

Abstract
Background and Objectives
Hearing loss is the largest potentially modifiable risk factor for dementia. Early evaluation and intervention are crucial for older adults with cognitive impairment. However, pure-tone audiometry (PTA), the gold standard, may have limitations. This study reviewed auditory tests for detecting hearing loss in this population, comparing to PTA.
Materials and Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we conducted a systematic review in PubMed, Scopus, and Embase. Ten studies (1,071 participants) comparing auditory tests and PTA in patients with dementia and mild cognitive impairment were included.
Results
Electrophysiological and behavioral tests demonstrated strong correlation and accurate hearing impairment detection compared to PTA. Conversely, self-reported assessment showed weaker correlations when aligned with hearing thresholds.
Conclusions
This study highlights the potential of electrophysiological and behavioral auditory tests in detecting hearing impairment in older adults with cognitive impairment, emphasizing the need for further research to develop practical screening protocols for this vulnerable population.
Keywords: Hearing loss, Cognitive impairment, Hearing screening, Audiometry, Dementia
Introduction
Nowadays, the population trend has shifted toward an aging society. Dementia, a neurocognitive disorder with acquired loss of cognitive abilities in at least one domain and impaired functional abilities with varying manifestations and etiologies, is one of the leading causes of disability in the older adult population, affecting their physical, emotional, social, as well as placing an enormous economic burden on the society as a whole [1]. Despite the fact that there is no cure for dementia at present, there are efforts to prevent the disease, decrease its symptoms, and slow its progression by minimizing its risk factors [2]. Among the known risk factors, hearing impairment is regarded as the largest potentially modifiable risk factor [3,4] with a 1.9-fold relative risk for dementia [4]. A recent randomized controlled trial demonstrated the positive effect of hearing aid usage in individuals at risk of cognitive impairment, reducing the risk of cognitive decline compared to those without hearing aid use [5]. The findings of this trial are supported by meta-analysis, which also showed that hearing aid use has been associated with both short- and long-term improvements in cognition, including cognitive tests as well as longer term changes in cognition [6]. In the realm of tertiary prevention, the restoration of auditory input by hearing intervention led to increased social stimulation and decreased cognitive load and indirectly affected cognition through sensory deprivation and information degradation hypotheses [7]. Recent studies showed that treating hearing loss in cognitively impaired patients improves their dementia related-behavioral symptoms, communication, and quality of life [8-10]. Therefore, the necessity of adopting hearing interventions has been emphasized over many years.
Nevertheless, the assessment of hearing thresholds, a crucial step in the overall process, is problematic for those with deteriorating cognitive capacities. Pure-tone audiometry (PTA), a behavioral measurement of hearing threshold in which the patient responds to sound stimuli via headphones at each frequency under controlled ambient noise [11], is currently the gold standard for testing hearing levels. This procedure is relatively complex and necessitates patient cooperation. A recent study offers strategies, based on the author’s clinical experience, for modifying standard audiometry to assist in determining hearing thresholds in individuals with dementia [12]. Moreover, the test-retest reliability of hearing measures obtained from participants with mild dementia was comparable to that obtained from cognitively normal participants, according to a previous study [13]. However, a prior systematic review reported that only 56% to 59% of individuals with dementia can complete PTA [14]. Therefore, PTA may not be applicable for certain patient populations [11], such as those with varied severity of dementia. Furthermore, conventional PTA is not readily available in every setting because of expensive equipment expenses and the requirement for well-trained medical personnel. Diagnosing hearing loss for individuals with impaired cognition is an important barrier that still needs to be overcome.
As advocated by recent international practice recommendations [15], attempts have been made to discover a more accessible, pragmatic, precise, and rapid screening method as an alternative to traditional audiometry for recognizing hearing problems in this population. Several studies comparing the outcome of hearing tests administered to older adults with cognitive impairment to the gold standard have been published during the past several years. Accordingly, the purpose of this literature review was to consolidate and analyze publications about auditory tests in patients with dementia or mild cognitive impairment (MCI), with the emphasis on diagnostic performance relative to PTA.
Materials and Methods
This review was carried out according to Preferred reporting items for systematic review and meta-analyses (PRISMA) statement [16]. The PICO was defined as follows. Patients (P) were older adults who were diagnosed with MCI or dementia (any type and severity). Intervention (I) was auditory tests. Comparison (C) was PTA, and outcome (O) was hearing impairment. The protocol was registered on PROSPERO (CRD42021273537).
Search strategy
A systematic literature search was performed to identify all publications from inception to September 16, 2021, via PubMed, Scopus, and Embase. The search was updated on November 21, 2023. To ascertain articles about screening hearing loss and cognitive impairment, we used the search strategy that developed by combination of free text terms and MeSH term. The complete search strategy was attached in Supplementary Table 1 in the online-only Data Supplement. The citation of included full-text articles were reviewed for additional relevant studies.
Study selection
Studies with individual data for comparing the performance of hearing tests and PTA were included. Exclusion criteria included foreign-language studies without English translation available, irrelevant studies according to the study PICO, and studies with insufficient data. In addition, review articles, letters/commentaries, abstracts, conference proceedings, and nonobtainable full-text studies were excluded. Results were exported into and implemented on Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) for the review process.
After removing duplicates, two independent reviewers (PL and PJ) conducted a screening of title and abstract, followed by full-text articles considered relevant. Any discrepancies were resolved by a third reviewer (NU).
Data extraction and quality assessment
The study title, author, location, publication year, participants (such as baseline characteristics and diagnosis), and hearing evaluation methods were all extracted from each article. All study findings, the diagnostic performance and accuracy of hearing threshold when comparing hearing tests and PTA, e.g., correlation coefficients, regression coefficients, sensitivity, and specificity were summarized. We used Quality Assessment of Diagnostic Accuracy-2 (QUADAS-2) [17] to assess the methodological quality of studies included in the review.
