

Abstract
Introduction:
The aim of this study is to illustrate a case in which the use of a dorsal spanning plate followed by volar plating may be indicated in the setting of a complex intra-articular distal radius fracture. Combined dorsal spanning plate and volar plating is a rare procedure reserved typically for comminuted fractures of the distal radius. This case highlights the first reported incidence in which a dorsal spanning plate of a distal radius fracture resulted in the volar displacement of the fragments, requiring subsequent volar plating. In the end, the outcome was favorable, as the follow-up imaging displayed good bone healing and union with minimal complications.
Case Report:
A 52-year-old male presented to the ED at our institution following a traumatic fall onto his left upper extremity. Radiographic imaging revealed fractures at the midshaft of the humerus as well as a very distal three-part intra-articular radius fracture. Due to the nature of the patient’s distal radius fracture, initial fixation with a dorsal spanning plate was planned. However, follow-up imaging 3 weeks postoperatively revealed volar displacement of his fracture, so the patient underwent open reduction internal fixation with a volar distal radius plate. Follow-up over the next few months displayed a union of the fracture fragments and the dorsal spanning plate was removed 4 months postoperatively with imaging showing no complications.
Conclusion:
We present this case to highlight the complication of volar displacement that may follow initial dorsal spanning plate fixation of a three-part intra-articular distal radius fracture that can be resolved with the addition of a volar plate, as well as possible indications for combined dorsal spanning plate and volar plate fixation of complex distal radius fractures at the time of initial fixation.
Keywords: Distal radius, volar plate, spanning plate, fracture, comminution, intra-articular fracture
Learning Point of the Article:
Dorsal spanning plate fixation with subsequent volar plating of a comminuted distal radius fracture can be a viable option in patients with complex fracture patterns.
Introduction
Distal radius fractures (DRFs) are a common orthopedic injury with pediatric and elderly populations being at the greatest risk due to underdeveloped skeletal structure in children and the prevalence of osteoporosis in the elderly [1]. The most common mechanism of injury in the geriatric population is a low-energy fall from a standing position onto a dorsally outstretched hand, whereas in younger populations this typically results from high-energy trauma [1]. Current treatments of DRFs consist of operative and non-operative management, although there is no consensus on which is best and in many cases, treatment modality is dependent on the surgeon and specific patient case including the amount of fracture displacement. Non-operative treatments include closed reduction with plaster casting or splint, but studies have shown significantly greater radial deviation and ulnar variance in patients with non-surgical treatment of DRF compared to patients with surgical treatment [2]. Surgical techniques for DRF treatment include intramedullary fixation, external fixation, open reduction and internal fixation (ORIF), and arthroscopic fixation [3]. Intra-articular distal radius fractures are a subset of DRFs that involve fracture propagation into the wrist joint itself. These types of fractures indicate a high-energy trauma that are often difficult to manage conservatively and are typically treated operatively. Techniques for intra-articular DRFs include closed reduction and casting, pins, and plaster, percutaneous pinning, external fixation, and the most commonly used management technique of ORIF. ORIF is often done with volar plating and has been found to have better outcomes due to early motion and lesser complication rates of tendon irritation and rupture [4]. It has been shown that nearly 80% of intra-articular distal radius fractures can be fixed by a volar plate alone [5]. However, severely comminuted or complicated fractures may require additional dorsal fixation with a dorsal plate. Current literature suggests that a double plate construct can be applied and is more effective in situations of lunate facet comminution with dorsoulnar fragmentation [5, 6]. Indications for this combined plating method with both a volar and dorsal plate are not well described in the literature, and dorsal spanning plate use for an intra-articular DRF is a less common technique [7, 8]. We present a case in which a patient with a comminuted intra-articular distal radius fracture required combined dorsal spanning and volar plating to fully capture and reduce this fracture.
Case Report
A 52-year-old male presented to the emergency department (ED) at our institution following a traumatic fall. The patient stated he was retrieving something from his attic on an approximately 4-foot-tall ladder when he fell from the ladder onto the concrete below on his left arm and shoulder. He felt immediate pain and a “spasm” sensation in his left upper extremity. A physical examination revealed pain and swelling of his left wrist along with observable deformity and pain of the mid left humerus. There was no extremity edema or loss of sensation noted. There was no deformity of the left shoulder or clavicle. Subsequent X-rays of his left wrist revealed a transverse midshaft left humerus fracture as well as a very distal intra-articular left distal radius fracture (Fig. 1). Due to the polytrauma aspect of his upper extremity, operative fixation was indicated and discussed with the patient to which he consented. Due to the short segment and comminuted distal radius fracture pattern, a dorsal spanning plate was decided to aid in holding the patient’s fracture pattern out to length with anticipated ligamentotaxis. The initial thought was that there would not be sufficient bone stock given the comminution for a volar plate or rim plate, thus risking inadequate fixation and hardware failure. There could be an argument for a wrist-spanning external fixator; however, a dorsal spanning plate was the preferred treatment of choice by the attending physician over an external fixator due to the risk of injury to the superficial radial nerve. After a lengthy discussion with the patient including risks and benefits, the patient was agreeable to all aspects of this discussion and decision.
