

Abstract
Background:
Allied healthcare professionals face the intricate challenge of preventing burnout, which is marked by emotional exhaustion, depersonalisation and diminished personal accomplishment. Physical activity is proposed as a mitigating strategy that promises to reduce and effectively address burnout among allied healthcare professional.
Aim:
The study aimed to determine the correlation between personal accomplishment and burnout among allied healthcare professionals.
Methods:
A quantitative, non-experimental, cross-sectional, correlational design following the TREND statement amongst 82 allied healthcare professionals was conducted using the Maslach Burnout Inventory and the Global Physical Activity Questionnaire. Burnout was assessed using its three diagnostic characteristics: emotional exhaustion, depersonalisation and personal accomplishment.
Results:
Participants (45.1%) experienced a low degree of emotional exhaustion, but overall, for the entire group emotional exhaustion was moderate (M = 20.51; standard deviation = 10.5), similar to depersonalisation (M = 6.46; standard deviation ±4.90), with 46.3% of the participants experiencing a low degree of depersonalisation. In the personal accomplishment category, 22% experienced a low degree of personal accomplishment; overall, for the entire group, personal accomplishment was low (M = 33.35; standard deviation = 7.58). Most participants (65.9%) engaged in moderate-intensity physical activities. The number of days performing moderate-intensity physical activity at work significantly increases the odds of allied healthcare professional experiencing low levels of emotional exhaustion, depersonalisation and personal accomplishment by 1.92, 2.33 and 2.09, respectively (p < 0.05).
Conclusions:
Engaging in moderate-intensity physical activities increases the likelihood of allied healthcare professionals experiencing low emotional exhaustion, depersonalisation and personal accomplishment degrees. It underscores the importance of implementing physical activity programmes to improve healthcare and alleviate the effect of burnout in allied healthcare professional.
Keywords: Depersonalisation, emotional exhaustion, exercise, personal accomplishment, psychosocial health, service profession
Introduction
An allied healthcare professional (AHP)’s role is to provide services to others, necessitating substantial personal commitment. The equilibrium between occupational demands and personal replenishment is inherently precarious. Researchers define burnout as an employee’s work-related state characterised by extreme tiredness, reduced emotional regulation and cognitive processing, and mental distancing. 1 It is an occupation-related psychological syndrome consisting of emotional, physical and cognitive exhaustion. 2 Consequently, the emotional, mental, and physical well-being of their patients and themselves is an escalating concern among AHPs. 3
Italian researchers stated that the burnout phenomenon has been extensively investigated among healthcare professionals, mainly focusing on physicians and nurses. However, the literature concerning burnout in clinical research is poor and often neglects the other professional categories involved. 4 In South Africa, the available literature on the prevalence and degree of burnout among AHPs is limited. However, a study by Du Plessis et al. among therapists in private practice revealed that 57.14% experienced a high degree of emotional exhaustion (EE), 20.40% scored high on the depersonalisation (DP) scale, and 38.77% reported a low degree of personal accomplishment (PA) (p < 0.05). 5 The study concluded that these findings are consistent with international trends, indicating that South African therapists may be at a heightened risk for developing burnout. In the absence of recent literature, it is challenging to address burnout among AHPs. Hence, in the absence of current literature, initiating and implementing effective intervention programmes to prevent further negative consequences and improve AHPs’ quality of service, job satisfaction and quality of life is challenging.
Physical activity is an underutilised and low-cost intervention that can affect health on several platforms. 6 Researchers state that physical activity is considered one of the most relevant strategies for promoting biopsychosocial health. 7 Physical activity may enhance social resources, provide social support, and strengthen social networks and relationships, aiding in burnout prevention. 8 This is particularly beneficial for AHPs, who often work in multidisciplinary environments. Healthy social relationships can lead to improved clinical care. Building social networks outside work can help individuals feel more supported in managing occupational stress. As Kandola et al. noted physical activity is associated with mastery experiences and a sense of personal control, leading to increased self-efficacy. This can directly mitigate burnout, as depersonalisation is a diagnostic factor, and improved self-efficacy can help prevent the onset or progression of burnout. 9
A longitudinal study, both cross-sectionally and prospectively conducted by De Vries and Bakker showed that off-job physical activity was negatively related to primary and secondary burnout symptoms and that physical activity may act as a self-regulation strategy corroborated by other researchers.10–12 A recent systematic review found that physical activity is often associated with a reduced risk of burnout, particularly in emotional exhaustion and depersonalisation domains. 13 In the absence of literature in the South African context showing if physical activity can mitigate the degree of burnout in AHPs, this study aims to determine the correlation between physical activity and burnout among AHPs.