Results
Our search strategy yielded 2,382 results, of which 756 were removed as duplicates. After a screening of the titles and abstracts, 1,574 articles were excluded. Full texts of 52 papers were obtained and 8 matched the inclusion criteria and were included in this review. Through the reference list of the included papers, 2 additional studies were identified (Fig. 1). A total of 10 studies were included in this review, including 3 studies that used electrophysiological tests [18-20] and 2 studies that used behavioral tests [21,22]. Five studies utilized self-perceived hearing questionnaires [23-27], with 3 providing data assessing caregivers [23,26,27]. The characteristics and key findings of the included studies are summarized in Tables 1-3.
Fig. 1.
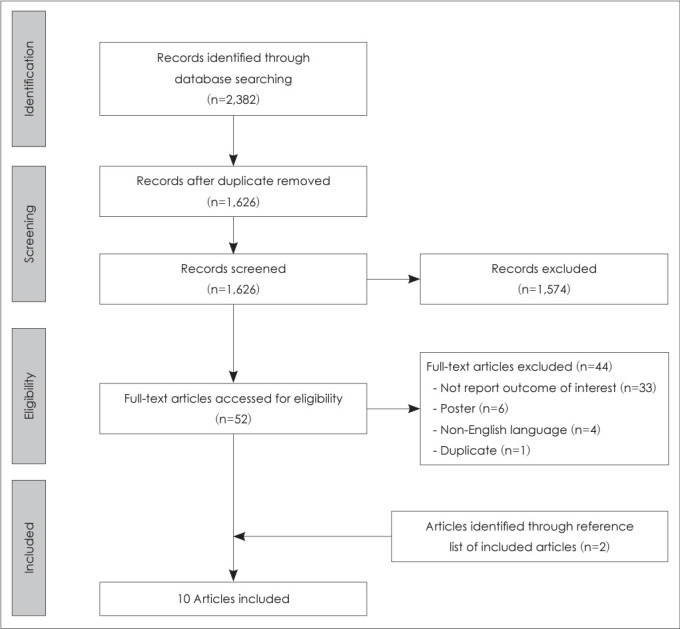
PRISMA flow diagram for inclusion and exclusion of studies.
Table 1.
Characteristics and findings of included studies using electrophysiological hearing tests
| Study | Sample | Criteria diagnosis for cognitive impairment | Auditory test | Results |
|---|---|---|---|---|
| Villeneuve, et al. [18] | 12 Patients (23 ears): 8 AD and 4 MCI; Mean age 82.1 yrs; Mean MMSE 21.3 | - AD: the American National Institute on Aging and the Alzheimer’s Association | Auditory steady-state response (ASSR) | A significant correlation (p<0.05) between pure-tone average and estimated ASSR thresholds for all frequencies (r=0.55, p=0.006 for 500 Hz; r=0.58, p=0.005 for 1,000 Hz; r=0.61, p=0.003 for 2,000 Hz; r=0.66, p=0.002 for 4,000 Hz) |
| - MCI: the Peterson’s criteria | ||||
| Gates, et al. [19] | 42 Patients (probable AD): 22 with CDR score of 0.5 and 20 with CDR score of 1; Mean age 76 yrs for CDR 0.5 and 78.3 y for CDR 1 | Probable AD: clinical diagnostic criteria of AD | - Distortion-product otoacoustic emissions (DPOE) | The regression of pure-tone average on DPOE threshold was significant for all frequencies, strongest for 2,000 Hz (r2=0.45 and 0.68 for right ear and left ear, respectively), no significant differences across the CDR group. The ABR thresholds were within 10 dB to 20 dB of the behavioral pure-tone thresholds and did not vary by age, gender, ear, or CDR group |
| - Auditory brainstem response (ABR) | ||||
| Bott, et al. [20] | 6 Patients: 1 questionable, 1 mild, and 4 moderate dementia; Mean age 85 yrs | No information about criteria diagnosis | Cortical automatic threshold estimation (CATE) | Strong significant correlations between CATE and pure-tone average threshold for all frequencies (r2=0.52, p=0.008 for 500 Hz; r2=0.79, p=0.0001 for 1,000 Hz; r2=0.71, p=0.0005 for 2,000 Hz; r2=0.92, p<0.0001 for 4,000 Hz) |
AD, Alzheimer’s disease; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; CDR, Clinical Dementia Rating
The included studies were published between 1989 and 2022. Four of the 10 articles were conducted in the United States [19,21,23,27], 2 in Canada [22,26], and 1 each in the UK [25], Australia [20], France [18], and South Korea [24]. Four out of the 10 studies were cross-sectional, 3 were case-control, 2 was prospective, and 1 was retrospective. Most studies (6/10) recruited participants from memory clinic/program, while 2 studies recruited residents from long term care, 1 involved adult medicine clinic-based samples, and 1 was a cohort study representing communities. The sample size varied between 6 and 801 individuals. Among a total of 1,071 patients, 690 were diagnosed with MCI and 381 with dementia of any type.
Three studies have reported the correlation between the estimated hearing threshold level obtained from hearing tests and PTA [18-20]. The correlation between questionnaire scores and pure-tone average obtained from audiometry was documented in 2 studies [24,25]. Four studies provided estimates of diagnostic accuracy (sensitivity, specificity, positive predictive value, and negative predictive value) [21-23,27], with 1 study presenting raw data in a table [23]. In 1 study, the interclass correlation between hearing rating and PTA was reported to establish the reliability of the test [26]. Rendering a meta-analysis was considered inappropriate in light of the considerable heterogeneity across studies on the basis of hearing measurement methods and reported outcomes.
Quality of studies
All studies were evaluated for risk of bias and applicability, in the domains of patient selection, index test, reference test, and flow and timing, according to QUADAS-2 tool. For the evaluation of risk of bias, 2 studies [25,26] included patients with documented hearing loss, while 1 excluded [24]. Consequently, there was high concern regarding their applicability of patient selection. Except for 2 studies [21,22], most of the studies did not address the sequence of index and reference tests. Four studies [19,20,23,26] had missing data on the analysis and were rated as high risk within the flow and timing domain. Risk of bias for individual studies and summary plot according to QUADAS-2 are presented in Table 4 and Fig. 2.
