

Abstract
The study aimed to illustrate how contact (from match‐event data) and head acceleration event (HAE) (from instrumented mouthguard [iMG]) data can be combined to inform match limits within rugby. Match‐event data from one rugby union and rugby league season, including all competitive matches involving players from the English Premiership and Super League, were used. Playing exposure was summarised as full game equivalents (FGE; total minutes played/80). Expected contact and HAE exposures at arbitrary thresholds were estimated using match‐event and iMG data. Generalised linear models were used to identify differences in contact and HAE exposure per FGE. For 30 FGEs, forwards had greater contact than backs in rugby union (n = 1272 vs. 618) and league (n = 1569 vs. 706). As HAE magnitude increased, the differences between positional groups decreased (e.g., rugby union; n = 34 and 22 HAE >40 g for forwards and backs playing 30 FGEs). Currently, only a relatively small proportion of rugby union (2.5%) and league (7.3%) players exceeded 25 FGEs. Estimating contact and HAEs per FGE allows policymakers to prospectively plan and model estimated overall and position‐specific loads over a season and longer term. Reducing FGE limits by a small amount would currently only affect contact and HAE exposure for a small proportion of players who complete the most minutes. This may be beneficial for this cohort but is not an effective HAE and contact exposure reduction strategy at a population level, which requires individual player management. Given the positional differences, FGE limits should exist to manage appropriate HAE and contact exposure.
Keywords: athlete welfare, collision sport, player monitoring, policy
Highlights
Estimating contact events and head acceleration events (HAEs) per full game equivalents (FGE, i.e., 80 minutes) allows policymakers to prospectively plan and model estimated overall and position‐specific loads over a season and longer term.
Through retrospectively analysing FGE exposure, the findings demonstrate that only a small proportion of rugby players would be affected by a feasible reduction in FGE limits, but the difference in contact and HAE exposure for these players could be significant over the duration of a playing career.
Per FGE in both rugby codes, forwards have a greater expected contact and head acceleration event exposure than backs, and thus any implemented FGE limits should at least be position group‐specific and ideally incorporate individual player management.
1. INTRODUCTION
Rugby union (RU) and rugby league (RL) are contact sports (Naughton et al., 2020; Paul et al., 2022) with a relatively high injury incidence compared to other team sports (King et al., 2022; Williams et al., 2022). Governing bodies continue to make law and policy decisions to reduce potential injury risks to players (Hendricks et al., 2014, 2023; Raftery et al., 2020). In RU, law modification trials (e.g., reduce legal height of tackle) have been undertaken, attempting to reduce the risk of concussion (Stokes et al., 2021; van Tonder et al., 2023). Similarly, limits on playing exposure (i.e., number of matches and/or minutes played) have been considered. Based on the association between playing exposure and injury risk, players are limited to 30 full game equivalents (FGEs; i.e., 30 × 80 min) or 35 match involvements (>20‐min duration) per season (Williams et al., 2017). In RL, there are currently no published limits on the number of matches or minutes players can participate in.
There is a growing concern surrounding the long‐term effects of concussion and repeated head impacts in sport (Eliason et al., 2023; Iverson et al., 2023; Patricios et al., 2023). Consequently, contact and head acceleration event (HAE) exposure of players is being considered (McCormack et al., 2022; Tierney et al., 2021; Tooby et al., 2023). Match‐event data can provide the contact exposure a player experiences (e.g., ball‐carry and tackle). Likewise, instrumented mouthguards (iMGs) provide a valid measure of HAEs (Jones et al., 2022; Tooby et al., 2024). Excluding training, a player's overall contact and HAE exposure can be managed prospectively by limiting the number of matches they can participate in. Although match‐event and HAE data have been considered within the literature individually (Rennie et al., 2022; Tooby et al., 2023), these two measures have not yet been combined. Using known HAE rates from a sample of iMG data, alongside match‐event data, can provide expected HAE exposures for players (i.e., estimated number of HAEs based on match‐events and/or FGEs), which can then be used to prospectively consider appropriate match limits. This could be applied across all levels of sport, even in the absence of iMGs, which are now common in some professional rugby competitions. (Roe et al., 2024; Rugby Football League, 2023; World Rugby, 2023).
The aim of this study was to illustrate how a sample of iMG data could be combined with match‐event data to provide population level HAE and contact information and inform match limits using professional RU and RL in England as examples. The specific research questions were (i) what is the current distribution of FGE? (ii) what is the contact exposure per FGE? (iii) what is the expected HAE exposure per FGE across a range of thresholds (>20 g, >40 g, >1500 rad/s2 and >3000 rad/s2)? and (iv) practically, how would changing the FGE limits affect the expected contact and HAE exposure using the current FGE distribution?
2. METHODS
Event level match data were obtained for each player who participated in the Premiership (RU) or Super League (RL) from Stats Perform (Stats Perform, London, UK) for one full season of a competitive rugby match play. For RU, 324 matches were considered between 1/9/21 and 31/7/22, including matches from the Premiership (n = 156), Premiership Rugby Cup (n = 28), European Challenge Cup (n = 23), European Champions Cup (n = 33), 6 Nations (n = 15), the Rugby Championship (n = 12) and other Internationals, including the Autumn and July internationals (n = 57). For RL, 215 matches were considered between 1/2/22 and 31/12/22, including the Super League (n = 167), Challenge Cup (n = 15), Rugby League World Cup (n = 31) and Friendly Internationals (n = 2). All competitions were included to capture the total match, contact and estimated HAE exposure experienced by players. Ethics approval was obtained prior to analysis.
This study focused specifically on players who participated in the Premiership (RU) or Super League (RL) but considered all matches they played in during a season of competitive match play (including European competitions and international matches). Playing and contact exposures were identified using Stats Perform match event data and estimated HAE exposures were calculated across all matches using previously published HAE rates.
2.1. Data pre‐processing
To be included in the analysis, players were required to have played at least 1 min of a competitive match play in the Premiership (RU) or Super League (RL). This resulted in a total playing population of 598 RU (n = 347 forwards and n = 251 backs) and 402 RL (n = 183 forwards, n = 182 backs and n = 37 unassigned) players. Playing positions were provided by Stats Perform within their match‐event data.
