

Abstract
Background:
Hypertension is a prevalent non-communicable disease and unequivocally one of the most serious health threats of the twenty-first century. The prevention of both immediate and long-term consequences depends on ongoing therapeutic education.
Aims:
To assess Tunisian hypertensive patients’ knowledge of hypertension and then evaluate the impact of an educational program on knowledge among this population.
Methods:
A randomized controlled trial was carried out among 639 hypertensive patients in Tunisia. The control group received only basic medical care, while the experimental group acquired additionally an educational program. The data collection tool was a questionnaire that included an information sheet and the Hypertension Knowledge Level Scale (HK-LS).
Results:
Before to the implementation of the program, only 12.1% of the participants had a good level of knowledge about hypertension (12.8% for the experimental group, vs. 10.5% for the control group, P=0.57). Following the program’s deployment, the rate of good level of knowledge became 63.6% for the experimental group vs. 11.4% for the control group, P<0.001). The results revealed that the experimental group showed a significant amelioration in the total score of the HK-LS: from 58.49 to 76.94%, P<0.0001. In contrast, no significant amelioration was noted in the control group. Concerning the six dimensions of the scale, the amelioration in the experimental group was observed in all dimensions, except the treatment dimension.
Conclusion:
Overall, the findings indicated low levels of knowledge about hypertension. This kind of approach proved an effective improvement in disease-related knowledge and may be essential for hypertension management.
Keywords: hypertension, knowledge, randomized controlled trial, therapeutic education
Introduction
Highlights
Hypertension management depends on the level of knowledge about the disease.
The education of patients is the key component of hypertension management.
Implementing a healthcare education campaign serves to remedy a lack of health-related knowledge.
Hypertension (HTN) is a first-rate cause of cardiovascular conditions as well as premature death worldwide. Due to its expanding prevalence, HTN is an international problem for public health, especially for countries with low to middle incomes1. In 2019, more than one billion hypertensive patients lived in these countries, accounting for 82% of the hypertensive patients globally2. The prevalence of HTN in the regions of the Middle East and northern Africa is 26.2%3.
HTN treatment focuses on lifestyle adjustments that decrease blood pressure while enhancing the efficacy of HTN medications4. Although there are plenty of HTN care recommendations, blood pressure management remains challenging among patients with HTN. Consequently, educating individuals on their medical condition is extremely important for improving blood pressure control, health status, and overall quality of life5.
Likewise, increased levels of HTN knowledge are linked to improved self-management practices, medication compliance, social support, a healthy lifestyle, self-care, and self-efficacy6–9.
Indeed, there are specific variations between regions in the level of knowledge about HTN. For example, in Lebanon it has been reported that 25.1% of hypertensive patients had an adequate level of knowledge10, while in Morocco, only 7% of participants had good knowledge about HTN11.
Several factors are associated with greater knowledge of HTN. By identifying them, adequate educational programs can be tailored to patients to assist them in their HTN control12. According to interventional studies in the Middle East, educational programs are effective in increasing HTN-related knowledge13–15.
In Tunisia, few studies reported facts about hypertensive patients’ level of health-related knowledge. Therefore, this study aimed to assess Tunisian hypertensive patients’ level of knowledge about HTN and to evaluate the effect of an educational program on knowledge among this population.
Materials and methods
Study design and setting
This randomized controlled trial (RCT) was carried out from May 2021 to December 2022 in Sfax City, Tunisia.
Participants
The study population consisted of adults with HTN recruited from the department of general medicine. The inclusion criteria included having a diagnosis of HTN, being over 18 years old, and taking antihypertensive medications. The exclusion criteria were pregnancy, communication impairment, and missing one educational session. Following the application of these criteria, the patients were enrolled in one of the two groups (experimental or control). The control group received only basic medical care, while the experimental group acquired additionally an educational program.
To ensure allocation concealment, the randomization procedure used consecutively ordered, closed, sealed envelopes issued by a third party not involved in the study. Throughout the recruitment process, the researcher unsealed the envelopes for random allocation.
Sample size
The number of participants recruited was determined using the effect size from a previous study performed in Iran13, which is centered on the score of the HTN knowledge outcomes (mean difference=2.19, SD=2.81). The parameter settings were the level of significance α=0.0001, power (1 – β)=0.98, and drop-off rate of 20%, resulting in 490 participants in the experimental group and 245 in the control group.