Table 4.
Quality assessment of enrolled studies using QUADAS-2
| Study | Risk of bias |
Applicability concerns |
|||||
|---|---|---|---|---|---|---|---|
| Patient selection | Index test | Reference standard | Flow and timing | Patient selection | Index test | Reference standard | |
| Villeneuve, et al. [18] |

|
|
|

|
|
|
|
| Gates, et al. [19] |

|
|
|
|
|
|
|
| Bott, et al. [20] |
|
|
|
|
|
|
|
| Uhlmann, et al. [21] |
|
|
|
|
|
|
|
| Frank, et al. [22] |
|
|
|
|
|
|
|
| Gold, et al. [23] |
|
|
|
|
|
|
|
| Lee, et al. [24] |
|
|
|
|
|
|
|
| Utoomprurkporn, et al. [25] |
|
|
|
|
|
|
|
| Hopper, et al. [26] |
|
|
|
|
|
|
|
| Kim, et al. [27] |
|
|
|
|
|
|
|
low risk; high risk; unclear risk
Fig. 2.

Overall risk of bias and applicability concern on the QUADAS-2 tool of the enrolled studies.
Electrophysiological hearing tests and PTA
There were 3 studies that compared hearing threshold levels from PTA to various electrophysiological measurements (Table 1). One prospective study performed auditory steady state response (ASSR)—an auditory evoked potential (AEP) that can be used to objectively estimate hearing sensitivity in individuals [28]—in patients with MCI and Alzheimer’s disease [18]. A significant correlation (p<0.05) between PTA and estimated ASSR thresholds were found for all frequencies: r=0.55, p=0.006 for 500 Hz; r=0.58, p=0.005 for 1,000 Hz; r=0.61, p=0.003 for 2,000 Hz; and r=0.66, p=0.002 for 4,000 Hz. Notably, there was no correlation between the Mini-Mental State Examination (MMSE) score and the discrepancies between ASSR and PTA thresholds for any frequency.
Another study used cortical automatic threshold estimation (CATE) [20], a type of AEP, for assessing demented and also noticed substantial significant correlations between CATE and PTA threshold for all frequencies (r2=0.52, p=0.008 for 500 Hz; r2=0.79, p=0.0001 for 1,000 Hz; r2=0.71, p=0.0005 for 2,000 Hz; r2=0.92, p<0.0001 for 4,000 Hz). Notably, the sample size was relatively limited (n=6) due to the exclusion of participants who did not complete the PTA or CATE for a variety of reasons (refusal to wear headphones/electrodes, desire to quit due to lengthy procedure, inability to follow PTA instructions).
Distortion-product otoacoustic emissions (DPOE) was used in 1 cross-sectional study [19]. The regression of PTA on DPOE threshold was significant for all frequencies with the strongest at 2,000 Hz (r2=0.45 and 0.68 for right ear and left ear, respectively), and there was no significant difference between subgroups 0.5 and 1 on the Clinical Dementia Rating (CDR) scale. When auditory brainstem response (ABR) testing was done, the ABR thresholds were within 10 dB to 20 dB of the pure-tone thresholds and were independent of age, gender, ear, and CDR groups.
Behavioral hearing tests and PTA
Two studies evaluated the diagnostic accuracy of behavioral hearing tests to the gold standard (Table 2). In 1 study, the performance of several physical examination batteries and air conduction screening audiometry for screening hearing loss (defined as pure-tone average 40 dB HL from the speech frequencies 0.5, 1, 2, and 3 kHz) in patients with mild to moderate dementia was investigated [21]. All screening tools exhibited exceptional performance. The tuning fork-512 Hz and -1,024 Hz, finger rub, and whispered voice tests had respective specificity of 0.53, 0.63, 0.85, and 0.78 when sensitivity for detecting 40-dB hearing loss was 0.9. The specificity was greater when the sensitivity was lower at 0.8. (0.82, 0.95, 0.95, and 0.89 for tuning fork-512 Hz and 1,024 Hz, finger rub, and whispered voice tests, respectively). The air-conduction screening test had a high sensitivity (1.0) for the inability to hear one or more tones, but low specificity (0.50). Whereas for failure to hear 3 of 4 tones, specificity was higher (0.97), but sensitivity was lower (0.70). The receiver operative characteristic (ROC) curve areas were excellent results for all modalities (0.85, 0.92, 0.94, 0.94, and 0.95 for tuning fork-512 Hz, tuning fork-1,024 Hz, finger rub, whispered voice tests, and air conduction screening audiometry, respectively). Notably, interobserver/test-retest reliability was moderate to high (intraclass correlation coefficient 0.58–0.90) through all screening tests.
Table 2.
Characteristics and findings of included studies using behavioral hearing tests
| Study | Sample | Criteria diagnosis for cognitive impairment | Auditory test | Results |
|---|---|---|---|---|
| Uhlmann, et al. [21] | 34 Patients (probable AD); Mean age 76.1 yrs | Probable AD: The clinical diagnostic criteria for AD (“probable” classification) | - 512-Hz and 1,024-Hz tuning fork | ROC curve areas for tuning fork-512 Hz, tuning fork-1,024 Hz, finger rub, whispered voice tests, and air conduction screening audiometry were 0.85, 0.92, 0.94, 0.94, and 0.95, respectively |
| - Finger rub | ||||
| - Whispered voice test | ||||
| - Air conduction screening audiometry | ||||
| Frank, et al. [22] | 25 Patients: 19 MCI and 6 mild dementia; Mean age 73.84 yrs | No information about criteria diagnosis | iPad-based SHOEBOX QuickTest hearing screener | Sensitivity 100%, specificity 66.7%, PPV 76% (95% CI 59%-88%), NPV 100%, accuracy 84% (hearing loss was defined as pure-tone average threshold >30 dB) |
AD, Alzheimer’s disease; MCI, mild cognitive impairment; PPV, positive predictive value; NPV, negative predictive value; CI, confidence interval; ROC, receiver operating characteristic
Another study adopted newly designed hearing screening equipment to examine patients with MCI and mild dementia [22]. The SHOEBOX QuickTest application consists of two components: a set of 4 questions accompanied by presentations of pure tones at 1, 2, and 4 kHz. Hearing disability was defined as threshold from conventional pure-tone average >30 dB. The iPad-based screening test demonstrated an overall accuracy of 84%, with a sensitivity of 100% and a specificity of 66.7%. Positive predictive value was 76% (95% confidence interval [CI] 59%–88%) while negative predictive value was 100%. Additionaly, 72% (95% CI 60.0%–84.1%) of conventional audiometry thresholds fell within the 10 dB range of the SHOEBOX QuickTest. Notably, 72% of patients were able to finish the exam on the first attempt, while just 12% required 3 attempts because they did not reply quickly enough or did not comprehend the task on the first effort.