Total playing exposure in FGEs for each player was calculated as the sum of their minutes played from all match involvements across all competitions, as identified by Stats Perform, divided by 80. The division by 80 converted playing exposure to FGE units similar to previous research (Williams et al., 2017, 2023) and is more intuitive than the total duration (e.g., 24 FGEs vs. 1920 min).
Contact exposure for each player was calculated as the sum of contact event counts, extracted from match‐event data. All definitions and coding for contact events were based on the Stats Perform user manual. In RU, any ball‐carry leading to contact, tackle event, missed tackle event where the player was “bumped off” and ruck involvement were considered as contact events based on previous iMG research (Tooby et al., 2023). In RL, any ball‐carry leading to contact, tackle event and missed tackle event where the player was “bumped off” were considered as contact events. In both codes, tackle and missed tackle events were grouped together as tackle events for the calculation of HAE exposures.
The example HAE rates for RU were taken from published literature (Tooby et al., 2023), which were based on 42 men's forwards and 23 men's backs. The example HAE rates for RL were calculated using the same methodology, from a sample of unpublished data (75 men's forwards and 75 men's backs). In both codes, all players wore the same manufacturer's custom fit iMGs (Prevent Biometrics), which has previously been validated (Jones et al., 2022). Mean incidences for both codes and an example HAE exposure calculation are provided in Table 1. The HAE exposure for each player was calculated at four arbitrary thresholds (peak linear acceleration [PLA] >20 g and >40 g and peak angular acceleration [PAA] >1500 rad/s2 and >3000 rad/s2). The thresholds were selected in line with previous research (Wang et al., 2021) indicating an impact producing a PLA of 10 g typically produces a PAA of 750 rad/s2 and were provided to illustrate differences in the conclusions drawn when a range of arbitrary thresholds were used. The HAE exposures were calculated as the sum of each contact event count multiplied by its incidence of HAEs above each threshold and a per minute of playing time “other HAEs” rate, which was made up of HAEs experienced by players not associated with events coded for individual players by Stats Perform (e.g., scrums, lineouts, mauls and other contact events). These data were used to calculate estimated mean HAE numbers from match‐event data per season.
TABLE 1.
Mean incidence of HAEs per contact event for each positional group and HAE threshold.
| Contact event | >20 g | >40 g | >1500 rad/s2 | >3000 rad/s2 | >20 g | >40 g | >1500 rad/s2 | >3000 rad/s2 |
|---|---|---|---|---|---|---|---|---|
| Forward | Back | |||||||
| Rugby union | ||||||||
| Ball‐carry | 0.26 | 0.03 | 0.25 | 0.01 | 0.24 | 0.04 | 0.22 | 0.04 |
| Tackle | 0.21 | 0.03 | 0.23 | 0.04 | 0.28 | 0.05 | 0.27 | 0.06 |
| Ruck | 0.10 | 0.01 | 0.07 | 0.01 | 0.12 | 0.01 | 0.08 | 0.01 |
| Other (per min) | 0.02 | 0.00 | 0.02 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 |
| Rugby league | ||||||||
| Ball‐carry | 0.12 | 0.01 | 0.14 | 0.01 | 0.12 | 0.02 | 0.13 | 0.02 |
| Tackle | 0.11 | 0.01 | 0.13 | 0.02 | 0.11 | 0.01 | 0.15 | 0.02 |
| Other (per min) | 0.00 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 |
Note: Example: A rugby union forward with 100 playing minutes, which included 30 tackles, 10 ball‐carries and 50 ruck involvements. Contact exposure: 30 tackles + 10 carries + 50 rucks = 90. HAE >20 g exposure: (30 tackles*0.26 [HAEs >20 g per tackle]) + (10 carries*0.21 [HAEs >20 g per carry]) + (50 rucks*0.10 [HAEs >20 g per ruck]) + (100 min played*0.02 [HAEs >20 g per minute played]) = 16.9.
2.2. Statistical analysis
To estimate the expected contact and HAE exposure conditional on the number of FGEs and position, generalised linear models were used. These models utilised a Poisson distribution, with an identity link function to allow the linear relationship between minutes played and contact counts to be evaluated. The use of the identity link function also ensured that differences between positions could be evaluated in raw units rather than odds ratios. Ten models were run (five for RU and five for RL). One model used to estimate contact exposure in each sport and four models for HAE exposure at different thresholds (>20 g, >40 g, >1500 rad/s2 and >3000 rad/s2). In all models, the fixed effects included were position, FGEs played and the position*FGEs played interaction term, which allowed for differences in FGE slopes between positions to be estimated. No statistical hypotheses or effect size thresholds were considered in this study. The root mean squared error (RMSE) was calculated to establish the variability between expected values and observed values in this sample. Results are reported as integers in raw count units (95% confidence intervals).
Descriptive statistics were used to calculate the practical impact of reducing FGE limits on the expected contact and HAE exposure and the number of players who would be affected by a reduction in FGE limits (i.e., the number of players who played a greater number of FGEs than the reduced limit within the season analyzed). The implication was analyzed for FGE limits from ≤20 FGEs to ≤30 FGEs for practical illustration purposes. For RU, all values are compared to the current limit, ≤30 FGEs; for RL, values are compared to ≤33 FGEs, the largest amount completed by a player within the current study.
3. RESULTS
3.1. Distribution of playing exposure in rugby union and rugby league players
The highest proportion of players played 0–5 FGEs in both RU (29.8%) and RL (29.6%) (Figure 1). In RU, 12.0% of players completed >20 FGEs and 2.5% completed >25 FGEs (Figure 1A). In RL, 19.2% of players completed >20 FGEs and 7.2% completed >25 FGEs (Figure 1B).
FIGURE 1.
