

Abstract
Background
Behçet’s disease (BD) is a rare, multisystemic inflammatory disorder with a diverse range of manifestations, primarily affecting the mucocutaneous and ocular systems. While vascular involvement is less frequent it can be severe, with coronary aneurysms being particularly rare.
Case description
We report a 28-year-old male with BD who developed a giant anterior interventricular artery aneurysm. The patient, initially managed with azathioprine and colchicine, presented with acute chest pain and elevated cardiac markers. Imaging revealed a coronary aneurysm measuring 5.03 cm. Due to the inflammatory nature of the aneurysm surgical intervention was initially deferred, and the patient was treated with corticosteroids and cyclophosphamide. Despite these treatments, recurrent symptoms prompted the initiation of infliximab therapy. Administered at 5 mg/kg at weeks 0, 2 and 6, with subsequent doses every two months, infliximab led to a significant reduction in aneurysm size to 3.73 cm.
Conclusion
This case highlights the effectiveness of infliximab in managing giant coronary aneurysms associated with BD, demonstrating its potential as a treatment option for severe vascular complications in BD. The substantial reduction in aneurysm size following infliximab therapy underscores the need for further investigation into its role in treating such rare but serious manifestations of BD.
LEARNING POINTS
A giant coronary aneurysm is a rare complication of Behçet’s disease.
Infliximab effectively reduced the aneurysm size.
Imaging shows a substantial decrease in aneurysm size after infliximab treatment.
Keywords: Behçet’s disease, giant coronary aneurysm, infliximab, cardiovascular complications
INTRODUCTION
Behçet’s disease (BD) is a multisystemic inflammatory disorder first described in 1937, characterised primarily by oral and genital ulcers, and ocular lesions. It can also involve the nervous, musculoskeletal, pulmonary and cardiovascular systems[1]. Although vascular involvement is less common it can be severe, with coronary aneurysms being particularly rare[2]. Treatment traditionally includes corticosteroids and immunosuppressants; however, biologic therapies such as infliximab have shown promise, especially in severe or refractory cases. This report describes a young patient with BD who developed a giant coronary aneurysm and responded effectively to infliximab, highlighting its potential as a viable treatment option for severe vascular complications in BD.
CASE DESCRIPTION
A 28-year-old male had been diagnosed with BD four years prior, and presented initially with oral aphthae, genital ulcers and lower limb venous thrombosis. Over time, the disease progressed with recurrent episodes of venous thrombosis and increasing frequency of ulcers. He was on immunosuppressive therapy with azathioprine and colchicine. The diagnosis of Behçet’s disease was confirmed based on the International Study Group criteria[3] that includes recurrent oral ulcers, genital ulcers and other systemic manifestations. The patient presented with acute chest pain lasting over 6 hours, radiating to the left upper extremity. He had no history of smoking, hypertension, diabetes, hyperlipidaemia or family cardiovascular risk. A cardiovascular examination was largely unremarkable. Electrocardiography (EKG) showed transient ST segment elevation in the lateral leads. Laboratory tests revealed elevated cardiac troponin levels (2.63 μg/l; normal level: <0.04 μg/l) and a significant increase in C-reactive protein (200 mg/l; normal level: <5 mg/l). Additionally, hyperleukocytosis was observed (23 G/l; normal range: 4–10 G/l), while other routine blood tests were within normal limits.
Echocardiography identified moderate pericardial effusion and hypokinesis of the apical segment as well as the distal third of the anterior wall and interventricular septum. A thoraco-abdominal computed tomography (CT) scan revealed a giant anterior interventricular artery aneurysm measuring approximately 5.03 cm (Fig. 1). Given the inflammatory nature of the aneurysm, surgical intervention was deferred initially. The patient was treated with a bolus of methylprednisolone and cyclophosphamide. Due to the recurrence of coronary symptoms, infliximab therapy was initiated at a dose of 5 mg/kg at weeks 0, 2 and 6, and subsequently every two months. A follow-up CT scan after just three infliximab doses showed a reduction in aneurysm size to 3.73 cm (Fig. 2). This positive response led to the continuation of infliximab treatment to reduce the risk of severe postoperative complications.
Figure 1.

Thoraco-abdominal CT showing a giant coronary aneurysm in the anterior interventricular artery before infliximab treatment, measuring 5.03 cm.
Figure 2.
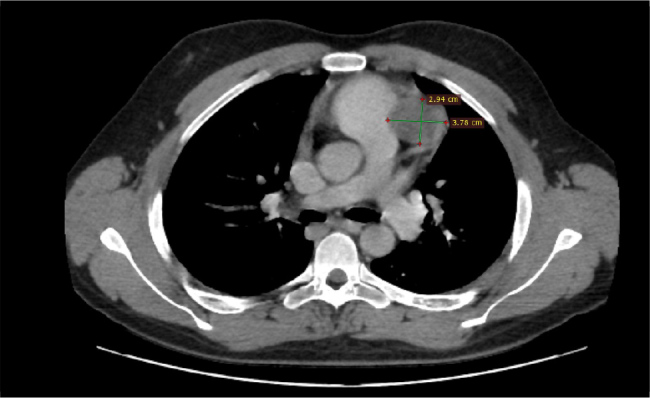
Thoraco-abdominal CT showing a significant reduction in the coronary aneurysm in the anterior interventricular artery after infliximab treatment, measuring approximately 3.73 cm.