Methods
Research design and setting
The study employed a quantitative approach with a non-experimental, descriptive, cross-sectional, correlational design conducted amongst AHPs in private practice in the eThekwini Metropolitan Municipality, KwaZulu-Natal province, South Africa. KwaZulu-Natal has the second largest population in South Africa. 14 It is divided into a single metropolitan municipality (eThekwini Metropolitan Municipality) and 10 district municipalities subdivided into 43 local municipalities. 15
The Transparent Reporting of Evaluations with Non-randomized Designs (TREND) checklist for reporting standards of behavioural and public health intervention evaluations involving non-randomised designs were adhered to. 16 Adhering to the TREND checklist improves the credibility and replicability of our findings by ensuring that critical details about the study, such as participant selection, intervention procedures, outcome measures and statistical analysis, are reported consistently as reflected in our methods section.
Sampling
South Africa’s healthcare infrastructure is divided into the public and private sectors. Statistics South Africa’s Quarterly Employment Survey reported that from July to September 2020, 360,274 people, including various healthcare professionals, were employed in the private health and social work sector. 15 As of 27 November 2022, the Health Professionals Council of South Africa (HPCSA) listed 3160 active practitioners in KwaZulu-Natal, comprising 331 audiologists, 221 biokineticists (clinical exercise physiologists), 805 occupational therapists, 1317 physiotherapists, 358 speech therapists, and 128 speech therapists and audiologists. 17 Two hundred eighty-three practitioners were sampled using the Raosoft calculator to achieve a margin of error under 5% and a 95% confidence level. 18 They were recruited from private practice in the eThekwini Metropolitan Municipality using online ads, social media posts, word of mouth, and emails from professional bodies applying the inclusion criteria of being registered with the HPCSA and their respective internal governing bodies, employed full-time, actively engaged in patient care within private practice in the eThekwini Municipality, aged 21–65, and from all sociodemographic groups in South Africa. Participants were excluded if they were healthcare students, interns, community service students, locum or part-time practitioners, public or non-private sector AHPs, and those not using physical rehabilitation interventions as a treatment modality. Interested and eligible participants received a link to an informed consent form for signing and the online survey.
Data collection tools
Participants’ presence and severity of burnout were measured via Google Forms using the Maslach Burnout Inventory (MBI) and physical activity using the Global Physical Activity Questionnaire (GPAQ). An online questionnaire was chosen for safety reasons and non-contact facilitation due to COVID-19 safety protocols. The GPAQ is a valid and reliable for measuring moderate-to-vigorous physical activity (MVPA) or changes in MVPA, 19 respectively, similar to the MBI for assessing burnout across several occupations and healthcare professionals. 20 The MBI consists of 22 items on a Likert-type scale. 21 The responses to the 22 questions correspond to 3 subsections (emotional exhaustion, depersonalisation and diminished personal accomplishment) in establishing burnout, with scoring done on a scaling system between low, medium and high. 22 The scoring of the three subsections is as follows for emotional exhaustion ⩽17 (low degree), 18–29 (moderate degree), and ⩾30 (high degree); depersonalisation ⩽5 (low degree), 6–11 (moderate degree), and ⩾12 (high degree); personal accomplishment ⩽33 (low degree), 34–39 (moderate degree), and ⩾40 (high degree). The GPAQ subjectively collects information on physical activity participation across three domains and includes reporting sedentary behaviour. 23 It comprises 16 questions across 3 domains (activity at work, travel to and from places, and recreational activities). Both questionnaires are available as supplemental material.
Data analysis
The data were analysed using the Statistical Package for Social Sciences (SPSS®) software, version 28 (SPSS Inc., Chicago, IL, USA). 24 The Shapiro–Wilks test was used to test the distribution of the data, which were shown to be normally distributed. Continuous variables were summarised as the means, standard deviations (SD) and percentages. Univariable logistic regressions were performed to describe the relationship between physical activity and measures of burnout. A p-value of <0.05 indicated statistical significance.
Ethics statement
The Universities’ Humanities and Social Sciences Research Ethics Committee approved the study (HSSREC/00004122/2022). All procedures in this study involving human participants followed the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Results
Demographic profile
Eighty-two AHPs completed the online survey. Among the analysed participants, biokineticists (clinical exercise physiologists) represented 63.4% (n = 52), physiotherapists constituted 24.4% (n = 20) and a small fraction of occupational therapists, audiologists and speech therapists collectively accounted for 11% (n = 10). Additionally, 1.2% of the data was classified as missing or incomplete during system analysis. Regarding experience, 22% of participants had less than 1 year (n = 18), 28% had 2–4 years (n = 23), 37.8% had 5 years or more (n = 31), and 12.2% did not specify their experience level (n = 10).