Intervention
The intervention was composed of three 45-minute educational sessions held in a private office in the department of general medicine every four months. The main goal of the educational program was to enhance the patients’ understanding of HTN.
The sessions occurred alternating between group and individual sessions using the face-to-face method. A range of educational techniques, including presentations, interactions, and explanations, were used. Following each session, all participants in the experimental group received supplemental materials drafted in Tunisian dialect, such as books, posters, and leaflets.
The program covered an extensive range of themes. The initial meeting focused on the definition of HTN and the diet. The next section covered blood pressure monitoring, HTN management, and its consequences. The latest meeting centered around medication management, keeping an active lifestyle, and the necessity of regular exercise.
Measures
Face-to-face interviews were used to collect data through a questionnaire consisting of two sections. The initially included covers the characteristics of patients, while the subsequent goes over HTN knowledge evaluation. The first interview was held three months before the first educational session, and the final interview was held four months after the last session. Each patient’s interview lasts around 15 min.
Patient’s characteristics
The data collection sheet included patients’ socio-demographic characteristics, such as sex, age, level of education, and occupation, as well as medical data, such as HTN duration and blood pressure.
Hypertension knowledge
The HTN Knowledge Level Scale (HK-LS), translated in Arabic, was used to evaluate participants’ HTN knowledge16. The scale contains 22 items divided into six sub-dimensions: medical treatment (4 items), definition (2 items), drug compliance (4 items), diet (2 items), lifestyle (5 items), and complications (5 items). Each item requests that participants respond either “right”, “false”, or “I have no idea”. True responses were assigned one point, while incorrect responses were assigned zero. The score ranged from zero to 22 and was converted to a grade point average out of 100. Higher scores indicate an increased understanding of HTN16. A score above 75% was considered good; a score between 50 and 75% was moderate, while a score below 50 was deemed low.
These measures (scores) were collected at baseline (T0) and at the end of the study (T1) in all patients.
Statistical analyses
The data was processed with the Statistical Package for Social Sciences (SPSS) version 20.0. The data distribution was determined using the Kolmogorov–Smirnov test. Quantitative variables were presented using mean values and standard deviations even for those with an abnormal distribution. Categorical variables were presented as frequencies and percentages. The experimental and control groups’ baseline data were compared applying the Pearson’s χ2 and student or Mann–Whitney tests, depending on the application conditions. The amelioration of the scores of knowledge was estimated by the difference (score T1—score T0). The HK-LS scores were compared between groups using the Mann–Whitney U test and throughout the same group using the Wilcoxon test. The significance threshold was fixed at P less than 0.05.
Ethical considerations
The Committee for the Protection of Persons granted its ethical approval. Before data collection, permission was obtained from the director of the general medicine department. Measures have been taken to respect participants’ rights and freedoms. Written informed consent was obtained from the patient for publication. A duplicate copy of the written consent could be obtained for inquiry by the Editor-in-Chief of this journal upon request. The confidentiality of the collected data, as well as the anonymity of the participants, are respected.
Results
Patients’ characteristics
In this RCT, 750 hypertensive patients were enrolled. They randomly assigned 500 patients to the experimental group and 250 to the control group. During the intervention, 111 patients were dropped out, including 71 from the experimental group and 40 from the control group. As a result, a total of 639 patients were involved in the study’s analysis (Fig. 1).
Figure 1.
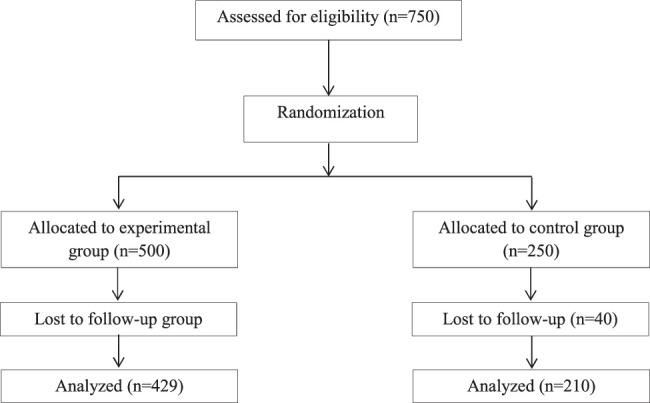
Flow diagram for study participants.
