p<0.05, and the Spearman correlation coefficient and Chi-square test were used to assess relationships between quantitative and qualitative variables.
Results
Overall, athletes with a higher total FMS™ score performed better on the BSA as well. The professional athletes scored 2.58 points higher than the amateurs on total FMS™ scores (p<0.001).
Professional athletes scored better on the BSA than amateurs (p<0.001). A statistically significant, positive moderate correlation was revealed between the FMS™ total score and the squat total score (r=0.68; p=0.005).
Conclusions
A higher FMS™ score in bodybuilders is associated with a higher BSA score. Professional bodybuilders have higher FMS™ scores and higher BSA scores than amateurs. Greater experience in bodybuilding is associated with the compliance with several BSA criteria: trunk position, frontal knee alignment, tibial translation angle, foot position in all three back squat variations with different external loads, and descent with the training weight.
Level of Evidence
3b
Keywords: Functional Movement Screen, bodybuilding, back squat assessment, back squat performance, fundamental movements.
INTRODUCTION
The competence of fundamental movements may relate to safe participation in physical activities and reduction of the risk of injuries. Development and training of these movements should be essential elements in sports,1,2 e.g., in bodybuilding. Bodybuilders perform many exercises/movements consistently,3 and the squat is one of the most important core movements that contributes to the enhancement athletic performance,1 and is widely used by amateur and professional athletes. The back squat recruits most of the major muscles of the lower body, including the quadriceps, hamstrings, glutes, and calves, while also engaging the trunk muscles, such as the abdominals and lower back, to ensure coordinated timing and activation of all muscles involved in the movement.1,4 The dynamics of the squat exercise under different circumstances have been thoroughly investigated in the past.4 For instance, Kristiansen et al.4 explored the squat of skilled weightlifting athletes and their inter- and intra-individual variability while performing this exercise, and Fry et. al.5 examined the effect of knee position on hip and knee torques during the back squat, while Escamilla et al.6 explored biomechanical parameters while performing the back squat with varying stance widths, and Swinton et. al.7 compared the biomechanics of the box squat, traditional squat, and powerlifting squat.
To further assess and identify biomechanical movement deficiencies, Myer and colleagues proposed the Back Squat Assessment (BSA).1,8 This screening tool allows for evaluation of an athlete’s strength, mobility, and neuromuscular control.1,9–13 Another popular screening tool used in sports is the Functional Movement Screen™ (FMS™).14,15 The FMS™ assesses seven distinct fundamental patterns, to identify functional movement deficiencies, asymmetry, and compensatory mechanisms, and to evaluate neuromuscular control, mobility, balance, and stability.16–18 Both the FMS™ and BSA screening tools offer simple methods for the evaluation of movement.
The purpose of this research was to examine the quality of professional and amateur bodybuilders’ functional movements and the quality of the back squat performance. A secondary purpose was to discern whether greater experience in bodybuilding was associated with better scores on the BSA. It was hypothesized that professional bodybuilders would demonstrate higher back squat and FMS™ scores, and would squat closer to the BSA standard, as professionals have more experience in bodybuilding than amateurs.
METHODS AND MATERIALS
The permission of the Center for Bioethics (No. BEC-SR(M)-197) was obtained to conduct the study. From October 8, 2020 to November 10, 2020 athletes from four Lithuanian cities participated in the study.19
Subjects
Twenty-six bodybuilders who were between 20 and 35 years old were recruited to participate in the study as shown in Table 1. Athletes were divided into two groups: professionals and amateurs as indicated in.
Table 1. List of criteria for the selection, inclusion, and exclusion of athletes, and the recruitment method of the study.