Self-perceived hearing assessments and PTA
Five studies assess the hearing of older adults with cognitive impairment by questionnaire (Table 3). Of these, 2 studies used Hearing Handicap Inventory for Elderly (HHIE), the effective screening self-reported questionnaire for identifying hearing impairment in older adults [29,30]. One study enrolling 46 MCI patients used a validated Korean version of HHIE [31] and found a weak, nonsignificant correlation between total K-HHIE score and PTA (r=0.260 [95% CI -0.030, 0.548], p>0.05) [24]. The outcomes were identical when categorizing MCI patients into with and without frontal-executive dysfunction (FED) subgroups (r=0.105 and r=0.083 with p>0.05 for MCI with and without FED, respectively). Interestingly, a substantial correlation was discovered in normal cognition group (r= 0.335, p<0.05).
Table 3.
Characteristics and findings of included studies using self-perceived hearing assessment
| Study | Sample | Criteria diagnosis for cognitive impairment | Auditory test | Results |
|---|---|---|---|---|
| Gold, et al. [23] | 52 Patients: 30 probable AD with mean MMSE 18.2 (Group 1) and 22 other forms of cognitive impairment with mean MMSE 22.9 (Group 2); mean age 77.2 yrs for group 1 and 75.5 yrs for group 2 | Probable AD: The criteria of the National Institute of Neurological and Communicative Disorder Association | Hearing Handicap Inventory for Elderly-screening version (HHIE) | For self-patient assessment (HHIE-S), sensitivity 30.4%, specificity 100%, PPV 100%, NPV 8.6%, accuracy 34.7% |
| For caregiver assessment (HHIE-SP), sensitivity 42.4%, specificity 100%, PPV 100%, NPV 13.6%, accuracy 47.2% (Values were calculated from raw data when failure was defined as: 1) pure-tone average >40 dB, 2) HHIE score >18, or 3) a passing score (<18) on the HHIE and no response to a 25 dB HL pure tone) | ||||
| Lee, et al. [24] | 46 MCI patients: 15 MCI with FED with mean K-MMSE 25, and 30 MCI without FED with mean K-MMSE 26; Mean age 66.56 yrs for MCI with FED and 68.56 yrs for MCI without FED | MCI: the Peterson’s criteria | Korean version of Hearing Handicap Inventory for the Elderly (K-HHIE) | For total MCI patients, adjusted correlation analysis by depression levels showed a weak positive, nonsignificant correlation between K-HHIE score and pure-tone average (Spearman’s rho=0.260 [95% CI -0.03, 0.548]) |
| Utoomprurkporn, et al. [25] | 28 Patients: 13 MCI with hearing impairment (mean MoCA-HA 22.03), 15 dementia with hearing impairment (mean MoCA-HA 15.20); Mean age 83.8 and 80.8 yrs for MCI and dementia group, respectively | MCI: ICD-10 criteria | - The modified Amsterdam Inventory for Auditory Disability (mAIAD) | Weak and nonsignificant correlations were found between the overall mAIAD score and pure-tone average (r=-0.24, p=0.197 and r=-0.50, p=0.069 for MCI and dementia group, respectively) |
| Dementia: ICD-10 criteria | - The Speech, Spatial and Qualities of Hearing Scale (SSQ) | Weaker and nonsignificant correlations were found between the overall SSQ score and pure-tone average (r=-0.19,p=0.321 and r=-0.37, p=0.169 for MCI and dementia group, respectively) | ||
| Hopper, et al. [26] | 25 Dementia: Long term care resident-based | No information about criteria diagnosis | Resident Assessment Instrument– Minimum Data Set 2.0 (RAI-MDS) by health care staff | A weak, significant intraclass correlation coefficient was found between pure-tone average category and the RAI-MDS rating (r=0.286, p=0.015) |
| Kim, et al. [27] | - 801 Self-rated assessment: 608 MCI (mean age 80.4 yrs), 193 dementia (mean age 82.7 yrs) | No information about criteria diagnosis | - Self-rated assessment: “best describe [their] hearing” (6-rating scale) | - For self-rated assessment: |
| - Proxy-rated assessment: “significant hearing difficulties that interfere with daily communication.” (Yes/No) | MCI: sensitivity 61.1%, specificity 84.9% | |||
| - 520 Proxy-rated assessment | Dementia: sensitivity 52.6%, specificity 81.2% | |||
| - For proxy-rated assessment: | ||||
| MCI: sensitivity 65.7%, specificity 83.3% | ||||
| Dementia: sensitivity 73.3%, specificity 60.3% | ||||
| (“Test positive” was defined as: | ||||
| - Pure-tone average ≥40 dB | ||||
| - “moderate trouble” or greater in self-rated assessment | ||||
| - “Yes” in proxy-rated assessment) |
AD, Alzheimer’s disease; MCI, mild cognitive impairment; MMSE, Mini-Mental State Examination; K-MMSE, Korean version of Mini-Mental State Examination; PPV, positive predictive value; NPV, negative predictive value; CI, confidence interval; FED, frontal-executive dysfunction; MoCA-HA, Montreal Cognitive Assessment for hearing-aid users; ICD-10, International Classification of Diseases, Tenth Revision
Another study assessed cognitively impaired patients (HHIE-S) from a memory clinic and their caregivers (HHIE-SP) by using the HHIE screening version [23]. The authors reported data in terms of “pass/fail” and defined “failure” as: 1) no response to a 40-dB HL during PTA, 2) HHIE score >18 or higher, and 3) a passing score (<18) on the HHIE and no response to a 25 dB HL pure tone. There was no statistically significant difference between the proportion of patients who passed or failed the PTA and the HHIE-S. Both HHIE-S (sensitivity=30.4%, specificity=100%, accuracy=34.7%) and HHIE-SP (sensitivity=42.4%, specificity=100%, accuracy=47.2%) revealed low sensitivity and accuracy but high specificity when derived from raw data. Notably, the discrepancy between the pass-fail rates on the HHIE-S and the HHIE-SP was significant (χ2=5.58, p<0.05), with caregivers reporting a disability more than patients.