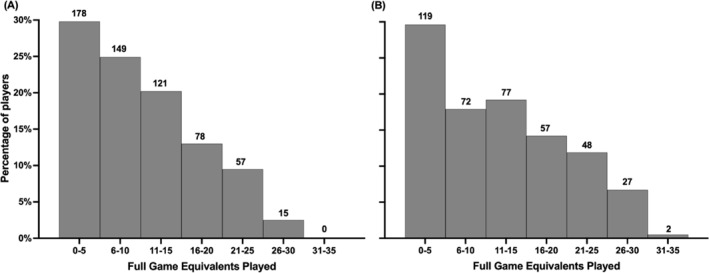
The percentage and number of players who are exposed to a range of FGEs in a competitive season of (A) rugby union and (B) rugby league match play.
3.2. Contact exposure per FGE
Figure 2 shows the expected contact exposure for RU (Figure 2A) and RL (Figure 2B) as a function of the FGEs played. Forwards experience more contacts per FGE than backs in both RU and RL. In RU, for every FGE played, forwards experience 42 (42–43) contacts, and backs experience 20 (20–21) contacts. In RL, for every FGE played, forwards experience 51 (51–52) contacts, and backs experience 24 (23–24) contacts.
FIGURE 2.
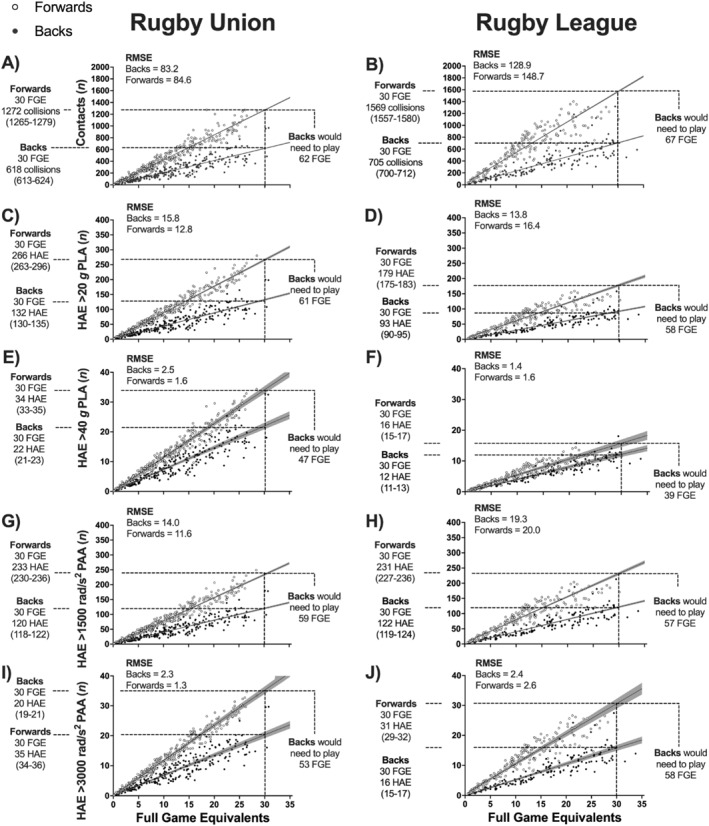
The number of contacts (A, B), and HAEs for PLA >20 g (C, D), PLA >40 g (E, F), PAA >1500 rad/s2 (G, H) and PAA >3000 rad/s2 (I, J) for rugby union and rugby league players based on FGEs. The Y‐axis scales for Figures C, D, G and H are 5 times smaller than Figures A, B. The Y‐axis scales for Figures E, F, I, and J are 50 and 10 times smaller than Figures A, B and Figures C, D, G and H. The shaded area around lines represents 95% confidence intervals. The dashed lines illustrate the number of contacts and HAEs for 30 FGEs, and the number of FGEs needed to have the same number of contacts as 30 FGEs. FGE, full game equivalents; HAE, head acceleration events; RMSE, root mean square error.
3.3. HAE exposure per FGE
Figure 2C–J show the expected HAE exposure at different thresholds for FGEs played. In RU and RL, forwards have a greater HAE exposure per FGE than backs for all thresholds. For HAE >20 g, the expected exposure was 9 (9–9) per FGE for forwards and 4 (4–4) per FGE for backs in RU. In RL, this was 6 (6–6) per FGE for forwards and 3 (3–3) per FGE for backs. For HAE >1500 rad/s2, the expected exposure was 8 (8–8) per FGE for forwards and 4 (4–4) per FGE for backs in RU. In RL, this was 8 (7–8) per FGE for forwards and 4 (4–4) per FGE for backs.
3.4. What is the practical impact of a change in FGE limits?
Table 2 shows the expected contact exposure for a player per season based on FGEs and the expected reduction in the number of contacts as FGE limits are reduced in RU and RL. Tables 3 and 4 provide similar information for expected HAE exposure at the four arbitrary thresholds. Together, the tables show differences in the maximum contact and HAE exposures by different FGE limits.
TABLE 2.
Expected contact exposure per season, the difference in the number of contacts compared to the 30 FGE limit for rugby union and 33 FGEs (current maximum FGEs played) in rugby league and the number of players who would have a reduced contact exposure per season based on current FGE limits in rugby union and maximum FGEs played in rugby league.