| Recruitment method | Selection criteria | Inclusion criteria | Exclusion criteria |
|---|---|---|---|
| Official invitation to participate in the study by the Lithuanian Fitness and Bodybuilding Federation | Time since the last competition | Less than 3 years prior | More than 3 years prior |
| Age | Between 18 and 35 years old | Younger than 18 and older than 35 years old | |
| Injuries | No injuries and/or conditions that could affect the study | Had injuries and/or conditions that may have affected the study | |
| Participation in competitions | Participation in International Fitness and Bodybuilding Federation (IFBB) competitions | Participation in other than IFBB federation competitions |
Methods
Functional Movement Screen™ (FMS™)
The FMS™ is widely used in sports practice to assess foundational movement patterns. Seven functional movements are evaluated during the test, including the deep squat, in-line lunge, hurdle step, active straight leg raise and shoulder mobility, trunk stability push-up, and rotary stability. After performing these movements, the athletes also had to perform three clearing tests, which included spinal flexion, extension, and a shoulder test.14,17 Each of the seven functional movements was performed three times, and the best performance was scored.14,17,20 All of the movement patterns were scored separately from 0 to 3 points. If the athlete felt pain in any part of the body, 0 points were given. A score of 1 was given when the athlete was unable to fully complete the movement, and a score of 2 was given when the athlete was able to complete the movement but performed the task with compensation of adjacent regions. If the athlete was able to perform the movement without a visible deficit or compensation, they were given a maximum rating of 3 points.14,20 If the athlete received a different number of points while performing a movement on both sides of the body, the lower score of the two was used for the total FMS™ score. The sum of the athlete’s performance scores for all seven movement patterns resulted in a total FMS™ score. The highest possible total FMS™ score is 21.14
The Back Squat Assessment (BSA)
The BSA is used to assess the quality of movement, dysfunction, deficit, or compensation during the back squat exercise. After identifying the deficiencies during the fundamental movement pattern of the back squat, clinicians can prescribe corrective exercises1 and reduce existing asymmetries, deficits, and compensations, which can affect the quality of training and athletes’ performances. In total, the BSA screening tool has 10 criteria. During the back squat performance, the clinician assesses three movement mechanics criteria, three upper body criteria, and four lower body criteria. When evaluating the movement mechanics, attention is paid to the recruitment, timing, and coordination; when evaluating the criteria of descent, the depth, and ascent are observed. When assessing the upper body, the head position, thoracic position, and torso position are monitored. And finally, when assessing the lower body, the hip position, frontal plane knee alignment, tibial translation angle, and foot position are inspected.1 Every professional and amateur athlete performed three back squats. The back squats were performed with different external loads: first with no weight, then with an Olympic bar weighing 20 kilograms, and finally with which the weight that the athlete was currently training. Each of the ten criteria was scored as either 0 or 1. If the criterion was fulfilled correctly, it was scored as 1 point. If the criterion did not meet the standard, the athlete was given 0 points. There were three back squat attempts. The repetition with the highest score was evaluated. A maximum score of 10 indicated the best back squat performance.19 A total back squat score was calculated by adding and averaging the scores for the weightless back squat, the back squat with the Olympic bar, and the back squat with which the weight that the athlete was currently training. Back squat performance trials were recorded from two angles. One of the two tripods (BRAUN Lightweight BLT 100S) was placed in front of the athlete and captured the frontal plane, while the second tripod was set to the right side of the athlete and captured performance from the sagittal plane. Two iPhone X devices were placed on the tripods. In order to start recording the video in the two planes with two devices at the same time, two remote controls were used. A certified physiotherapist performed the evaluation of the quality of the back squat.
Figure 1. Squat with different load intensities in the sagittal plane at the end of the movement. On the left side (A) - without weight, in the middle (B) - with the Olympic bar, and on the right side (C) with the training weight.

Additional Considerations for the Functional Movement Screen™ and Back Squat Assessment
It is important for conditioning experts and athletic health care professionals to ensure precise estimations of variables to reduce uncertainty and avoid incorrect conclusions in the monitoring process.18 It is known that tester’s experience can affect scoring of screening tests. For that reason, the BSA screening tool was chosen to reduce subjectivity as much as possible, and the use of structured, detailed, verbal instructions assist in promoting inter-rater reliability. Since the FMS™ scoring is standardized, clinicians across varying professions can use this tool,15,21 and to reduce error in scoring, the professional should have been instructed in and be familiar with the screening tool (>100 trials).18 Despite the known shortcomings of the tests, the BSA and FMS™ were chosen because they are easy to use, low-cost, time-efficient, and widely accessible to personal trainers, physical therapists, and other practitioners.
Ten Criteria of the Back Squat Assessment
Head position. For the athlete to meet the first criterion, their head must maintain a neutral alignment, which is in a slight physiological extension, and the neck is in line with the torso.1 It is equally important to pay attention to the athlete’s gaze. The gaze should be directed straight or slightly above the midline (Figure 2, criterion 1).1,22 The athlete should avoid placing their head too far forward or backwards, and tilting it to either side.1,23
Figure 2. Ten back squat criteria: on the left side in a sagittal plane (A) 1 – head position and gaze direction; 2 – thoracic position; 3 – trunk position; 6 – tibial translation angle; 7 – foot position; 9 – depth; on the right side in a frontal plane (B) 4 – hip position; 5 – frontal knee alignment; 7 – foot position; 8 – ascent; 10 – descent.