The outcomes of this study were comparable those of a study that investigated patient with normal cognition, MCI, and dementia using the modified Amsterdam Inventory for Disability (mAIAD) and the speech, spatial, and hearing qualities scale (SSQ) [25]. Both were validated questionnaires for assessing real-life hearing function in individuals. The study found weak correlations between self-assessment questionnaire scores and PTA in MCI group, and moderate correlations in the dementia group [32,33]. For mAIAD, there were weak to moderate, nonsignificant correlations between overall scores and PTA (r=-0.24, p=0.197 and r=-0.50, p=0.069 for MCI and dementia group, respectively). Corresponding to SSQ, weak to moderate, nonsignificant correlations were found (r=-0.19, p=0.321 and r=-0.37, p=0.169 for MCI and dementia group, respectively). In contrast, moderate to high correlations were observed between the overall mAIAD (Pearson correlation r=-0.59, p=0.001) and SSQ scores (Pearson correlation r=-0.55, p=0.002) and the PTA in the group with normal cognition. Notably, robust correlations were observed in all groups between the total scores of both questionnaires and their respective domains, including speech, spatial, and sound quality.
One retrospective review study used the Resident Assessment Instrument–Minimum Data Set 2.0 (RAI-MDS), which classified hearing difficulties into 4 categories, to examine the hearing status of long-term care residents with dementia as rated by their healthcare staff [26]. On-site air-conduction audiometry was conducted by an audiologist in a quiet room with ambient noise level not exceeding 45 dB to obtain the pure-tone average. A weak correlation between PTA category and RAI-MDS rating was confirmed using an intraclass correlation coefficient (r=0.286, p=0.015). Notably, 11 of 25 participants had hearing loss that was either unidentified or underestimated by this assessment.
One study deployed data from a prospective cohort study in the community, employing determined cognitive diagnoses and audiometric data for calculating diagnostic accuracy between PTA and self- and proxy-rated hearing assessments [27]. Participants were required to describe their unaided hearing, while proxies were asked about “the significant hearing difficulties that interfere with daily communication.” Hearing loss was defined as PTA threshold ≥40 dB from audiometry, moderate trouble or greater in self-rated assessments, and “Yes” response for proxy-rated assessments. The sensitivity and specificity of self-rated hearing assessments for dementia patients (52.6% and 81.2%, respectively) were lower than for those with MCI (61.1% and 84.9%, respectively) and even lower than individuals with normal cognitive function (71.2% and 85.9%, respectively). In the case of proxy-rated hearing assessments, low sensitivity was observed in both the MCI and dementia groups (65.7% and 73.3%, respectively).
Discussion
Based on systematic review of 10 studies, it can be asserted that electrophysiological and behavioral hearing tests exhibited commendable diagnostic performance compared to PTA for accurately detects hearing loss in MCI and dementia. Conversely, subjective reports of hearing may tend to underestimate the actual prevalence of hearing loss in this particular population. These findings carry significant implication for the development of screening protocol designed to identify hearing loss in individual with cognitive impairment.
Our results suggest several notable findings. First of all, electrophysiological hearing tests, including DPOE, ABR, ASSR, and CATE showed remarkable significant correlations with PTA thresholds. A plausible explanation is that these methods can be implemented without patient participation. People with dementia have impairment of cognitive and functioning capacities [34]. Standard audiometry is regarded as demanding complex multi-domain of cognitive function at each step, hence, only about half of those with impaired cognitive function can accomplish audiometry [14]. For instance, complex attention is required for the task of pressing a button each time a tone is heard. Over time, executive functioning, learning, and memory are needed to follow procedure instructions and recall the word. This limitation can be solved by the electrophysiological test, which also provides accurate thresholds. Regardless, one of the included studies reported that some individuals could not endure this method due to its equipment and long duration [20]. In addition, this approach does not alleviate the shortage of advanced audiologic services in some regions.
Based on this review, we observed that the behavioral hearing test was more consistently related with PTA than self-perceived hearing assessment. The simple and familiar physical examination battery tests, such as the tuning fork test, whisper voice test, and finger rub test, proved to be highly sensitive screening techniques [21]. Moreover, the approach involving equipment such as an audiometry screener and an application to hearing screening achieved high sensitivity and overall accuracy in patients with MCI and dementia [21,22]. The results were similar to those found in older adults with normal cognition [35,36]. Screening tests and interventions are mostly developed under the principles of being accurate, reliable, affordable, and efficient for target populations [37], particularly for application-based methods that simplify the conventional approach for usability. Even though a previous systematic review revealed a relatively lower area under curve (AUC) in the older adult group (AUC=0.9, 95% CI 0.87–0.92) compared to younger aged group (AUC=0.96, 95% CI 0.94–0.97), smartphone-based audiometry remains highly accurate for detecting hearing impairment [36]. More studies that investigate the value of these devices in cognitive impairment populations are needed.