The comparison of the characteristics of the patients having followed the study protocol in the two groups demonstrated that the groups under consideration were homogeneous. The baseline socioeconomic characteristics and medical data of research participants are shown in Table 1.
Table 1.
Participants’ socio-demographic characteristics and medical data.
| Variables | Experimental group (n=429) | Control group (n=210) | P |
|---|---|---|---|
| Age (years) | 0.20a | ||
| Mean (SD) | 64.28 (8.5) | 63.3 (9.18) | |
| Sex, n, (%) | 0.20b | ||
| Male | 128 (29.8) | 73 (34.8) | |
| Female | 301 (70.2) | 127 (65.2) | |
| Level of education, n (%) | 0.51 b | ||
| Illiterate | 80 (18.6) | 48 (22.9) | |
| Primary | 238 (55.5) | 105 (50.0) | |
| Secondary | 95 (22.1) | 50 (23.8) | |
| University | 16 (3.7) | 7 (3.3) | |
| Occupation, n (%) | 0.06 b | ||
| Unemployed | 366 (85.3) | 167 (79.5) | |
| Employee | 63 (14.7) | 43 (20.5) | |
| Duration of Hypertension (years) | 0.23 a | ||
| Mean (SD) | 11.43 (8.21) | 10.62 (7.49) | |
| Systolic blood pressure (mmHg) | 0.59 a | ||
| Mean (SD) | 149.60 (14.50) | 150.3 (14.9) | |
| Diastolic blood pressure (mmHg) | 0.91 a | ||
| Mean (SD) | 84.16 (9.50) | 84.08 (8.70) | |
| Complications of hypertension, n (%) | 0.81 b | ||
| Yes | 58 (13.5) | 27 (12.9) | |
| No | 371 (86.5) | 183 (87.1) |
Student’s t-test.
Pearson’s χ2 test.
Knowledge about hypertension
Before the program implementation
Only 12.1% of participants had a good level of knowledge about HTN hypertension (12.8% for the experimental group, vs. 10.5% for the control group, P=0.57). While 75.5% showed a moderate level (Table 2).
Table 2.
Knowledge about hypertension among the experimental group/control group in pre and post-test.
| Pre-test | Post-test | |||||
|---|---|---|---|---|---|---|
| Total (N=639) | Experimental group (N=429) | Control group (N=210) | Total (N=639) | Experimental group (N=429) | Control group (N=210) | |
| D1: Definition of hypertension, n (%) | ||||||
| Low | 555 (86.9) | 367 (85.5) | 188 (98.5) | 294 (46.0) | 106 (24.7) | 188 (89.5) |
| Moderate | 0 | 0 | 0 | 104 (16.3) | 103 (24.0) | 1 (0.5) |
| High | 84 (13.1) | 62 (14.5) | 22 (10.5) | 241 (37.7) | 220 (51.3) | 21 (10.0) |
| P value | 0.16b | <0.001b | ||||
| D2: Treatment, n (%) | ||||||
| Low | 1 (0.2) | 1 (0.2) | 0 | 1 (0.2) | 1 (0.2) | 0 |
| Moderate | 4 (0.8) | 1 (0.2) | 3 (1.4) | 8 (1.3) | 4 (0.9) | 4 (1.9) |
| High | 634 (99.2) | 427 (99.5) | 207 (98.6) | 630 (98.5) | 424 (98.8) | 206 (98.1) |
| P value | 0.33a c | 0.45a c | ||||
| D3: Medication compliance, n (%) | ||||||
| Low | 456 (71.4) | 302 (70.4) | 154 (73.3) | 367 (57.4) | 215 (50.1) | 152 (72.4) |
| Moderate | 151 (23.6) | 109 (25.4) | 42 (20.0) | 233 (36.5) | 190 (44.3) | 43 (20.5) |
| High | 32 (5.0) | 18 (4.2) | 14 (6.7) | 39 (6.1) | 24 (5.6) | 15 (7.1) |
| P value | 0.16b | <0.001b | ||||
| D4: Lifestyle, n (%) | ||||||
| Low | 519 (81.2) | 347 (80.9) | 172 (81.9) | 472 (73.9) | 304 (70.9) | 168 (80.0) |
| Moderate | 79 (12.4) | 58 (13.5) | 21 (10.0) | 130 (20.3) | 104 (24.2) | 26 (12.4) |
| High | 41 (6.4) | 24 (5.6) | 17 (8.1) | 37 (5.8) | 21 (4.9) | 16 (7.6) |
| P value | 0.24b | 0.001 b | ||||
| D5: Diet, n (%) | ||||||
| Low | 2 (0.3) | 1 (0.2) | 1 (0.5) | 2 (0.3) | 1 (0.2) | 1 (0.5) |
| Moderate | 5 (0.8) | 5 (1.2) | 0 | 9 (1.4) | 7 (1.6) | 2 (1.0) |