Thoracic position. The thoracic spine should be vertical during the entire back squat movement (Figure 2, criterion 2).1,24 The glenohumeral joint should be externally rotated, in a slightly depressed position, and the forearms in line with the torso help to keep the thoracic spine straight. The athlete’s scapulas must be in a depressed and retracted position.1
Trunk position. It is necessary that the lumbar spine maintains a neutral, slightly lordotic position while keeping the core stable throughout the squat (Figure 2, criterion 3).1 A mistake that should be avoided is excessive forward lean of the trunk because it increases the shear forces in the lumbar region.1,25 The correct position of the trunk is ensured by the presence of the trunk and tibia in parallel alignment when viewed from the side (Figure 2, criterion 6).1
Hip position. Throughout the exercise, the position of the hips should be symmetrical (Figure 2, criterion 4),1,23 malpositioning can be seen when one is higher or lower than the other, or rotated to one side or the other. The incorrect position of the hips can also be visualized by the non-horizontal and inclined position of the barbell when viewed from the front. The position of the pelvis is equally important, i.e., it must also remain in a neutral, anterior pelvic tilt position throughout the squat. Athletes often break this rule by demonstrating a posterior pelvic tilt or so-called “butt wink” at the end of the descent phase.1
Frontal plane knee alignment. Throughout the movement, the hip, knee, and ankle joints must remain in one vertical line when viewed from the front (Figure 2, criterion 5), and the knee joint with the tibia should be perpendicular to the floor. A knee valgus position that occurs when the knee joint and tibia cross a vertical line inward, and a knee varus position, that occurs when the knee joint and tibia cross a vertical line outward, are considered deficits.1,10
Tibial translation angle. The tibial translation angle can be greater or lesser depending on the ratio of the length of the femur to the torso of the athlete. However, regardless of body composition, it is recommended that the angle of the tibia is parallel with the angle of the trunk when viewed from the side (Figure 2, criterion 3, 6).1
Foot position. The feet are supposed to be tightly placed on the ground throughout the entire back squat motion. The feet tilting inwards, outwards, or lifting of the heel or toes off the ground are considered a deficit (Figure 2, criterion 7).1,24
Descent. This phase should begin with the hip hinge.1,26 One of the criteria that determines that an athlete performs a descent well is maintaining the same distance between the shoulders and hips during the movement. The tempo should be at least 2:1, meaning the descent should be slower than the ascent due to gravity assistance when descending. A failure to comply with this criterion is considered when athletes descend too quickly, unevenly, haphazardly, and without smoothness.1
Depth. The recommended depth is reached when the athlete descends until the upper part of the thighs is perpendicular to the floor (Figure 2, criterion 9).1,23 One of the main mistakes athletes make is incomplete squats that lack required depth.1
Ascent. Like the descent phase, the ascent should start from the hips. When performing a reverse hip hinge, the hips and shoulders should go up at an equal speed, maintaining the same distance throughout the entire phase.1
Statistical Analysis
IBM SPSS 21.0 software was used to assess the research data. Due to the small sample sizes in the study, non-parametric criteria were chosen. The Wilcoxon test was used to compare two dependent samples, and the Mann-Whitney U test was used to compare two independent samples. To equate three dependent samples, Friedman’s test was selected. Quantitative data are represented as mean () and standard deviation (± SD) – ( ± SD). Qualitative data are presented in absolute and relative frequencies. To estimate the relationship between two quantitative variables, the Spearman correlation coefficient was computed. The Chi-square (χ2) test analyzed qualitative variables. The differences at p<0.05 were considered statistically significant.
RESULTS
The study involved 26 athletes. The group of professional bodybuilders consisted of five men and six women, a total of 11 athletes. The group of amateur bodybuilders consisted of seven men and eight women, a total of 15 athletes. The number of professional and amateur athletes in the study was not statistically different (p=0.557), nor was the number of males and females among the amateurs (p=1) and professionals (p=1). The sports experience of amateur athletes in bodybuilding was 5.33 ± 4.62 years, and the sports experience of professional athletes in bodybuilding was 11.27 ± 4.54 years. The comparison of these two groups of athletes revealed that the years of experience in this sport were statistically significantly different (U=21.5; p<0.001), with the professionals having more experience in bodybuilding than the amateurs.
In the process of analyzing all bodybuilders, regardless of their experience, it was established that the participants with a higher total FMS™ score performed better on the BSA as well. A statistically significant, positive, and moderate correlation was revealed between the FMS™ total score and the BSA total score (r=0.68; p=0.005).
While evaluating the total FMS™ score between the groups, it was found that more experienced professional athletes scored 2.58 points higher than less experienced amateurs. A statistically evident difference (U=11.5; p<0.001) was found while comparing the results of FMS™ between amateur and professional bodybuilders (Figure 3).
Figure 3. Comparison of the FMS™ results between amateur and professional bodybuilders.