In contrast to the aforementioned auditory tests, self-reported hearing assessments could not precisely reflect hearing difficulties in cognitive impairment [23-25,27]. There are many possible explanations for this. People with dementia may have difficulty communicating in real-life situations due to auditory dysfunction, commonly known as auditory processing disorder. They may suffer from impaired perception of sound features, auditory scene analysis, recognition of sounds, and auditory hallucinations [38]. This deficit may be reflected in the score of the mAIAD and the SSQ, which focus on the recognition of sound, speech, and localization of sound, as observed in the study of Utoomprurkporn, et al. [25]. However, these deficits are not necessarily correlated pure-tone thresholds. Another possibility is that dementia’s severity and patients’ fluctuating capacity may affect their ability to comprehend the measurement [39]. The multiple-item and multiple-choice structure of the questionnaire may impede its successful completion. Another explanation is their denial attitude or poor self-perception about their hearing deficit, which is similar to general older adult populations [40,41]. Unsurprisingly, in this review, the caregivers reported hearing difficulties more frequently than the patients themselves, and one study found a strong correlation with PTA [26]. Future studies that explore demented patients and their caregivers by self-perceived assessment questionnaire would be informative to strengthen our conclusion.
Hearing loss accounts for 20% of global population [42]. In addition, the prevalence of moderate to severe hearing loss increases with age, from 12.7% at 60 years to nearly 60% at 90 years of age [42]. In populations with MCI and dementia, previous studies reported the prevalence of hearing loss ranging from 50% to greater than 90%, varying across studies [23,43-45]. Remarkably, the prevalence tends to be higher than in the general age-matched population [23,43,45]. A number of evidences sustain the notion that hearing loss may conduce to cognitive decline through via sensory deprivation and the information-degradation hypotheses, or both conditions may be consequence of overall neural degeneration associated with aging; the common cause hypothesis [7]. In light of current understanding of the hearing-dementia association, hearing aids may be a potentially beneficial intervention for dementia. The restoration of auditory stimuli by hearing aids may improve social communication and decrease cognitive load, consequently lessening the progression of neuropsychiatric symptoms (NPS) of dementia through indirect pathway. According to previous studies, the use of hearing assistive devices has been shown to benefit not only patients but also caregivers [46].
The World Health Organization encourages hearing screening for all older adults over the age of 50 using audiological, otoscopic examinations and whispered voice tests, as well as, cost-effective and simple-to-use screening tools such as automated hearing testing, digits-in-noise tests via mobile applications, booth-less audiometry, and telemedicine services [42]. For people living with dementia, the multidisciplinary team, consisting of professionals such as audiologist, otologist, speech and language pathologist, geriatric and occupational therapist, rehabilitation specialists, dementia specialist, and care home manager, collaborated to develop specific practical recommendations aimed at recognizing and managing hearing and vision impairment. Their primary goal is to facilitate early detection, precise diagnosis, and prompt intervention to improve sensory impairment that significantly impact individuals’ quality of life [15]. The ideal screening tools should be validated, reliable, fast, and widely accessible to professionals and patients to enable early detection of sensory impairment. Basic options such as self-administered questionnaires, mobile-based screening, and bedside screening methods including whispered voice, finger rub, and watch tick tests should be offered. Based on our comprehensive review, we also highlight the screening options for hearing loss in this population, as indicated in Table 5.
Table 5.
Modalities of choice for screening hearing loss in older adults with cognitive impairment
| Screening options | |
|---|---|
| Basic option | Bedside tests [21] |
| - 512-Hz and 1024-Hz tuning fork | |
| - Finger rub | |
| - Whispered voice | |
| Otoacoustic emission (OAE) [19] | |
| Air conduction screening audiometry [21] | |
| Mobile-based screening test e.g., SHOEBOX QuickTest [22] | |
| Alternative options for obtaining hearing threshold | Auditory brainstem response (ABR) [19] |
| Auditory steady-state response (ASSR) [18] | |
| Cortical automatic threshold estimation (CATE) [20] | |
| Considerations for older adults with cognitive impairment | Provide concise and simple instructions |
| Kindly ensure patient to bring their best corrected glasses for optimum vision | |
| Allocate ample time for the appointment and test, allowing flexibility to accommodate breaks if necessary | |
| Evaluate the patient’s cognitive status to perform properly hearing assessment |
Limitation
Only 10 researches matched the inclusion criteria, and the sample sizes of some of these studies are rather small. Due to the heterogeneity of hearing screening tests, variations in reference test criteria (PTA), and reported outcomes, a meta-analysis was precluded. In addition, the majority of the participants had MCI or mild to moderate dementia. None of the participants in the study had severe dementia, which may alter test results owing to cognitive ability. Additional study involving the accuracy of auditory test on the large scale and disparities in dementia severity is warranted.
Conclusion
In conclusion, alternative hearing screening tests based on electrophysiological and behavioral approaches appear dependable among older adults with cognitive impairment, when compared to conventional PTA in diagnosing hearing loss. Whereas self-perceived hearing assessment is distinctly inconsistent with PTA, according to findings of our review. Further work is needed to delineate the optimal screening method for recognizing hearing loss in individual with cognitive impairment.
Acknowledgments
None
Footnotes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: all authors. Data curation: Patcharaorn Limkitisupasin, Piyawat Jongpradubgiat. Formal analysis: Patcharaorn Limkitisupasin, Piyawat Jongpradubgiat. Funding acquisition: Patcharaorn Limkitisupasin. Investigation: Patcharaorn Limkitisupasin, Piyawat Jongpradubgiat. Methodology: all authors. Project administration: Nattawan Utoomprurkporn. Resources: Patcharaorn Limkitisupasin. Software: Patcharaorn Limkitisupasin. Supervision: Nattawan Utoomprurkporn. Validation: Patcharaorn Limkitisupasin, Nattawan Utoomprurkporn. Visualization: Patcharaorn Limkitisupasin, Nattawan Utoomprurkporn. Writing—original draft: Patcharaorn Limkitisupasin, Nattawan Utoomprurkporn. Writing—review & editing: Patcharaorn Limkitisupasin, Nattawan Utoomprurkporn. Approval of final manuscript: all authors.
Funding Statement
This work was supported by Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University [grant number GA66/15] and Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University [grant number RA-MF-14/66].