Burnout among allied healthcare professionals
As shown in Figure 1, 45.1%, 46.3% and 22.0% of the participants experienced low EE, DP and PA degrees, respectively. However, further analysis showed that the overall degree of experiencing EE for the entire group is moderate (M = 20.51; SD ± 10.5), with an MBI score of 18–29 for EE classified as moderate. Depersonalisation was similarly moderate (M = 6.46; SD ± 4.90), with an MBI score of 6–11 for DP classified as moderate. Finally, their overall degree of experiencing PA is low (M = 33.35; SD ± 7.58), with an MBI score of ⩽33 categorised as low.
Figure 1.
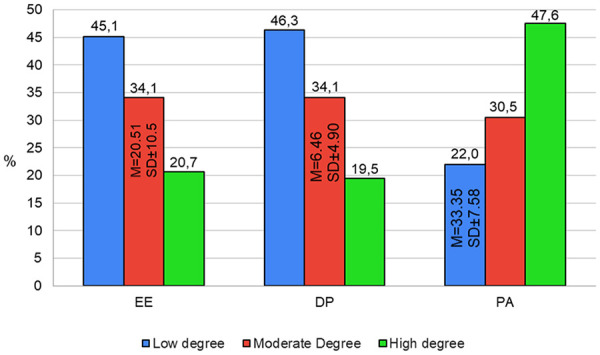
Participant’s degree of burnout.
EE: emotional exhaustion; DP: depersonalisation; PA: personal accomplishment; M: mean; SD: standard deviation; %: percentage.
Physical activity levels of allied healthcare professionals
Table 1 shows a significant 80.5% (p < 0.001) of the AHPs indicated that they do not engage in vigorous-intensity and 65.9% (p = 0.005) in moderate-intensity activities at work that cause large increases in breathing or heart rate, like carrying or lifting heavy loads or running hard for at least 10 min continuously. A significant 87.8% indicated that they do not continuously walk or cycle from place to place for more than 10 min (p < 0.001). A significant portion of participants reported participating in vigorous-intensity (68.3%; p = 0.001) and moderate-intensity (73.2%; p < 0.001) sports, fitness or recreational activities that cause a small increase in breathing or heart rate, such as swimming or cycling for at least 10 min continuously.
Table 1.
AHPs physical activities domestically, work, for sports, fitness or recreational (leisure) purposes.
| Physical activities | Yes/no | n | % | p-Value |
|---|---|---|---|---|
| Do your activities at work involve vigorous-intensity activity that causes large increases in breathing or heart rate, like carrying heavy loads, running hard, lifting heavy loads or digging for at least 10 min continuously? | Yes | 16 | 19.5 | 0.001 |
| No | 66 | 80.5 | ||
| Do your activities at work involve moderate-intensity activity that causes small breathing or heart rate increases, such as brisk walking or carrying light loads for at least 10 min continuously? | Yes | 54 | 65.9 | 0.005 |
| No | 28 | 34.1 | ||
| Do you continuously walk or use a bicycle (pedal cycle) for at least 10 min to get to and from places? | Yes | 10 | 12.2 | 0.001 |
| No | 72 | 87.8 | ||
| Do you do any vigorous-intensity sports, fitness or recreational (leisure) activities that cause large increases in breathing or heart rate, like running or football, for at least 10 min continuously? | Yes | 56 | 68.3 | 0.001 |
| No | 26 | 31.7 | ||
| Do you do any moderate-intensity sports, fitness or recreational (leisure) activities that cause a small increase in breathing or heart rate, such as brisk walking, cycling, swimming and volleyball) for at least 10 min continuously? | Yes | 60 | 73.2 | 0.001 |
| No | 22 | 26.8 |
AHP: allied healthcare professional.
Further analysis showed that a larger portion of participants engage in vigorous- and moderate-intensity recreational activities, sports and fitness, respectively (n = 56/68.3%, n = 60/73.2%), compared to engaging in their daily occupational and domestic vigorous- and moderate-intensity physical activities, respectively (n = 16/19.5%, n = 54/65.9%).