DISCUSSION
BD is renowned for its venous complications – such as deep vein thrombosis – but arterial involvement, including coronary aneurysms, is considerably less common, occurring in approximately 6.3 to 15.3% of BD cases[1]. The initial clinical presentation often consists of an acute coronary syndrome[4]. Traditional management has focused on symptomatic relief and controlling the underlying inflammation.
Coronary artery aneurysms in BD pose considerable challenges due to their potential to induce myocardial ischaemia and other severe cardiovascular complications. Their rarity complicates management, as these aneurysms can lead to significant adverse outcomes, including rupture and impaired cardiac function[5,6]. Effective management requires a careful balance of traditional and innovative therapeutic strategies to mitigate associated risks and improve patient outcomes. In general, medical treatment based on immunosuppressants is strongly recommended before any surgical procedure, as supported by reported cases[7]. This case significantly contributes to the literature by documenting the successful use of infliximab, a TNF-alpha inhibitor, in managing a giant coronary aneurysm in a patient with BD. Despite the rarity of coronary aneurysms in BD and the limited treatment guidelines for such complications, the patient experienced a notable reduction in aneurysm size from 5.03 cm to 3.73 cm following the infliximab therapy.
This outcome is significant because it suggests that infliximab, primarily used for severe and refractory forms of BD, may also be effective in managing severe arterial complications such as giant coronary aneurysms. Previous studies have highlighted infliximab’s efficacy in treating severe vascular involvement in BD[8], though evidence for its use specifically in coronary aneurysms is limited. The significance of this case lies in its demonstration of infliximab’s potential to reduce aneurysm size and mitigate the acute coronary syndrome associated with BD. Key points include:
Promising treatment strategy: The successful management of the giant coronary aneurysm with infliximab offers a new therapeutic option for patients with similar complications, particularly those who are not candidates for, or have contraindications to, surgical intervention.
Notable reduction in aneurysm size: The observed reduction suggests that infliximab may play a role in stabilising or even reversing the progression of arterial aneurysms in BD, potentially impacting clinical management strategies and patient outcomes.
Need for further research: This case underscores the importance of further research into the use of infliximab for cardiovascular complications in BD. More extensive studies are needed to confirm these findings and refine treatment protocols. It also emphasises the need for a multidisciplinary approach in managing complex BD cases, involving rheumatologists, cardiologists and cardiovascular surgeons to optimise patient care.
CONCLUSION
Our case highlights the potential of infliximab as an effective treatment for giant coronary aneurysms in BD. Its success in reducing aneurysm size and the positive clinical outcomes observed underscore the need for further research. Future studies should explore infliximab’s role in broader treatment protocols for BD-related cardiovascular complications, aiming to refine management strategies and improve patient outcomes.
Acknowledgements
A pre-print version of this article exists on the repository Authorea.
Footnotes
Conflicts of Interests: The Authors declare that there are no competing interests.
Patient Consent: Written consent obtained before production of this manuscript.
REFERENCES
- 1.Leccese P, Yazici Y, Olivieri I. Behcet’s syndrome in nonendemic regions. Curr Opin Rheumatol. 2017;29:12–16. doi: 10.1097/BOR.0000000000000349. [DOI] [PubMed] [Google Scholar]
- 2.Sarica-Kucukoglu R, Akdag-Kose A, Kayabali M, Yazganoglu KD, Disci R, Erzengin D, et al. Vascular involvement in Behçet’s disease: a retrospective analysis of 2,319 cases. Int J Dermatol. 2006;45:919–921. doi: 10.1111/j.1365-4632.2006.02832.x. [DOI] [PubMed] [Google Scholar]
- 3.Criteria for diagnosis of Behcet’s disease. International Study Group for Behcet’s Disease. Lancet. 1990;335:1078–1080. [PubMed] [Google Scholar]
- 4.Schiff S, Moffatt R, Mandel WJ, Rubin SA. Acute myocardial infarction and recurrent ventricular arrhythmias in Behçet’s syndrome. Am Heart J. 1982;103:438–440. doi: 10.1016/0002-8703(82)90289-7. [DOI] [PubMed] [Google Scholar]
- 5.Kariyanna PT, Shah P, Jayarangaiah A, Chowdhury YS, Lazaro D. Acute coronary syndrome in Behcet’s syndrome: a systematic review. Eur J Rheumatol. 2021;8:31–35. doi: 10.5152/eurjrheum.2020.19213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wechsler B, Du LT, Kieffer E. Manifestations cardio-vasculaires de la maladie de Behçet. [Cardiovascular manifestations of Behçet’s disease]. Ann Med Interne (Paris) 1999;150:542–554. French. [PubMed] [Google Scholar]
- 7.Meric M, Oztas DM, Ugurlucan M, Tireli E, Dayioglu E. Giant left anterior descending coronary artery aneurysm in a patient with Behçet’s disease. Braz J Cardiovasc Surg. 2022;37:605–608. doi: 10.21470/1678-9741-2020-0665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yoshimi R. The diagnosis and management of vasculo-Behçet’s disease. Intern Med. 2019;58:3–4. doi: 10.2169/internalmedicine.1657-18. [DOI] [PMC free article] [PubMed] [Google Scholar]