*-p<0.001
The professional athletes scored 8.64 ± 1.01 points on the BSA during the weightless back squat, while the amateurs scored 6.27 ± 0.96 points, which was statistically significantly different (U=6.5; p<0.001). The amateurs with the Olympic bar scored 6.07 ± 0.88 points, and the professionals scored 8.64 ± 1.03 points, which was also significantly different (U=5; p<0.001). Finally, using the training weight, the amateurs scored 5.93 ± 1.1 points while the professionals scored 8.82 ± 0.98, again, significantly different (U=4; p<0.001).
A statistically significant difference was found within the amateur’s group (χ2(2)=7.6; p=0.022) when comparing the back squat performance without weight, the squat with the Olympic bar, and the squat with the training weight. Post hoc analyses demonstrated that only a statistically significant result when comparing the performance without weight and squat performance with the training weight (Z= -2.236; p=0.031), while no statistically significant differences were revealed between the squat performance without weight and with the Olympic bar (Z= -1.732; p=0.125), or the squat performance with the Olympic bar and with the training weight (Z= -1.414; p=0.250). Comparing professionals’ weightless back squat, back squat with an Olympic bar, and using training weight, no statistically significant differences were found (χ2(2)=4; p=0.135).
A detailed analysis of the compliance with the criteria during the performance of the back squat between the amateur and professional bodybuilders revealed that the athletes equally performed the following criteria while squatting without weight: head position (p=0.218), which was met by 80% of the amateurs and 54.5% of the professionals; thoracic position, which was met by 80% of the amateurs and 72.7% of the professionals (p=1); hip position, which was met by 86.7% of the amateurs and all of the professionals (p=0.492); descent which was met by 66.7% of the amateurs and 90.9% of the professionals (p=0.197); depth, which was met by 80% of the amateurs and 81.8% of the professionals (p=1); ascent, which was met by 60% of the amateurs and by 81.8% of the professionals (p=0.395). During the squat with the Olympic bar, the athletes also complied with the following criteria equally: head position, which was met by 80% of the amateurs and 54.4% of the professionals (p=0.218); thoracic position, which was met by 80% of the amateurs and 72.7% of the professionals (p=1); hip position, which was met by 86.7% of the amateurs and all of the professionals (p=0.492); descent, which was met by 60% of the amateurs and 90% of the professionals (p=0.178); depth, which was met by 73.3% of the amateurs and 81.8% of the professionals (p=1); ascent, which was met by 53.3% of the amateurs and 81.8% of the professionals (p=0.217). Finally, during the squat with a training weight, the athletes also equally performed the following criteria: head position, which was met by 80% of the amateurs and 54.5% of the professionals (p=0.218); thoracic position, which was met by 80% of the amateurs and 72.7% of the professionals (p=1); hip position, which was met by 86.7% of the amateurs and all of the professionals (p=0.492); depth, which was met by 66.7% of the amateurs and 90.9% all of the professionals (p=0.197), and ascent, which was met by 53.3% of the amateurs and 81.8% of the professionals (p=0.217).
Further analysis of the results revealed that during the squat without weight the following criteria were performed differently between the amateurs and the professionals: trunk position (p=0.005), frontal plane knee alignment (p=0.024), tibial translation angle (χ2(1)=8.11; p=0.004), and foot position (p=0.010) (Figure 4). The same results were obtained during the squat with the Olympic bar, i.e., the professional and amateur athletes performed the following criteria differently: trunk position (p=0.005), frontal plane knee alignment (p=0.024), tibial translation angle (χ2(1)=8.11; p=0.004), foot position (p=0.010) (Figure 4). Both groups of athletes during the squat with a training weight also fulfilled the following criteria contrastly: trunk position (p=0.005), frontal plane knee alignment (p=0.024), tibial translation angle (χ2(1)=8.11; p=0.004), foot position (p=0.010), and descent (p=0.010) (Figure 4).
Figure 4. The distribution of the squat criteria not met by the amateurs and the professionals.
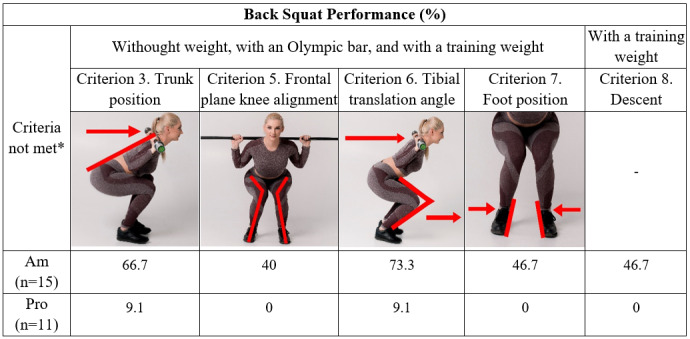
Am – amateurs
Pro – professionals
*Indicates significant difference at p<0.05
DISCUSSION
According to Wang et al.27 and Vehrs et al.,16 the FMS™ method is used to assess the quality of principal movements, to discover deficits, evaluate mobility, balance, and stability, and to identify movement disorganization, as well as asymmetries in athletes of different sports. However, much less research has been done on this topic in the area of bodybuilding.