Table 2 gives us insight into the amount of time, measured in days and minutes, invested in different types of physical activities and the physical activity habits of AHPs. During a typical week, the participants engaged in vigorous-intensity activities at work, with an average of 4.28 days a week (M = 4.28, SD ± 1.57). They did this for a minimum of 5 and 600 min, with an average of 190.63 min daily (M = 190.63, SD ± 197.37). In an average week, they participated in moderate-intensity activities at work with an average of 4.64 days a week (M = 4.64, SD ± 1.45); they did this for a minimum of 15 min and a maximum of 600 min a day with an average of 173.27 min a day (M = 173.27, SD ± 149.90).
Table 2.
Amount of days and minutes a week spent on physical activities and sedentary behaviour (N = 82).
| Time spent engaging in physical activities (days) | Min/max | Mean/SD |
|---|---|---|
| In a typical week at work, how many days do you do vigorous-intensity activities as part of your activities? | 1/7 | 4.28/1.57 |
| In a typical week at work, how many days do you do moderate-intensity activities as part of your activities? | 1/7 | 4.64/1.45 |
| In a typical week, how many days do you continuously walk or bicycle for at least 10 min to get to and from places? | 1/7 | 3.40/1.99 |
| In a typical week, how many days do you do vigorous-intensity sports, fitness or recreational (leisure) activities? | 1/7 | 3.89/1.66 |
| In a typical week, how many days do you do moderate-intensity sports, fitness or recreational (leisure) activities? | 1/7 | 3.23/1.70 |
| Time spent engaging in physical activities and sedentary behaviour (min) | ||
| How much time do you spend doing vigorous-intensity activities at work on a typical day | 5/600 | 190.63/197.37 |
| How much time do you spend doing moderate-intensity activities at work on a typical day? | 15/600 | 173.27/149.90 |
| How much time do you spend walking or bicycling for travel on a typical day? | 0/300 | 70.77/106.51 |
| How much time do you spend doing vigorous-intensity sports, fitness or recreational activities on a typical day? | 30/360 | 82.41/56.78 |
| How much time do you spend doing moderate-intensity sports, fitness or recreational (leisure) activities on a typical day? | 0/180 | 62.74/36.05 |
| How much time do you usually spend sitting or reclining on a typical day? | 30/960 | 281.52/213.42 |
Min: minimum; Max: maximum; SD: standard deviation.
Throughout a typical week, the participants walked or cycled continuously for at least 10 min to get to and from places, with an average of 3.40 days a week (M = 3.40, SD ± 1.99). They did this for a minimum of 0 min and a maximum of 300 min a day, with an average of 70.77 min a day (M = 70.77, SD ± 106.51) (Table 2).
Over an ordinary week, the participants engaged in vigorous-intensity sports, fitness or recreational activities, with an average of 3.89 days a week (M = 3.89, SD ± 1.66). They did this for a minimum of 30 min and a maximum of 360 min, for an average of 82.41 min daily (M = 82.41, SD ± 56.78). Similarly, they participated in moderate-intensity sports, fitness and recreational activities in a typical week, with an average of 3.23 days a week (M = 3.23, SD ± 1.70). They did this type of activity for a minimum of 0 min and a maximum of 180 min daily, for an average of 62.74 min a day (M = 62.74, SD ± 36.05).
Lastly, it was found that on a typical day, participants spent a minimum of 30 min and a maximum of 960 min a day sitting or reclining sedentary behaviour. They did this for an average of 281.52 min daily (M = 281.52, SD ± 213.42).
Relationship between physical activity and burnout among allied healthcare professionals
Table 3 illustrates that the number of days performing moderate-intensity physical activity at work is significantly related to an increase in odds of 1.92, 2.33 and 2.09 of AHPs experiencing a low degree of EE, DP and PA (p < 0.05). Similarly, the number of days performing moderate-intensity physical activities work is significantly related with an increase in odds of 2.09 of AHPs experiencing a moderate degree of DP (p < 0.05).
Table 3.
Relationship between physical activity (number of days/week) and burnout among AHPs.
| Physical activity | Burnout degree | Emotional exhaustion | Depersonalisation | Personal accomplishment | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | SE | p-Value | OR (95% CI) | SE | p-Value | OR (95% CI) | SE | p-Value | ||
| Vigorous-intensity activity at work | Low degree | 1 (0.51, 1.97) | 0.35 | 1.000 | 1.48 (0.61, 3.64) | 0.46 | 0.388 | 2.53 (0.49, 2.99) | 0.84 | 0.267 |
| Moderate degree | 1.35 (0.54, 3.36) | 0.47 | 0.521 | 1.06 (0.53, 2.13) | 0.36 | 0.869 | 0.91 (0.47, 1.75) | 0.34 | 0.770 | |
| Moderate-intensity activity at work | Low degree | 1.92 (1.03, 3.57) | 0.32 | 0.040* | 2.33 (1.26, 4.31) | 0.32 | 0.007* | 2.09 (1.08, 4.07) | 0.34 | 0.029* |
| Moderate degree | 0.84 (0.51, 1.37) | 0.25 | 0.478 | 1.82 (1.03, 3.22) | 0.29 | 0.040* | 0.88 (0.57, 1.35) | 0.22 | 0.552 | |
| Walking/cycling to and from places | Low degree | 1 (0.43, 2.34) | 0.43 | 1.000 | 1.53 (0.56, 4.16) | 0.51 | 0.407 | 2.26 (0.51, 0.06) | 0.76 | 0.286 |
| Moderate degree | 1.27 (0.70, 2.29) | 0.30 | 0.423 | 1.77 (0.65, 4.84) | 0.51 | 0.264 | 1.54 (0.82, 2.87) | 0.32 | 0.177 | |
| Vigorous-intensity sports, recreational activity | Low degree | 1 (0.62, 1.60) | 0.24 | 0.98 | 0.69 (0.39, 1.23) | 0.29 | 0.203 | 0.94 (0.63, 1.41) | 0.21 | 0.759 |
| Moderate degree | 1.03 (0.63, 1.69) | 0.25 | 0.91 | 0.90 (0.50, 1.63) | 0.30 | 0.732 | 0.98 (0.68, 1.41) | 0.19 | 0.910 | |
| Moderate-intensity sports, recreational activity | Low degree | 0.73 (0.46, 1.15) | 0.23 | 0.18 | 0.63 (0.39, 1.01) | 0.24 | 0.057 | 1.12 (0.76, 1.65) | 0.20 | 0.581 |
| Moderate degree | 1 (0.99, 1.01) | 0.00 | 0.75 | 1.01 (0.99, 1.02) | 0.00 | 0.067 | 1 (0.99, 1.01) | 0.00 | 0.185 | |
OR: odds ratio; CI: confidence interval; SE: standard error; AHP: allied healthcare professional.
p < 0.05.
Table 4 shows that the number of minutes per day performing moderate-intensity sports, fitness or recreational activities is significantly related to an increase in odds of 1.02 of AHPs experiencing a low degree of PA (p < 0.05). The number of minutes per day being sedentary is significantly not related with an odds of 1.0 of AHPs experiencing a low degree of EE (p < 0.05) and odds of 1.0 for experiencing a moderate degree of EE (p < 0.01).
Table 4.
Relationship between physical activity (minutes per day) and burnout among AHPs.
| Physical activity | Burnout degree | Emotional exhaustion | Depersonalisation | Personal accomplishment | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | SE | p-Value | OR (95% CI) | SE | p-Value | OR (95% CI) | SE | p-Value | ||
| Vigorous-intensity activity at home | Low degree | 1 (0.99, 1.01) | 0.00 | 0.989 | 1 (0.99, 1.01) | 0.00 | 0.570 | 1.01 (0.99, 1.02) | 0.01 | 0.091 |
| Moderate degree | 1 (0.99, 1.01) | 0.00 | 0.935 | 1.01 (0.99, 1.02) | 0.01 | 0.219 | 1.01 (1.0, 1.02) | 0.01 | 0.094 | |
| Moderate-intensity activity at home | Low degree | 1 (0.99, 1.01) | 0.00 | 0.177 | 1.01 (0.99, 1.02) | 0.00 | 0.086 | 1 (0.99, 1.01) | 0.00 | 0.152 |
| Moderate degree | 1 (0.99, 1.01) | 0.00 | 0.745 | 1.01 (0.99, 1.02) | 0.00 | 0.067 | 1 (0.99, 1.01) | 0.00 | 0.185 | |
| Walking/cycling to and from places | Low degree | 0.99 (0.98, 1.01) | 0.01 | 0.411 | 1.08 (0.99, 1.31) | 0.10 | 0.410 | 1.02 (0.98, 1.06) | 0.02 | 0.354 |
| Moderate degree | 0.97 (0.94, 1.02) | 0.02 | 0.216 | 1.09 (0.90, 1.31) | 0.10 | 0.374 | 1.02 (0.98, 1.06) | 0.02 | 0.356 | |
| Vigorous-intensity sports, recreational activity | Low degree | 1.02 (0.10, 1.05) | 0.02 | 0.199 | 1 (0.99, 1.02) | 0.01 | 0.844 | 1 (0.99, 1.01) | 0.01 | 0.628 |
| Moderate degree | 1.01 (0.98, 1.05) | 0.02 | 0.366 | 1 (0.98, 1.02) | 0.01 | 0.967 | 0.99 (0.98, 1.01) | 0.01 | 0.256 | |
| Moderate-intensity sports, recreational activity | Low degree | 1.02 (0.99, 1.04) | 0.01 | 0.182 | 1 (0.98, 1.02) | 0.01 | 0.882 | 1.02 (1.00, 1.04) | 0.01 | 0.025* |
| Moderate degree | 1.01 (0.98, 1.04) | 0.01 | 0.459 | 0.97 (0.95, 1.00) | 0.01 | 0.057 | 0.99 (0.98, 1.01) | 0.01 | 0.417 | |
| Sedentary behaviour | Low degree | 1 (0.99, 1.00) | 0.00 | 0.011* | 1 (0.99, 1.00) | 0.00 | 0.869 | 1 (0.99, 1.00) | 0.00 | 0.181 |
| Moderate degree | 1 (0.99, 1.00) | 0.00 | 0.003** | 1 (0.99, 1.00) | 0.00 | 0.767 | 1 (0.99, 1.00) | 0.00 | 0.475 | |
OR: odds ratio; CI: confidence interval; SE: standard error; AHP: allied healthcare professional.
p < 0.05; **p < 0.01.
Discussion
In a cross-sectional correlational study among AHPs in eThekwini, South Africa, the most important finding was that the number of days AHPs participated in moderate-intensity physical activities at work enhanced their probability of encountering reduced degrees of EE, DP and PA. We further found that the number of minutes per day performing moderate-intensity sports, fitness or recreational activities is significantly related to increased odds of AHPs experiencing a low degree of PA. Our results are consistent with other researchers’ findings. 25 Although the participants in the Greco study followed an 8-week moderate to vigorous intensity combined exercise training intervention, there was a significant reduction in EE and DP and increased PA. Ochentel et al. concluded in their meta-analysis of four randomised control trials (RCTs) that exercise significantly decreased burnout, specifically the EE component of burnout. 12 Our findings are significant given that EE is one of the primary and most common characteristics of burnout across its various conceptualisations. This study demonstrated that physical activity might alleviate or control burnout by reducing the degree of EE experienced by an individual. By mitigating EE, we equip AHPs with an enhanced ability to care for themselves, as their role necessitates emotional investment. The capacity to manage this investment safeguards the health of both the clinician and the patient. Conversely to being physically active, a not surprising finding is that our results showed that sedentary time does not impact the likelihood of experiencing low or moderate EE among AHPs. It underscores again the importance of AHPs engaging in physical activity as a protective measure against burnout.
Our results showed that the overall degree of AHPs experiencing EE is moderate, similar to depersonalisation, contrasting the findings of Du Plessis et al. who reported that rehabilitation staff in South Africa scored high on EE and DP. 5 However, other researchers corroborate our findings for EE and DP by reporting a moderate degree of burnout amongst Spanish physiotherapists across the three dimensions of burnout on the MBI. 26 For PA, the same study by González-Sánchez et al. 26 contrast the findings of our study with the AHPs experiencing an overall low degree but supported by Du Plessis et al. who reported that rehabilitation participants similarly experienced a low degree of personal PA. It is essential to note that for a diagnosis of burnout, participants must exhibit high levels of EE and DP, along with low levels of personal PA. 5 Based on these diagnostic criteria, it can be inferred that the AHPs are on the threshold of experiencing burnout.
The results showed AHPs had a moderate physical activity level, with the majority, 65.9%, engaging in moderate-intensity activities at work, spending 4.64 days a week and 173.27 min daily on this activity. The AHPs physical activity levels were assessed using the GPAQ, whereas Marques-Sule et al. assessed physical activity levels using the European Health Interview Survey-Physical Activity, making comparisons difficult. 27 Nonetheless, Marques-Sule et al. established that 65.9% of the AHPs in their study engaged in moderate-intensity at work. 27 Like the current study, researchers assessed healthcare worker’s physical activity levels using the GPAQ. 28 Although the intensity of the healthcare worker’s physical activities was not specified, the findings are almost similar to those established in the current study, as 54.4% of healthcare workers were classified as physically active. The physical activity levels of AHP must be interpreted in light of the nature of their occupations, which typically involve a combination of standing, walking, lifting, exercise demonstration, manual therapy treatments and sitting.