|
FGEs |
Rugby union | Rugby league | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Contact exposure per player per season (95% CI) | Difference in number of contacts compared to 30 FGE | Players with reduced contact exposure based on current 30 FGE limit (% of playing population) | Contact exposure per player per season (95% CI) | Difference in number of contacts compared to 33 FGEs | Players with reduced contact exposure based on 33 FGE comparison (% of playing population) | |||||||||
| Forwards | Backs | Forwards | Backs | Overall | Forwards | Backs | Forwards | Backs | Forwards | Backs | Overall | Forwards | Backs | |
| ≤30 | 1272 (1265–1279) | 618 (613–624) | ‐ | ‐ | ‐ | ‐ | ‐ | 1569 (1557–1580) | 705 (697–712) | −154 | −71 | 2 (0.5%) | 0 (0.0%) | 2 (1.1%) |
| ≤29 | 1230 (1223–1236) | 598 (593–603) | −42 | −21 | 3 (0.5%) | 0 (0.0%) | 3 (1.2%) | 1518 (1507–1528) | 681 (674–688) | −205 | −94 | 3 (0.7%) | 1 (0.5%) | 2 (1.1%) |
| ≤28 | 1187 (1181–1194) | 577 (572–582) | −85 | −41 | 3 (0.5%) | 0 (0.0%) | 3 (1.2%) | 1466 (1456–1477) | 658 (650–665) | −257 | −118 | 9 (2.2%) | 1 (0.5%) | 8 (4.4%) |
| ≤27 | 1145 (1139–1151) | 557 (552–562) | −127 | −62 | 5 (0.8%) | 1 (0.3%) | 4 (1.6%) | 1415 (1405–1425) | 634 (627–641) | −308 | −142 | 16 (4.0%) | 2 (1.1%) | 14 (7.7%) |
| ≤26 | 1103 (1096–1109) | 536 (532–541) | −169 | −82 | 5 (0.8%) | 1 (0.3%) | 4 (1.6%) | 1364 (1354–1373) | 611 (604–617) | −359 | −165 | 22 (5.5%) | 3 (1.6%) | 19 (10.4%) |
| ≤25 | 1060 (1054–1066) | 516 (511–520) | −212 | −103 | 15 (2.5%) | 4 (1.2%) | 11 (4.4%) | 1312 (1303–1321) | 587 (580–594) | −410 | −189 | 29 (7.2%) | 6 (3.3%) | 23 (12.6%) |
| ≤24 | 1018 (1012–1024) | 495 (491–499) | −254 | −124 | 23 (3.8%) | 8 (2.3%) | 15 (6.0%) | 1261 (1252–1270) | 563 (557–570) | −462 | −212 | 35 (8.7%) | 7 (3.8%) | 28 (15.4%) |
| ≤23 | 976 (970–981) | 474 (470–478) | −296 | −144 | 37 (6.2%) | 16 (4.6%) | 21 (8.4%) | 1210 (1202–1218) | 540 (534–546) | −513 | −236 | 42 (10.4%) | 10 (5.5%) | 32 (17.6%) |
| ≤22 | 933 (928–939) | 454 (450–458) | −338 | −165 | 49 (8.2%) | 23 (6.6%) | 26 (10.4%) | 1158 (1151–1166) | 516 (510–523) | −564 | −260 | 50 (12.4%) | 13 (7.1%) | 37 (20.3%) |
| ≤21 | 891 (886–896) | 433 (430–437) | −381 | −185 | 62 (10.4%) | 28 (8.1%) | 34 (13.5%) | 1107 (1100–1114) | 493 (487–499) | −616 | −283 | 60 (14.9%) | 15 (8.2%) | 45 (24.7%) |
| ≤20 | 849 (844–853) | 413 (409–416) | −443 | −206 | 72 (12.0%) | 34 (9.8%) | 38 (15.1%) | 1056 (1049‐106) | 469 (463–475) | −667 | −307 | 77 (19.2%) | 24 (13.1%) | 53 (29.1%) |
Note: Counts are rounded to the nearest integer. The number of rugby union and rugby league players with reduced contact exposure is compared to current FGE limits in rugby union and the current maximum FGE played in rugby league. Data are also presented in Figure 1A,B.
TABLE 3.
Expected HAE exposure per player per season and the difference in HAE exposure compared to current FGE limits (30 FGEs) in rugby union.
| FGEs | HAE exposure per player per season (95% CI) | Difference in HAE exposure compared to current limits (30 FGE) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PLA >20 g | PLA >40 g | PAA >1500 rad/s2 | PAA >3000 rad/s2 | PLA >20 g | PLA >40 g | PAA >1500 rad/s2 | PAA >3000 rad/s2 | |||||||||
| Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | |
| ≤30 | 266 (263–269) | 132 (130–135) | 34 (33–35) | 22 (21–23) | 233 (230–236) | 120 (118–122) | 35 (34–36) | 20 (19–21) | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ | ‐ |
| ≤29 | 257 (254–260) | 128 (125–130) | 33 (32–34) | 21 (20–22) | 225 (222–228) | 116 (114–118) | 34 (33–35) | 20 (19–21) | −9 | −4 | −1 | −1 | −8 | −4 | −1 | −1 |
| ≤28 | 248 (245–251) | 123 (121–126) | 32 (31–33) | 20 (20–21) | 218 (215–221) | 112 (110–114) | 33 (32–34) | 19 (18–20) | −18 | −9 | −2 | −1 | −16 | −8 | −2 | −1 |
| ≤27 | 239 (236–242) | 119 (117–121) | 31 (30–32) | 20 (19–21) | 210 (207–213) | 108 (106–110) | 32 (31–33) | 18 (17–19) | −27 | −13 | −3 | −2 | −23 | −12 | −4 | −2 |
| ≤26 | 230 (228–233) | 115 (112–117) | 30 (29–31) | 19 (18–20) | 202 (200–205) | 104 (102–106) | 31 (30–32) | 18 (17–18) | −35 | −18 | −5 | −3 | −31 | −16 | −5 | −3 |
| ≤25 | 222 (219–224) | 110 (108–112) | 28 (27–29) | 18 (17–19) | 194 (192–197) | 100 (98–102) | 29 (28–30) | 17 (16–18) | −44 | −22 | −6 | −4 | −39 | −20 | −6 | −3 |
| ≤24 | 213 (210–215) | 106 (104–108) | 27 (26–28) | 18 (17–18) | 187 (184–189) | 96 (94–98) | 28 (27–29) | 16 (15–17) | −53 | −26 | −7 | −4 | −47 | −24 | −7 | −4 |
| ≤23 | 204 (201–206) | 101 (100–103) | 26 (25–27) | 17 (16–18) | 179 (177–181) | 92 (90–94) | 27 (26–28) | 16 (15–16) | −62 | −31 | −8 | −5 | −54 | −28 | −8 | −5 |
| ≤22 | 195 (193–197) | 97 (95–99) | 25 (24–26) | 16 (15–17) | 171 (169–173) | 88 (86–90) | 26 (25–27) | 15 (14–16) | −71 | −35 | −9 | −6 | −62 | −32 | −9 | −5 |
| ≤21 | 186 (184–188) | 93 (91–94) | 24 (23–25) | 15 (15–16) | 163 (161–165) | 84 (83–86) | 25 (24–25) | 14 (14–15) | −80 | −39 | −10 | −7 | −70 | −36 | −11 | −6 |
| ≤20 | 177 (175–179) | 88 (87–90) | 23 (22–23) | 15 (14–15) | 156 (154–158) | 80 (79–82) | 24 (23–24) | 14 (13–14) | −88 | −44 | −11 | −7 | −78 | −40 | −12 | −7 |
Note: Counts and differences are rounded to the nearest integer.