The first aim of this study was to assess the links between the quality of functional movements and the quality of back squat performance in bodybuilders. It is already known that higher FMS™ scores are associated with higher lower extremity strength in professional soccer players,28,29 and that a strong association exists between flexibility and the capacity of movement that is observed.29,30 Equally important is the link between morphology, trunk strength, and the quality of movement patterns.29,31,32 Thus, in general the findings of this study indicate that regardless of experience, the bodybuilders who got higher total FMS™ scores demonstrated higher rates of the back squat performances as well (r=0.68; p=0.005). These findings suggest that as an athlete’s FMS™ score increases, their squat score also improves. Therefore, it can be assumed that athletes with a higher FMS™ score perform the back squat with higher quality.
The second aim of this study was to measure the quality of the functional movements as scored by the FMS™ between amateur and professional bodybuilders. It was found that the less experienced amateur athletes scored 15.87 ± 1.3 points and more experienced professional athletes scored 18.45 ± 1.13 points, which was statistically significantly different (U=11.5; p<0.001). The higher FMS™ scores observed in professionals may suggest that they have better neuromuscular control, balance, postural stability, and functional mobility, although each of these specific constructs were not measured. Tafuri et al.,33 analyzed FMS™ outcomes among CrossFitters, weightlifters, and amateur bodybuilders, finding that CrossFitters scored 15.2 ± 1.7 points, weightlifters scored 14.8 ± 2 points, and amateur bodybuilders scored 14.2 ± 1.9 points, and that all three groups of athletes results were not statistically different (F=2.28; p=0.10). This suggests that the level of skill and experience play an important role, because in the current study the professionals had more experience in bodybuilding than the amateurs did (U=21.5; p<0.001), while in the study of Tafuri et al.,33 CrossFitters, weightlifters, and amateur bodybuilders had experience that was not significantly different (p=0.15). Despite the current study analyzing the total FMS™ score, Vehrs’ et al.16 have suggested that it is valuable to pay attention to scores on individual screening tests, deficits, asymmetry, compensations or other deviations from the standard of movement patterns and their possible causes. Such an approach could help athletes not just to understand their strengths and weaknesses and also how to evolve or correct them.
The third aim of this study was to compare amateur and professional bodybuilders’ quality of the back squat performance with different intensities of load between groups and within groups. The comparison of the results between the groups revealed that more experienced professional bodybuilders meet more BSA criteria while performing the back squat than less experienced amateurs did in all three back squat variations (weightless, with an Olympic bar, and with a training weight). These results suggest that amateur bodybuilders who include the back squat exercise in their daily training routine and participate in international competitions still lack the quality while performing the back squat. To perform the squat qualitatively, i.e. meeting the back squat criteria requires time and experience. This is an ongoing process, which cannot be simplified and reached easily with 100 percent quality. In line with this, a comparison of the results within the groups revealed that amateurs performed the squat differently from professionals, with amateurs showing varying quality in their back squats. In contrast, the professional athletes performed the back squat with consistent quality, regardless of the additional weight. The results suggest that the back squat, especially with the additional loads, should be supervised by the clinicians, physical therapists or personal trainers more intentionally. While squatting with a heavier weight, and not meeting BSA criteria, bodybuilders may compromise quality even more, which can put athletes at a higher risk for injuries or chronic conditions. A similar focus on the back squat can be found in the study by Kristiansen et al.,4 which explored the variability in performance among skilled weightlifters. Their results demonstrated that experienced weightlifting athletes showed evident inter- and intra-individual variability during successfully performed back squats.4 It is possible that the different results between the professional bodybuilders in the current study and the experienced weightlifters in the study by Kristiansen et al.4 exists due to the small sample size in the current study. Even though the authors’ utilized mathematical statistical methods to minimize the influence of sample size to the findings, this remains a limiting factor of this study. Nevertheless, it should be pointed out that the training goals and characteristics of athletes in bodybuilding and weightlifting are also distinct. Bodybuilders are ranked on aesthetics, and their accomplishments depend on the symmetry, size, physical presentation, depth, and definition of the muscles,34–36 while weightlifters’ achievements depend on characteristics such as explosive power, speed, and strength.37–39 Also, it must be noted that prior to the evaluation the authors’ were unable to monitor bodybuilders’ training load, differences in training method, volume, and frequency, and these types of data can enrich further studies.
