

Abstract
Background
Blended therapy (BT) combines digital with face-to-face psychological interventions. BT may improve access to treatment, therapy uptake, and adherence. However, research is scarce on the structure of BT models.
Objective
We synthesized the literature to describe BT models used for the treatment of psychological disorders in adults. We investigated whether BT structure, content, and ratio affected treatment efficacy, uptake, and adherence. We also conducted meta-analyses to examine treatment efficacy in intervention-control dyads and associations between treatment outcomes versus BT model structure.
Methods
PsycINFO, CINAHL, Embase, ProQuest, and MEDLINE databases were searched. Eligibility criteria included articles published in English till March 2023 that described digital and face-to-face elements as part of an intervention plan for treating psychological disorders in adult patients. We developed a coding framework to characterize the BT interventions. A meta-analysis was conducted to calculate effect size (ES; Cohen d and 95% CIs) regarding pre- and posttreatment outcomes in depression and anxiety versus BT structure. The review was registered with PROSPERO and followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Results
Searches identified 8436 articles, and data were extracted from 29 studies. BT interventions were analyzed and classified according to mode of interaction between digital and face-to-face components (integrated vs sequential), role of the components (core vs supplementary), component delivery (alternate vs case-by-case), and digital materials assignment mode (standardized vs personalized). Most BT interventions (n=24) used a cognitive behavioral therapy approach for anxiety or depression treatment. Mean rates of uptake (91%) and adherence (81%) were reported across individual studies. BT interventions were more effective or noninferior to treatment as usual, with large spread in the data and a moderate to large ES in the treatment of depression (n=9; Cohen d=–1.1, 95% CI –0.6 to –1.6, P<.001, and z score=–4.3). A small, nonsignificant ES was found for anxiety outcomes (n=5; Cohen d=–0.1, 95% CI –0.3 to 0.05, P=.17, and z score=–1.4). Higher ESs were found in blended interventions with supplementary design (depression: n=11, Cohen d=–0.75, 95% CI –0.56 to –0.95; anxiety: n=8, Cohen d=–0.9, 95% CI –0.6 to –1.2); fewer (≤6) face-to-face sessions (depression: n=9, Cohen d=–0.7, 95% CI –0.5 to –0.9; anxiety: n=7, Cohen d=–0.8, 95% CI –0.3 to –1.3); and a lower ratio (≤50%) of face-to-face versus digital sessions (depression: n=5, Cohen d=–0.8, 95% CI –0.6 to –1.1; anxiety: n=4, Cohen d=–0.8, 95% CI 0.006 to –1.6).
Conclusions
This study confirmed integrated BT models as feasible to deliver. We found BT to be effective in depression treatment, but anxiety treatment results were nonsignificant. Future studies assessing outcomes across different psychological disorders and therapeutic approaches are required.
Trial Registration
PROSPERO CRD42021258977; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=258977
Keywords: systematic review, blended psychological therapy, blended care, face-to-face, online, psychological intervention, intervention design, digital care, digital mental health, psychological disorder
Introduction
The Impact of Psychological Disorders
Psychological disorders affect approximately 1 billion people globally and were responsible for 10% of the prepandemic global burden of disease in 2019, with estimates of the mental health burden increasing [1]. Depression and anxiety disorders cost US $1 trillion per year globally [2]. Evidence-based, effective mental health care is available, but its provision does not reach everyone who needs it [2,3].
Digital (or Online) Therapy
Digital psychological therapy provides an opportunity to enhance patient access to psychological treatment [4,5] and is recommended by the World Health Organization as a cornerstone of “comprehensive, integrated and responsive mental health and social care services” [1]. Research regarding digital therapy has largely focused on internet-delivered cognitive behavioral therapy (CBT), demonstrating its efficacy and cost-effectiveness [6,7], particularly in the treatment of depression and anxiety [8-12]. Although uptake and adherence to digital therapy in the research setting have shown improvement [13], engagement is still low, particularly in routine mental health care [14-17]. In addition, research suggests stakeholder preference for face-to-face interventions [18,19]. A systematic review [20] reported on concerns raised by health professionals about the use of digital therapy alone, including perceived nonsuitability for patients due to symptom severity, lack of digital access and literacy, and perception of digital treatment as being less engaging than face-to-face treatments. This review indicated that blended psychological therapy (also called “blended therapy” or “blended care”) was perceived as a midway option between digital and face-to-face therapy.
Blended Therapy
Blended therapy (BT) is a model of care that combines digital and face-to-face delivery of psychological therapy, integrating benefits from both modalities. Specifically, the face-to-face component is delivered by a mental health professional, such as a psychologist, while the digital component is patient driven [21-23]. Integrating digital therapy with face-to-face interventions in a blended model has the potential to save professionals’ and patients’ time (eg, transport to and from the clinic); increase the frequency of sessions; improve treatment uptake, adherence, and maintenance; and boost therapy effects [24-26].
A systematic review by Erbe et al [24] (N=44) found that BT may improve dropout rates and save health professionals’ time compared with exclusively face-to-face interventions. Despite increasing evidence of the benefits of blended psychological therapy for patients [22,24], there is a lack of research specifically focused on “what, how, where, and when” BT is effective to inform future BT interventions [21,22,27]. The rationale for our systematic review emerges from the scarcity of data specifically focusing on BT processes including BT content and structure, which hinders scientific reproducibility of BT and impacts its implementation success.
Objectives of This Review
Seeking to address these gaps in BT literature, our systematic review and meta-analysis expands on the work of Erbe et al [24] and aims to (1) identify and describe the structure, content, and ratio of the face-to-face and digital components in BT interventions applied for the treatment of psychological disorders and (2) investigate whether there is an association among the structure, content, and ratio of blended components and the treatment efficacy of, uptake of, and adherence to BT.
Methods
Design
This review followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [28] guidelines and was registered with PROSPERO (CRD42021258977). The PRISMA checklist is provided in Multimedia Appendix 1.
Search Strategy
The PsycINFO, CINAHL, Embase, ProQuest, and MEDLINE databases were searched using keywords and Medical Subject Headings terms—“blended”; “online”; “face-to-face”; “treatment”; “therapy”; “care”; “mental disorders”; “psychological distress”; and “psychological disease”—for articles published in English (Multimedia Appendix 2). The search included articles published till May 2022, and an updated search was conducted in March 2023. Reference lists of the included studies were also manually searched.
Study Selection
Inclusion and Exclusion Criteria
Studies that described or applied an intervention where both digital and face-to-face elements were integrated or delivered sequentially were included. We included studies in which the participants were aged ≥18 years and diagnosed with a psychological disorder. Studies solely investigating populations other than this target group (health care professionals, student cohorts, employees, etc) were excluded.
Comparators
The comparator or control groups included treatment as usual (pharmacological or psychological intervention and standard medical care), waitlist, or other interventions.
Data Abstracted
The primary focus was the intervention design, including descriptions of the structure, content, and ratio of the sessions used in each model. Secondary outcomes were (1) a psychological therapy approach used in the BT models, (2) patient groups for which BT was applied, (3) treatment efficacy, (4) uptake and adherence, (5) health service outcomes (eg, cost-effectiveness), (6) patients’ acceptability of BT, (7) therapeutic alliance rates, and (8) barriers and facilitators reported.
Article Screening and Selection
All search results were uploaded into Covidence software [29]. Two reviewers (KFN-Z and JMS) screened the titles and abstracts independently. Full-text reviews based on the eligibility criteria were conducted by KFN-Z and PB or JMS.
Data Extraction
Data extraction was conducted by KFN-Z using a purpose-designed data extraction template. Extraction results were partially reviewed (6/29, 20%) by a second coder (JMS) to assess accuracy. To capture any missing data, the corresponding authors were e-mailed twice. Data extracted included the following: (1) study characteristics—authors, year of publication, country, study setting, study aims, study type, sample size, control group (where applicable), therapy approach applied, primary or secondary psychological outcomes, and symptom assessment measures and participant characteristics such as age, sex, diagnosed psychological disorders, severity of symptoms, and individual study outcomes; (2) intervention characteristics—BT intervention design based on the structure, content, and ratio of BT sessions; number, periodicity, and duration (in minutes) of face-to-face and digital sessions; treatment length (in weeks); and (3) BT intervention outcomes—treatment efficacy, uptake, adherence, cost-effectiveness, acceptability, therapeutic alliance, and barriers and facilitators to BT reported.