Figure 1.

Left wrist X-rays revealing distal intra-articular distal radius fracture.
The patient was taken to the operating room where general anesthesia and antibiotics were administered according to typical operating room protocol. Attention was first turned to fixation of the left distal radius. All soft tissue was elevated from the bony surfaces ensuring a smooth passageway for the plate without entrapment of any tendon. The fracture was reduced with traction. A 3.5 mm plate was passed along the dorsal aspect of the forearm and aligned proximally over the shaft of the radius and distally over the 3rd metacarpal (Fig. 2). Following this, the humerus was fixed in typical fashion with plate fixation and 8 appropriately sized cortical and locking screws. The patient recovered well postoperatively with minimal complaints of pain.
Figure 2.
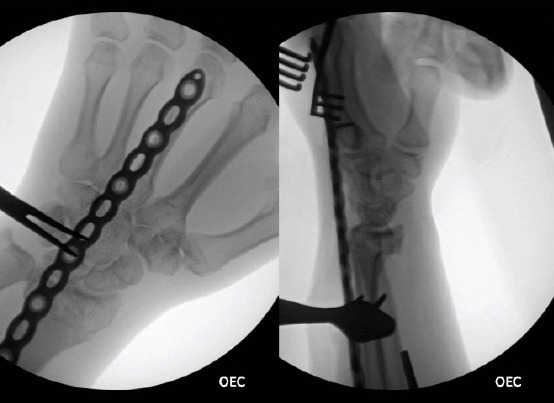
Intraoperative X-rays taken of left wrist distal radius fracture following dorsal spanning plate fixation.
He returned 4 weeks later for follow-up, with X-rays revealing volar displacement of his fracture (Fig. 3). The addition of volar plate fixation was offered to which the patient consented. After preparing the patient according to proper operative protocol and careful dissection to expose his distal radius fracture through a Volar Henry approach, a significantly comminuted distal radius fracture was found. Attempts to reduce the volar displaced fragment were performed. We made sure to capture and buttress the comminuted fracture pieces of the distal aspect of the volar plate knowing that we would have limited fixation to put screws into the distal row of the plate. A single locking screw was able to be placed in the distal row to capture the largest fragment volar aspect (Fig. 4). The patient tolerated the procedure well and was met with no post-operative complications.
Figure 3.

X-rays at 4-week follow-up after initial dorsal spanning plate fixation reveal volar displacement of the fracture.
Figure 4.
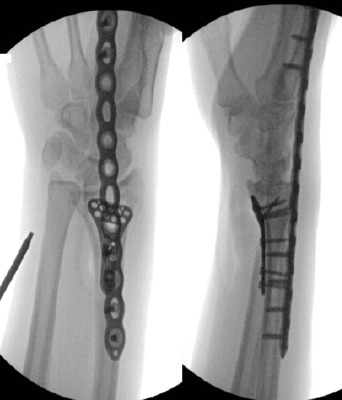
Intraoperative X-ray imaging of left wrist combined volar plating and dorsal spanning plate.
Follow-up imaging 3 months postoperatively revealed adequate healing and union of his fracture, the patient was in minimal pain and was still in a splint (Fig. 5). The patient returned 4 months postoperatively for removal of the dorsal spanning plate and underwent manipulation under anesthesia simultaneously. It is known that both dorsal spanning plates and external fixators may lead to stiffness of the wrist joint, osteopenia throughout the distal arm and hand, and atrophy of the surrounding forearm and hand musculature. His surgical procedure was uneventful, and the dorsal spanning plate was removed without any complications intraoperatively or postoperatively (Fig. 6). Patient was seen 2 weeks postoperatively after removal of the dorsal spanning plate with adequate pain control and reasonable post-surgical range of motion, pain, and tenderness. The patient had 35° of flexion in the operated wrist and 45° of extension, the plan at this time was to start therapy soon to restore the range of motion. The patient was referred to physical therapy for mobilization of the wrist joint and strengthening of the forearm musculature. He was advised to return to the clinic as needed if he had any issues with his range of motion. The patient did not follow up and is presumed to be doing well. Mid-term follow-up outside the perioperative period is a limitation of this report.