Lastly, the fourth aim of this study was to find out whether more experience in bodybuilding is associated with meeting the BSA criteria. After analyzing the athletes’ back squat performance, it was found that less experienced amateurs and more experienced professionals performed some criteria equally, and some criteria differently. The following criteria were met equally and are not associated with compliance to the BSA: head position, thoracic position, hip position, depth, ascent in all three back squat variations with different external loads, and descent without weight or with the Olympic bar, as both amateur and professional athletes met these criteria equally. At the same time, the criteria that were different among athletes were the following: trunk position, frontal knee alignment, tibial translation angle, foot position in all three back squat variations with different external loads, and descent with the training weight. These results indicate that greater experience in bodybuilding is related to meeting the mentioned BSA criteria, as professionals performed back squats better, overall, than amateurs did. Naturally, these criteria are interdependent, and often, when one of them is not met, deficits can also be observed in adjacent regions as well. The correct position of the trunk is ensured by the presence of the trunk and tibia in parallel when viewed from the side, but these guidelines require correct feet and knee joint positions too.1 From an observational standpoint, the knee varus position, while assessing frontal plane knee alignment criterion, is a much less frequent deficiency compared to the knee valgus position.1 Lorenzetti et al.40 found that the athletes with less squatting experience were more likely to exhibit knee varus position when squatting without additional load, and knee varus was less common in the athletes with more squatting experience, while in the current study, the amateurs tended toward more knee valgus alignment. However, the alignment of lower structures, such as the feet, can also be influenced by the positioning of higher ones.1 Regarding the last criterion, it should be noted that monitoring uneven, too rapid, and unsmooth movement while descending often means insufficiency of back squat performance, which can be noticed more often in the athletes who have less squatting experience.1,11 The analysis of amateur bodybuilders’ descent in the current study allowed the observation of similar results. Interestingly, Miletello et al.11 found that skilled competitive collegiate powerlifters take longer while descending than powerlifting athletes who attended high school and who were beginners.4 The comparison of the performance of world-class and less experienced athletes of powerlifting revealed that more skilled athletes also take longer to descend, indicating more control.4,41
CONCLUSIONS
The results of the current study indicate that higher FMS™ scores in bodybuilders are associated with a better BSA scores during the performance of the back squat. Professional bodybuilders have higher FMS™ scores and higher BSA scores during back squat performances than amateurs. Amateur bodybuilders perform back squats with varying quality, depending on the amount of additional load, whereas professional bodybuilders, regardless of the weight, perform back squats with consistent quality. Greater experience in bodybuilding is associated with the compliance with the following BSA criteria: trunk position, frontal knee alignment, tibial translation angle, foot position in all three back squat variations with different external loads, and descent with the training weight, as professionals met these criteria more commonly than amateurs. Further studies are needed to evaluate training load, method, volume, frequency, and other parameters that can influence the quality of the back squat exercise performance.
Conflicts of interest
The authors report no conflicts of interest.
References
- The back squat: A proposed assessment of functional deficits and technical factors that limit performance. Myer G. D., Kushner A. M., Brent J. L.., et al. 2014Strength Cond J. 36(6):4–27. doi: 10.1519/SSC.0000000000000103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fundamental movement skills in children and adolescents: review of associated health benefits. Lubans D. R., Morgan P. J., Cliff D. P.., et al. 2010Sports Med. 40(12):1019–1035. doi: 10.2165/11536850-000000000-00000. [DOI] [PubMed] [Google Scholar]