| High | 632 (98.9) | 423 (98.6) | 209 (99.5) | 628 (98.3) | 421 (98.1) | 207 (98.5) |
| P value | 0.43 a c | 0.69 a c | ||||
| D6: Complications, n (%) | ||||||
| Low | 499 (78.1) | 333 (77.6) | 166 (79.0) | 223 (34.9) | 58 (13.5) | 165 (78.6) |
| Moderate | 117 (18.3) | 79 (18.4) | 38 (18.1) | 103 (16.1) | 67 (15.6) | 36 (17.1) |
| High | 23 (3.6) | 17 (4.0) | 6 (2.9) | 313 (49.0) | 304 (70.9) | 9 (4.3) |
| P value | 0.77b | <0.001b | ||||
| Total Hypertension Knowledge Level Scale, n (%) | ||||||
| Low | 79 (12.4) | 55 (12.8) | 24 (11.4) | 34 (5.3) | 2 (0.5) | 32 (15.2) |
| Moderate | 483 (75.5) | 319 (74.4) | 164 (78.1) | 308 (48.2) | 154 (35.9) | 154 (73.3) |
| High | 77 (12.1) | 55 (12.8) | 22 (10.5) | 297 (46.5) | 273 (63.6) | 24 (11.4) |
| 0.57b | <0.001b | |||||
Fisher test.
Pearson test.
Low and moderate vs. High.
The dimensions concerning treatment and diet had the best scores (99.2% high scores for the treatment dimension and 98.9% high scores for the diet dimension). In contrast, the dimension of complications had the worst score. The details of all dimensions were resumed in Table 3. The final score of knowledge was not significantly different between the two groups (58.49% for the experimental group vs. 58.18% for the control group; P=0.635).
Table 3.
Knowledge about hypertension among the experimental group/control group in pre-test/post-test
| Variables | Experimental group (N=429) | Control group (N=210) | P a |
|---|---|---|---|
| D1: Definition of hypertension | |||
| Pre-test mean (SD) | 14.45 (35.20) | 10.47 (30.69) | 0.149 |
| Post-test mean (SD) | 63.28 (41.56) | 10.23 (30.18) | <0.0001 |
| Mean of differences | 48.8 (56.04) | −0.23 (44.4) | <0.0001 |
| P valueb | <0.0001 | 0.88 | |
| D2: Treatment | |||
| Pre-test mean (SD) | 99.76 (3.59) | 99.52 (3.96) | 0.18 |
| Post-test mean (SD) | 99.53 (4.53) | 99.36 (4.56) | 0.45 |
| Mean of differences | −0.23 (5.8) | −0.15 (6.09) | 0.86 |
| P valueb | 0.60 | 0.48 | |
| D3: Medication compliance | |||
| Pre-test mean (SD) | 44.28 (18.83) | 43.80 (20.78) | 0. 227 |
| Post-test mean (SD) | 51.74 (20.12) | 44.28 (21.17) | 0.000 |
| Mean of differences | 7.45 (27.08) | 0.47 (29.2) | <0.0001 |
| P valueb | 0.001 | <0.0001 | |
| D4: Lifestyle | |||
| Pre-test mean (SD) | 22.06 (30.13) | 25.06 (30.51) | 0.099 |
| Post-test mean (SD) | 42.73 (21.54) | 27.77 (30.68) | <0.0001 |
| Mean of differences | 20.58 (36.43) | 2.22 (43.3) | <0.0001 |
| P valueb | <0.0001 | 0.72 | |
| D5: Diet | |||
| Pre-test mean (SD) | 98.23 (6.47) | 97.46 (8.71) | 0.155 |
| Post-test mean (SD) | 98.56 (6.23) | 93.88 (10.48) | <0.0001 |
| Mean of differences | 0.34 (8.7) | −3.57 (14.09) | <0.0001 |
| P valueb | 0.37 | <0.0001 | |
| D6: Complications | |||
| Pre-test mean (SD) | 34.08 (20.18) | 33.52 (19.36) | 0.321 |
| Post-test mean (SD) | 78.55 (20.61) | 33.42 (20.06) | <0.0001 |
| Mean of differences | 43.9 (29.5) | −0.09 (26.6) | <0.0001 |
| P valueb | <0.0001 | 0.87 | |
| Total: Hypertension Knowledge Level Scale | |||
| Pre-test mean (SD) | 58.49 (11.99) | 58.18 (11.66) | 0.635 |
| Post-test mean (SD) | 76.94 (10.96) | 57.85 (11.72) | <0.0001 |
| Mean of differences | 18.3(16.75) | −0.32 (16.2) | <0.0001 |
| P valueb | <0.0001 | 0.993 | |
Mann–Whitney U test.
Wilcoxon test.
(Scores /100).