Figure 5.

Follow up at 3 months after the addition of a volar plate showing good bone healing and union.
Figure 6.

Intraoperative X-ray of the left wrist following removal of the dorsal spanning plate.
Discussion
Intra-articular distal radial fractures are one of the most common fractures [9, 10]. These fractures are projected to continue increasing in incidence as participation in sports-related activities increases and as life expectancy increases as well [1].
Treatment of an intra-articular DRF with a volar locking plate or dorsal locking plate is well-documented in the current literature [11]. In some cases, fractures that cannot be captured with a traditional volar plate may implement the use of a dorsal spanning plate. However, there is limited documentation of intra-articular distal radius fractures fixated with a volar locking plate combined with a dorsal wrist-spanning plate. In addition, all reported cases were with either concomitant volar plating and dorsal spanning plate or with volar plating initially before dorsal spanning plate use in a later surgery [7, 8, 12]. Indications for dorsal spanning plate use in the setting of a distal radius fracture were up to the surgeon’s discretion at the time or as a salvage option in a fracture that was initially treated but presented with non-union [7, 8]. We present this case as an indication for initial dorsal spanning plate fixation of a complex intra-articular distal radius fracture followed by the addition of a volar plate to fully capture the fracture.
The case described here was a complex, polytrauma patient with a comminuted intra-articular distal radius fracture. Fixation with volar plating or dorsal plating alone would not have been able to fully capture the extremely distal fracture. Initial fixation with a dorsal spanning plate allowed for excellent restoration of volar tilt and radial height to be achieved. Subsequent volar plating allowed for adequate reduction of the displaced radial fragments.
Golden et al. describe the use of a dorsal spanning plate in the management of a polytraumatized patient well for distal radius fractures. An added benefit discussed is the use of a dorsal spanning plate in combination with other fixation techniques such as volar plating [13].
External fixators and Kirschner wires are also viable and effective options for the fixation of distal radius fractures in addition to dorsal spanning plating. However, the literature does not provide consensus on technique but seems to favor external fixators in more simple fracture patterns [14]. Oftentimes, treatment modalities are guided by surgeon training and preference. Several studies show that more complex fracture patterns of the distal radius demonstrate better radiographic outcomes and union rates with dorsal spanning plate and staged plating fixation [14-16]. One study comparing external fixation to bridge plating revealed an increased complication rate in the external fixation group of 33.3% compared to 11.5% [15]. Complications unique to the use of external fixators include pin site infections which can be treated with increasing pin care and oral antibiotics. If left untreated, there is a risk of pin loosening and potential loosening of the external fixator construct. Mohamed et al. also discussed how the external fixator group noted two patients that developed chronic regional pain syndrome, whereas there was zero in the bridge plating group [15].
Given the complexity of the patient’s fracture pattern, it was felt that initial dorsal spanning plate fixation gave the most optimal chance at fracture healing. While dorsal spanning plate fixation may have delayed mobilization of the wrist joint in this patient, literature has shown that there are no functional outcome differences in varying immobilization periods following treatment for a distal radius fracture [17].
Our patient case described here supports their statement in that an initial dorsal spanning plate followed by volar plating was successful in fixation and achieving the union of an intra-articular distal radius fracture with minimal complications.
Conclusion
Each patient’s trauma and fracture is different, and treatment of distal radial fractures should be determined by the surgeon based on specific radiograph findings and intraoperative considerations. However, the case presented here offers a fixation method for complex comminuted intra-articular distal radius fractures with an initial dorsal spanning plate followed by subsequent volar plating.
Clinical Message.
This case report highlights a unique situation in which an initial 3-part intra-articular distal radius fracture could not be fully captured and reduced with a traditional volar plate. An initial dorsal spanning plate was used which initially demonstrated proper fixation of the fracture. However, follow-up X-rays revealed volar displacement of the fracture which required subsequent combined volar plating. Indications for the use of a dorsal spanning plate in distal radius fractures are poorly highlighted in literature and the authors feel that this case highlights a situation in which it can be indicated.
Biography



Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report
References
- 1.Nellans KW, Kowalski E, Chung KC. The epidemiology of distal radius fractures. Hand Clin. 2012;28:113–25. doi: 10.1016/j.hcl.2012.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ju JH, Jin GZ, Li GX, Hu HY, Hou RX. Comparison of treatment outcomes between nonsurgical and surgical treatment of distal radius fracture in elderly: A systematic review and meta-analysis. Langenbecks Arch Surg. 2015;400:767–79. doi: 10.1007/s00423-015-1324-9. [DOI] [PubMed] [Google Scholar]
- 3.He B, Tian X, Ji G, Han A. Comparison of outcomes between nonsurgical and surgical treatment of distal radius fracture: A systematic review update and meta-analysis. Arch Orthop Trauma Surg. 2020;140:1143–53. doi: 10.1007/s00402-020-03487-3. [DOI] [PubMed] [Google Scholar]
- 4.Chhabra AB, Yildirim B. Adult distal radius fracture management. J Am Acad Orthop Surg. 2021;29:e1105–16. doi: 10.5435/JAAOS-D-20-01335. [DOI] [PubMed] [Google Scholar]
- 5.Hadzhinikolova M, Zderic I, Ciric D, Barcik JP, Enchev D, Baltov A, et al. Volar versus combined dorsal and volar plate fixation of complex intraarticular distal radius fractures with small dorsoulnar fragment - a biomechanical study. BMC Musculoskelet Disord. 2022;23:35. doi: 10.1186/s12891-021-04989-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Senehi R, Walsh J. Technique: Dorsal spanning wrist plate. J Orthop Trauma. 2021;35:S22–3. doi: 10.1097/BOT.0000000000002157. [DOI] [PubMed] [Google Scholar]
- 7.Bradley H, Rodriguez J, Ahn J, Sammer D, Golden A, Koehler D. Evaluation of radiographic parameters following dorsal wrist-spanning plate fixation of distal radius fractures to the second versus third metacarpal. J Hand Surg Am. 2022;48:10. doi: 10.1016/j.jhsa.2022.03.008. [DOI] [PubMed] [Google Scholar]
- 8.Mithani SK, Srinivasan RC, Kamal R, Richard MJ, Leversedge FJ, Ruch DS. Salvage of distal radius nonunion with a dorsal spanning distraction plate. J Hand Surg Am. 2014;39:981–4. doi: 10.1016/j.jhsa.2014.02.006. [DOI] [PubMed] [Google Scholar]
- 9.Rundgren J, Bojan A, Mellstrand Navarro C, Enocson A. Epidemiology, classification, treatment and mortality of distal radius fractures in adults: An observational study of 23,394 fractures from the national Swedish fracture register. BMC Musculoskelet Disord. 2020;21:88. doi: 10.1186/s12891-020-3097-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury. 2006;37:691–7. doi: 10.1016/j.injury.2006.04.130. [DOI] [PubMed] [Google Scholar]
- 11.Ring D, Prommersberger K, Jupiter JB. Combined dorsal and volar plate fixation of complex fractures of the distal part of the radius. J Bone Joint Surg Am. 2005;87(Suppl 1):195–212. doi: 10.2106/JBJS.E.00249. [DOI] [PubMed] [Google Scholar]
- 12.O'Sullivan D, Carroll P, Galbraith J. A case of a combined distal radius and lunate fracture in association with Kienböck's disease. Cureus. 2022;14:e31161. doi: 10.7759/cureus.31161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Golden AS, Kapilow JM. Distal radius fractures and the dorsal spanning plate in the management of the polytraumatized patient. J Orthop Trauma. 2021;35:S6–10. doi: 10.1097/BOT.0000000000002204. [DOI] [PubMed] [Google Scholar]
- 14.Brennan SA, Kiernan C, Beecher S, O'Reilly RT, Devitt BM, Kearns SR, et al. Volar plate versus k-wire fixation of distal radius fractures. Injury. 2016;47:372–6. doi: 10.1016/j.injury.2015.08.040. [DOI] [PubMed] [Google Scholar]
- 15.Mohamed MA, Abdel-Wanis ME, Said E, Abdel-Aziz IA, Ahmed AM, Addosooki A. Dorsal bridge plating versus bridging external fixation for management of complex distal radius fractures. Injury. 2022;53:3344–51. doi: 10.1016/j.injury.2022.08.010. [DOI] [PubMed] [Google Scholar]
- 16.Ficke B, Ransom EF, Hess MC, Moon AS, McKissack HM, Shah A, et al. Outcomes of staged treatment for complex distal radius fractures. Cureus. 2018;10:e3273. doi: 10.7759/cureus.3273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Quadlbauer S, Pezzei C, Jurkowitsch J, Rosenauer R, Kolmayr B, Keuchel T, et al. Rehabilitation after distal radius fractures: Is there a need for immobilization and physiotherapy? Arch Orthop Trauma Surg. 2020;140:651–63. doi: 10.1007/s00402-020-03367-w. [DOI] [PubMed] [Google Scholar]