- The activation of gluteal, thigh, and lower back muscles in different squat variations performed by competitive bodybuilders: implications for resistance training. Coratella G., Tornatore G., Caccavale F.., et al. 2021Int J Environ Res Public Health. 18(2):1–11. doi: 10.3390/ijerph18020772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inter- and intra-individual variability in the kinematics of the back squat. Kristiansen M., Rasmussen G. H. F., Sloth M. E.., et al. 2019Hum Mov Sci. 67(1):1–10. doi: 10.1016/j.humov.2019.102510. [DOI] [PubMed] [Google Scholar]
- Effect of knee position on hip and knee torques during the barbell squat. Fry A. C., Smith J. C., Schilling B. K. 2023Strength Cond J. 17(4):629–633. doi: 10.1519/1533-4287(2003)017<0629:eokpoh>2.0.co;2. [DOI] [PubMed] [Google Scholar]
- A three-dimensional biomechanical analysis of the squat during varying stance widths. Escamilla R. F., Fleisig G. S., Lowry T. M.., et al. 2001Med. Sci. Sports Exerc. 33(6):984–998. doi: 10.1097/00005768-200106000-00019. [DOI] [PubMed] [Google Scholar]
- A biomechanical comparison of the traditional squat, powerlifting squat, and box squat. Swinton P. A., Ray Lloyd, Keogh J. W. L.., et al. 2012Strength Cond J. 26(7):1805–1816. doi: 10.1519/JSC.0b013e3182577067. [DOI] [PubMed] [Google Scholar]
- Clinical movement analysis to identify muscle imbalances and guide exercise. Hirth C. J. 2007Athl Ther Today. 12(4):10–14. doi: 10.1123/att.12.4.10. [DOI] [Google Scholar]
- Clark M., Lucett S. NASM's essentials of corrective exercise training. Wolters Kluwer Health/Lippincott Williams & Wilkins; Philadelphia: [Google Scholar]
- Effects of technique variations on knee biomechanics during the squat and leg press. Escamilla R. F., Fleisig G. S., Zheng N.., et al. 2001Med Sci Sports Exerc. 33(9):1552–1556. doi: 10.1097/00005768-200109000-00020. [DOI] [PubMed] [Google Scholar]
- A biomechanical analysis of the squat between competitive collegiate, competitive high school, and novice powerlifters. Miletello W. M., Beam J. R., Cooper Z. C. 2009J Strength Cond Res. 23(5):1611–1617. doi: 10.1519/JSC.0b013e3181a3c6ef. [DOI] [PubMed] [Google Scholar]
- Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. Myer D. G., Ford R. K., Palumbo P. J. 2005J Strength Cond Res. 19(1):51–60. doi: 10.1519/13643.1. [DOI] [PubMed] [Google Scholar]
- Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. Myer D. G., Paterno V. M., Ford R. K. 2008J Strength Cond Res. 22(3):987–1014. doi: 10.1519/JSC.0b013e31816a86cd. [DOI] [PubMed] [Google Scholar]
- Associations between Functional Movement Screen scores and performance variables in surf athletes. Silva B., Clemente F. M., Martins F. M. 2018J Sports Med Phys Fit. 58(5):583–590. doi: 10.23736/S0022-4707.17.07154-7. [DOI] [PubMed] [Google Scholar]
- Using the Functional Movement ScreenTM to evaluate the effectiveness of training. Frost M. D., Beach T. A. C., Callaghan J. P. 2012J Strength Cond Res. 26(6):1620–1630. doi: 10.1519/JSC.0b013e318234ec59. [DOI] [PubMed] [Google Scholar]
- Assessment of dysfunctional movements and asymmetries in children and adolescents using the Functional Movement Screen–A narrative review. Vehrs P. R., Uvacsek M., Johnson A. W. 2021Int J Environ Res Public Health. 18(23):1–19. doi: 10.3390/ijerph182312501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pre-participation screening: the use of fundamental movements as an assessment of function – Part 2. Cook G., Burton L., Hoogenboom B. 2006N Am J Sports Phys Ther. 1(3):132–139. [PMC free article] [PubMed] [Google Scholar]
- Efficacy of the Functional Movement Screen: a rewiev. Kraus K., Schrutz E., Taylor W. R.., et al. 2014J Strength Cond Res. 28(12):3571–3584. doi: 10.1519/JSC.0000000000000556. [DOI] [PubMed] [Google Scholar]
- Iljinaitė V., Poškaitis V., Berškienė K. The comparison and correlation among the quality of functional movements, the perception of dynamic stereotype of movement, and the regularity of performance in bodybuilding; Kaunas, Lithuania. [Google Scholar]
- Functional Movement Screening: the use of fundamental movements as an assessment of function – Part 1. Cook G., Burton L., Hoogenboom B. J.., et al. 2014Int J Sports Phys Ther. 9(3):396–409. [PMC free article] [PubMed] [Google Scholar]
- The Functional Movement Screen's ability to detect changes in movement patterns after a training intervention. Minthorn L. M., Fayson S. D., Stobierski L. M.., et al. 2015J Sport Rehabil. 24(3):322–326. doi: 10.1123/jsr.2013-0146. [DOI] [PubMed] [Google Scholar]
