

Abstract
This Points to Remember column discusses the differential diagnosis of acute myocardial infarction with normal coronary arteries, one example of which is Takotsubo cardiomyopathy. In the case presented below, the diagnosis of Takotsubo cardiomyopathy was based on the characteristic appearance of the left ventricular apical bulging, normal coronary arteries, and the resolution of the wall motion abnormalities within a relatively short period of time.
Keywords: Takotsubo cardiomyopathy, stress cardiomyopathy, broken heart syndrome, intramyocardial small vessel disease
A 73-year-old female presented with dull substernal chest pain described as tightness and pressure; it began several hours prior to admission and was described as 9/10 in intensity and radiating to the back. She was short of breath and had profuse diaphoresis and lightheadedness, symptoms she had never experienced before. She had a prior history of hypertension, medically controlled, but no other risk factors for coronary artery disease. Home medication was losartan 50 mg daily. Her physical examination showed blood pressure of 100/60 mm Hg and heart rate of 102 bpm and was otherwise unremarkable. An electrocardiogram showed sinus tachycardia with nonspecific ST segment depression in the precordial leads. In the emergency department, troponin T was elevated. She was admitted with a presumptive diagnosis of acute coronary syndrome.
She was placed on aspirin and intravenous heparin and given fluids. Sequential troponin T confirmed the diagnosis of acute non-ST-elevation myocardial infarction (NSTEMI). Subsequent electrocardiograms showed T wave inversion across the precordial leads.
An echocardiogram showed a normal-sized left ventricle with preserved global systolic function with an ejection fraction of 50% to 55%. There were significant regional wall motion abnormalities with severe hypokinesis of the distal septum and apex. Right ventricular function was normal and valve structure and function were normal with only mild mitral regurgitation.
Cardiac catheterization was performed the following day. The left main and left and right coronary arteries showed minimal luminal irregularity with no significant stenosis (Figures 1, 2). Left ventriculography showed systolic ballooning of the apex with otherwise normal ventricular contraction (Figure 3).
Figures 1, 2.
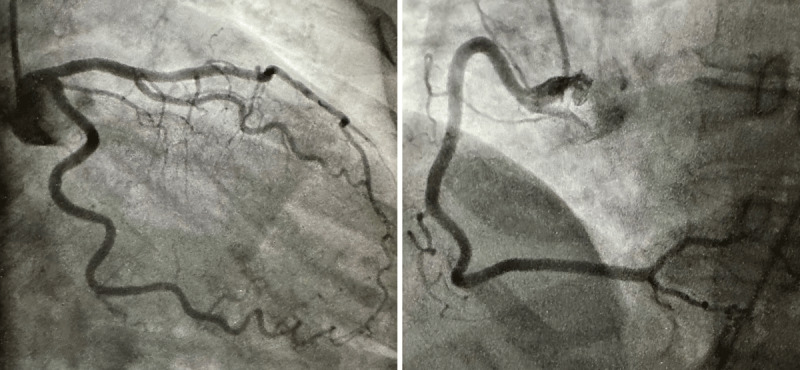
The left main and left/right coronary arteries showed minimal luminal irregularity with no significant stenosis.
Figure 3.
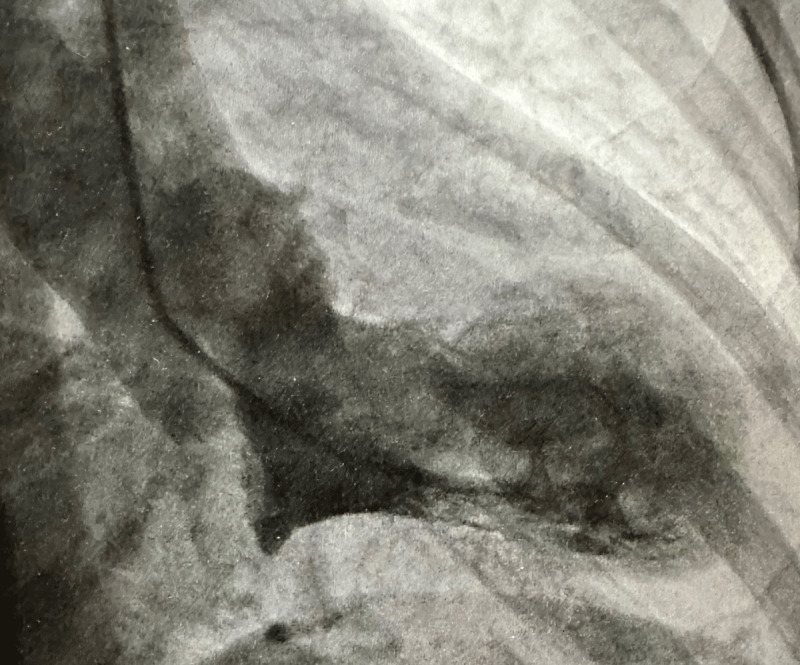
Left ventriculography showed systolic ballooning of the apex with otherwise normal ventricular contraction.
Based on these findings, a diagnosis of Takotsubo cardiomyopathy was made. A retrospective history of the recent death of a friend was noted.
Two days later, the patient was discharged on aspirin, clopidogrel, carvedilol, and losartan.
The patient was seen in follow-up 2 weeks, 1 month, and 2 months following admission and was clinically doing well. An echocardiogram done at 2 months showed normalization of left ventricular function and contraction with no evidence of regional wall motion abnormality.
Discussion
The differential diagnosis of acute myocardial infarction with normal coronary arteries includes the following1:
Transient mechanical vascular obstruction including coronary artery spasm, coronary embolism, in situ thrombosis, myocardial bridge, and coronary artery dissection
Intramyocardial small vessel disease including diabetes mellitus, collagen vascular diseases, infiltrative diseases, connective tissue diseases, and neuromuscular diseases
Abnormalities of supply and demand
Trauma with myocardial contusion
Takotsubo cardiomyopathy
Misinterpretation of the coronary angiogram
In this patient, the diagnosis of Takotsubo cardiomyopathy was correct based on the characteristic appearance of the left ventricular apical bulging,2 normal coronary arteries, and the resolution of the wall motion abnormalities within a relatively short period of time.
Points to Remember
The name comes from a Japanese fishing pot used to catch octopus called the “Tako-Tsubo” pot.
In many but not all patients, a history of an intense emotional or physical experience can be noted, which has led to the alternate names “Stress Cardiomyopathy” or “Broken Heart Syndrome.”
The syndrome can occur at any age in both men and women, but it mostly affects older women.
The signs and symptoms are similar to those of a heart attack.
The rise of troponin is often lower than the degree of left ventricular dysfunction would suggest.
Since the exact mechanism of the syndrome is unclear, so too are the treatment options. Treatment consists of medications to reduce afterload, aspirin, and high-dose statins. Occasionally nitrates, diuretics, and beta blockers may be needed. Many patients also receive antiplatelet or anticoagulant drugs, generally for a short period of time and based on the possibility that a transient clot accounted for the findings.3
Although the prognosis for full recovery is very good in most, some patients with large areas of akinesis and low ejection fraction may develop congestive heart failure, arrhythmias, and cardiogenic shock. Intense treatment with guideline-directed medical therapy for congestive heart failure will on occasion be necessary.4
Competing Interests
The author has no competing interests to declare.
References
- 1.Raizner, AE, Chahine RA. Myocardial Infarction With Normal Coronary Arteries. In: Hurst JW, editor. The Heart. New York, NY: McGraw-Hill Health Professions Division; 1979. [Google Scholar]
- 2.Sato TH, Uchida T, Dote KMI. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm. In: Kodama, K, Haze, K, Hori, M, editors. Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure. Tokyo, Japan: Kagakuhyoronsha Publishing Co; 1990. p. 56-64. [Google Scholar]
- 3.Singh T, Khan H, Gamble DT, Scally C, Newby DE, Dawson D. Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications. Circulation. 2022. Mar 29;145(13):1002-1019. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ghadri JR, Wittstein IS, Prasad A, et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur Heart J. 2018. Jun 7;39(22):2032-2046. doi: [DOI] [PMC free article] [PubMed] [Google Scholar]