TABLE 4.
Expected HAE exposure per player per season and the difference in HAE exposure compared to the current maximum FGE played (33 FGEs) in rugby league.
| FGEs | HAE exposure per player per season (95% CI) | Difference in HAE exposure compared to current maximum time played (33 FGE) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PLA >20 g | PLA >40 g | PAA >1500 rad/s2 | PAA >3000 rad/s2 | PLA >20 g | PLA >40 g | PAA >1500 rad/s2 | PAA >3000 rad/s2 | |||||||||
| Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | Fwds | Bcks | |
| ≤30 | 179 (175–183) | 93 (90–95) | 16 (15–17) | 12 (11–13) | 231 (227–236) | 122 (119–124) | 31 (29–32) | 16 (15–17) | −18 | −9 | −2 | −1 | −23 | −12 | −3 | −2 |
| ≤29 | 173 (169–177) | 90 (87–92) | 16 (15–17) | 12 (11–12) | 224 (220–228) | 118 (115–120) | 30 (28–32) | 15 (14–16) | −23 | −12 | −2 | −2 | −30 | −16 | −4 | −2 |
| ≤28 | 167 (163–171) | 86 (84–88) | 15 (14–16) | 11 (11–12) | 216 (212–220) | 114 (111–116) | 29 (27–30) | 15 (14–16) | −29 | −15 | −3 | −2 | −38 | −20 | −5 | −3 |
| ≤27 | 161 (158–165) | 83 (81–85) | 15 (14–16) | 11 (10–12) | 209 (205–213) | 109 (107–112) | 28 (26–29) | 14 (13–15) | −35 | −19 | −3 | −2 | −46 | −24 | −6 | −3 |
| ≤26 | 155 (152–159) | 80 (78–82) | 14 (13–15) | 11 (10–11) | 201 (197–205) | 105 (103–108) | 27 (25–28) | 14 (13–14) | −41 | −22 | −4 | −3 | −53 | −28 | −7 | −4 |
| ≤25 | 149 (146–153) | 77 (75–79) | 14 (13–15) | 10 (9–11) | 194 (190–197) | 101 (99–103) | 26 (24–27) | 13 (12–14) | −47 | −25 | −4 | −3 | −61 | −33 | −8 | −4 |
| ≤24 | 144 (141–147) | 74 (72–76) | 13 (12–14) | 10 (9–10) | 186 (183–189) | 97 (95–99) | 25 (23–26) | 13 (12–13) | −53 | −28 | −5 | −4 | −68 | −37 | −9 | −5 |
| ≤23 | 138 (135–141) | 71 (69–73) | 13 (12–14) | 9 (9–10) | 178 (175–181) | 93 (91–95) | 24 (22–25) | 12 (11–13) | −58 | −31 | −5 | −4 | −76 | −41 | −10 | −5 |
| ≤22 | 132 (129–135) | 68 (66–69) | 12 (17–19) | 9 (8–9) | 171 (168–174) | 89 (87–91) | 23 (22–24) | 12 (11–12) | −64 | −34 | −6 | −4 | −83 | −45 | −11 | −6 |
| ≤21 | 126 (124–129) | 65 (63–66) | 18 (17–20) | 8 (8–9) | 163 (160–166) | 85 (83–87) | 22 (21–23) | 11 (10–12) | −70 | −37 | −6 | −5 | −91 | −49 | −12 | −6 |
| ≤20 | 120 (118–123) | 62 (60–63) | 19 (18–20) | 8 (8–9) | 156 (153–158) | 81 (79–83) | 21 (20–22) | 11 (10–11) | −76 | −40 | −7 | −5 | −99 | −53 | −13 | −7 |
Note: Counts and differences are rounded to the nearest integer.
In RU, if FGE limits were reduced from 30 to 20 per season, the expected contact exposure for a forward playing 30 versus 20 FGEs would decrease from 1272 (1265–1279) to 849 (844–843). For backs, it would decrease from 618 (613–624) to 413 (409–416). The expected HAE >20 g exposure would decrease from 266 (263–269) to 177 (175–179) for forwards and from 132 (130–135) to 88 (87–90) for backs playing 30 versus 20 FGEs. Based on the distribution of FGEs completed in RU (Figure 1), these changes would affect 72 (12.0%) of players (34 [9.8%] forwards and 38 [15.1%] backs).
In RL, a FGE limit of 20 per season compared to the maximum FGEs played (i.e., 33 vs. 20 FGEs) would reduce the expected contact exposure from 1723 (1710–1736) to 1056 (1049–1063) for forwards and from 777 (770–783) to 470 (466–474) for backs. The expected HAE >20 g exposure would decrease from 196 (192–201) to 120 (118–123) for forwards and from 102 (99–104) to 62 (60–63) for backs playing 33 versus 20 FGEs. Based on the distribution of FGEs completed in RL, these changes would affect 77 (19.2%) of players (24 [13.1%] forwards and 53 backs [29.1%]).
4. DISCUSSION
The aim of this study was to combine a sample of iMG data with match‐event data to provide population level contact and HAE exposure information and inform match limits using professional RU and RL. There are two key findings. Firstly, a relatively large reduction in FGE match limits is required to impact a large proportion of players within the respective rugby populations, given the current competition structure (i.e., available matches to play) and squad management policies (e.g., player rotation or recovery from injury). However, the career‐long cumulative impact of reduced FGEs (and subsequent contact and HAEs) may be important for the small proportion of players who would be affected by a reduction in FGEs and should be considered by policymakers, alongside individual player management strategies. The FGE match limits will likely evolve over time, in line with the increased collective understanding of the dose‐response relationship between contact and HAE and any negative health outcomes. Secondly, forwards experience significantly more contact and HAEs per FGE than backs. Therefore, if the intention in managing game exposure is to reduce head impact load, the appropriateness of forwards and backs having the same FGE limits should be considered. Consequently, any implemented FGE limits should be position group‐specific, and possibly even position‐specific based on future research.
4.1. Combining samples of iMG data with match‐event data
In this study, using a sample of iMG data combined with match‐event data, insights into expected contact and HAE exposures were made. Although the results are extrapolated estimations, they show that important insights can be gleaned without access to iMG data from the full population of players. Instrumented mouthguards have now been mandated as part of the HIA protocol in the elite game globally, including within some professional RU and RL competitions (Rugby Football League, 2023; World Rugby, 2023). This will make it possible to individually manage players based on HAE limits, if desired. The method used in this study can be used concurrent to individual player management strategies. Individual player data will only be available after the activity, whereas the method used in this study can prospectively plan for expected contact and HAEs, based on FGEs. Furthermore, where iMGs are not available (e.g., sub‐elite levels), the method used in this study can support planning if representative iMG and match event data can be sourced. Other applications not considered in this study include the ability to assess the impact of law modification trials on overall HAE exposure through the manipulation of the rate multipliers and the ability to retrospectively estimate HAE exposure for previous seasons. Furthermore, researchers may wish to consider the relationship between iMG data and blood biomarkers of traumatic brain injury (O'Brien et al., 2023) and/or typical neurological responses (D'Arcy et al., 2024). Both measures could add further objectivity to the monitoring of collision frequency and intensity outcomes, which may help inform future law modifications.
4.2. Practical impact of a change in FGE limits within professional rugby
Within RU, reducing FGE limits from 30 to 25 FGEs would affect 2.5% of players, while a reduction to 20 FGEs would affect 12.0%. In RL, introducing FGE limits at 25 FGEs would affect 7.2% of players, whereas introducing a limit of 20 FGEs would affect 19.2%. These differences suggest that the use of FGE limits may be relatively more effective in RL than RU. The impact of reducing FGE limits could be important for players with the greatest playing exposures, especially when considered over a 10‐season career. Given the associations between estimated cumulative head accelerations and traumatic encephalopathy (Daneshvar et al., 2023), a reduction across a 10‐year playing career may have real life consequences, particularly for forwards. The challenge for rugby's governing bodies is to reduce this exposure for all players, by managing HAEs on an individual level, and potentially complement this with limits on playing time that would further reduce exposure in the relatively small cohort of players who currently experience the highest risk by virtue of match involvements and FGEs.
4.3. Positional differences
Clear positional group differences were present for contact and HAE exposures between forwards and backs. If a RU forward played 30 FGEs, they would have 1272 contacts and 34 HAEs >40 g. A back would need to play 62 FGEs to have a similar contact exposure and 47 FGEs to have similar HAE >40 g exposure (Figure 2, Tables 2, 3, 4). This position group difference is similar although less pronounced for RL. Whilst a definitive FGE, contact or HAE limit does not exist, even reducing the FGE limit to 20 in forwards would not reduce their contacts and HAEs below the number experienced by backs in 30 FGEs. Based on these differences, positional FGE guidelines may be beneficial; however, a more definitive understanding of what is considered clinically important in terms of both individual and cumulative magnitude of head loading may be required to fully inform such guidelines.
4.4. Further considerations within FGE limits
Reducing HAE exposure may be informative for brain‐health‐based guidelines (Daneshvar et al., 2023), and using contact exposure may be more appropriate if all injuries were considered, given approximately 68.9% of all injuries (i.e., musculoskeletal and neurological) occur within the contact events considered in this study (Williams et al., 2022). Another consideration is the rate of accumulation of FGE (i.e., 10 FGEs could be 10 full matches or 40 × 20‐min match appearances), which was not considered in this study. A different number of matches for the same FGE output may provide different physical and psychological burdens within and between players, influencing the efficacy of the limits implemented. Furthermore, FGE limits should be balanced against the commercial demands of the sport and the requirement for the wider playing squad to be large enough for all matches to be completed while still allowing planned and enforced rest periods. The required playing population from by a change in FGE limits should be evaluated alongside expected injury rates and other factors causing a player to be unavailable (e.g., international commitments). Considering these factors should ensure that unfeasible FGE limits are not implemented with unforeseen consequences. A potential unintended positive outcome from FGE limits is the enhanced development of younger/squad rotation players. Currently, ∼50% of players across both codes play 0–10 FGEs per season. As the playing time of the top players is reduced, the remaining minutes will be completed by these other players, potentially accelerating their development in top‐tier competition (Till et al., 2020) and reducing their risk of injury when they do play (Williams et al., 2017, 2023).
4.5. Limitations
While providing useful insights regarding the combination of samples of iMG and match‐event data, this study has some limitations. Due to the methods of data collection within professional rugby at the time of analysis, the sample of iMG data was not random (i.e., iMGs were worn by players voluntarily). Therefore, it is unclear whether it is representative of the whole population. Secondly, as only top tier competitions were included within the study, the distributions of playing exposure may differ slightly for players at lower levels (i.e., no loan club matches were included if they took place below the top tier). The decision to include only top tier competitions was taken for consistency between RU and RL. Related to this, there is no consideration of the training exposure experienced by players. As players train more than they play, this could influence their overall HAE exposure and may therefore need to be considered in the management of players. Finally, the use of secondary data (i.e., the commercially available match‐event data) was necessary within this study but presents potential limitations as the authors were unable to perform any measure of quality control with respect to the coding provided. The use of this data ensured that exposures for contact events were grouped together from a HAE perspective. However, it should be noted that each contact event may have its own unique highly physical demands which are not considered in this paper and may be relevant for the monitoring of players (e.g., with respect to injury/fatigue management).
4.6. Conclusions
This study introduced a method through which iMG data could be combined with match‐event data to provide population level HAE information and inform playing exposure limits using professional RU and RL as examples. From a practical perspective, introducing FGEs would affect only a small proportion of the playing population. However, the career‐long cumulative impact of these changes for affected players may be important and should be considered. Differences between positional groups were also identified, with forwards having greater contact and HAE exposure than backs in both rugby codes. Consequently, FGE and contact exposure guidelines should be position‐specific. However, multiple factors should be considered when proposing FGE limits, including all injuries, the commercial success of the sport, squad sizes and the development of low FGE players.
CONFLICT OF INTEREST STATEMENT
TS and GR are part‐funded by World Rugby and Premiership Rugby. MC is employed by Premiership Rugby. CO is part‐funded by the Rugby Football League. JT is part‐funded by World Rugby, Premiership Rugby and the Rugby Football League. LS and ÉF are employed by World Rugby. CR is employed by South Africa Rugby Union. KR is employed by the New Zealand Rugby Union. KS and SK are employed by the Rugby Football Union. GT has received funding from World Rugby. RT is employed by World Rugby as a consultant. BJ is employed by Premiership Rugby and the Rugby Football League as a consultant, and has received research funding from Prevent Biometrics and World Rugby.
ACKNOWLEDGMENTS
The authors would like to acknowledge instrumented mouthguard managers from each club.
REFERENCES
- Daneshvar, Daniel H. , Nair Evan S., Baucom Zachary H., Rasch Abigail, Abdolmohammadi Bobak, Uretsky Madeline, Saltiel Nicole, et al. 2023. “Leveraging Football Accelerometer Data to Quantify Associations Between Repetitive Head Impacts and Chronic Traumatic Encephalopathy in Males.” Nature Communications 14(1): 3470. 10.1038/s41467-023-39183-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Arcy Ryan C. N., McCarthy David, Harrison Derek, Levenberg, Zander , Wan, Julian , Hepburn, Aidan , Kirby, Eric D. , et al. 2024. “An Objective Neurophysiological Study of Subconcussion in Female and Male High School Student Athletes.” 10.1101/2024.03.20.24304610. [DOI]
- Eliason, Paul H. , Galarneau J.‐Michel, Kolstad Ash T., Pankow M. Patrick, West Stephen W., Bailey Stuart, Miutz Lauren, et al. 2023. “Prevention Strategies and Modifiable Risk Factors for Sport‐Related Concussions and Head Impacts: A Systematic Review and Meta‐Analysis.” British Journal of Sports Medicine 57(12): 749–761. 10.1136/bjsports-2022-106656. [DOI] [PubMed] [Google Scholar]
- Hendricks, Sharief , Emery Carolyn, Jones Ben, Brown James Craig, Dane Kathryn, West Stephen W., Stokes Keith A., Gray Richie, and Tucker Ross. 2023. “‘Tackling’ Rugby Safety through a Collective Approach.” British Journal of Sports Medicine 57(10): 562–563. 10.1136/bjsports-2023-107020. [DOI] [PubMed] [Google Scholar]
- Hendricks, Sharief , Lambert Mike I., Brown James C., Readhead Clint, and Viljoen Wayne. 2014. “An Evidence‐Driven Approach to Scrum Law Modifications in Amateur Rugby Played in South Africa.” British Journal of Sports Medicine 48(14): 1115–1119. 10.1136/bjsports-2013-092877. [DOI] [PubMed] [Google Scholar]
- Iverson, Grant L. , Castellani Rudolph J., Cassidy J. David, Schneider Geoff M., Schneider Kathryn J., Echemendia Ruben J., Bailes Julian E., et al. 2023. “Examining Later‐In‐Life Health Risks Associated With Sport‐Related Concussion and Repetitive Head Impacts: A Systematic Review of Case‐Control and Cohort Studies.” British Journal of Sports Medicine 57(12): 810–824. 10.1136/bjsports-2023-106890. [DOI] [PubMed] [Google Scholar]
- Jones, Ben , Tooby James, Weaving Dan, Till Kevin, Owen Cameron, Begonia Mark, Stokes Keith A., et al. 2022. “Ready for Impact? A Validity and Feasibility Study of Instrumented Mouthguards (iMGs).” British Journal of Sports Medicine 56(20): 1171–1179. 10.1136/bjsports-2022-105523. [DOI] [PubMed] [Google Scholar]
- King, Doug , Clark Trevor, Hume Patria, and Hind Karen. 2022. “Match and Training Injury Incidence in Rugby League: A Systematic Review, Pooled Analysis, and Update on Published Studies.” Sports Medicine and Health Science 4: 75–84. 10.1016/j.smhs.2022.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCormack, Sam , Till Kevin, Wenlock Jessica, Whitehead Sarah, Stokes Keith A., Bitcon Mark, Brown James, et al. 2022. “Contributors to Negative Biopsychosocial Health or Performance Outcomes in Rugby Players (CoNBO): A Systematic Review and Delphi Study Protocol.” BMJ Open Sport Exercise Medicine 8(4): e001440. 10.1136/bmjsem-2022-001440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Naughton, Mitchell , Jones Ben, Hendricks Sharief, King Doug, Murphy Aron, and Cummins Cloe. 2020. “Quantifying the Collision Dose in Rugby League: A Systematic Review, Meta‐Analysis, and Critical Analysis.” Sports Medicine—Open 6(1): 6. 10.1186/s40798-019-0233-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rugby Football League. New for 2024. https://www.rugby‐league.com/new‐for‐2024 (accessed 31 December 2023).