- The effect of the direction of gaze on the kinematics of the squat exercise. Donnelly D. V., Berg W. P., Fiske D. M. 2006J Strength Cond Res. 20(1):145–150. doi: 10.1519/R-16434.1. [DOI] [PubMed] [Google Scholar]
- Sport specialization: developmental and learning issues. Branta C. F. 2010J Phys Educ Recreat Dance. 81(8):19–28. doi: 10.1080/07303084.2010.10598521. [DOI] [Google Scholar]
- Executive functions in children aged 6 to 13: a dimensional and developmental study. Brocki K. C., Bohlin G. 2004Dev Neuropsychol. 26(2):571–593. doi: 10.1207/s15326942dn2602_3. [DOI] [PubMed] [Google Scholar]
- Dynamically and statically determined low back movements during lifting. Mcgill S. M., Norman R. W. 1985J Biomech. 18(12):877–885. doi: 10.1016/0021-9290(85)90032-6. [DOI] [PubMed] [Google Scholar]
- Trunk and hip control neuromuscular training for the prevention of knee joint injury. Myer G. D., Chu D. A., Brent J. L.., et al. 2008Clin Sports Med. 27(3):425–448. doi: 10.1016/j.csm.2008.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Can the Functional Movement Screen method identify previously injured wushu athletes? Wang D., Lin X. M., Kulmala J. P.., et al. 2021Int J Environ Res Public Health. 18(2):1–9. doi: 10.3390/ijerph18020721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lower limb strength asymmetry and Functional Movement Screen values in professional soccer players. Sannicandro I., Giacomo C., Traficante P. 2019MOJ Sports Med. 3(3):59–62. doi: 10.15406/mojsm.2019.03.00081. [DOI] [Google Scholar]
- Effects of combination movement patterns quality and physical performance on injuries in young athletes. Koźlenia D., Domaradzki J. 2021Int J Environ Res Public Health. 18(11):1–10. doi: 10.3390/ijerph18115536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prediction of Functional Movement ScreenTM performance from lower extremity range of motion and core tests. Chimera N. J., Knoeller S., Cooper R.., et al. 2017Int J Sports Phys Ther. 12(2):173–181. [PMC free article] [PubMed] [Google Scholar]
- Association between motor competence and Functional Movement Screen scores. Silva B., Rodrigues L. P., Clemente F. M.., et al. 2019PeerJ. 7(8):1–18. doi: 10.7717/peerj.7270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anthropometry, physical and movement features, and repeated-sprint ability in soccer players. Campa F., Semprini G., Messina G.., et al. 2018Int J Sports Med. 40(2):100–109. doi: 10.1055/a-0781-2473. [DOI] [PubMed] [Google Scholar]
- CrossFit athletes exhibit high symmetry of fundamental movement patterns: a cross-sectional study. Tafuri S., Notarnicola A., Monno A.., et al. 2016Muscles Ligaments Tendons J. 6(1):157–160. doi: 10.32098/mltj.01.2016.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Training programs designed for muscle hypertrophy in bodybuilders: a narrative review. Alves R. C., Prestes J., Enes A.., et al. 2020Sports. 8(11):1–15. doi: 10.3390/sports8110149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perfil morfológico de culturistas Brasileiros de elite em período competitivo. Cyrino E. S., Sobrinho J. M. S., Maestá N.., et al. 2008Rev. Bras. de Medicina do Esporte. 14(5):460–465. [Google Scholar]
- Training practices and ergogenic aids used by male bodybuilders. Hackett D. A., Johnson N. A., Chow C. M. 2013J Strength Cond Res. 27(6):1609–1617. doi: 10.1519/JSC.0b013e318271272a. [DOI] [PubMed] [Google Scholar]
- The masters athlete in olympic weightlifting: training, lifestyle, health challenges, and gender differences. Huebner M., Meltzer D., Ma W.., et al. 2020PLoS ONE. 15(12):1–19. doi: 10.1371/journal.pone.0243652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Power production by olympic weightlifters. Garhammer J. 1980Med Sci Sports Exerc. 12(1):54–60. doi: 10.1249/00005768-198021000-00011. [DOI] [PubMed] [Google Scholar]
- Unique aspects of competitive weightlifting: performance, training and physiology. Storey A., Smith H. K. 2012J Sports Med. 42(9):769–790. doi: 10.1007/BF03262294. [DOI] [PubMed] [Google Scholar]
- How to squat? Effects of various stance widths, foot placement angles and level of experience on knee, hip and trunk motion and loading. Lorenzetti S., Ostermann M., Zeidler F.., et al. 2018BMC Sports Sci. Med. Rehabilitation. 10(1):1–11. doi: 10.1186/s13102-018-0103-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- A kinematic model of performance in the parallel squat by champion powerlifters. McLaughlin T., Dillman C. J., Lardner T. J. 1997Med Sci Sports Exerc. 9(2):128–133. [PubMed] [Google Scholar]