After the program implantation
Following the program’s deployment, the rate of good level of knowledge became 63.6% for the experimental group versus 11.4% for the control group, P<0.001) (Table 2).
For the experimental group, the Wilcoxon test showed a significant amelioration in the total score of the HK-LS (mean difference (MD): 18.3) and in 4 dimensions: Definition (MD: 48.8, P<0.0001), medical compliance (MD: 7.45; P=0.001), lifestyle (MD: 20.58, P<0.0001), and complications (MD: 43.9, P<0.0001) (Table 3).
The comparison of the two groups showed a significantly higher amelioration in the experimental group in the total score of the HK-LS (md for the experimental group: 18.3, versus (−0.32) for the control group, P<0.001). This amelioration in the experimental group was observed in all dimensions of the scale except the treatment dimension (Table 3).
Discussion
Key outcomes of the current study demonstrate the usefulness of the educational program in raising health-related knowledge among Tunisian patients with HTN. Furthermore, the results of this study revealed a notable lack of knowledge about HTN. Overall, the majority of this population (87.9%) has a moderate or low level of knowledge, while just 12.1% have a good level of knowledge.
Previous studies have pointed out that the minority of the patients with HTN had a good level of knowledge about HTN, which supports our findings. According to a Malaysian study, the great majority of patients had a poor or moderate level of HTN-related knowledge (32.8% and 51.3%, respectively), and only 15.9% had a good level of knowledge about HTN17. Besides, a study conducted in Indonesia showed that 85.9% of patients had moderate or a low level of knowledge, while only 14.1% had good knowledge about HTN18.
Understanding and recognizing the repercussions of a lack of knowledge in patients with HTN is required to restrain its long-term complications. Indeed, studies have demonstrated positive correlations between the patients’ level of knowledge and their attitude10. Other studies demonstrated associations between knowledge and blood pressure control19, self-efficacy and self-care practices6, dietary salt intake20, medication adherence21, and overall quality of life22.
Then, tailored interventions are implemented for patients to enhance their comprehension of the disease, which will ultimately be useful to control HTN. The current study’s findings demonstrated that, following program implementation, the rate of good level of knowledge became 63.6% for the experimental group versus 11.4% for the control group, P<0.001). For the experimental group, the results showed a significant amelioration in the total score of the HK-LS and in 4 dimensions (definition of HTN, medication compliance, complications, and lifestyle).The comparison of the two groups showed a significantly higher amelioration in the experimental group in the total score of the HK-LS. This amelioration in the experimental group was observed in all dimensions of the scale, except the treatment dimension. These results align with systemic reviews, which reveal that health education interventions improve the disease-related knowledge among those affected by non-transmissible illness residing in low-to-middle-income countries23, particularly those with HTN24,25.
Indeed, the exemplary approach for educating patients to enhance their level of knowledge remains unidentified due to the variety of educational techniques, suppliers, and subjects available. Recent studies demonstrated an improvement in knowledge in spite of adopting varied educational strategies and approaches, particularly health literacy programs via mobile phones25; theory-based interventions26; community-based interventions27; self-care home-based interventions28; and self-management programs29. Furthermore, the instructional strategy employed in the present research was self-care and self-management education through complementary approaches. Reviews revealed that these methods are effective in enhancing knowledge28,29.
Multiple experimental studies that partially or entirely address the issues discussed in the present RCT adequately prove the beneficial influence of health education on knowledge about HTN. According to an integrative review, HTN self-care interventions increase knowledge and improve home-based HTN management. Indeed, knowledge remained an excellent predictor for HTN management. In fact, moderate (OR=1.80, 95% CI 1.01–3.20, P=0.046) and good knowledge of HTN (OR=2.10, 95% CI 1.00–4.50, P=0.049) have been associated with improved HTN control. Hypertensive patients with good knowledge about HTN were 6.19 times more positively related to good self-care practices and 2.58 times more likely to engage in physical exercise. Furthermore, recognizing the negative impact of salt, alcohol, and smoking, as well as the positive effects of physical exercise, enhanced HTN control28.
The beneficial impact of health education interventions on knowledge is also confirmed by a systematic review and meta-analysis, proving that therapeutic education using mHealth was successful in enhancing the knowledge of HTN, managing drugs, improving self-efficacy, maintaining a healthy lifestyle, and allowing an earlier diagnosis of elevated blood pressure29. In addition, mHealth helps HTN patients become more conscious of their medical condition. In actuality, this type of technology has the ability to help attain the goal of universal community care by expanding accessibility and extending healthcare assistance to isolated communities as well as underprivileged regions29.
Although a variety of mobile health techniques have been described in the past few years, evidence on their widespread and beneficial implementation in low- and middle-income countries is limited and unexplored. The majority of the programs that have been previously applied in these regions are still insubstantial and on a pilot level, with insufficient proof of significant improvement methods, uncertain cost benefits, and ambiguous results for patients30. However, tailoring the programs of intervention to the specific requirements of the patients through customized care education will increase the intervention’s outcomes. In reality, communication is the cornerstone of all individualization protocols31.
Thus, our study revealed the significance of implementing therapeutic education among hypertensive patients in our country. The large sample size and the use of a specific Arabic scale (HK-LS) are the strongest points. However, certain constraints to this study need to be noted. The first is that this RCT occurred during the COVID-19 pandemic. In fact, this pandemic has an influence on HTN patients by disturbing both daily routine and typical medical care, including the management of chronic illnesses, especially HTN. But, in reality, for hypertensive patients, the pandemic intensified existing hurdles rather than creating new ones32. However, our findings have importance as they relate to a vulnerable population whose beliefs might help in preventing disease and its consequences. Cardiovascular risk factors, as well as knowledge about the diseases, serve as key elements in effectively implementing public health interventions33. Finally, the data were collected exclusively from one healthcare institution.
Accordingly, a Tunisian-specific interventional program has been implemented for this group with HTN. Then, it may be valuable in planning subsequent initiatives and developing public instructions. Programs of education, in combination with substantial assistance and devotion, is a crucial prevention plan that may contribute to promoting Tunisian community health34.
Conclusion
The findings of this RCT reveal a lack of health-related knowledge and prove the efficacy of educational initiative in enhancing knowledge of Tunisian patients with HTN. Significant improvements in the four domains of the HK-LS (definition of HTN, medication compliance, lifestyle, and complications) were observed following the deployment of an engaging and individualized strategy. Consequently, the study’s findings can help caregivers become more enthusiastic about supporting this group of vulnerable people as they cope with their medical conditions.
Ethical approval
Ethical approval was granted from the Committee for the Protection of Persons (CPP SUD N° 0472/2023).
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Source of funding
None.
Author contribution
All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript. F.T. : conceptualization, methodology, formal analysis, investigation, writing—original draft, project administration I.T.: conceptualization, methodology, formal analysis, writing—original draft. J.J.: methodology, formal analysis, validation, supervision, project administration. H.S.: methodology, formal analysis, validation, supervision, project administration.
Conflicts of interest disclosure
The authors declare no conflicts of interest.
Research registration unique identifying number (UIN)
Reaserchregistry10241, at 29/04/2024.
Guarantor
Fatma Turki.
Data availability statement
Not available.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Acknowledgement
The contributors of the study extend their appreciation to the director and the staff of the “National Fund for Social Security” Polyclinic of Sfax for the assistance they provided. Tunisia’s Ministry of Higher Education and Scientific Research, as well as the Ministry of Health, supported this research.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 11 October 2024
Contributor Information
Fatma Turki, Email: fatma.turki.kch@gmail.com.
Imen Turki, Email: imen_turki1992@hotmail.fr.
Jihen Jedidi, Email: jdiditrabelsijihen@gmail.com.
Houyem Said, Email: said_houyem@yahoo.fr.
References
- 1. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol 2020;16:223–237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Zhou B, Carrillo-Larco RM, Danaei G, et al. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021;398:957–980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Balouchi A, Rafsanjani MHAP, Al-Mutawaa K, et al. Hypertension and pre-hypertension in Middle East and North Africa (MENA): a meta-analysis of prevalence, awareness, treatment, and control. Curr Probl Cardiol juill 2022;47:101069. [DOI] [PubMed] [Google Scholar]
- 4. de Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care 2017;40:1273–1284. [DOI] [PubMed] [Google Scholar]
- 5. Estrada D, Sierra C, Soriano RM, et al. Grade of knowledge of hypertension in hypertensive patients. Enferm Clínica Engl Ed 2020;30:99–107. [DOI] [PubMed] [Google Scholar]
- 6. Darvishpour A, Mansour-ghanaei R, Mansouri F. The relationship between health literacy, self-efficacy, and self-care behaviors in older adults with hypertension in the north of Iran. HLRP Health Lit Res Pract 2022;6. [cité 12 mai 2024]. Disponible sur: https://journals.healio.com/ 10.3928/24748307-20221013-01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Zhang Q, Huang F, Zhang L, et al. The effect of high blood pressure-health literacy, self-management behavior, self-efficacy and social support on the health-related quality of life of Kazakh hypertension patients in a low-income rural area of China: a structural equation model. BMC Public Health 2021;21:1114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Delavar F, Pashaeypoor S, Negarandeh R. The effects of self-management education tailored to health literacy on medication adherence and blood pressure control among elderly people with primary hypertension: a randomized controlled trial. Patient Educ Couns 2020;103:336–342. [DOI] [PubMed] [Google Scholar]
- 9. Gaffari-fam S, Babazadeh T, Oliaei S, et al. Adherence to a health literacy and healthy lifestyle with improved blood pressure control in Iran. Patient Prefer Adherence 2020;14:499–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Machaalani M, Seifeddine H, Ali A, et al. Knowledge, attitude, and practice toward hypertension among hypertensive patients residing in Lebanon. Vasc Health Risk Manag 2022;18:541–553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Essayagh T, Essayagh M, El Rhaffouli A, et al. Prevalence of uncontrolled blood pressure in Meknes, Morocco, and its associated risk factors in 2017. PLoS One 2019;14:e0220710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Lugo-Mata ÁR, Urich-Landeta AS, Andrades-Pérez AL, et al. Factors associated with the level of knowledge about hypertension in primary care patients. Med Univ 2017;19:184–188. [Google Scholar]
- 13. Abedini S, Pourjalil F, Mohseni S. The impact of an educational program based on the BASNEF model on knowledge and self-care behaviors of patients with hypertension. Health Scope 2020;9. [cité 21 nov 2023]. Disponible sur: https://brieflands.com/articles/healthscope-95588.html#abstract [Google Scholar]
- 14. Kurt D, Gurdogan EP. The effect of self-management support on knowledge level, treatment compliance and self-care management in patients with hypertension. AJAN - Aust J Adv Nurs 2022;39. [cité 21 nov 2023];Disponible sur: https://www.ajan.com.au [Google Scholar]
- 15. Walsh JL, Aridi H, Fathallah J, et al. Impact of a hospital-based educational intervention on dietary salt-related knowledge and behaviour in a cardiac care unit population in Lebanon. Cardiovasc Diagn Ther 2018;8:14655–14155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Eshah NF, Al-Daken LI. Assessing public’s knowledge about hypertension in a community-dwelling sample. J Cardiovasc Nurs 2016;31:158–165. [DOI] [PubMed] [Google Scholar]
- 17. Mohammed AH, Hassan BAR, Suhaimi AM, et al. Hypertension knowledge, awareness, and attitude among the hypertensive population in Kuala Lumpur and rural areas in Selangor, Malaysia. J Public Health avr 2021;29:443–450. [Google Scholar]
- 18. Anam K. Examines the correlation between knowledge, demographic characteristics, and hypertension incidence among outpatients in a community health center located in Banjarmasin, Indonesia. Pak J Life Soc Sci PJLSS 2023;21. [cité 11 mai 2024];Disponible sur: https://www.pjlss.edu.pk/articles/2023_1/54-61.htm [Google Scholar]
- 19. Ragavan RS, Joshi R, Evans RG, et al. Additive association of knowledge and awareness on control of hypertension: a cross-sectional survey in rural India. J Hypertens 2021;39:107–116. [DOI] [PubMed] [Google Scholar]
- 20. Mohd Isa D, Shahar S, He FJ, et al. Associations of health literacy with blood pressure and dietary salt intake among adults: a systematic review. Nutrients 2021;13:4534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Guo A, Jin H, Mao J, et al. Impact of health literacy and social support on medication adherence in patients with hypertension: a cross-sectional community-based study. BMC Cardiovasc Disord 2023;23:93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Chen YY, Lee MC, Wu SFV, et al. Disease knowledge, self-efficacy, and quality of life in patient with hypertensive nephropathy. Clin Nurs Res 2022;31:1179–1188. [DOI] [PubMed] [Google Scholar]
- 23. Heine M, Lategan F, Erasmus M, et al. Health education interventions to promote health literacy in adults with selected non‐communicable diseases living in low‐to‐middle income countries: a systematic review and meta‐analysis. J Eval Clin Pract 2021;27:1417–1428. [DOI] [PubMed] [Google Scholar]
- 24. Kappes M, Espinoza P, Jara V, et al. Nurse-led telehealth intervention effectiveness on reducing hypertension: a systematic review. BMC Nurs 2023;22:19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Israfil I, Kusnanto K, Yusuf A, et al. The effect of health education intervention through mobile phone on hypertension patients : a systematic review. Med J Malaysia 2022;77:232–236. [PubMed] [Google Scholar]
- 26. Mohebbi B, Sabouri M, Tol A. Application of health education and promotion theory-based interventions on patients with cardiovascular disease: a systematic review. J Educ Health Promot 2021;10:236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ndejjo R, Hassen HY, Wanyenze RK, et al. Community-based interventions for cardiovascular disease prevention in low-and middle-income countries: a systematic review. Public Health Rev 2021;42:1604018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Konlan KD, Shin J. Determinants of self-care and home-based management of hypertension: an integrative review. Glob Heart 2023;18:16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Li R, Liang N, Bu F, et al. The effectiveness of self-management of hypertension in adults using mobile health: systematic review and meta-analysis. JMIR MHealth UHealth 2020;8:e17776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Istepanian RSH. Mobile health (m-Health) in retrospect: the known unknowns. Int J Environ Res Public Health 2022;19:3747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ricci L, Villegente J, Loyal D, et al. Tailored patient therapeutic educational interventions: a patient‐centred communication model. Health Expect 2022;25:276–289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Foster M, Etchin A, Pope C, et al. The impact of COVID-19 on hypertension and hypertension medication adherence among underrepresented racial and ethnic groups: a scoping review. Curr Hypertens Rep 2023;25:385–394. [DOI] [PubMed] [Google Scholar]
- 33. Wernly B, Wernly S, Magnano A, et al. Cardiovascular health care and health literacy among immigrants in Europe: a review of challenges and opportunities during the COVID-19 pandemic. J Public Health 2022;30:1285–1291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Abid L, Hammami R, Chamtouri I, et al. Epidemiologic features and management of hypertension in Tunisia, the results from the Hypertension National Registry (NaTuRe HTN). BMC Cardiovasc Disord 2022;22:131. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not available.