- O'Brien, William T. , Wright David K., van Emmerik Ashley L. J. J., Bain Jesse, Brkljaca Robert, Christensen Jennaya, Yamakawa Glenn R., et al. 2023. “Serum Neurofilament Light as a Biomarker of Vulnerability to a Second Mild Traumatic Brain Injury.” Translational Research 255: 77–84. 10.1016/j.trsl.2022.11.008. [DOI] [PubMed] [Google Scholar]
- Patricios, Jon S. , Schneider Kathryn J., Dvorak Jiri, Ahmed Osman Hassan, Blauwet Cheri, Cantu Robert C., Davis Gavin A., et al. 2023. “Consensus Statement on Concussion in Sport: The 6th International Conference on Concussion in Sport–Amsterdam, October 2022.” British Journal of Sports Medicine 57(11): 695–711. 10.1136/bjsports-2023-106898. [DOI] [PubMed] [Google Scholar]
- Paul, Lara , Naughton Mitchell, Jones Ben, Davidow Demi, Patel Amir, Lambert Mike, and Hendricks Sharief. 2022. “Quantifying Collision Frequency and Intensity in Rugby Union and Rugby Sevens: A Systematic Review.” Sports Medicine—Open 8(1): 12. 10.1186/s40798-021-00398-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raftery, Martin , Tucker Ross, and Falvey Éanna Cian. 2020. “Getting Tough on Concussion: How Welfare‐Driven Law Change May Improve Player Safety‐A Rugby Union Experience.” British Journal of Sports Medicine 55(10): 527–529. 10.1136/bjsports-2019-101885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rennie, Gordon , Weaving Dan, Hart Brian, Dalton‐Barron Nicholas, and Jones Ben. 2022. “Tackle and Ball Carrier Demands of Rugby League: A Seven‐Year League‐wide Study Including over 1,000,000 Tackle Events.” Journal of Science and Medicine in Sport 25(10): 850–854. 10.1016/j.jsams.2022.07.002. [DOI] [PubMed] [Google Scholar]
- Roe, Gregory , Whitehead Sarah, Starling Lindsay, Allan David, Cross Matt, Falvey Éanna, Kemp Simon, et al. 2024. “Embracing the Impact from Instrumented Mouthguards (iMGs): A Survey of iMG Managers’ Perceptions of Staff and Player Interest into the Technology, Data and Barriers to Use.” European Journal of Sport Science 24(6): 670–681. 10.1002/ejsc.12101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokes, Keith A. , Locke Duncan, Roberts Simon, Henderson Lewis, Tucker Ross, Ryan Dean, and Kemp Simon. 2021. “Does Reducing the Height of the Tackle through Law Change in Elite Men’s Rugby Union (The Championship, England) Reduce the Incidence of Concussion? A Controlled Study in 126 Games.” British Journal of Sports Medicine 55(4): 220–225. 10.1136/bjsports-2019-101557. [DOI] [PubMed] [Google Scholar]
- Tierney, Gregory , Weaving Daniel, Tooby James, Al‐Dawoud Marwan, Hendricks Sharief, Phillips Gemma, Stokes Keith A., Till Kevin, and Jones Ben. 2021. “Quantifying Head Acceleration Exposure via Instrumented Mouthguards (iMG): A Validity and Feasibility Study Protocol to Inform iMG Suitability for the TaCKLE Project.” BMJ Open Sport Exercise Medicine 7(3): e001125. 10.1136/bmjsem-2021-001125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Till, Kevin , Weakley Jonathon, Read Dale B., Phibbs Padraic, Darrall‐Jones Josh, Roe Greg, Chantler Sarah, et al. 2020. “Applied Sport Science for Male Age‐Grade Rugby Union in England.” Sports Medicine—Open 6(1): 14. 10.1186/s40798-020-0236-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tooby, James , Till Kevin, Gardner Andrew, Stokes Keith, Tierney Gregory, Weaving Daniel, Rowson Steve, et al. 2024. “When to Pull the Trigger: Conceptual Considerations for Approximating Head Acceleration Events Using Instrumented Mouthguards.” Sports Medicine 54(6): 1361–1369. 10.1007/s40279-024-02012-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tooby, James , Woodward James, Tucker Ross, Jones Ben, Falvey Éanna, Salmon Danielle, Bussey Melanie Dawn, Starling Lindsay, and Tierney Gregory. 2023. “Instrumented Mouthguards in Elite‐Level Men’s and Women’s Rugby Union: The Incidence and Propensity of Head Acceleration Events in Matches.” Sports Medicine 54(5): 1327–1338: Published Online First. 10.1007/s40279-023-01953-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Tonder, Riaan , Starling Lindsay, Surmon Sean, Viviers Pierre, Kraak Wilbur, Boer P.‐Henk, Jordaan Esme, et al. 2023. “Tackling Sport‐Related Concussion: Effectiveness of Lowering the Maximum Legal Height of the Tackle in Amateur Male Rugby—A Cross‐Sectional Analytical Study.” Injury Prevention 29(1): 56–61. 10.1136/ip-2022-044714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, Timothy , Kenny Rebecca, and Wu Lyndia C.. 2021. “Head Impact Sensor Triggering Bias Introduced by Linear Acceleration Thresholding.” Annals of Biomedical Engineering 49(12): 3189–3199. 10.1007/s10439-021-02868-y. [DOI] [PubMed] [Google Scholar]
- Williams, Sean , Kay Ella, Bryan Richard, Lambert Mark, Cross Matthew, West Stephen W., Kemp Simon, and Stokes Keith A.. 2023. “The Influence of Match Exposure on Injury Risk in Elite Men’s Rugby Union.” Journal of Science and Medicine in Sport 26(1): 25–30. 10.1016/j.jsams.2022.10.016. [DOI] [PubMed] [Google Scholar]
- Williams, Sean , Robertson Charli, Starling Lindsay, McKay Carly, West Stephen, Brown James, and Stokes Keith. 2022. “Injuries in Elite Men’s Rugby Union: An Updated (2012–2020) Meta‐Analysis of 11,620 Match and Training Injuries.” Sports Medicine 52(5): 1127–1140. 10.1007/s40279-021-01603-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams, Sean , Trewartha Grant, Kemp Simon P. T., Brooks John H. M., Fuller Colin W., Taylor Aileen E., Cross Matthew J., Shaddick Gavin, and Stokes Keith A.. 2017. “How Much Rugby Is Too Much? A Seven‐Season Prospective Cohort Study of Match Exposure and Injury Risk in Professional Rugby Union Players.” Sports Medicine 47(11): 2395–2402. 10.1007/s40279-017-0721-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Rugby . World Rugby Integrates Smart Mouthguard Technology to the Head Injury Assessment as Part of New Phase of Global Player Welfare Measures. World Rugby. https://www.world.rugby/news/875212?lang=en (accessed December 31, 2023). [Google Scholar]