Supplementary Materials
The online-only Data Supplement is available with this article at https://doi.org/10.7874/jao.2023.00507.
Search strategy
REFERENCES
- 1.World Health Organization . Geneva: World Health Organazation; 2023. Dementia [Internet] [cited 2023 December 12]. Available from: https://www.who.int/news-room/fact-sheets/detail/dementia. [Google Scholar]
- 2.Sabayan B, Sorond F. Reducing risk of dementia in older age. JAMA. 2017;317:2028. doi: 10.1001/jama.2017.2247. [DOI] [PubMed] [Google Scholar]
- 3.Livingston G, Sommerlad A, Orgeta V, Costafreda SG, Huntley J, Ames D, et al. Dementia prevention, intervention, and care. Lancet. 2017;390:2673–734. doi: 10.1016/S0140-6736(17)31363-6. [DOI] [PubMed] [Google Scholar]
- 4.Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396:413–46. doi: 10.1016/S0140-6736(20)30367-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lin FR, Pike JR, Albert MS, Arnold M, Burgard S, Chisolm T, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. 2023;402:786–97. doi: 10.1016/S0140-6736(23)01406-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yeo BSY, Song H, Toh EMS, Ng LS, Ho CSH, Ho R, et al. Association of hearing aids and cochlear implants with cognitive decline and dementia: a systematic review and meta-analysis. JAMA Neurol. 2023;80:134–41. doi: 10.1001/jamaneurol.2022.4427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Powell DS, Oh ES, Reed NS, Lin FR, Deal JA. Hearing loss and cognition: what we know and where we need to go. Front Aging Neurosci. 2021;13:769405. doi: 10.3389/fnagi.2021.769405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kim AS, Garcia Morales EE, Amjad H, Cotter VT, Lin FR, Lyketsos CG, et al. Association of hearing loss with neuropsychiatric symptoms in older adults with cognitive impairment. Am J Geriatr Psychiatry. 2021;29:544–53. doi: 10.1016/j.jagp.2020.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mamo SK, Reed NS, Price C, Occhipinti D, Pletnikova A, Lin FR, et al. Hearing loss treatment in older adults with cognitive impairment: a systematic review. J Speech Lang Hear Res. 2018;61:2589–603. doi: 10.1044/2018_JSLHR-H-18-0077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leroi I, Simkin Z, Hooper E, Wolski L, Abrams H, Armitage CJ, et al. Impact of an intervention to support hearing and vision in dementia: The SENSE-Cog Field Trial. Int J Geriatr Psychiatry. 2020;35:348–57. doi: 10.1002/gps.5231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.British Society of Audiology . Recommended procedure: pure-tone air-conduction and boneconduction threshold audiometry with and without masking. Bathgate: British Society of Audiology; 2018. [Google Scholar]
- 12.Dawes P, Littlejohn J, Bott A, Brennan S, Burrow S, Hopper T, et al. Hearing assessment and rehabilitation for people living with dementia. Ear Hear. 2022;43:1089–102. doi: 10.1097/AUD.0000000000001174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McClannahan KS, Chiu YF, Sommers MS, Peelle JE. Test-retest reliability of audiometric assessment in individuals with mild dementia. JAMA Otolaryngol Head Neck Surg. 2021;147:442–9. doi: 10.1001/jamaoto.2021.0012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bott A, Meyer C, Hickson L, Pachana NA. Can adults living with dementia complete pure-tone audiometry? A systematic review. Int J Audiol. 2019;58:185–92. doi: 10.1080/14992027.2018.1550687. [DOI] [PubMed] [Google Scholar]
- 15.Littlejohn J, Bowen M, Constantinidou F, Dawes P, Dickinson C, Heyn P, et al. International practice recommendations for the recognition and management of hearing and vision impairment in people with dementia. Gerontology. 2022;68:121–35. doi: 10.1159/000515892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155:529–36. doi: 10.7326/0003-4819-155-8-201110180-00009. [DOI] [PubMed] [Google Scholar]
- 18.Villeneuve A, Hommet C, Aussedat C, Lescanne E, Reffet K, Bakhos D. Audiometric evaluation in patients with Alzheimer’s disease. Eur Arch Otorhinolaryngol. 2017;274:151–7. doi: 10.1007/s00405-016-4257-1. [DOI] [PubMed] [Google Scholar]
- 19.Gates GA, Karzon RK, Garcia P, Peterein J, Storandt M, Morris JC, et al. Auditory dysfunction in aging and senile dementia of the Alzheimer’s type. Arch Neurol. 1995;52:626–34. doi: 10.1001/archneur.1995.00540300108020. [DOI] [PubMed] [Google Scholar]
- 20.Bott A, Hickson L, Meyer C, Bardy F, Van Dun B, Pachana NA. Is cortical automatic threshold estimation a feasible alternative for hearing threshold estimation with adults with dementia living in aged care? Int J Audiol. 2020;59:745–52. doi: 10.1080/14992027.2020.1746976. [DOI] [PubMed] [Google Scholar]
- 21.Uhlmann RF, Rees TS, Psaty BM, Duckert LG. Validity and reliability of auditory screening tests in demented and non-demented older adults. J Gen Intern Med. 1989;4:90–6. doi: 10.1007/BF02602346. [DOI] [PubMed] [Google Scholar]
- 22.Frank A, Goldlist S, Mark Fraser AE, Bromwich M. Validation of SHOEBOX QuickTest hearing loss screening tool in individuals with cognitive impairment. Front Digit Health. 2021;3:724997. doi: 10.3389/fdgth.2021.724997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gold M, Lightfoot LA, Hnath-Chisolm T. Hearing loss in a memory disorders clinic. A specially vulnerable population. Arch Neurol. 1996;53:922–8. doi: 10.1001/archneur.1996.00550090134019. [DOI] [PubMed] [Google Scholar]
