

Abstract
Introduction:
The two techniques to fix a torn ACL are the Transportal and All-Inside Techniques. However, the argument about which method is better for functional outcomes keeps going on. The aim was to look at how well these two treatments worked and their effects. We hypothesized that All-Inside and Transportal ACL reconstruction procedures would yield similar functional results.
Materials and Methods:
The study included 45 patients with ACL insufficiency from AIIMS, Raipur, India. Half of each ACL approach was represented by 22 AI and 23 TP participants, randomly assigned to each group. Preoperative and post-operative VAS, IKDC, and range of motion were determined at 1, 3, and 6 months. The study used IBM SPSS v20 for Data Analysis, comparing two groups using a t-test. P < 0.05 was fixed for Statistical significance.
Results:
The study was dominated by young males (86.7%, 18–30 years), mainly students (44.4%). Comparable IKDC scores over time (P = 0.628); significant VAS score difference (P = 0.001). A similar movement range (P = 0.153) was observed. AI group had slightly smaller grafts (non-significant, P = 0.235). Similar Lachmann Grade distributions pre- and post-surgery; no significant post-operative complication in either group.
Conclusion:
When comparing the methods’ functionalities, no statistically significant gaps emerged. All-Inside approach preserves bone and gracilis tendon, reduces post-operative pain, and strengthens knee flexors. Although, early rehabilitation favors all inside, both methods are equally effective over time. In comparison to the traditional Transportal Technique, All Inside has a greater learning curve and costs more.
Keywords: ACL Reconstruction, anterior cruciate ligament, Transportal Technique, All-Inside Technique, tibiofemoral joint, randomized controlled trial, knee surgery etc
Learning Point of the Article:
The study reinforces that both All-Inside (AI) and Transportal (TP) ACL reconstruction techniques offer comparable functional outcomes, as measured by IKDC scores and range of motion.
Introduction
The ACL prevents the tibia from sliding anteriorly relative to the femur, ensuring appropriate knee function. Patients with ACL tears undergo ACLR, a surgical technique that fixes knee stability and function using a graft from the patient or a donor. ACL tears are prevalent in sports [1]. In addition to physical activities, road traffic accidents (RTA) contribute to ACL injuries in India [2]. According to Brophy, around 2 hundred thousand ACLRs are performed annually in the US [3]. Surgical procedures cost close to $20,000 each, totaling $4 billion annually. The ACL injury incidence is equally significant in non-athlete individuals [4].
Tearing an ACL not only hinders the patient’s ability to do everyday tasks but also potentially creates significant financial and medical challenges. Previous study indicates that a significant proportion (31%) of the individuals with ACL injuries had a notable level of autonomous walking disability [5]. In addition, 44% of these patients had moderate to severe impairments in their ability to conduct daily basic activities. Furthermore, a significant majority of individuals, namely 77%, had the inability to resume their athletic endeavor’s at the same degree of intensity after their accident. There is a link between ACL damage and a greater incidence of knee osteoarthritis, which might lead to a reduction in mobility and independence [6, 7]. It has also been found that sportspersons who have had ACL torn are more likely to display symptoms of knee osteoarthritis early than their non-athletic counterparts [8]. The prevalence of ACL damage remains uncertain, as shown by Meisterling et al. [9].
According to Holm [10], despite undergoing surgical repair, a significant proportion of persons, roughly 79%, experience the development of knee osteoarthritis. In addition, after 2 years, about 20% of these individuals suffer from reinjury. The high expense of medical care and the dread of a second injury or the onset of arthritis have raised the stakes in the sporting world. Approximately 25% of young individuals who have ACL damage may encounter a subsequent ACL injury throughout their athletic endeavor’s. In addition, these athletes tend to spend a greater amount of time on the disabled list (DL), around 50% more than their counterparts who did not previously sustain a knee injury. Despite the continuous study aimed at identifying the contributing variables to possible knee injuries in athletes, the occurrence of such injuries persists, and the existing management and preventative methods prove ineffective. Consequently, the occurrence of a knee injury, particularly one affecting the ACL, has a significant influence on subsequent athletic performance. There is a pressing need for a precise functional assessment instrument and intervention to effectively address the current trend of injuries and ascertain the elements that contribute to athletes’ susceptibility to such injuries.
The investigation aims to compare the functional outcomes (Range of Movement, Pain employing the VAS scale, subjective functional results using the IKDC score) of the Transportal Technique and All-Inside Technique in patients undergoing arthroscopic ACLR.
Materials and Methodology
The design of the study is a randomized control trial and randomization was achieved using a table of random numbers. The study was conducted for a period of 2 years after obtaining ethical clearance approval, sample collection – 12 months, follow-up – 6 months. The population of the study consisted of all patients who presented in the Department of orthopedics with ACL insufficiency after meeting the inclusion and exclusion criteria. The functional outcomes were assessed with IKDC scores, VAS Scores, and range of movement (Gauged by Goniometer).
Participants
Patients with Torn ACL (Imaging and clinically Diagnosed) were recruited for between the age group of 18–45 years, were willing to give consent, and had Grades II to III and the Insufficiency was symptomatic. The study was gathered at the Department of Orthopedics. The participants were then allocated to study group I (AIT) and group II (TPT) as per the table of random numbers to achieve randomization.
<H2>Exclusion criteria
Subjects were excluded on these points:(I) Not willing to study, (ii) Diabetes, hypertension, immunosuppressive disorders, Bleeding disorders, (iii) Multi ligament injury, (iv) Signs of infection, and (v) ACL injury associated with fracture.
Interventions
All Inside ACL reconstruction
The All-Inside Technique involves creating tunnels and placing the graft entirely from within the joint. Lubowitz et al., [11] used the GraftLink approach to create a “second-generation All-Inside ACLR” method. The retrograde drilling technique necessitates the creation of distinct tibial and femoral sockets, which are then secured using “cortical suspension button devices on both the tibia and femur” for graft fixation. The graft construct distinguishes the current method from its predecessors. A graft preparation station is used to aid in the suturing of a “quadrupled tendon” into a loop shape, which is then attached to a suspensory fixation device on both ends, similar to the connecting chain links. The approach described by McCarthy et al. [12] has been modified to perform ACLR in “skeletally immature individuals” with epiphyseal involvement. GraftLink, the current AI ACLR method, owes much to the advancement of 2nd-gen “cortical suspensory fixation devices.” These tools include movable graft loops that, after the button is turned, attach the graft to the cortex by drawing it into the socket. To ensure that as much of the graft as possible is incorporated into the socket, this tool enables tensioning of the graft after it has been inserted.
The use of sockets, as opposed to whole bone tunnels, conserves bone integrity, a factor that might be advantageous in scenarios necessitating future revision reconstruction or in the context of numerous ligament reconstruction procedures. Furthermore, it has been suggested by Benea et al. [13] that employing this approach may lead to a decrease in post-operative discomfort and edema due to the avoidance of any damage to the extra-articular cortices and periosteum. The other advantages of this ACLR technique include bone preservation technique, requiring a shorter graft length compared to the Transportal Technique, facilitated graft tensioning through suspensory fixation devices, and improved cosmetic appearance. The All-Inside Technique has been identified as having several notable drawbacks. Firstly, it presents a steep learning curve due to its inherent technical complexity. Second, there is a potential risk of the graft “bottoming out,” which can lead to insufficient tension. Last but not least, the expensive nature of this method may be traced back to the need for a special retrograde drill targeting equipment for each tunnel.
The patient is placed in a face-up posture after receiving spinal/epidural anesthesia. One of the tourniquet’s posts goes just outside the knee. To maintain a knee bend of around 90 degrees, a foot roll is used. Diagnostic tests are performed.
Diagnostic arthroscopy is done. ACL tear is confirmed. Other associated ligament tears like PCL and collaterals are checked for their integrity. Meniscus are then probed for any tears and also, and we check for RAMP lesions. Once the diagnosis is confirmed, we go to the next step of graft preparation.
Preparation for graft harvest
The incision is made at a location that is one finger’s width below and one finger’s breadth medial to the tibial tuberosity. Pes ansarinus is identified. Gracilis is proximal whereas semitendinosus is found to be distal. Usually in All-Inside Techniques, harvesting semitendinosus alone serves the purpose. In case the graft is not in adequate length/diameter, Gracilis can also be harvested. Muscle coverings over the graft are then removed using a scale/blade giving attention not to damage the graft. Once muscle tissues are peeled off, the graft is then placed in an antibiotic-loaded normal saline. The two tight ropes (end button) are kept hold on both sides of the graft preparatory station. Then graft is passed through both loops until it is quadrupled. The two free ends are then sutured together. The knot should be on the inside loop. The graft is secured on both ends using vicryl and knots are made to sit inside the graft. Graft length and diameter are measured using a scale and graft size block. A graft with a double or triple-loop configuration can be made measuring about 6.5 cm in length and possessing a minimum diameter of 8 mm (Fig. 1).
Figure 1.
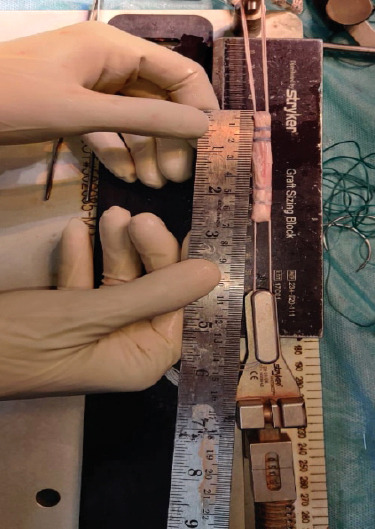
(a) Graft is prepared, and fixed on two sides with adjustable loops length is measured using a scale.
Tranportal ACL reconstruction
Song et al. [14] noticed that the femoral tunnel length is comparatively shorter when contrasted with the transtibial femoral tunnel length.
Due to its potential to construct a femoral tunnel that is more exact in terms of anatomical alignment, the Transportal Technique in ACL repair has been supported as a preferable alternative to the standard transtibial operation [15, 16]. Compared to the transtibial method, the Transportal approach positions the femoral tube with more accuracy, as shown by Song et al. [14] There are issues with the ACL graft and femoral tunnel forming a steep angle during knee extension, as pointed up by Song et al. [14]. A shorter “femoral tunnel length” is a possible downside of the Transportal approach utilized in ACLR, as indicated by many studies [17, 18].
The All-Inside approach was followed for both patient positioning and diagnostic arthroscopy.
Graft harvesting and preparation: A 4 to 5-cm oblique vertical incision was given over just the medial and just below to tibial tuberosity. Using a tendon stripper, STG is isolated and extracted. Muscle coverings over the graft are removed using a scale/blade. The graft is then placed in the graft preparatory station. One end is fixed whip suture using ethibond followed by the other end. Depending on the diameter we opt for, usually 8 mm/9 mm we triple/quadruple the graft. Graft length and diameter were checked using a scale and graft size block. Endobutton is then fixed to the one end of the graft (femoral side) using a tight knot with ethibond. A graft is then passed through the loop; the graft is made with triple/quadruple strands as per the diameter of the tunnel (Fig. 2-5)
Figure 2.
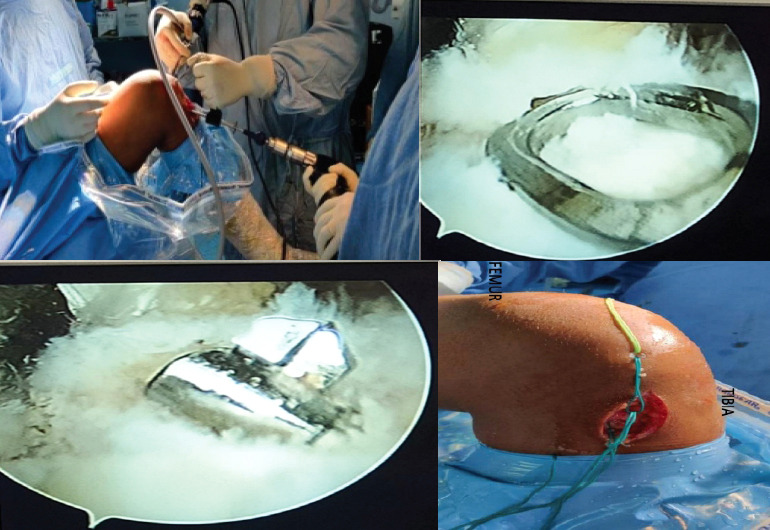
The tibial tunnel is prepared using a tibial zig angled at 55°. Flip cutter is used for the retrograde drilling of the tibial socket. To prevent soft tissue from getting in the way, both the femoral and tibial loops are taken out through anteromedial port.
Figure 3.

(a, b) Graft is being passed through the femoral suture loop and pulled through the femoral socket. (c, d) The endo button goes through the tunnel, and the graft is pulled till the flip occurs at the femoral cortex.
Figure 4.

(a, b, and c) Graft is pulled through the tibial socket, and an adjustable button system is used to seat the graft, (d) Graft is secured with the ABS in the tibial side.
Figure 5.

Preoperative and post-operative X-rays of cases.
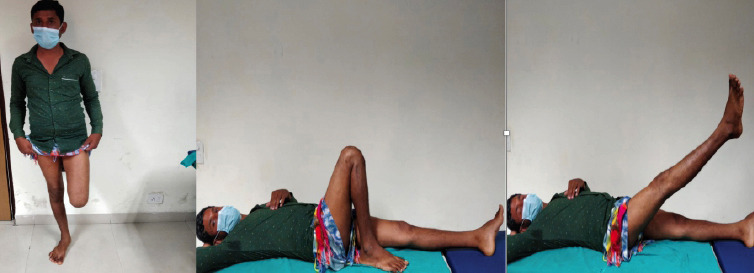
The functional outcomes of each group were assessed using the IKDC scores, a patient-completed instrument comprising two items on sports activities, seven items on knee function, and two items on knee symptoms. The possible score is one hundred, with zero representing the worst symptoms or lowest function, and one hundred representing the highest function. The intensity of the pain was measured using VAS scores, where 0 indicates “no pain” and 10 indicates “pain as severe as it gets.” Patients’ range of motion was quantified through the utilization of a goniometer. The assessments were conducted one, three, and six months after the procedure. (Fig. 6).
Figure 6.
(a, b, and c) Graft is pulled through the tibial socket, and an adjustable button system is used to seat the graft, (d) Graft is secured with the ABS in the tibial side.
Sample size
By calculating the standard deviation, the sample size was determined and (d) minimum difference was detected for the mean of flexion deficit results at follow-up after surgery taken from the previous study [19] where Mean + SD for Conventional (Transportal) Group was 24.16 + 18.45 and All-Inside Group was 13.38 + 11.87.
N = 2*(Zα+Zβ)2×σ 2 /δ 2
Substituting the values in the formula we got a sample size of 30 for 2 groups. Fortunately, a greater number of participants enrolled in the study. A total of 45 patients were included in the study 22 in the AIT group and 23 in the TPT Group.
Data analysis
IBM SPSS Statistics for Windows, version 20, was utilized for the statistical analysis. Following a summary, the data were subsequently presented. In the case of continuous variables, the mean (± SD) was used. Proportions were used to represent categorical variables. To analyze qualitative variables, the unpaired t-test and Mann-Whitney test were utilized. When analyzing qualitative variables, the Chi-square test or Fisher’s exact test was utilized. The criterion for determining significance was P < 0.05.
Results
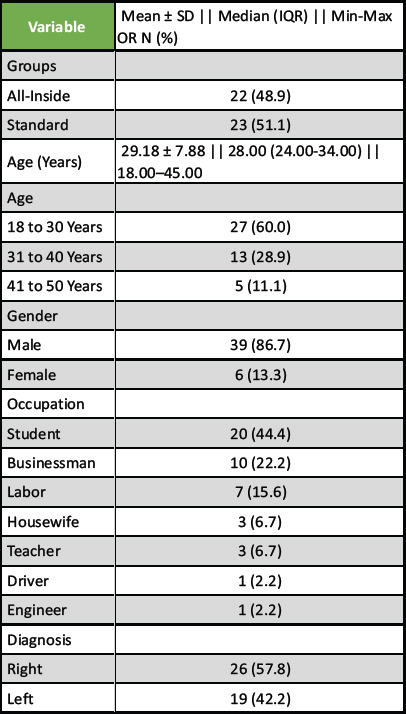
Half of the patients were randomized to “All-Inside” and half to “Standard”. The average age was 29.18, with most participation 18–30. Males (86.7%) and diverse occupations were represented, with students (44.4%) being the largest. The diagnosis was equally even between right (57.8%) and left (42.2) limbs (Table 1).
Table 1.
Demographics of the studies individuals
Both groups showed significant changes in scores over time. The difference was significant in 1st month and 3rd month. In the end, neither group had significantly different score improvements from the other (P = 0.628) (Tables 3-5). There was no statistically significant difference observed in the ages of patients (P = 0.117), median age of participants between the genders (P = 0.414), and distribution of graft sizes (P = 0.235). The Chi-Squared Test reveals a statistically significant discrepancy in the distribution of grafts (P < 0.001) (Table 2).
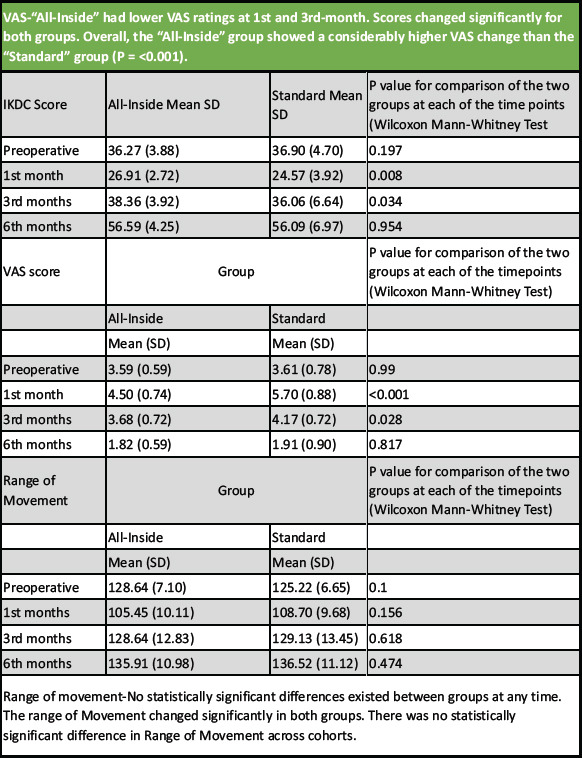
Table 2.
Analysis of the Two Groups’ IKDC Score VAS Score and Range of movement Development, IKDC-Both groups showed significant changes in IKDC score over time. The difference was significant in 1st month and 3rd month. In the end, neither group had significantly different score improvements from the other (P = 0.628). VAS-”All-Inside” had lower VAS ratings at 1st and 3rd-month. Scores changed significantly for both groups. Overall, the “All-Inside” group showed a considerably higher VAS change than the “Standard” group (P = <0.001).
Discussion
ACL injuries are rising among young individuals and non-contact athletes. The ACL wreckage is currently considered a serious ligament injury because of its impact on physical health and financial burden on the active population. The study comprised 45 ACL rupture patients, 22 of whom were randomly assigned to All Inside and 23 to Standard (Transportal). About 65 ACL-torn patients visited the department throughout this investigation. After fulfilling the inclusion and exclusion criteria, 45 were chosen. The bulk of patients (44.4%) were students, indicating that they are the most physically active and prone to injuries. The second largest category in the study was businessmen (22.3%), followed by laborers (15.6%), etc. Half the patients were in the AI group and half in the Standard group. The research is on the entire population, not only athletes, hence most patients were male (86.7% vs. 13.3%). Patients are more likely to be injured in their right limb (57.8%) than their left (42.2%). Sixty percent were 18–30, 29.1% 31–40, and 11.1% 41–50. Higher levels of physical activity among 18–30-year olds are also linked to injury risk. According to Sutton et al., [20] female athletes had three times more ACL injuries than male athletes. Quadriceps angle and tibial slope may contribute. Females have smaller ACL and notch widths, although how this affects injury risk is unclear. The mean age of ACL tear patients was 19 years or younger, similar to Bloom et al. [21].
Bhimani et al. [22] meta-analysis supports IKDC and VAS results. The All-Inside Technique and standard (Transportal) groups improved physical and mental Short Form-12 (SF-12) and IKDC scores similarly post-operatively. The Transportal group had a substantially higher VAS pain level than the All all-within-method group. Even though the VAS score showed a statistically significant difference between groups. Both groups had similar functional results determined by IKDC score, VAS scale, and Range of movement. VAS scores favored All Inside. The investigation indicated no significant Lachmann Grade test difference between groups (P = 1.000). The study found no significant difference in complication between the two groups (P = 1.000). Stiffness and Flip cutter breakage were complications with All-Inside Technique in this study. One stiffness and one infection occurred in the standard technique. Fine and delicate Flip cutter construction is the main factor. ACL restoration often involves broken flip cutters and other tools because of their fragility, incorrect application, and limited knee joint movement. Problem with All Inside method. [23]. The results match Bhimani et al. [22]. Unlike Bhimani et al. and us, Kouloumentas et al. [24]. reported three AIT patients with surgical sequelae such as Cyclops syndrome, septic arthritis, and ACL failure. Singh et al. [23] also pointed out the breakage of flipcutter®, in which they concluded that the flipcutter® has revived the All-Inside ACLR with reliable results but is expensive and delicate. Another major disadvantage of All Inside ACL reconstruction is the learning curve as it is way more complex than other arthroscopic techniques [25]. The study aimed to determine if arthroscopic ACLR employing the All-Inside strategy yields better functional outcomes than the Standard (Transportal) method. The patient’s range of motion, VAS pain, and IKDC subjective functional findings were assessed in this study. After assembling and processing the data, the two approaches yield identical functional results. Our hypothesis is supported by this finding.
Conclusion
The study discovered no statistically significant functional differences between the two methods. There are several benefits of the All-Inside Technique over standard Transportal ACL reconstruction surgery, including the preservation of bone and the gracilis tendon, less post-operative discomfort, and increased knee flexor strength. Even though the early rehabilitation period is in favor of all inside, both techniques are equally the same over a longer period. All Inside has the disadvantage of a higher learning curve and, the costlier method in comparison with standard Transportal Technique.
Clinical Message.
The comparative study on All-Inside (AI) and Transportal (TP) Techniques for ACL reconstruction suggests that both approaches offer similar functional outcomes in terms of knee stability and range of motion. Surgeons can confidently choose either technique based on patient-specific factors, without compromising long-term recovery.
Biography




Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report
References
- 1.John R, Dhillon MS, Syam K, Prabhakar S, Behera P, Singh H. Epidemiological profile of sports-related knee injuries in northern India: An observational study at a tertiary care centre. J Clin Orthop Trauma. 2016;7:207–11. doi: 10.1016/j.jcot.2016.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ahmed S, Ashraf M, Sahanand S, Rajan DV. Can ACL tears be restricted to sports injuries alone?A retrospective analysis. Indian J Orthop. 2021;55:402–8. doi: 10.1007/s43465-021-00387-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brophy RH, Wright RW, Matava MJ. Cost analysis of converting from single-bundle to double-bundle anterior cruciate ligament reconstruction. Am J Sports Med. 2009;37:683–7. doi: 10.1177/0363546508328121. [DOI] [PubMed] [Google Scholar]
- 4.Nagaraj R, Kumar MN. Revision anterior cruciate ligament reconstruction in the nonathlete population. Indian J Orthop. 2019;53:154–9. doi: 10.4103/ortho.IJOrtho_673_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dhinsa BS, Nawaz SZ, Gallagher KR, Skinner J, Briggs T, Bentley G. Outcome of combined autologous chondrocyte implantation and anterior cruciate ligament reconstruction. Indian J Orthop. 2015;49:155–63. doi: 10.4103/0019-5413.152442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lohmander LS, Englund PM, Dahl LL, Roos EM. The longterm consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Am J Sports Med. 2007;35:1756–69. doi: 10.1177/0363546507307396. [DOI] [PubMed] [Google Scholar]
- 7.Joseph C, Pathak SS, Aravinda M, Rajan D. Is ACL reconstruction only for athletes? Int Orthop. 2008;32:57–61. doi: 10.1007/s00264-006-0273-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lohmander LS, Östenberg A, Englund M, Roos H. High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 2004;50:3145–52. doi: 10.1002/art.20589. [DOI] [PubMed] [Google Scholar]
- 9.Meisterling SW, Schoderbek RJ, Andrews JR. Anterior cruciate ligament reconstruction. Oper Tech Sports Med. 2009;17:2–10. [Google Scholar]
- 10.Holm I, Øiestad BE, Risberg MA, Gunderson R, Aune AK. No differences in prevalence of osteoarthritis or function after open versus endoscopic technique for anterior cruciate ligament reconstruction: 12-Year follow-up report of a randomized controlled trial. Am J Sports Med. 2012;40:2492–8. doi: 10.1177/0363546512458766. [DOI] [PubMed] [Google Scholar]
- 11.Lubowitz JH, Amhad CH, Anderson K. All-inside anterior cruciate ligament graft-link technique: Second-generation, noincision anterior cruciate ligament reconstruction. Arthroscopy. 2011;27:717–27. doi: 10.1016/j.arthro.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 12.McCarthy MM, Graziano J, Green DW, Cordasco FA. Allepiphyseal, all-inside anterior cruciate ligament reconstruction technique for skeletally immature patients. Arthrosc Tech. 2012;1:e231–9. doi: 10.1016/j.eats.2012.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Benea H, D'Astorg H, Klouche S, Bauer T, Tomoaia G, Hardy P. Pain evaluation after all-inside anterior cruciate ligament reconstruction and short term functional results of a prospective randomized study. Knee. 2014;21:102–6. doi: 10.1016/j.knee.2013.09.006. [DOI] [PubMed] [Google Scholar]
- 14.Song EK, Kim SK, Lim HA, Seon JK. Comparisons of tunnel-graft angle and tunnel length and position between transtibial and transportal techniques in anterior cruciate ligament reconstruction. Int Orthop. 2014;38:2357–62. doi: 10.1007/s00264-014-2457-0. [DOI] [PubMed] [Google Scholar]
- 15.Giron F, Cuomo P, Edwards A, Bull AM, Amis AA, Aglietti P. Double-bundle “anatomic” anterior cruciate ligament reconstruction: A cadaveric study of tunnel positioning with a transtibial technique. Arthrosc J Arthrosc Relat Surg. 2007;23:7–13. doi: 10.1016/j.arthro.2006.08.008. [DOI] [PubMed] [Google Scholar]
- 16.Kopf S, Forsythe B, Wong AK, Tashman S, Irrgang JJ, Fu FH. Transtibial ACL reconstruction technique fails to position drill tunnels anatomically in vivo 3D CT study. Knee Surg Sport Traumatol Arthrosc. 2012;20:2200–7. doi: 10.1007/s00167-011-1851-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wang JH, Kim JG, Lee DK, Lim HC, Ahn JH. Comparison of femoral graft bending angle and tunnel length between transtibial technique and transportal technique in anterior cruciate ligament reconstruction. Knee Surg Sport Traumatol Arthrosc. 2012;20:1584–93. doi: 10.1007/s00167-011-1781-9. [DOI] [PubMed] [Google Scholar]
- 18.Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ. Transtibial versus anteromedial portal drilling for anterior cruciate ligament reconstruction: A cadaveric study of femoral tunnel length and obliquity. Arthroscopy. 2010;26:342–50. doi: 10.1016/j.arthro.2009.12.006. [DOI] [PubMed] [Google Scholar]
- 19.Sahu DSK, Ganesh DA. All-inside technique versus conventional Transportal anterior cruciate ligament reconstruction: A retrospective study. Int J Orthop Sci. 2020;6:39–44. [Google Scholar]
- 20.Sutton KM, Bullock JM. Anterior cruciate ligament rupture: Differences between males and females. J Am Acad Orthop Surg. 2013;21:41–50. doi: 10.5435/JAAOS-21-01-41. [DOI] [PubMed] [Google Scholar]
- 21.Bloom DA, Wolfert AJ, Michalowitz A, Jazrawi LM, Carter CW. ACL injuries aren't just for girls: The role of age in predicting pediatric ACL injury. Sports Health. 2020;12:559–63. doi: 10.1177/1941738120935429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bhimani R, Shahriarirad R, Ranjbar K, Erfani A, Ashkani-Esfahani S. Transportal versus all-inside techniques of anterior cruciate ligament reconstruction: A systematic review. J Orthop Surg Res. 2021;16:734. doi: 10.1186/s13018-021-02872-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Singh K, Dutt S, Sabat D, Sehrawat R, Kumar V, Singh P. Flipcutter®breakage during All-inside ACL reconstruction: Possible technical errors and tips to avoid misadventure. J Arthrosc Joint Surg. 2021;8 10.1016/j.jajs.2021.01.001. [Google Scholar]
- 24.Kouloumentas P, Kavroudakis E, Charalampidis E, Kavroudakis D, Triantafyllopoulos GK. Superior knee flexor strength at 2 years with all-inside short-graft anterior cruciate ligament reconstruction vs a conventional hamstring technique. Knee Surg Sport Traumatol Arthrosc. 2019;27:3592–8. doi: 10.1007/s00167-019-05456-9. [DOI] [PubMed] [Google Scholar]
- 25.Noronha JC, Oliveira JP. Inside-out tibial tunnel drilling technique for all-inside anterior cruciate ligament reconstruction. Arthrosc Tech. 2018;7:e373–7. doi: 10.1016/j.eats.2017.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]