The data must be elucidated, considering that the data were collected 3 months after all the National State of Disaster COVID-19 lockdown regulations had been lifted in South Africa, and patients could freely move around. In the same breath, it was a stage when AHPs practices were not yet busy, as they were slowly picking up and rebuilding their practices. This notion is supported by De Hert, who states that burnout develops over phases; therefore, an individual’s presentation of symptoms and risk factors may change over time as the stimulus or environment changes. 3
The study’s findings have to be interpreted against some limitations experienced: First, the study’s validity was potentially undermined by a decreased sample size due to a lower participant response rate, which is common in online surveys. Second, despite its convenience, the online data collection method offers limited mechanisms to ensure participants fully complete the questionnaire and provide accurate responses. Third, the sample was predominantly comprised of biokinetics and physiotherapy professionals, potentially affecting result generalisation. Finally, studies that utilised self-reported burnout surveys among AHPs in a South African context are almost non-existent, making it difficult to draw comparisons to the cultural and socioeconomic factors at play.
Conclusions
The study’s findings indicate that the frequency of days AHPs engaged in moderate-intensity physical activities at work increased their likelihood of experiencing lower degrees of EE, DP and enhanced PA, underscoring the invaluable impact physical activity has by mitigating AHPs burnout and overall benefitting their biopsychosocial health. The AHPs overall degree of experiencing EE and DP was moderate, and their overall degree of experiencing PA is low, indicating that they are on the cusp of experiencing burnout.
In South Africa, the National Priorities Framework in Research ranks mental health fourth under the disease burden, unfortunately, with a notable lack of attention and resources directed toward conditions like burnout. As the current study looked at burnout as a condition and its relation to physical activity, both under-researched areas, the study addressed a vast gap in the literature among AHPs and other service personnel in the eThekwini Metropolitan Municipality and South Africa, calling for the conception and implementation of combative strategies, and guide evidence-based exercise interventions for managing burnout and improving AHPs job satisfaction and health-related quality of life.
Supplemental Material
Supplemental material, sj-docx-1-smo-10.1177_20503121241297060 for Correlation between physical activity and burnout amongst allied healthcare professionals in eThekwini, South Africa by Jeanne Martin Grace and Léchay Moodley in SAGE Open Medicine
Acknowledgments
None.
Footnotes
Author contributions: JMG and LM, contributed to the conception and design of the study. LM collected the data. All the authors contributed to the interpretation of the results. JMG drafted the first version of the manuscript. All the authors critically revised the manuscript for relevant intellectual content. All the authors made a significant contribution to the research and the development of the manuscript and approved the final version for publication. No form of payment was given to anyone to produce the manuscript.
Data availability statement: Data are available upon request, subject to limitations associated with confidentiality.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement: Ethical approval for this study was obtained from the Universities’ Humanities and Social Sciences Research Ethics Committee (Approval No. HSSREC/00004122/2022). All procedures in this study involving human participants followed the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent: Written informed consent was obtained from all subjects before the study.
Permission to reproduce material from other sources: Note applicable.
Trial registration: Not applicable.
Clinical trial registration: Not applicable.
ORCID iD: Jeanne Martin Grace  https://orcid.org/0000-0001-6848-6500
https://orcid.org/0000-0001-6848-6500
Supplemental material: Supplemental material for this article is available online.
References
- 1. Schaufeli WB, Desart S, De Witte H. Burnout assessment tool (BAT)—development, validity, and reliability. Int J Environ Res Public Health 2020; 17(24): 9495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians: a systematic review. JAMA 2018; 320(11): 1131–1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. De Hert S. Burnout in healthcare workers: prevalence, impact and preventative strategies. Local Reg Anesth 2020; 13: 171–183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Cagnazzo C, Filippi R, Zucchetti G, et al. Clinical research and burnout syndrome in Italy – only a physicians’ affair? Trials 2021; 22: 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Du Plessis T, Visagie S, Mji G. The prevalence of burnout amongst therapists working in private physical rehabilitation centers in South Africa: a descriptive study. S Afr J Occup Ther 2014; 44(2): 11–15. [Google Scholar]
- 6. Ridgers ND, Timperio A, Brown H, et al. A cluster-randomised controlled trial to promote physical activity in adolescents: the Raising Awareness of Physical Activity (RAW-PA) study. BMC Public Health 2017; 17: 6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Thiel A, Sudeck G, Gropper H, et al. The iReAct study – a biopsychosocial analysis of the individual response to physical activity. Contemp Clin Trials Commun 2020; 17: 100508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Rueger SY, Malecki CK, Pyun Y, et al. A meta-analytic review of the association between perceived social support and depression in childhood and adolescence. Psychol Bull 2016; 142(10): 1017–1067. [DOI] [PubMed] [Google Scholar]
- 9. Kandola A, Ashdown-Franks G, Hendrikse J, et al. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev 2019; 107: 525–539. [DOI] [PubMed] [Google Scholar]
- 10. De Vries JD, Bakker AB. The physical activity paradox: a longitudinal study of the implications for burnout. Int Arch Occup Environ Health 2022; 95(5): 965–979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Naczenski LM, De Vries JD, Van Hooff ML, et al. Systematic review of the association between physical activity and burnout. J Occup Health 2017; 59(6): 477–494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ochentel O, Humphrey C, Pfeifer K. Efficacy of exercise therapy in persons with burnout: a systematic review and meta-analysis. J Sports Sci Med 2018; 17(3): 475–484. [PMC free article] [PubMed] [Google Scholar]
- 13. Mincarone P, Bodini A, Tumolo MR, et al. Association between physical activity and the risk of burnout in health care workers: systematic review. JMIR Pub Health Surveill 2024; 18(3): e49772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Statistics South Africa (Stats SA). Statistics South Africa Annual Report 2022/2023 (Book 1). Stats SA, https://www.statssa.gov.za/publications/AnnualReport/StatisticsSouthAfricaAnnualReport202223_Book1.pdf (2023, accessed 10 March 2023).
- 15. National Department of Health. Statistics South Africa’s Quarterly Employment Survey. National Department of Health, https://www.health.gov.za/ (2019, accessed 10 July 2022).
- 16. Des Jarlais DC. TREND (Transparent Reporting of Evaluations with Nonrandomized Designs). In: Moher D, Altman DG, Schulz KF, et al. (eds.) Guidelines for Reporting Health Research: A User’s Manual. Wiley Online Library, 2014. [Google Scholar]
- 17. Health Professions Council of South Africa (HPCSA). Health Professions Council of South Africa. Statistics. Health Professions Council of South Africa, https://hpcsa.co.za/?contentId=412&actionName=Publications (2022, accessed 27 November 2022).
- 18. Raosoft Inc. Raosoft sample size calculator. Raosoft Inc., http://www.raosoft.com/samplesize.html (2022, accessed 22 August 2022). [Google Scholar]
- 19. Cleland CL, Hunter RF, Kee F, et al. Validity of the Global Physical Activity Questionnaire (GPAQ) in assessing the levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health 2014; 14: 1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Ogunsuji O, Ogundipe H, Adebayo O, et al. Internal reliability and validity of Copenhagen burnout inventory and Oldenburg burnout inventory compared with Maslach burnout inventory among Nigerian resident doctors: a pilot study. Dubai Med J 2022; 5(2): 1–7. [Google Scholar]
- 21. Robinson J. Encyclopedia of Quality of Life and Well-Being Research. Dordrecht: Springer, 2014. [Google Scholar]
- 22. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory: third edition. In:Zalaquett CP, Wood RJ. (eds.) Evaluating Stress: A Book of Resources. 3rd ed. New York: The Scarecrow Press, 1997. pp.191-218. [Google Scholar]
- 23. Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): nine country reliability and validity study. J Phys Act Health 2009; 6(6): 790–804. [DOI] [PubMed] [Google Scholar]
- 24. IBM Corp. IBM SPSS Statistics for Windows (Version 27.0) [Computer software]. Armonk, NY: IBM Corp., 2021. [Google Scholar]
- 25. Greco G. Effects of combined exercise training on work-related burnout symptoms and psychological stress in helping professionals. J Hum Sport Exerc 2021; 16(2): 424–434. [Google Scholar]
- 26. González-Sánchez B, López-Arza MV, Montanero-Fernández J, et al. Burnout syndrome prevalence in physiotherapists. Rev Assoc Med Bras 2017; 63(4): 361–365. [DOI] [PubMed] [Google Scholar]
- 27. Marques-Sule E, Miró-Ferrer S, Muñoz-Gómez E, et al. Physical activity in health care professionals as a means of primary prevention of cardiovascular disease: a STROBE compliant cross-sectional study. Medicine (Baltimore) 2021; 100(22): e26184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Abu Saad H, Low P, Jamaluddin R, et al. Level of physical activity and its associated factors among primary healthcare workers in Perak, Malaysia. Int J Environ Res Public Health 2020; 17(16): 5947. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-docx-1-smo-10.1177_20503121241297060 for Correlation between physical activity and burnout amongst allied healthcare professionals in eThekwini, South Africa by Jeanne Martin Grace and Léchay Moodley in SAGE Open Medicine