- 24.Lee SJ, Kim H, Kim LS, Kim JH, Park KW. Effects of frontal-executive dysfunction on self-perceived hearing handicap in the elderly with mild cognitive impairment. PLoS One. 2019;14:e0210014. doi: 10.1371/journal.pone.0210014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Utoomprurkporn N, Stott J, Costafreda SG, Bamiou DE. Lack of association between audiogram and hearing disability measures in mild cognitive impairment and dementia: what audiogram does not tell you. Healthcare. 2021;9:769. doi: 10.3390/healthcare9060769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hopper T, Slaughter SE, Hodgetts B, Ostevik A, Ickert C. Hearing loss and cognitive-communication test performance of long-term care residents with dementia: effects of amplification. J Speech Lang Hear Res. 2016;59:1533–42. doi: 10.1044/2016_JSLHR-H-15-0135. [DOI] [PubMed] [Google Scholar]
- 27.Kim AS, Betz JF, Albert M, Deal JA, Faucette SP, Oh ES, et al. Accuracy of self- and proxy-rated hearing among older adults with and without cognitive impairment. J Am Geriatr Soc. 2022;70:490–500. doi: 10.1111/jgs.17558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Korczak P, Smart J, Delgado R, Strobel TM, Bradford C. Auditory steady-state responses. J Am Acad Audiol. 2012;23:146–70. doi: 10.3766/jaaa.23.3.3. [DOI] [PubMed] [Google Scholar]
- 29.Lichtenstein MJ, Bess FH, Logan SA. Diagnostic performance of the hearing handicap inventory for the elderly (screening version) against differing definitions of hearing loss. Ear Hear. 1988;9:208–11. doi: 10.1097/00003446-198808000-00006. [DOI] [PubMed] [Google Scholar]
- 30.Ventry IM, Weinstein BE. The hearing handicap inventory for the elderly: a new tool. Ear Hear. 1982;3:128–34. doi: 10.1097/00003446-198205000-00006. [DOI] [PubMed] [Google Scholar]
- 31.Park S, Han GC, Cho Y, Byun JY, Shin JE, Chu H, et al. Standardization for a Korean version of Hearing Handicap Inventory for the Elderly. Korean J Otorhinolaryngol-Head Neck Surg. 2011;54:828–34. [Google Scholar]
- 32.Meijer AG, Wit HP, TenVergert EM, Albers FW, Muller Kobold JE. Reliability and validity of the (modified) Amsterdam Inventory for Auditory Disability and Handicap. Int J Audiol. 2003;42:220–6. doi: 10.3109/14992020309101317. [DOI] [PubMed] [Google Scholar]
- 33.Gatehouse S, Noble W. The Speech, Spatial and Qualities of Hearing Scale (SSQ) Int J Audiol. 2004;43:85–99. doi: 10.1080/14992020400050014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Hugo J, Ganguli M. Dementia and cognitive impairment: epidemiology, diagnosis, and treatment. Clin Geriatr Med. 2014;30:421–42. doi: 10.1016/j.cger.2014.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Feltner C, Wallace IF, Kistler CE, Coker-Schwimmer M, Jonas DE. Screening for hearing loss in older adults: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2021;325:1202–15. doi: 10.1001/jama.2020.24855. [DOI] [PubMed] [Google Scholar]
- 36.Chen CH, Lin HH, Wang MC, Chu YC, Chang CY, Huang CY, et al. Diagnostic accuracy of smartphone-based audiometry for hearing loss detection: meta-analysis. JMIR Mhealth Uhealth. 2021;9:e28378. doi: 10.2196/28378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Dobrow MJ, Hagens V, Chafe R, Sullivan T, Rabeneck L. Consolidated principles for screening based on a systematic review and consensus process. CMAJ. 2018;190:E422–9. doi: 10.1503/cmaj.171154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hardy CJ, Marshall CR, Golden HL, Clark CN, Mummery CJ, Griffiths TD, et al. Hearing and dementia. J Neurol. 2016;263:2339–54. doi: 10.1007/s00415-016-8208-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Perfect D, Griffiths AW, Vasconcelos Da Silva M, Lemos Dekker N, McDermid J, Surr CA. Collecting self-report research data with people with dementia within care home clinical trials: benefits, challenges and best practice. Dementia (London) 2021;20:148–60. doi: 10.1177/1471301219871168. [DOI] [PubMed] [Google Scholar]
- 40.Chang HP, Ho CY, Chou P. The factors associated with a self-perceived hearing handicap in elderly people with hearing impairment--results from a community-based study. Ear Hear. 2009;30:576–83. doi: 10.1097/AUD.0b013e3181ac127a. [DOI] [PubMed] [Google Scholar]
- 41.Jupiter T, Palagonia CL. The hearing handicap inventory for the elderly screening version adapted for use with elderly Chinese American individuals. Am J Audiol. 2001;10:99–103. doi: 10.1044/1059-0889(2001/010). [DOI] [PubMed] [Google Scholar]
- 42.Chadha S, Kamenov K, Cieza A. The world report on hearing, 2021. Bull World Health Organ. 2021;99:242-a. doi: 10.2471/BLT.21.285643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Gyanwali B, Hilal S, Venketasubramanian N, Chen C, Loo JHY. Hearing handicap in Asian patients with dementia. Am J Otolaryngol. 2020;41:102377. doi: 10.1016/j.amjoto.2019.102377. [DOI] [PubMed] [Google Scholar]
- 44.Nirmalasari O, Mamo SK, Nieman CL, Simpson A, Zimmerman J, Nowrangi MA, et al. Age-related hearing loss in older adults with cognitive impairment. Int Psychogeriatr. 2017;29:115–21. doi: 10.1017/S1041610216001459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lopes LDC, Magaldi RM, Gândara MER, Reis ACB, Jacob-Filho W. Prevalence of hearing impairment in patients with mild cognitive impairment. Dement Neuropsychol. 2007;1:253–9. doi: 10.1590/S1980-57642008DN10300006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Hubbard HI, Mamo SK, Hopper T. Dementia and hearing loss: interrelationships and treatment considerations. Semin Speech Lang. 2018;39:197–210. doi: 10.1055/s-0038-1660779. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy