

Abstract
Background:
Dermatology lags behind other medical specialties in workforce diversity, particularly regarding gender, race, and ethnicity. This study aims to analyze the current demographics of dermatology physicians in the United States, comparing them with other medical specialties, the overall population of practicing U.S. physicians, and the U.S. population as a whole.
Design and Method:
Data from the Association of American Medical Colleges and the U.S. Census Bureau (2007–2022) were used to evaluate gender, racial, and ethnic diversity within dermatology. Demographic factors analyzed included gender, race, and ethnicity, with racial categories grouped as White, Asian, and underrepresented minorities in medicine (URiM). Chi-square tests assessed the fit of gender and age distributions with population proportions, while linear regression models examined trends over time.
Results:
From 2007 to 2021, the number of dermatologists grew by 22.9%, with a corresponding decrease in population per dermatologist, indicating growth relative to the general population. The proportion of female dermatologists rose by 68.1% during this period, while the male proportion declined by 5.1%. From 2019 to 2022, a significant linear increase (p < 0.001) in URiM representation among dermatology residents was observed, with a model-predicted annual increase of 1.6%.
Conclusions:
The increasing diversity in dermatology may be attributed to initiatives such as scholarships and mentorship programs implemented by dermatology organizations and residency programs. By fostering a more diverse workforce, dermatology can better address the healthcare needs of a diverse population and promote health equity across all demographics.
Keywords: Dermatology, diversity, trends, gender, URiM
Introduction
Facilitating beneficial patient-physician relationships is crucial for healthcare services, and diversity of healthcare providers, in particular, is important for this success. Patients often feel more comfortable discussing their health issues with physicians who share their racial and ethnic background*, as well as their age group1,2; minority patients often prefer physicians of the same race and express greater satisfaction and engagement for their interactions with race-concordant physicians compared to their interactions with race-discordant physicians. 3 For example, Black patients perceive that Black dermatologists have a better understanding of the patients’ skin conditions compared to non-Black dermatologists. 4 This study aims to assess current diversity gaps among dermatology physicians, and to forecast future demographic trajectories. Identifying and understanding these disparities are essential components for policymakers to create a healthcare system that is equitable and effective in meeting the needs of our society.
It is crucial to study the diversity in the physician workforce for several reasons, such as reducing health care disparities, promoting equity, and providing more satisfactory health care services.5,6 In a 2019 report, the Association of American Medical Colleges (AAMC) noted that the medical profession is predominantly White (56.2%) and male (64.1%), contrasting with broader U.S. demographics. 7 Numerous studies highlight gender inequalities in medical professions, emphasizing women’s underrepresentation in leadership positions as a significant concern.8–10 As of December 31st, 2022, among all the U.S. physician workforce 75.3% belongs to the White and Asian race groups while 63.73% of total population representing White and Asians. This implies individuals from demographic groups representing minority ethnic backgrounds, such as Black or African American, Hispanic, Latino or of Spanish Origin, Non-Hispanic, Native Hawaiian/Other Pacific Islander, and others, are disproportionately underrepresented in the medical workforce compared to their population proportions. This cohort of individuals is grouped as Underrepresented Minorities in Medicine, abbreviated as URiM. URiM individuals experience lower promotion rates compared to their White counterparts and are less likely to occupy senior faculty and leadership roles.11–13 Moreover, the impact extends to medical education, where greater representation of URiM individuals among medical school faculty can influence the trajectory of URiM students, leading them to more diverse and inclusive career paths. 14
Dermatology physicians make up a small proportion of the total physician workforce, representing approximately 1% of active physicians in the U.S. as per 2022. 15 However, the demand for dermatology physicians is growing, due to the rising prevalence of skin-related health concerns. Several studies have raised concerns that the demographic makeup of dermatology physicians does not mirror the total population with respect to gender, age, race and ethnicity, and other factors.16–18 A study notes that the disparities between the demographic makeup of dermatology physicians and that of the total population are worsening over time. 3 AAMC data from 2015 highlighted that the entry of trainees from URiM individuals into the dermatology workforce has been minimal. 19 In dermatology, there are fewer program directors from URiM groups than expected for their age group, and the same is true for female program directors. This makes it more challenging for physicians from underrepresented groups to find role models and mentors. 20 A study using U.S. Census Bureau to 2018 revealed that, in academic dermatology, females were underrepresented in higher ranking positions like chairs, professors, and associate professors, but overrepresented in lower ranking positions like instructors and assistant professors. 21 As of 2016, women held 23% of current dermatology chair positions, while among dermatology fellowship program directors, 26% were in dermatologic surgery and 34% in dermatopathology. 22 Additionally, a recent cross-sectional study revealed that, on average, 37% (SD 12%) of editorial board members in leading dermatology journals were women, and only 5 out of 20 journals (25%) had women editors-in-chief. 23 Another study, using data from 1970 to 2018, also suggests that higher-ranking positions in academic dermatology are associated with lower diversity by gender, race, and ethnicity. 24
Enhancing diversity, equity, inclusion, and belonging not only reduces health care inequalities but also leads to patient satisfaction and better outcomes.25,26 To address the disparities in dermatology, it’s crucial for specialty organizations and educational institutions to actively implement equitable practices and inclusive actions. 27 A study using data from 2011 to 2021 found that efforts to increase gender diversity in dermatology have been effective, consistently maintaining female residents in dermatology at above 60%. 28 Lu et al. 21 discussed potential solutions to address barriers in gender, racial and ethnic diversity within academic dermatology. Implementing actions like enhancing URiM representation in residency training, increasing URiM faculty numbers, and establishing an open forum for URiM individuals and women ensures diversity and inclusion in academic dermatology. Recognizing this disparity, collaborative endeavors between national dermatology organizations, dermatology residency programs, and medical schools have been initiated to reduce URiM dermatology physicians within the U.S. healthcare system. 29 To effectively implement measures to increase diversity and reduce underrepresentation among dermatology physicians, we must first gain a clear picture of the current demographic makeup of dermatology physicians. To address this, we examined data from the AAMC and the U.S. Census Bureau to quantify gender, age, racial and ethnic diversity among dermatology physicians in comparison to other specialized areas, to the population of total physicians, and to the population of the United States as a whole. Three action items to increase the presence of URiM certified dermatologists were identified by the American Academy of Dermatology President’s Conference on Diversity in Dermatology. 30 These action items include admitting more URiM students into medical school, generating interest in dermatology programs, and recruiting them into dermatology residency programs.
Methodology
To conduct a comprehensive evaluation of gender, racial and ethnic diversity within the field of dermatology, we collected data from the following sources: the AAMC,31–41 and the U.S. Census Bureau. 42 The Census data set was used to obtain gender, race, and ethnicity data for the U.S. population for the period 2007–2022. The AAMC data sets contained data on gender only for the years 2007, 2010, 2013, 2015, 2017, 2019, and 2021; and data for race and ethnicity for the years 2019–2022. The AAMC data sets encompassed active physicians within the U.S. We analyzed the following demographic factors: specialties (Dermatology, Cardiovascular Disease, General Surgery, Internal Medicine, Obstetrics and Gynecology (OBGYN), Ophthalmology, Pediatrics, Plastic Surgery, or Urology); gender (male, female); and race and ethnicity (White, Asian and URiM). The AAMC defines URiM as racial and ethnic populations that have lower proportional representation in the medical profession compared to their share of the general population. 43 It is noteworthy that in this study, all physicians of races and ethnicities other than Asian and White are collapsed into one group and considered as URiM. The data considered in this study are from physicians actively practicing within the United States, interchangeably referred to as U.S. physicians or active U.S. physicians.
We employed Chi-square tests for goodness of fit to assess whether the age and gender distributions of dermatology physicians in each year matched those of both the active physician population and those of the overall U.S. population for each year available in our datasets. Linear regression models were fitted to examine whether there exist significant trends in dermatology over time for gender, age, race, and ethnicity. A z-test for proportions was used to test for significant differences in the population proportions of females in dermatology compared to other specialized areas. The significance level for all analyses was 0.05. Statistical analyses were conducted with R statistical software (version 4.3.2).
Results
Trends in dermatology by specialized area
Table 1 shows the number of active U.S. physicians of all specialties and the number of active dermatology physicians, both by absolute number and in proportion to the total U.S. population. We observed that the number of dermatology physicians increased by 22.9% between 2007 and 2021, while the proportion of dermatology physicians among all physicians remained constant: dermatologists made up 1.36% of all active physicians in 2007, and 1.34% in 2021. This suggests that it has maintained a consistent presence relative to the total physician population. From 2007 to 2021, there was a decrease in the number of people both per physician and per dermatology physician; this illustrates a growth in both the total number of physicians and total dermatology physicians relative to the total population. This could be influenced by evolving healthcare dynamics or changes in demand within the field of dermatology.
Table 1.
Comparison of total physicians (all specialties) and dermatology physicians, 2007–2021.
| Year | Active U.S. physicians (All specialties) | Active U.S. dermatology physicians | ||
|---|---|---|---|---|
| Count | People per physician | Count | People per physician | |
| 2007 | 764,772 | 395 | 10,390 | 29,030 |
| 2010 | 799,472 | 387 | 10,820 | 28,563 |
| 2013 | 829,962 | 381 | 11,363 | 27,821 |
| 2015 | 860,939 | 373 | 11,706 | 27,458 |
| 2017 | 892,856 | 365 | 12,051 | 27,028 |
| 2019 | 938,980 | 353 | 12,516 | 26,481 |
| 2021 | 949,658 | 344 | 12,767 | 25,579 |
From 2007 to 2021, the number of dermatology physicians grew from 10,390 to 12,767, an increase of 22.9% (Table 1, Figure 1). This rate of growth was higher than that of other specialties: internal medicine and pediatrics, the next fastest growing specialties, grew by only 14.7% and 11.6%, respectively, with plastic surgery, obstetrics and gynecology, and ophthalmology experiencing lower growth. In contrast, general surgery decline by −7%. The distinct positive growth trajectory of dermatology, underscores its pivotal role and rising demand for dermatological expertise, solidifying its position as a dynamic force in the evolving landscape of specialized medical care.
Figure 1.
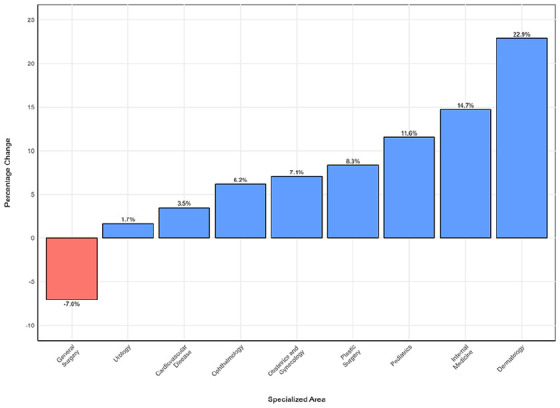
Percent change in the number of physicians in the U.S. by specialized area, 2007–2021.
Trends in dermatology by gender
Female representation among dermatology physicians increased steadily from 3964 (38.2%) in 2007 to 6665 (52.2%) in 2021 (Table 2, Figure 2). The percentage of female physicians in all specialties also increased, though at a slightly slower pace; however, the gap between the percentage of female dermatology physicians and that of total female active physicians has widened over time. During this period, the percentage of females in the overall U.S. population remained constant at around 50%.
Table 2.
Chi-square goodness of fit test results for the comparison of the distribution of female dermatology physicians to both total female population distribution and total female physicians distribution, 2007–2021.
| Year | Active female dermatologists | * |
*
|
||
|---|---|---|---|---|---|
| Expected | p value | Expected | p value | ||
| 2007 | 3964 | 5267 | <0.001 | 2939 | <0.001 |
| 2010 | 4467 | 5497 | <0.001 | 3287 | <0.001 |
| 2013 | 5076 | 5763 | <0.001 | 3701 | <0.001 |
| 2015 | 5514 | 5938 | <0.001 | 3977 | <0.001 |
| 2017 | 5889 | 6111 | <0.001 | 4238 | <0.001 |
| 2019 | 6372 | 6347 | 0.650 | 4539 | <0.001 |
| 2021 | 6665 | 6428 | <0.001 | 4732 | <0.001 |
Note that represents the distribution of female dermatology physicians in the U.S., denotes the distribution of U.S. female population, and refers to distribution of the female physicians in the U.S. Here, and represent the null and alternative hypotheses, respectively.
Figure 2.
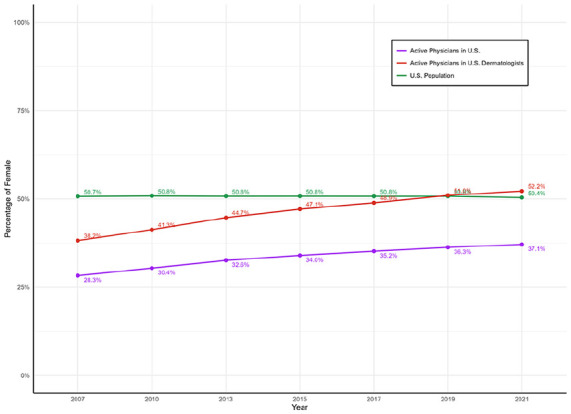
Percentage of female representation among dermatology physicians, total physicians, and total population, 2007–2021.
We employed a chi-square test for goodness of fit to assess the concordance between the percentage of female dermatology physicians and the percentage of both total female physicians and total female population. We found that, at a 95% confidence level, the female representation in dermatology deviates from that of the total population for all years in our data set except 2019 (Table 2, Figure 2). From 2007 to 2017, the proportional share of female dermatologists was significantly lower than the proportion of females in total population, reached parity with it in 2019, and exceeded it in 2021. Similarly, we employed a chi-square test for goodness of fit to examine whether the percentage of female dermatology physicians aligned with the percentage of female physicians. We found that at 95% confidence level, the percentage of female dermatology physicians exceeding that of total physicians in all years. Thus, the gender distribution of U.S. dermatologists significantly differed from that of U.S. physicians over the entire study period.
Figure A1 (see Supplemental Appendix) illustrates the change in number and proportion of both male and female dermatology physicians from 2007 to 2021. The number of male dermatology physicians decreased from 6421 (61.8%) in 2007 to 6091 (47.8%) in 2021, with a significant downward trend (p-value < 0.001). Thus, the proportion of female dermatology physicians increased by 68.1% from 2007 to 2021, while the male proportion decreased by 5.1%. It appears that the growth in the number of dermatology physicians from 2007 to 2021 (2377 net new dermatologists) was due to increasing female representation.
In both 2007 and 2021, pairwise comparison showed that the female proportion of dermatology physicians significantly exceeded the female proportion of all other specialties examined, except for obstetrics and gynecology and pediatrics, at a 5% significance level (Figure A2). In 2007, the percentage of total female physicians as 28.3%, while in 2021 it increased to 37.1%. Thus, for both years, the proportion of female dermatology physicians surpasses that of total female physicians.
Trends in dermatology by racial and ethnic profile
We analyzed the demographics of U.S. dermatology residents from 2019 to 2022 and observed several notable trends. Figure 3 illustrates a declining trend in the percentage of White representation among dermatology residents from 2019 to 2022, while the percentages of Asian and URiM individuals increased during the same time period. The increase from 2019 to 2020 was 15.3% to 16.2%. That’s a rate of increase of 5.9% . This same number from 2021 to 2022 was 16.1% increase, thus the rate of increase almost tripled, and it highlights the representation of URiM is both increasing and accelerating. From 2019 to 2022, we observed a significant linear association (p-value < 0.001) between the percentage values of URiM dermatology residents and year, with the linear regression model indicating a 1.6% increase in URiM representation for each year index.
Figure 3.
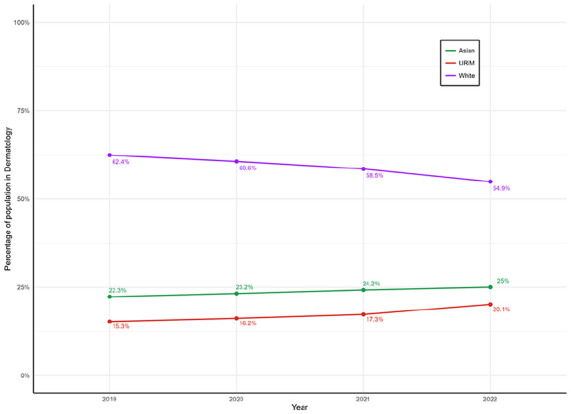
Proportion of population in U.S. dermatology residents by race and ethnicity, 2019–2022.
Figure A3 (see Supplemental Appendix) illustrates URiM representation in active physicians by specialized area from 2019 to 2022. Dermatology is the third lowest specialized area by URiM percentage: URiM individuals are less represented in dermatology compared to most other specialties considered in this study. Among all specialties, ophthalmology had the lowest URiM percentage across all years. Pediatrics exhibited the highest URiM percentage in 2019, which decreased over the next 2 years: in 2022, obstetrics and gynecology exhibited the highest URiM percentage. Recently, the URiM percentage among dermatology physicians surpassed 20%; if this trend continues, dermatology may surpass plastic surgery in URiM percentage.
Discussion
Here, we examine changes in the demographic makeup of dermatology physicians over time and compare this makeup to physicians in other specialized areas, to the total physician population, and to the total U.S. population. The total number of dermatology physicians in the U.S. was 10,390 in 2007 and 12,767 in 2021, representing a percent increase of 22.9%. This illustrates an overall increase in the field of dermatology in the U.S during this time, which also highlights a downward trend in the patient-to-dermatologist ratio over the span of time. Thus, the field of dermatology is increasing both in absolute numbers and in comparison, to the total population. This may be due to the advancement of the field of dermatology through dermatology education and training, 44 or the integration of new technologies, such as tele-dermatology, which increase access to dermatology physicians. 45
It has been demonstrated that there has been a significant increase in the number of female physicians in the U.S. 46 Our study replicates this observation: we found that the percentage of female physicians have consistently risen from 2007 to 2021 across all specialized areas examined. In dermatology specifically, we observed a notable increase in the percentage of female dermatology physicians, from 38.2% in 2007 to 52.2% in 2021. During this period, the percentage of females in the total population remained around 50%. Currently, the gender demographics of dermatology physicians do not match that of the total population, as females are slightly, yet significantly, overrepresented compared to their share of the total population. Though this overrepresentation was only observed in the most recent year of our data set, 2021, given current trends it will likely continue into the future. This likely results from both an increase in the intake of female medical students into the dermatology field, as well as a small net decrease in the number of male dermatology physicians.
From 2019 to 2022, there were fewer dermatology physicians from URiM groups compared to either White or Asian dermatology physicians. Dermatology was notably less representational of the total URiM population compared to other specialized areas; however, dermatology has shown a consistent increase in the proportion of URiM individuals during the time examined, and the rate of increase has also increased each year. It can thus be anticipated that future representation of URiM individuals in dermatology will continue to increase. Several programs47–53 have been implemented to increase the URiM representation in dermatology. For example, The American Academy of Dermatology (AAD) and American Academy of Dermatology Association (AADA), in partnership with pharmaceutical companies, is introducing Pathways: Inclusivity in Dermatology. This program aims to boost the number of dermatologists in the U.S. from URiM communities. 47 Moreover, a one-on-one mentorship program is provided by the AADA. This one-on-one mentorship program pairs volunteer mentors with medical students to provide hands-on exposure in the field of dermatology, while also encouraging interest in dermatology as an attainable career path. 54 The Skin of Color Society is a nonprofit organization that promotes education, mentorship and advocacy committed to increasing diversity and inclusion in the field of dermatology to improve patient care. 55
Limitations
A major issue of this study is also that we are lumping all Asians together as one group, when in fact there are different populations and origins among Asians. Several of them, for example, Among and other Southeast Asians, experience healthcare disparities and are also underrepresented. This is a gap and shortcoming in our classification that is well recognized by Federal agencies. Furthermore, the AAMC data that was used for our analysis includes only the years 2007, 2010, 2013, 2015, 2017, 2019, and 2021, and thus does not contain data for all the years from 2007 to 2021.
Conclusion
The decline in the ratio of dermatology physicians to the total population reflects consistent growth within the field of dermatology in the United States. In dermatology, both female and URiM representation have risen significantly. Although URiM remain underrepresented compared to White and Asian dermatologists, this gap has been reduced over time, suggesting that representation from females and URiM individuals will continue to increase. Efforts, including scholarships, mentorship programs, and leadership training, have been implemented to enhance diversity, equity, and inclusion in dermatology, and have shown some success. Despite these initiatives, dermatology remains one of the least diverse medical fields, indicating the necessity for ongoing efforts to achieve sustained progress in diversifying the dermatology workforce.
Supplemental Material
Supplemental material, sj-docx-1-phj-10.1177_22799036241293815 for Analyzing diversity trends in dermatology: A comprehensive overview by Michael Mayo, Isuru Ratnayake, Sam Pepper, Mohammod Mahmudur Rahman, Md. Robiul Islam Talukder, Matthew McGuirk, Joshua Martinez, Adela Rambi Cardones, Jo Wick and Dinesh Pal Mudaranthakam in Journal of Public Health Research
Footnotes
Abbreviations: URiM: Underrepresented minorities in medicine
AAMC: Association of American Medical Colleges
OBGYN: Obstetrics and Gynecology
AAD: The American Academy of Dermatology
AADA: American Academy of Dermatology Association
NIH: National Institutes of Health
Data availability: The study uses publicly available data from the Association of American Medical Colleges (AAMC) and U.S. Census Bureau. Data sharing is available upon request.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs: Isuru Ratnayake  https://orcid.org/0000-0001-9596-781X
https://orcid.org/0000-0001-9596-781X
Mohammod Mahmudur Rahman
https://orcid.org/0009-0000-4659-9299
Supplemental material: Supplemental material for this article is available online.
References
- 1. Cooper-Patrick L, Gallo JJ, Gonzales JJ, et al. Race, gender, and partnership in the patient-physician relationship. JAMA 1999; 282(6): 583–589. [DOI] [PubMed] [Google Scholar]
- 2. García JA, Paterniti DA, Romano PS, et al. Patient preferences for physician characteristics in university-based primary care clinics. Ethn Dis 2003; 13(2): 259–267. https://www.jstor.org/stable/48666301. [PubMed] [Google Scholar]
- 3. Pandya AG, Alexis AF, Berger TG, et al. Increasing racial and ethnic diversity in dermatology: a call to action. J Am Acad Dermatol 2016; 74(3): 584–587. [DOI] [PubMed] [Google Scholar]
- 4. Gorbatenko-Roth K, Prose N, Kundu RV, et al. Assessment of black patients’ perception of their dermatology care. JAMA Dermatol 2019; 155(10): 1129–1134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Cohen JJ, Gabriel BA, Terrell C. The case for diversity in the health care workforce. Health Aff 2002; 21(5): 90–102. [DOI] [PubMed] [Google Scholar]
- 6. Institute of Medicine (US). Committee on institutional and policy-level strategies for increasing the diversity of the U.S. healthcare workforce. In: Bristow LR, Butler AS, Smedley BD. (eds.) In the nation’s compelling interest: ensuring diversity in the health-care workforce. Washington, DC: The National Academies Press, 2004. [PubMed] [Google Scholar]
- 7. Association of American Medical Colleges. Diversity in medicine: facts and figures 2019, 2019. https://www.aamc.org/data-reports/workforce/report/diversity-medicine-facts-and-figures-2019.
- 8. Glauser W. Rise of women in medicine not matched by leadership roles. CMAJ 2018; 190(15): E479–E480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Covington EL, Moran JM, Paradis KC. The state of gender diversity in medical physics. Med Phys 2020; 47(4): 2038–2043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Jena AB, Khullar D, Ho O, et al. Sex differences in academic rank in U.S. medical schools in 2014. JAMA 2015; 314(11): 1149–1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Mahoney MR, Wilson E, Odom KL, et al. Minority faculty voices on diversity in academic medicine: perspectives from one school. Acad Med 2008; 83(8): 781–786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rosenkranz KM, Arora TK, Termuhlen PM, et al. Diversity, equity and inclusion in medicine: why it matters and how do we achieve it? J Surg Educ 2021; 78(4): 1058–1065. Epub ahead of print 3 December 2020. DOI: 10.1016/j.jsurg.2020.11.013. [DOI] [PubMed] [Google Scholar]
- 13. Ajayi AA, Rodriguez F, de Jesus Perez V. Prioritizing equity and diversity in academic medicine faculty recruitment and retention. JAMA Heal Forum 2021; 2(9): e212426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Nguemeni Tiako MJ, Ray V, South EC. Medical schools as racialized organizations: how race-neutral structures sustain racial inequality in medical education—a narrative review. J Gen Intern Med 2022; 37(9): 2259–2266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Association of American Medical Colleges. Physician Specialty Data Report. AAMC, n.d. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 16. Lester J, Wintroub B, Linos E. Disparities in academic dermatology. JAMA Dermatol 2016; 152(8): 878–879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Gao Y, Fulk T, Mori W, et al. Diversity and career goals of graduating allopathic medical students pursuing careers in dermatology. JAMA Dermatol 2023; 159(1): 47. Published online 16 November 2022. DOI: 10.1001/jamadermatol.2022.4984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Williams JC, Valladares HC, Waul MA, et al. 15-Year diversity trends among dermatology resident trainees compared with other specialties. JAMA Dermatol 2023; 159(1): 104–106. Published online 16 November 2022. DOI: 10.1001/jamadermatol.2022.4991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Van Voorhees AS, Enos CW. Diversity in dermatology residency programs. J Investig Dermatol Symp Proc 2017; 18(2): S46–S49. [DOI] [PubMed] [Google Scholar]
- 20. Verschoore M, Sarkar R, Gupta M. Women leadership in dermatology: moving towards gender equality. Indian Dermatol Online J 2022; 13(1): 3–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lu JD, Tiwana S, Das P, et al. Gender and racial underrepresentation in academic dermatology positions in the United States: a retrospective, cross-sectional study from 2007 to 2018. J Am Acad Dermatol 2020; 83(5): 1513–1516. [DOI] [PubMed] [Google Scholar]
- 22. Nambudiri VE, Shi CR, Vleugels RA, et al. Academic dermatology leadership in the United States – addressing the gender gap. Int J Womens Dermatol 2018; 4(4): 236–237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Szeto MD, Sivesind TE, Kim LS, et al. Gender parity analysis of the editorial boards of influential dermatology journals: cross-sectional study. JMIR Dermatol 2024; 7: e40819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Xierali IM, Nivet MA, Pandya AG. US dermatology department faculty diversity trends by sex and underrepresented-in-medicine status, 1970 to 2018. JAMA Dermatol 2020; 156(3): 280–287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Swartz TH, Palermo AS, Masur SK, et al. The science and value of diversity: closing the gaps in our understanding of inclusion and diversity. J Infect Dis 2019; 220(220 Suppl 2): S33–S41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Gomez LE, Bernet P. Diversity improves performance and outcomes. J Natl Med Assoc 2019; 111(4): 383–392. [DOI] [PubMed] [Google Scholar]
- 27. Mason BS, Heath C, Parker J, et al. Diversity, equity, inclusion and belonging in dermatology. Dermatol Clin 2023; 41(2): 239–248. [DOI] [PubMed] [Google Scholar]
- 28. Okorie CL, Elkady D, Nambudiri VE. Trends in sex and ethnicity among U.S. dermatopathology and Mohs surgery trainees: 2011-2021. Arch Dermatol Res 2023; 315(8): 2471–2473. [DOI] [PubMed] [Google Scholar]
- 29. Akhiyat S, Cardwell L, Sokumbi O. Why dermatology is the second least diverse specialty in medicine: how did we get here? Clin Dermatol 2020; 38(3): 310–315. [DOI] [PubMed] [Google Scholar]
- 30. Pritchett EN, Park AJ, Vasquez R. Contextualizing the landscape of diversity, equity, and inclusion in dermatology. JAMA Dermatol 2023; 159(1): 19–21. [DOI] [PubMed] [Google Scholar]
- 31. 2008 Physician Specialty Data Center for Workforce Studies . Association of American Medical Colleges, 2008. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 32. 2012 Physician Specialty Data Book Center for Workforce Studies . Association of American Medical Colleges, 2012. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 33. 2014 Physician Specialty Data Book Center for Workforce Studies . Association of American Medical Colleges, 2014. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 34. 2016 Physician Specialty Data Report . Association of American Medical Colleges, 2016. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 35. 2018 Physician Specialty Data Report . Association of American Medical Colleges, 2018. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 36. 2020 Physician Specialty Data Report . Association of American Medical Colleges, 2020. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 37. 2022 Physician Specialty Data Report . Association of American Medical Colleges, 2022. https://www.aamc.org/data-reports/workforce/report/physician-specialty-data-report.
- 38. Association of American Medical Colleges. Table B-5: M.D. Residents by Race, Ethnicity, and Specialty, 2020. https://www.aamc.org/data-reports/students-residents/data/report-residents/2020/table-b5-md-residents-race-ethnicity-and-specialty.
- 39. Association of American Medical Colleges. Table B-5: M.D. Residents by Race, Ethnicity, and Specialty, 2021. https://www.aamc.org/data-reports/students-residents/data/report-residents/2021/table-b5-md-residents-race-ethnicity-and-specialty.
- 40. Association of American Medical Colleges. Table B-5: M.D. Residents by Race, Ethnicity, and Specialty, 2022. https://www.aamc.org/data-reports/students-residents/data/report-residents/2022/table-b5-md-residents-race-ethnicity-and-specialty.
- 41. Association of American Medical Colleges. Table B-5: M.D. Residents by Race, Ethnicity, and Specialty, 2023. https://www.aamc.org/data-reports/students-residents/data/report-residents/2023/table-b5-md-residents-race-ethnicity-and-specialty.
- 42. U.S. Census. Bureau. American Community Survey, 2019. 5-Year Estimates. https://data.census.gov.
- 43. Association of American Medical Colleges. Underrepresented in Medicine, n.d. https://www.aamc.org/what-we-do/equity-diversity-inclusion/underrepresented-in-medicine.
- 44. Byrne-Davis L, Cohen SN, Turner RR. Evaluating dermatology education and training. Clin Exp Dermatol 2022; 47(12): 2096–2099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Glines KR, Haidari W, Ramani L, et al. Digital future of dermatology. Dermatol Online J 2020; 26(10): 13030/qt75p7q57j. 10.5070/D32610050455. [DOI] [PubMed] [Google Scholar]
- 46. Boyle P. Nation’s physician workforce evolves: more women, bit older, and toward different specialties, 2 February 2021. https://www.aamc.org/news/nation-s-physician-workforce-evolves-more-women-bit-older-and-toward-different-specialties.
- 47. American Academy of Dermatology. Pathways: Inclusivity in Dermatology, n.d. https://www.aad.org/member/career/diversity/pathways.
- 48. Pino-Jones AD, Cervantes L, Flores S, et al. Advancing diversity, equity, and inclusion in hospital medicine. J Hosp Med 2021; 16(4): 198–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Lopez S, Lourido JO, Lim HW, et al. The call to action to increase racial and ethnic diversity in dermatology: a retrospective, cross-sectional study to monitor progress. J Am Acad Dermatol 2022; 86(3): e121–e123. [DOI] [PubMed] [Google Scholar]
- 50. Rice X, Uzoma B, Hoyer P. Addressing diversity in dermatology: implementation of formalized allyship. J Am Acad Dermatol 2022; 86(6): e275–e276. [DOI] [PubMed] [Google Scholar]
- 51. Handfield C, Anderson K, Wyles S. Strategies for equity-driven practice advancement in dermatology. Int J Dermatol 2023; 62(8): 1094–1095. [DOI] [PubMed] [Google Scholar]
- 52. Beer J, Heningburg J, Downie J, et al. Diversity in academic dermatology. J Drugs Dermatol 2022; 21(6): 674–676. [DOI] [PubMed] [Google Scholar]
- 53. Kiene J, Minion S, Rodriguez R, et al. Diversity, equity, and inclusion of dermatology journals and their editorial board members. JMIR Dermatol 2023; 6: e44217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Diversity mentorship program: Information for mentors . American Academy of Dermatology, 2024. https://www.aad.org/member/career/li/mentor/diversity.
- 55. Mentorship . Mentorship - Skin of Color Society, 2024. https://skinofcolorsociety.org/what-we-do/mentorship.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-phj-10.1177_22799036241293815 for Analyzing diversity trends in dermatology: A comprehensive overview by Michael Mayo, Isuru Ratnayake, Sam Pepper, Mohammod Mahmudur Rahman, Md. Robiul Islam Talukder, Matthew McGuirk, Joshua Martinez, Adela Rambi Cardones, Jo Wick and Dinesh Pal Mudaranthakam in Journal of Public Health Research