Data Analysis
To address the objectives of this review, quantitative variables regarding the BT intervention structure were summarized and described. We used descriptive statistics (mean, percentages, and range) to describe quantitative data regarding study and participant characteristics; BT intervention uptake, adherence, and completion rates; treatment length (in weeks); number, time (in minutes), ratio, and periodicity of face-to-face and digital sessions; treatment acceptability; efficacy; and therapeutic alliance. Barriers to and facilitators of BT were qualitatively analyzed using a thematic analysis [30] approach. Qualitative data on BT structure and content were analyzed using a content analysis approach [31]. Categories and subcategories were summarized in a framework that builds on the concepts described by Erbe et al [24] (Textbox 1).
Classification—blended model designs.
Interaction between face-to-face and digital components: integrated vs sequential
Integrated models present both the digital and face-to-face components as collaborating parts within a therapy regimen, with both components delivered within the course of the intervention [24].
-
Sequential models present the digital component delivered in entirety before or after face-to-face component delivery [24]. Sequential interventions start by delivering a “batch” of either face-to-face or digital sessions. Once the first “batch” is finished, the other component gets delivered.
Stepped care is considered a special type of sequential design in which the digital component is a step in the intervention sequence [24]. Stepped care interventions deliver the least intensive or costly treatment first and then progress to more intensive or aftercare treatment, if required. Hence, the “blend” in stepped care only effectuates after the first stage (digital) of treatment is complete and if patients require additional (face-to-face) care.
Role of the components in the intervention: core vs supplementary
Core components are an indispensable part of the blended intervention, as they deliver new therapeutic elements (ie, modules complement each other).
Supplementary components present content that has already been discussed during the intervention, that is, content of one component is supplementary to the content delivered in the main component. For example, face-to-face content may be supplemented by reinforcing exercises and homework on the web.
Delivery pattern of face-to-face or digital components: alternate vs case by case
-
Alternate delivery is a configuration in which each session is delivered by alternating face-to-face or digital components in a fixed ratio. The distribution of components is preset for the entire intervention; this may feature as a 1:1 ratio, but other ratios (eg, 2 digital to1 face-to-face) of distribution are possible.
Linear delivery is specific to sequential designs in which all digital sessions are delivered in a row followed by all face-to-face sessions in a row, or vice versa.
Case-by-case delivery is a configuration in which therapists assess and formulate a strategy for distributing the face-to-face or digital sessions adapted to the clients’ or patients’ needs on a case-by-case basis.
Digital content assignment: personalized vs standardized
Personalized content assignment is not preset; therapists and patients decide which materials to complete, tailoring them to patients’ needs.
Standardized content assignment is largely preset; materials are delivered to all patients undergoing treatment with little or no changes to content.
Meta-Analyses
Although a meta-analysis was not originally included in the registered protocol, data collection and analysis processes indicated the relevance of meta-analyzing treatment outcomes for enhancing systematic review results. The meta-analysis was conducted using the Comprehensive Meta-Analysis program [32] to investigate treatment efficacy between the treatment and control dyads. A meta-analysis of BT interventions only was also conducted to investigate associations between BT structure and content and treatment outcomes. Pre-post outcome means and SD, alongside data on sample size at post–time points were included in the analysis. Standardized difference in means (Cohen d) and 95% CIs were used as effect size (ES) measures, and z values were used to test the null hypothesis (ES=0). We used a random effects meta-analysis due to expected heterogeneity. ES was set to negative numbers to show the change in symptoms (the lower the number, the higher the reduction in symptoms). Heterogeneity was assessed using Q test (Q), I-squared (I2), Tau-squared (T2), and Tau (T) scores. Publication bias was assessed using funnel plots and the trim and fill method by Duval and Tweedie [33].
Risk of Bias and Quality Assessment
Two independent reviewers (KFN-Z and JMS) assessed the risk of bias using the National Institutes of Health Study Quality Assessment Tool (quantitative) [34], the Critical Appraisal Skills Programme qualitative checklist [35], or the Mixed Methods Appraisal Tool [36].
Results
Database Search Results
Database searches identified 2650 papers after removal of duplicates. Title and abstract screening resulted in 103 articles for full-text review. A total of 30 eligible articles were identified but only 29 were included in the review—one eligible paper was excluded as it reported the same data. The PRISMA diagram in Figure 1 [28] provides the details of the process.
Figure 1.
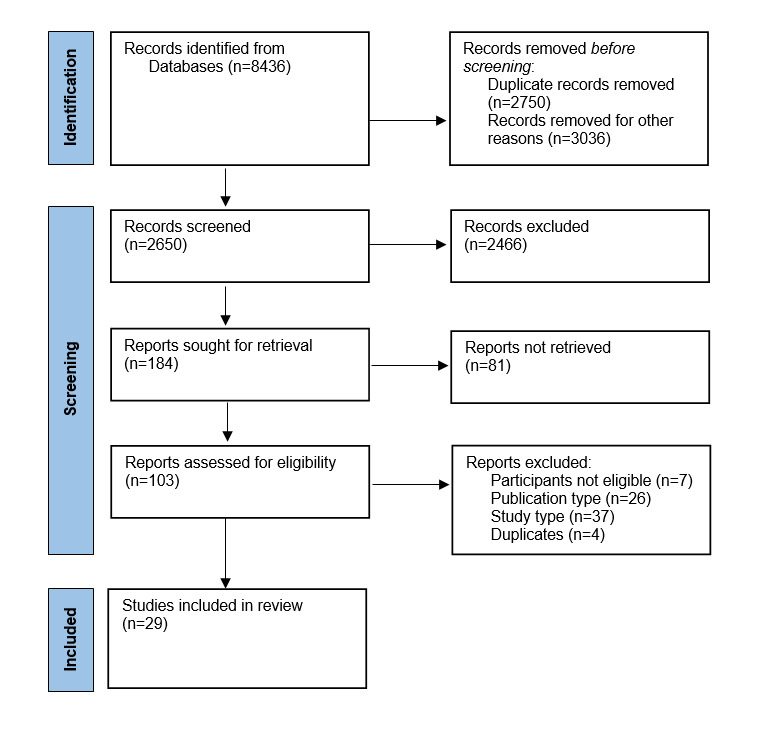
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 flow diagram.
Quality Assessment
Quality assessment deemed most studies (n=22) to be of “good quality” as they addressed most of the quality assessment criteria applied. Seven articles [23,37-42] were classified to be of “fair” quality (Multimedia Appendix 3).
Study Characteristics
Of the 29 articles, 25 (86%) were prospective studies (randomized controlled trials [RCTs], n=14; feasibility or pilot, n=4; cohort or single arm, n=7); 3 (10%) were retrospective analyses of cohort studies; and 1 (3%) study used qualitative methods only. Most BT interventions (22/29, 76%) primarily treated depression, either exclusively (13/29, 45%) or in combination with anxiety treatment (9/29, 31%). Most studies (28/29, 96%) used a CBT approach, with 3 (10%) combining CBT and other approaches such as dialectical behavioral therapy and acceptance and commitment therapy (n=2) and motivational interviewing (n=1). Outcomes assessed were primarily symptom reduction (25/29, 86%), although 4 (14%) studies reported on the intervention process or working alliance outcomes as the primary focus (Table 1).
Table 1.
Characteristics of reviewed studies.
| Study; country | Study setting | Study aims | Study design | Participants, N; BTa group, n; comparator, n | Therapy type; clinical outcomes |
| Askjer and Mathiasen [43], 2021 and Mathiasen et al [44],b 2022; Denmark | Specialized mental health care | Explore if WAc predicted treatment outcomes | Exploratory; secondary analysis from an RCTd | 76; 38; 38; comparator: F2Fe CBTf | CBT; WA, depressive symptoms |
| Berger et al [45], 2018; Germany | Routine outpatient psychotherapy practices | Investigate web-based treatment as adjunctive to depression treatment vs regular psychotherapy | Two-armed, pragmatic RCT | 98; 51; 47; comparator: TAUg: psychotherapy | CBT; depressive symptoms |
| Bisson et al [46], 2022; United Kingdom | Primary and secondary mental health settings | Determine if CBT-TFh was noninferior to F2F CBT-TF for PTSDi | Pragmatic, multicenter, noninferiority RCT | 196; 97; 99; comparator: F2F CBT-TF | CBT; severity of symptoms of PTSD |
| Cloitre et al [47], 2022; United States | Routine care in mental health outpatient clinics | Assess 2 ratios of F2F sessions to self-guided work on trauma-exposed veterans | Quasi-experiment with a noninferiority design | 202; 202; NCj | Transdiagnostic, trauma-informed CBT; PTSD and depression |
| Duffy et al [48], 2020; England | Specialized mental health care service | Investigate iCBTk as a prequel for high-intensity depression and anxiety treatment | Uncontrolled feasibility design (open study) | 123; 123; NC | CBT; anxiety and depression and work and social functioning |
| Etzelmueller et al [49], 2018; Germany | Routine care practice (clinics) | Evaluate patient experience of a blended iCBT service | Qualitative, semistructured interviews | 15; 15; NC | CBT; NDl depression |
| Høifødt et al [37], 2013; Norway | University outpatient clinic | Evaluate effectiveness and acceptability of a guided web-based program for depression | RCT | 106; 52; 54; comparator: delayed treatment, waitlist, or TAU | CBT; depression symptoms |
| Jacmon et al [42], 2009; Australia | Psychology private practice | Assess cost-effectiveness and convenience of partially digital depression treatment | Single-arm, pretest-posttest study | 9; 9; NC | CBT; depression levels |
| Kemmeren et al [50], 2019; France, Germany, Poland, and Netherlands | Multisetting (specialized mental health and routine primary care) | Examine use of and engagement to blended CBT for depression | Exploratory, secondary study from RCT | 231; 231; NC | CBT; ND depression |
| Kenter et al [51], 2013; Netherlands | Mental health care center; routine care | Report on the uptake of digital treatment, on the profile of patients who prefer digital therapy, and on symptom reduction vs waitlist | Observational study (electronic patient database) | 104; 55; 49; comparator: waitlist | PSTm; ND depression, anxiety, and burnout |
| Kenter et al [52], 2015; Netherlands | Mental health service | Compare the effects and costs between blended and F2F treatments | Naturalistic study: examined records of patients | 4448; 168; 4280; comparator: TAU: F2F | CBT; ND depression and anxiety |
| Kok et al [38], 2014; Netherlands | Outpatient clinics | Assess clinical effectiveness of internet-based guided self-help vs waitlist | RCT | 212; 105; 107; comparator: waitlist | Psychotherapy; phobia and avoidance behavior |
| Kooistra et al [23], 2016; Netherlands | Outpatient specialized mental health care center | Develop and evaluate a structured, blended CBT protocol for patients with depression | Focus-groups and single-arm, pre-post | 30; 9; NC (12 patients) | CBT; ND depression |
| Kooistra et al [26], 2019; Netherlands | Specialized mental health care (outpatient services) | Compare costs and effectiveness of blended vs standard CBT for depression | Pilot RCT with 2 parallel groups | 102; 53; 49; comparator: CBT-F2F | CBT; self-reported depression severity |
| Kooistra et al [53], 2020; Netherlands | Outpatient specialized mental health clinics | Investigate WA in bCBTn for depression | Exploratory, secondary study from pilot RCT | 92; 47; 45; comparator: regular CBT | CBT; ND depression levels |
| Lungu et al [54], 2020; United States | Employer program | Evaluate the effectiveness of a video-based CBT and internet intervention | Retrospective cohort study | 385; 385; NC | CBT+UTPo, ACTp, and DBTq; ND depression and anxiety |
| Ly et al [55], 2015; Sweden | Clinical setting | Evaluate a blended treatment for depression | Noninferiority RCT | 93; 46; 47; comparator: F2F BAr | BA; depression |
| Månsson et al [39], 2013; Sweden | Clinical setting | Explore clinical outcomes and user experiences of internet-delivered therapy. To develop or test a bCBT model | Mixed methods, case series, pilot study (pre-post re BT testing) | 23; 15; NC (patients, n=15; therapists, n=8) | CBT; ND anxiety and depression |
| Månsson et al [40], 2017; Sweden | Outpatient psychiatric clinic | Evaluate an internet-based support as adjunct to F2F CBT | Feasibility study | 54; 45; NC (patients, n=45; therapists, n=9) | CBT; ND anxiety and depression symptoms |
| Mol et al [56], 2018; Netherlands | Outpatient clinic | Explore therapist behaviors; adherence; and patient outcome in digital therapy | Observational study | 64; 45; NC (patients, n=45; therapists, n=19) | CBT; ND depression levels |
| Nakao et al [57], 2018; Japan | Outpatient medical institutions | Evaluate effectiveness of web-based bCBT in reducing therapist time in patients with depression | Single-blinded RCT | 40; 20; 20; comparator: waitlist + pharmacological treatment | CBT; depression symptoms |
| Romijn et al [41], 2021 and Romijn et al [58];b Netherlands | Outpatient specialized mental health care centers | Explore therapist fidelity to bCBT protocols for anxiety disorders | Mixed methods (derived from a larger RCT) | 114; 52; 62; comparator: CBT F2F | CBT; anxiety symptoms |
| Tarp et al [59], 2022; Denmark | Public municipal outpatient alcohol clinics | Describe development and testing of a digital program; participant experiences; and usability of BT | Feasibility and pilot study | 32; 22; NC (development: 7 therapists+3 patients) | CBT + motivational interviewing; —s (intervention system usability) |
| Thase et al [60], 2018; United States | Department of psychiatry of medical schools | Evaluate the efficacy of computer and therapist-assisted CBT vs standard CBT | Noninferiority RCT | 154; 77; 77; comparator: CBT F2F | CBT; depression symptom severity |
| van de Wal et al [61], 2017; Netherlands | Cancer hospitals: academic, regional, and outpatient | Investigate the efficacy of BT for FCRt in cancer survivors | RCT: 2-arm, parallel group, longitudinal | 88; 45; 43; comparator: TAU (any) | CBT; FCR severity |
| Vernmark et al [62], 2019; Sweden | Mental health care centers | Explore patient- and therapist-rated WA in bCBT and WA as a predictor for change | Exploratory secondary study from RCTs | 151; 75; NC | CBT; depression levels |
| Witlox et al [63], 2021; Netherlands | Mental health service at general practices | Examine the effectiveness of blended ACT for older adults with anxiety | RCT (single-blinded) | 314; 150; 164; comparator: TAU (FTF CBT) | ACT; anxiety severity |
| Wu et al [64], 2021; United States | Employer mental health program clinical services | Evaluate the outcomes of a blended care coaching program for anxiety and depression | Retrospective cohort analysis | 1496; 1496; NC | CBT-based + CBT, DBT, and ACT; anxiety and depression symptoms |
| Wu et al [65], 2021; United States | Employer mental health program clinical services | Examine the effectiveness and the impact of bCBT on anxiety and depression | Retrospective cohort analysis | 3401; 3401; NC | CBT+DBT and ACT; anxiety and depression symptoms |
aBT: blended therapy.
bLinked study.
cWA: working alliance.
dRCT: randomized controlled trial.
eF2F: face to face.
fCBT: cognitive behavioral therapy.
gTAU: treatment as usual.
hiCBT-TF: internet-guided cognitive behavioral therapy with trauma focus.
iPTSD: posttraumatic stress disorder.
jNC: no comparator.
kiCBT: internet-delivered cognitive behavioral therapy.
lND: not disclosed.
mPST: problem-solving therapy.
nbCBT: blended cognitive behavioral therapy.
oUTP: unified transdiagnostic protocol.
pACT: acceptance and commitment therapy.
qDBT: dialectical behavioral therapy.
rBA: behavioral activation.
sNot applicable.
tFCR: fear of cancer recurrence.
Collectively, the studies included a total of 12,322 (range 3-4448) patient participants, with 57.71% (n=7111) receiving BT interventions. Of the studies reporting on symptom reduction (28/29, 96%), all prescreened for clinical levels of psychological morbidity (Table 2).
Table 2.
Patient participants’ characteristics.
| Study | Age (y), mean (SD); range | Female, n (%) | Pre-post time points, assessment tool, psychological symptoms per group: mean (SD) and severity at baseline |
| Askjer and Mathiasen [43], 2021 | 35 (13.96); 18-71 | 56 (74) |
|
| Berger et al [45], 2018 | 43 (12.0); 19-73 | 65 (66) |
|
| Bisson et al [46], 2022 | 36 (13.4); 18 to >65 | 125 (64) |
|
| Cloitre et al [47], 2022 | 44 (11.73); 22-77 | 122 (60) |
|
| Duffy et al [48], 2020 | 41 (13.1); 17-80 | 85 (69) |
|
| Etzelmueller et al [49], 2018 | 55 (—); 24-64 | 18 (72) |
|
| Høifødt et al [37], 2013 | 36 (11.3); 19-63 | 77 (73) |
|
| Jacmon et al [42], 2009 | 35 (10.37); — | 4 (44) |
|
| Kemmeren et al [50], 2019 | 42 (12.9); 18-74 | 129 (64) |
|
| Kenter et al [51], 2013 | 37 (10.8); 18-61 | 73 (70) |
|
| Kenter et al [52], 2015 | 47 (18.7); 18-91 | 2442 (55) |
|
| Kok et al [38], 2014 | 35 (11.7); — | 130 (61) |
|
| Kooistra et al [23], 2016 | 38 (8.36); 27-50 | 5 (55) |
|
| Kooistra et al [26], 2019 | 39 (10.9); — | 64 (63) |
|
| Kooistra et al [53], 2020 | 38 (11.0); — | 43 (60) |
|
| Lungu et al [54], 2020 | 33 (8.0); — | 244 (64) |
|
| Ly et al [55], 2015 | 31 (11.4); 18-73 | 65 (70) |
|
| Månsson et al [39], 2013 | 43 (15); 22-70 | 10 (67) |
|
| Månsson et al [40], 2017 | 30 (10.6); 18-60 | 36 (80) |
|
| Mol et al [56], 2018 | 36 (12.3); 21-64 | 33 (73) |
|
| Nakao et al [57], 2018 | 40 (9.7); — | 20 (50) |
|
| Romijn et al [41], 2021 | 37 (11.0); 19-62 | 23 (52) |
|
| Tarp et al [59], 2022 | 47 (12); 28-73 | 7 (32) |
|
| Thase et al [60], 2018 | 46 (14.3); — | 102 (66) |
|
| van de Wal et al [61], 2017 | 59 (11.3); 31-77 | 47 (53) |
|
| Vernmark et al [62], 2019 | 35 (13.9); — | 54 (74) |
|
| Witlox et al [63], 2021 | 63 (5.70); 55-75 | 192 (61) |
|
| Wu et al [64], 2021 | 33 (8.62); — | 921 (62) |
|
| Wu et al [65], 2021 | 33 (8.68); — | 2218 (65) |
|
aPHQ-9: Patient Health Questionnaire-9.
bBT: blended therapy.
cBDI-II: Beck Depression Inventory II.
dGAD-7: Generalized Anxiety Disorder-7.
eCAPS-5: Clinician-Administered Posttraumatic Stress Disorder Scale for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
fPTSD: posttraumatic stress disorder.
gPCL-5: Posttraumatic Stress Disorder Checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
hNot available.
iiCBT: internet-delivered cognitive behavioral therapy.
jQIDS-16-SR: 16-Item Quick Inventory of Depressive Symptomatology, self-reported.
kBAI: Beck Anxiety Inventory.
lHADS: Hospital Anxiety and Depression Scale.
mMBI: Maslach Burnout Inventory.
nGAF: Global Assessment of Functioning.
oFQ: Fear Questionnaire.
pCES-D: Centre for Epidemiologic Studies Depression Scale.
qIDS-SR30: Inventory of Depressive Symptomatology Self-Rated.
rMADRS-S: Montgomery Åsberg Depression Rating Scale—self-rating version.
sGRID-HAMD: 17-item GRID-Hamilton Depression Rating Scale score.
tHDRS: Hamilton Depression Rating Scale.
uCWS: Cancer Worry Scale.
Primary outcomes of individual studies included efficacy or effectiveness (14/29, 48%) [37-39,45,46,48,54,55,57, 60,61,63-65]; working alliance (3/29, 10%) [43,53,62]; usability and uptake (3/29, 10%) [50,51,59]; feasibility (2/29, 7%) [23,42]; and patient or therapist (4/29, 14%) [40,41,49,56] experience. One (4%) study [47] explored multiple primary outcomes of therapeutic alliance, compliance, and symptom reduction, and 2 (7%) studies [26,52] reported dual outcomes of efficacy and cost.
Classification of BT Models
On the basis of the models defined by Erbe et al [24], the majority (26/29, 90%) of the studies reported an integrated intervention design, where new therapeutic content was delivered either (1) across both the face-to-face and digital modalities (core; n=14) or (2) primarily using one modality (usually the face-to-face component) with additional content delivered as supplementary material (n=12). Integrated interventions were the most common designs for addressing depression (n=14) and depression and or anxiety (n=8). Three studies were classified as sequential designs and described a core role for both face-to-face and digital components. One sequential model was delivered as stepped care in which most patients received digital therapy only.
BT delivery was further differentiated based on whether both components were delivered in a preset, alternate format or a tailored, case-by-case arrangement. Most integrated interventions (17/26, 65%) used an alternate delivery format. Therapeutic content within integrated and alternate designs had either core (9/17, 53%) or supplementary (8/17, 47%) roles.
In 19 (65%) studies, patients engaged with digital content following a standardized program with minimal tailoring of the materials presented. In contrast, 10 (35%) studies described a more personalized manner of assigning or interacting with digital content where the therapist and patient have more autonomy to choose, change, or create digital content according to individual need. An overview of model classifications is presented in Table 3.
Table 3.
Blended therapy model classification per study.
| Study | Interaction of F2Fa and digital components | Role of F2F and digital components | Pattern of delivery of F2F and digital | Digital content delivery | |||||||
|
|
Integrated | Sequential | Core | Supplementary | Alternate | Case by case | Personalized | Standardized | |||
| Askjer and Mathiasen [43], 2021 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Berger et al [45], 2018 | ✓ |
|
|
✓ |
|
✓ | ✓ |
|
|||
| Bisson et al [46], 2022 | ✓ |
|
|
✓ |
|
✓ | ✓ |
|
|||
| Cloitre et al [47], 2022 | ✓ |
|
|
✓ | ✓ |
|
|
✓ | |||
| Duffy et al [48], 2020b |
|
✓ | ✓ |
|
|
|
✓ |
|
|||
| Etzelmueller et al [49], 2018 | ✓ |
|
|
✓ |
|
✓ | ✓ |
|
|||
| Høifødt et al [37], 2013 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Jacmon et al [42], 2009 | ✓ |
|
✓ |
|
|
✓ |
|
✓ | |||
| Kemmeren et al [50], 2019 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Kenter et al [51], 2013b |
|
✓ | ✓ |
|
|
|
|
✓ | |||
| Kenter et al [52], 2015 | ✓ |
|
✓ |
|
|
✓ |
|
✓ | |||
| Kok et al [38], 2014b |
|
✓ | ✓ |
|
|
|
|
✓ | |||
| Kooistra et al [23], 2016 | ✓ |
|
|
✓ | ✓ |
|
|
✓ | |||
| Kooistra et al [26], 2019 | ✓ |
|
|
✓ | ✓ |
|
|
✓ | |||
| Kooistra et al [53], 2020 | ✓ |
|
|
✓ | ✓ |
|
|
✓ | |||
| Lungu et al [54], 2020 | ✓ |
|
|
✓ | ✓ |
|
✓ |
|
|||
| Ly et al [55], 2015 | ✓ |
|
|
✓ | ✓ |
|
✓ |
|
|||
| Månsson et al [39], 2013 | ✓ |
|
|
✓ |
|
✓ | ✓ |
|
|||
| Månsson et al [40], 2017 | ✓ |
|
|
✓ |
|
✓ | ✓ |
|
|||
| Mol et al [56], 2018 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Nakao et al [57], 2018 | ✓ |
|
✓ |
|
✓ |
|
✓ |
|
|||
| Romijn G et al [41], 2021 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Tarp et al [59], 2022 | ✓ |
|
✓ |
|
|
✓ |
|
✓ | |||
| Thase et al [60], 2018 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| van de Wal et al [61], 2017 | ✓ |
|
|
✓ | ✓ |
|
|
✓ | |||
| Vernmark et al [62], 2019 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Witlox et al [63], 2021 | ✓ |
|
✓ |
|
✓ |
|
|
✓ | |||
| Wu et al [64], 2021 | ✓ |
|
✓ |
|
|
✓ | ✓ |
|
|||
| Wu et al [65], 2021 | ✓ |
|
✓ |
|
|
✓ | ✓ |
|
|||
aF2F: face to face.
bSequential models present a linear pattern of delivery.
Structure, Content, and Ratio of Sessions in BT Models
Overview
Within the integrated model, 81% (21/26) of studies reported commencing BT with the face-to-face component. Five integrated interventions began treatment with the digital component; of those, 4 [38,42,47,51] used the digital component as the intervention “anchor”—that is, the digital component led the therapeutic process. One [48] sequential intervention (stepped care) used the digital modality as a prequel for high-intensity face-to-face treatment based on patient symptom severity. Digital sessions were mostly delivered via website platforms with individualized access. Overall, digital session components presented CBT-based content and followed the frameworks used in face-to-face settings. Digital content was typically asynchronous. Intervention structure and content is summarized in Multimedia Appendix 4.
Face-to-Face Versus Digital Sessions Distribution in BT Models
In total, 26 (87%) studies reported the number of face-to-face sessions, which ranged from 3 to 21 sessions (mean 7, SD 4.2). Of those reporting the number of face-to-face sessions, 24 (92%) used an integrated intervention design. Mean face-to-face session duration across studies was 49 minutes (SD 11.7, range 27-65 min/session). Periodicity of sessions were reported by 24 studies, with most of those studies describing face-to-face sessions as delivered weekly (12/24, 50%) [23,26,37,39,41,42,45,49,53,57,59,64].
A total of 20 (69%) studies reported on the number of digital sessions (mean 8, SD 3, range 4-14 sessions)—of those studies, 18 (90%) presented an integrated design. Although the mean time for digital sessions was largely undefined and unreported, 12 (41%) studies [37,40,45,47,50,52,57,60-63,65] reported that digital modules were typically developed to range between 15 and 60 minutes. Eight (28%) studies [42,45,46,48,57,59,60,64] allowed patients to complete modules at their own pace; 13 (45%) studies [39,40,42,45,48,49,54-56,60,61,64,65] reported digital sessions’ periodicity to be flexible; weekly (14/29, 48%) [23,26,37,38,41,46,47,51-53,57,59,62,63] or fortnightly (2/29, 7%) [43,50] completion was also reported.
Face-to-Face and Digital Ratio
In total, 16 (55%) studies [23,26,37,41,42,45-50,53,56,60,62,65] reported the ratio of face-to-face and digital sessions. Most of those studies had an integrated design (14/16, 88%) and typically delivered sessions at a 1:1 ratio (1 face-to-face to 1 digital).
Treatment Length
The BT mean length of treatment was 12 (SD 5.1, range 6-26) weeks; however, this was unreported for 5 studies [38,49,51,52,63] (Table 4).
Table 4.
Model classification versus session structure.
|
|
Integrated (n=26) | Sequential (n=3) | Core (n=17) | Supplementary (n=12) | Alternate (n=17) | Case by case (n=9) | Lineara (n=3) | Personalized (n=10) | Standardized (n=19) | |
| Treatment lengthb, mean (range); n | 12 (6-21); 23 | 21; (—c); 1 | 13 (6-26); 13 | 11 (6-21); 11 | 13 (6-26); 16 | 10 (6-12); 7 | 21; (—); 1 | 10 (6-21); 9 | 14 (8-26); 15 | |
| Face-to-face sessions | ||||||||||
|
|
Number, mean (range); n | 8 (3.5-21); 23 | 3.5 (0-10); 3 | 6 (0-12); 15 | 9 (4-21); 11 | 7 (3.5-12); 17 | 9 (4-21); 6 | 10; (—); 1 | 9 (4-21); 9 | 6 (0-12); 17 |
|
|
Time (min), mean (range); n | 49 (27-65); 17 | NRd; 0 | 47 (27-65); 9 | 51 (45-65); 8 | 46.5 (27-65); 12 | 55 (45-60); 5 | NR; 0 | 53 (44-60); 6 | 47 (27-65); 11 |
|
|
Periodicity | 1we: n=12; 2wf: n=4; 3wg: n=1; varh: n=7 | NR; (0) | 1w: n=6; 2w: n=3; 3w: n=1; var: n=3 | 1w: n=6; var: n=4; 2w: n=1 | 1w: n=6; 2w: n=4; 3w: n=1; var: n=6 | 1w: n=6; var: n=1 | NR | 1w: n=5; var: n=3 | 1w: n=7; 2w: n=4; 3w: n=1; var: n=4 |
| Digital sessions | ||||||||||
|
|
Number, mean (range); n | 9 (4-14); 17 | 4 (4-5); 2 | 7 (4-14); 11 | 9 (7-14); 8 | 7 (4-10); 11 | 10 (6-14); 6 | 4; 1 | 8 (4-14); 5 | 8 (4-14); 15 |
|
|
Time (min), mean (range); n | 38 (6-65); 8 | NR; 0 | 44 (30-65); 4 | 32 (6-62); 4 | 38 (28-65); 5 | 38 (6-62); 3 | NR; 0 | 36 (6-62); 4 | 40 (28-65); 4 |
|
|
Periodicity | 1w: n=13; 2w: n=1; var: n=12 | 2w: n=1; anyi: n=2 | 1w n=9; 2w: n=2; any: n=6 | 2w: n=4; any: n=8 | 1w: n=9; 2w: n=2; any: n=6 | 1w: n=2; any: n=7 | 1w: n=2; any: n=1 | 1w: n=1; any: n=9 | 1w: n=12; 2w; n=2; any: n=5 |
aLinear describes the delivery pattern typical of sequential designs.
bTreatment length is measured in weeks.
cNot applicable.
dNR: not reported.
e1w: weekly.
f2w: 2-weekly.
g3w: 3-weekly.
hvar: variable (eg, varied from weekly to fortnightly or other pattern).
iany: anytime (ie, no pattern from the outset).
Outcomes of BT Interventions
Treatment Uptake
In total, 25 (86%) studies reported on BT uptake mean rates (mean 91%, SD 10.2%, range 60%-100%). Of those, 24 (96%) studies [23,26,37-43,45-48,50,51,53,55-57,59-63] reported a mean uptake of 92% (SD 8.2%, range 73%-100%) and 1 (4%) study [49] reported a lower uptake (60%). A total of 14 (48%) studies reported on treatment completion rates, with an average of 61% (SD 29.4%, range 11.5%-100%) of patients completing treatment.
Treatment Adherence
Our review considered adherence as completing a minimum number of sessions determined by each study. However, adherence criteria differed across studies and there was a lack of data to confirm whether session structure or ratio influenced adherence to intervention. A total of 23 (279%) studies reported on BT adherence rates, with a mean of 81% (SD 11.8%). In total, 20 (69%) integrated studies reported on BT adherence (mean 83%, SD 11%, range 62%-100%). In contrast, all sequential studies (3/29, 10%) had a comparatively lower mean adherence (64%, SD 1.8). Dropout rates were reported in 25 (86%) studies, with 24 of those reporting <40% dropout rates (mean 18.5%, SD 17.2%, range 0%-38%). The intervention with the lowest adherence rate (16%) and highest dropout rate (84%) [38] had a sequential design.
Regarding the role of components within BT, interventions with supplementary designs presented higher adherence (mean 88%, SD 9%, range 72.5%-100%) than core designs (mean 76%, SD 11.7%, range 16%-100%). Details on the uptake and adherence reported per study are available in Multimedia Appendix 5.
Health Service Outcomes
Four (14%) studies reported on the impact of BT on therapist time: 2 studies [42,55] found a decrease, one study reported an increase [52], and one found no change [26] in the time needed to deliver therapy. Findings related to efficacy and costs were mixed, with one study [52] suggesting that BT was not cost-effective compared with face-to-face therapy, while another study [55] highlighted reduced costs due to the potential of BT for treating twice as many patients as compared with face-to-face treatment.
Patient Satisfaction and Working Alliance
Eight (28%) studies [23,37,38,43,45,46,49,63] reported on patient satisfaction with BT treatment—criteria for determining patient satisfaction were heterogeneous, but all studies reported it as “high.” Four (14%) studies [43,47,53,62] reported on working alliance and reported it as “high.” Two (7%) studies [43,62] suggested that the therapist-rated working alliance predicted treatment outcomes and that this may be specific to BT.
Barriers to and Facilitators of Intervention Uptake and Engagement
Potential barriers to intervention uptake reported [23,46,49,51,59] included a lack of understanding about the intervention and digital challenges. Reported [42,51,59] facilitators to intervention uptake included convenience and flexibility of the digital component, anonymity, and autonomy enabled by the BT design. Barriers to intervention engagement identified [37,38,42,45,46,48-50,56,61] included the good enough effect (ie, when patients drop out during the initial stages of the intervention arguing they “feel better” and “no longer need therapy” [66]), being left unchecked, reduced therapy support (ie, lack of therapist follow-up regarding digital activities), and digital challenges. Facilitators of intervention engagement included experience in the use of technology, a program tailored to patient-specific needs, patient-therapist digital communication between sessions, and a patient-therapist working alliance fostered throughout the intervention [37-39,43,45-50,52,57,64,65].
Treatment Efficacy
We conducted a meta-analysis to examine differences in treatment outcomes. There were only a sufficient number of studies to meta-analyze depression and anxiety outcomes.
Data pooled from 9 RCT studies demonstrated a moderate to large, significant improvement in depression symptoms (Cohen d=–1.1, 95% CI –0.6 to –1.6, P<.001). However, comparing treatment outcomes for anxiety interventions with controls (n=5), there was no significant improvement across studies (Cohen d=–0.1, 95% CI –0.3 to 0.05, P=.17). Between-study heterogeneity was high and did not change after conducting publication bias assessment using the funnel plot trim and fill method, both in the depression (Q=90.3; P<.001; I2=91.1; T2=0.1; T=0.7) and anxiety groups (Q=1.1; P=.17; I2=0; T2=0; T=0). We noted that estimates of heterogeneity are impacted by the very small number of studies analyzed (<10 studies).
Meta-analysis was also conducted to examine associations between depression and anxiety scores on various scales and BT structure. For depression, mixed-effect analysis suggested higher effects sizes for interventions where the therapeutic content was delivered primarily face to face with digital content supplementing the face-to-face content (n=11; Cohen d=–0.75, 95% CI –0.56 to –0.95) compared with digital therapeutic content delivered as core (n=10; Cohen d=–0.5, 95% CI –0.4 to –0.7)—however, differences were not statistically significant (P<.08). Similar associations were found for anxiety, with higher ESs for supplementary (n=8; Cohen d=–0.9, 95% CI –0.6 to –1.2) compared with core structure (n=5; Cohen d=–0.6, 95% CI –0.22 to –0.98). Mixed-effect analysis also indicated statistically significantly (P<.001) higher ESs for interventions with ≤6 face-to-face sessions both for depression (n=9; Cohen d=–0.7, 95% CI –0.5 to –0.9) and anxiety (n=7; Cohen d=–0.8, 95% CI –0.3 to –1.3) compared with interventions with >6 face-to-face sessions for depression (n=11; Cohen d=–0.6, 95% CI –0.4 to –0.8) and anxiety (n=5; Cohen d=–0.7, 95% CI –0.4 to –1). Similarly, interventions with >50% of sessions delivered digitally had higher ESs (P<.001) both for depression (n=5; Cohen d=–0.8, 95% CI –0.6 to –1.1) and anxiety (n=4; Cohen d=–0.8, 95% CI 0.006 to –1.6) compared with interventions where >50% sessions were delivered face to face, both for depression (n=9; Cohen d=–0.5, 95% CI –0.3 to –0.7) and anxiety (n=3; Cohen d=–0.58, 95% CI –0.3 to –0.9). Data regarding meta-analyses are available in Multimedia Appendix 6.
Discussion
Overview
We reviewed blended psychological therapy models and classified them according to their structure, content, and ratio of face-to-face and digital sessions. Most BT interventions were CBT-based and addressed depression—for which models with integrated and supplementary designs resulted in improved treatment efficacy. Interventions typically used an integrated design with the face-to-face component “anchoring” the intervention. Essential, therapeutic content across treatment designs was typically delivered as both face to face and digital (ie, a core design) and in an alternate pattern. However, several studies used digital components to supplement therapeutic content delivered face to face. Most interventions also relied on standardized digital content rather than content tailored to individual patients.
Our study confirms that BT leads to improved overall patient uptake (mean 91%) and adherence (mean 81%), contrasting with the lower uptake and adherence rates previously reported for digital therapy alone. For example, an observational cohort study analyzed clinical data from 15,882 patients assessed for digital-only treatment of various psychological disorders, reporting 22% uptake and 68% adherence rates [14]. In addition, review studies on digital therapy for depression and anxiety symptoms [16] and for depression alone [17] indicated mean uptake rates of 56% (range 21%-88%) and 88% (range 42%-100%), respectively, as well as mean adherence rates of 18% (range 7%-42%) and 60% (range 14%-93%), respectively. These contrasting findings suggest a potential connection between improved engagement with digital components when these are integrated into an intervention with a more prominent role of the therapist, that is, in a blended format.
Meta-Analysis Results: Treatment Versus Control Dyads
Across CBT-based RCTs, symptom reduction was observed for both depression and anxiety—although the reduction in anxiety symptoms was not substantial. Our result contrasts with overall findings on effectiveness of digital-only interventions exclusively addressing anxiety [67], which indicate effective outcomes. However, a subgroup analysis in that study confirmed similar ESs of both digital and face-to-face anxiety treatments. The lack of significance of our results might reflect the fact that only 1 included study addressed anxiety as a primary intervention outcome, while the other 4 interventions primarily targeted posttraumatic stress disorder, Fear of Cancer Recurrence, or depression. This suggests that transdiagnostic interventions may not be sufficient for treating anxiety—even with therapist guidance.
Meta-Analysis Results: BT Treatment Outcomes Versus the BT Model
Our analysis indicated that interventions that delivered face-to-face sessions for depression and anxiety in a lower ratio (≤50%) and in a lower number (≤6) had higher, statistically significant overall ESs. As the ratio of face-to-face sessions was similar in core or supplementary models, it is unclear what role digital sessions played in the delivery of therapeutic content compared with simply supplementing face-to-face sessions. Moreover, ESs for depression and anxiety in supplementary designs (Cohen d=–0.75 and Cohen d=–0.87, respectively) were higher than those in core designs (Cohen d=–0.53 and Cohen d=–0.6, respectively). Those findings suggest that therapeutic content may achieve better results when introduced by therapists and reinforced digitally—a characteristic of supplementary models, in which the digital component extends or reinforces face-to-face content. In addition, supplementary models might provide a more seamless transition between face-to-face and digital content as therapists can identify and discuss challenging topics with patients before they go on the web, what could result in enhanced patient engagement, adherence and treatment results. This argument is supported by studies on participants’ preference for BT models that enable greater therapist-patient interaction [21,50,68,69]. In addition, participants’ views reported across our study also suggest that improved digital access and support from therapist facilitated BT engagement.
The higher ESs of supplementary versus core designs may also reflect the therapists’ preference for face-to-face contact. This argument finds support in studies on health professionals’ preferences regarding face-to-face versus digital delivery, both in blended [68,70] and digital-only [20,71] interventions. Those studies suggest that, despite recognizing the advantages of digital interventions, professionals perceive face-to-face delivery as more attractive than digital delivery, which could influence the endorsement of digital therapy delivery as a supplement. This suggests that therapists might feel more comfortable engaging with and promoting the digital arm in a supplementary way.
In addition, it is possible that both therapists and patients expect the “bulk” of the therapeutic content to be delivered face to face in blended interventions, explaining why we found BT core models to be less efficacious than supplementary. Therapy expectations would also help explain the contrast of our results with research [67,72] on using digital therapy alone for depression and anxiety, which found digital interventions to be as good as or better than face-to-face interventions. Perhaps because patients engaging in digital-only treatment would expect therapeutic content to be delivered digitally, as there is no face-to-face option, they fare better on the digital component than they would in a BT model.
Optimizing Effectiveness, Time, and Resources in BT Treatment
One aim of BT interventions [24] is to enable better balance between treatment effects; patient engagement; treatment time; and the use of resources for both patients and therapists. BT models with integrated, core, alternate, and standardized designs allow for optimized treatment delivery. However, the results of our meta-analysis suggest that supplementary BT models are more effective. Considering these arguments, perhaps a midway alternative would be to promote a more digitally focused role of the therapist in a blended design. Following this idea, therapists would support and encourage patients to complete digital content as an enhancing adjunct to face-to-face contact—and not only as an “add-on” feature. A more digitally focused role of the therapist might promote increased patient engagement, enabling improved outcomes with lower doses of face-to-face treatment.
Study Limitations
We optimized database search terms with the assistance of a librarian; however, it is possible that eligible studies were not included in this review. In addition, the analysis did not assess the potential impact of heterogeneities found among selected studies on the variables analyzed, for example, whether different populations, settings, or therapeutic approach applied in the interventions might affect uptake or adherence or even the way blended sessions are delivered. Furthermore, the small number of studies included in our meta-analysis impacted the breadth of our results. In addition, there were limited studies describing intervention structure and content of both face-to-face and digital components in detail. Despite having contacted authors regarding missing data, several gaps remained on key variables investigated (eg, number and time of face-to-face and digital sessions, adherence parameters, and acceptability of intervention), which impacted the depth of analysis. Hence, the outcomes reported in this study should be interpreted with caution.
Recommendations
Despite growing evidence regarding BT efficacy, the lack of clearer, detailed data reporting on its structure and content poses challenges to scientific reproducibility of BT, possibly affecting its implementation success. Details related to the number, time, and distribution of sessions; specific content of both digital and face-to-face sessions, as well as the role, relevance, and influence of the digital component within the therapy plan; feedback on face-to-face and digital session content; and the use of assigned digital materials as well as the perception of its usefulness from the perspective of both therapists and patients are examples of useful data that are not adequately reported. We recommend that future studies include a more detailed reporting of methodology, particularly regarding the structure and content of sessions.
Conclusions
This systematic review examined blended models for the treatment of psychological disorders to identify what aspects of BT underpin effective treatment and improved engagement. Evidence suggests that implementing an integrated model is feasible in the treatment of psychological disorders. BT was reported as being either more effective or noninferior to face-to-face treatment, particularly when applied to the treatment of anxiety and depression. BT interventions studied reported high mean uptake and adherence rates, showing promise in improving engagement to treatment. Higher ESs were found for depression and anxiety outcomes in interventions with integrated, supplementary models; with a lower number of face-to-face sessions; and with a lower ratio of face-to-face versus digital sessions, suggesting that combining a more digitally focused therapist role with fewer face-to-face sessions can be effective and increase access to treatment.
To support improved reporting, we have developed a taxonomy for BT models based on the key themes identified in this review regarding model structure and components. Future studies detailing the structure and content of BT models may help identify suitable models for the treatment of different psychological disorders.
Acknowledgments
The Psycho-oncology Co-operative Research Group supported the development of this research. The Psycho-oncology Co-operative Research Group is funded by Cancer Australia through their Support for Clinical Trials Funding Scheme.
Abbreviations
- BT
blended therapy
- CBT
cognitive behavioral therapy
- ES
effect size
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCT
randomized controlled trial
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Database searches: examples.
Quality assessment.
Blended therapy structure: content described.
Uptake: adherence described.
Meta-analyses data: graphs.
Footnotes
Authors' Contributions: KFN-Z, HLS, PB, LB, and JMS were responsible for conceptualization and protocol development. The literature search was conducted by KFN-Z and JMS, and study selection was carried out by KFN-Z, JMS, and PB. Data analysis was performed by KFN-Z and JMS. The initial draft was prepared by KFN-Z and JMS, and all authors (KFN-Z, HS, PB, LB, and JMS) participated in reviewing and editing the draft.
Conflicts of Interest: None declared.
References
- 1.Comprehensive mental health action plan 2013-2030. World Health Organization (WHO) 2021. [2024-04-29]. https://www.who.int/publications/i/item/9789240031029 .
- 2.World health statistics 2022: monitoring health for the SDGs, sustainable development goals. World Health Organization (WHO) 2022. [2024-04-29]. https://www.who.int/publications/i/item/9789240051157 .
- 3.The WHO special initiative for mental health (2019-2023): universal health coverage for mental health. World Health Organization (WHO) 2019. [2024-04-29]. https://iris.who.int/handle/10665/310981 .
- 4.Guzman D, Ann-Yi S, Bruera E, Wu J, Williams JL, Najera J, Raznahan M, Carmack CL. Enhancing palliative care patient access to psychological counseling through outreach telehealth services. Psychooncology. 2020 Jan 10;29(1):132–8. doi: 10.1002/pon.5270. [DOI] [PubMed] [Google Scholar]
- 5.Sinclair C, Holloway K, Riley G, Auret K. Online mental health resources in rural Australia: clinician perceptions of acceptability. J Med Internet Res. 2013 Sep;15(9):e193. doi: 10.2196/jmir.2772. http://www.jmir.org/2013/9/e193/ v15i9e193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hadjistavropoulos HD, Schneider LH, Hadjistavropoulos T, Titov N, Dear BF. Effectiveness, acceptability and feasibility of an internet-delivered cognitive behavioral pain management program in a routine online therapy clinic in Canada. Can J Pain. 2018 Mar 21;2(1):62–73. doi: 10.1080/24740527.2018.1442675. https://europepmc.org/abstract/MED/35005367 .1442675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hedman E, Ljótsson B, Lindefors N. Cognitive behavior therapy via the internet: a systematic review of applications, clinical efficacy and cost-effectiveness. Expert Rev Pharmacoecon Outcomes Res. 2012 Dec;12(6):745–64. doi: 10.1586/erp.12.67. [DOI] [PubMed] [Google Scholar]
- 8.Christensen H, Batterham P, Calear A. Online interventions for anxiety disorders. Curr Opin Psychiatry. 2014 Jan;27(1):7–13. doi: 10.1097/YCO.0000000000000019. [DOI] [PubMed] [Google Scholar]
- 9.Hollinghurst S, Peters TJ, Kaur S, Wiles N, Lewis G, Kessler D. Cost-effectiveness of therapist-delivered online cognitive-behavioural therapy for depression: randomised controlled trial. Br J Psychiatry. 2010 Oct 02;197(4):297–304. doi: 10.1192/bjp.bp.109.073080.S0007125000253142 [DOI] [PubMed] [Google Scholar]
- 10.Saddichha S, Al-Desouki M, Lamia A, Linden IA, Krausz M. Online interventions for depression and anxiety - a systematic review. Health Psychol Behav Med. 2014 Jan 01;2(1):841–81. doi: 10.1080/21642850.2014.945934. http://europepmc.org/abstract/MED/25750823 .945934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Andersson G, Topooco N, Havik O, Nordgreen T. Internet-supported versus face-to-face cognitive behavior therapy for depression. Expert Rev Neurother. 2016 Dec 15;16(1):55–60. doi: 10.1586/14737175.2015.1125783. [DOI] [PubMed] [Google Scholar]
- 12.Emmelkamp PM. Effectiveness of cybertherapy in mental health: a critical appraisal. Stud Health Technol Inform. 2011;167:3–8. [PubMed] [Google Scholar]
- 13.Bisby MA, Karin E, Hathway T, Scott AJ, Heriseanu AI, Dudeney J, Fisher A, Gandy M, Cross S, Staples L, Titov N, Dear BF. A meta-analytic review of randomized clinical trials of online treatments for anxiety: inclusion/exclusion criteria, uptake, adherence, dropout, and clinical outcomes. J Anxiety Disord. 2022 Dec;92:102638. doi: 10.1016/j.janxdis.2022.102638.S0887-6185(22)00111-6 [DOI] [PubMed] [Google Scholar]
- 14.Cross SP, Karin E, Staples LG, Bisby MA, Ryan K, Duke G, Nielssen O, Kayrouz R, Fisher A, Dear BF, Titov N. Factors associated with treatment uptake, completion, and subsequent symptom improvement in a national digital mental health service. Internet Interv. 2022 Mar;27:100506. doi: 10.1016/j.invent.2022.100506. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(22)00013-6 .S2214-7829(22)00013-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Beatty L, Kemp E, Koczwara B. Finding my way from clinical trial to open access dissemination: comparison of uptake, adherence, and psychosocial outcomes of an online program for cancer-related distress. Support Care Cancer. 2022 Jun 22;30(10):7935–42. doi: 10.1007/S00520-022-07205-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fleming T, Bavin L, Lucassen M, Stasiak K, Hopkins S, Merry S. Beyond the trial: systematic review of real-world uptake and engagement with digital self-help interventions for depression, low mood, or anxiety. J Med Internet Res. 2018 Jun 06;20(6):e199. doi: 10.2196/jmir.9275. http://www.jmir.org/2018/6/e199/ v20i6e199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lipschitz JM, Van Boxtel R, Torous J, Firth J, Lebovitz JG, Burdick KE, Hogan TP. Digital mental health interventions for depression: scoping review of user engagement. J Med Internet Res. 2022 Oct 14;24(10):e39204. doi: 10.2196/39204. https://www.jmir.org/2022/10/e39204/ v24i10e39204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Klein B, Cook S. Preferences for e-mental health services amongst an online Australian sample? E J Appl Psychol. 2010 May 25;6(1):28–39. doi: 10.7790/ejap.v6i1.184. [DOI] [Google Scholar]
- 19.Wallin EE, Mattsson S, Olsson EM. The preference for internet-based psychological interventions by individuals without past or current use of mental health treatment delivered online: a survey study with mixed-methods analysis. JMIR Ment Health. 2016;3(2):e25. doi: 10.2196/mental.5324. http://mental.jmir.org/2016/2/e25/ v3i2e25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Davies F, Shepherd HL, Beatty L, Clark B, Butow P, Shaw J. Implementing web-based therapy in routine mental health care: systematic review of health professionals' perspectives. J Med Internet Res. 2020 Jul 23;22(7):e17362. doi: 10.2196/17362. https://www.jmir.org/2020/7/e17362/ v22i7e17362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.van der Vaart R, Witting M, Riper H, Kooistra L, Bohlmeijer ET, van Gemert-Pijnen LJ. Blending online therapy into regular face-to-face therapy for depression: content, ratio and preconditions according to patients and therapists using a Delphi study. BMC Psychiatry. 2014 Dec 14;14:355. doi: 10.1186/s12888-014-0355-z.s12888-014-0355-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Wentzel J, van der Vaart R, Bohlmeijer ET, van Gemert-Pijnen JE. Mixing online and face-to-face therapy: how to benefit from blended care in mental health care. JMIR Ment Health. 2016 Feb 09;3(1):e9. doi: 10.2196/mental.4534. https://mental.jmir.org/2016/1/e9/ v3i1e9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kooistra LC, Ruwaard J, Wiersma JE, van Oppen P, van der Vaart R, van Gemert-Pijnen JE, Riper H. Development and initial evaluation of blended cognitive behavioural treatment for major depression in routine specialized mental health care. Internet Interv. 2016 May;4:61–71. doi: 10.1016/j.invent.2016.01.003. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(16)00003-8 .S2214-7829(16)00003-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Erbe D, Eichert HC, Riper H, Ebert DD. Blending face-to-face and internet-based interventions for the treatment of mental disorders in adults: systematic review. J Med Internet Res. 2017 Sep 15;19(9):e306. doi: 10.2196/jmir.6588. https://www.jmir.org/2017/9/e306/ v19i9e306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fitzpatrick M, Nedeljkovic M, Abbott JA, Kyrios M, Moulding R. "Blended" therapy: the development and pilot evaluation of an internet-facilitated cognitive behavioral intervention to supplement face-to-face therapy for hoarding disorder. Internet Interv. 2018 Jun;12:16–25. doi: 10.1016/j.invent.2018.02.006. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(17)30039-8 .S2214-7829(17)30039-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kooistra LC, Wiersma JE, Ruwaard J, Neijenhuijs K, Lokkerbol J, van Oppen P, Smit F, Riper H. Cost and effectiveness of blended versus standard cognitive behavioral therapy for outpatients with depression in routine specialized mental health care: pilot randomized controlled trial. J Med Internet Res. 2019 Oct 29;21(10):e14261. doi: 10.2196/14261. https://www.jmir.org/2019/10/e14261/ v21i10e14261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kleiboer A, Smit J, Bosmans J, Ruwaard J, Andersson G, Topooco N, Berger T, Krieger T, Botella C, Baños R, Chevreul K, Araya R, Cerga-Pashoja A, Cieślak R, Rogala A, Vis C, Draisma S, van Schaik A, Kemmeren L, Ebert D, Berking M, Funk B, Cuijpers P, Riper H. European COMPARative effectiveness research on blended depression treatment versus treatment-as-usual (E-COMPARED): study protocol for a randomized controlled, non-inferiority trial in eight European countries. Trials. 2016 Aug 03;17(1):387. doi: 10.1186/s13063-016-1511-1. https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-016-1511-1 .10.1186/s13063-016-1511-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar 29;372:n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Covidence systematic review software. Veritas Health Innovation. [2024-04-29]. https://www.covidence.org/
- 30.Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006 Jan;3(2):77–101. doi: 10.1191/1478088706qp063oa. [DOI] [Google Scholar]
- 31.Neuendorf KA. The Content Analysis Guidebook. 2nd edition. Thousand Oaks, CA: Sage Publications; 2017. [Google Scholar]
- 32.Comprehensive meta-analysis. Version 4. Biostat, Inc. 2022. [2024-04-29]. https://meta-analysis.com/
- 33.Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000 Jun;56(2):455–63. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- 34.Study quality assessment tools. The National Heart, Lung, and Blood Institute (NHLBI) 2021. [2024-04-29]. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools .
- 35.CASP checklist: CASP qualitative studies checklist. Critical Appraisal Skills Programme. [2024-04-29]. https://casp-uk.net/casp-tools-checklists/qualitative-studies-checklist/
- 36.Hong Q, Pluye P, Fàbregues S, Bartlett G, Boardman F. Mixed methods appraisal tool (MMAT) version 2018. Department of Family Medicine. 2018. [2024-04-29]. http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf .
- 37.Høifødt RS, Lillevoll KR, Griffiths KM, Wilsgaard T, Eisemann M, Waterloo K, Kolstrup N. The clinical effectiveness of web-based cognitive behavioral therapy with face-to-face therapist support for depressed primary care patients: randomized controlled trial. J Med Internet Res. 2013 Aug;15(8):e153. doi: 10.2196/jmir.2714. http://www.jmir.org/2013/8/e153/ v15i8e153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kok RN, van Straten A, Beekman AT, Cuijpers P. Short-term effectiveness of web-based guided self-help for phobic outpatients: randomized controlled trial. J Med Internet Res. 2014 Sep 29;16(9):e226. doi: 10.2196/jmir.3429. https://www.jmir.org/2014/9/e226/ v16i9e226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Månsson KN, Skagius RE, Gervind E, Dahlin M, Andersson G. Development and initial evaluation of an internet-based support system for face-to-face cognitive behavior therapy: a proof of concept study. J Med Internet Res. 2013 Dec 10;15(12):e280. doi: 10.2196/jmir.3031. http://www.jmir.org/2013/12/e280/ v15i12e280 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Månsson KN, Klintmalm H, Nordqvist R, Andersson G. Conventional cognitive behavioral therapy facilitated by an internet-based support system: feasibility study at a psychiatric outpatient clinic. JMIR Res Protoc. 2017 Aug 24;6(8):e158. doi: 10.2196/resprot.6035. https://www.researchprotocols.org/2017/8/e158/ v6i8e158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Romijn G, Provoost S, Batelaan N, Koning J, van Balkom A, Riper H. Does it blend? Exploring therapist fidelity in blended CBT for anxiety disorders. Internet Interv. 2021 Sep;25:100418. doi: 10.1016/j.invent.2021.100418. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(21)00058-0 .S2214-7829(21)00058-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Jacmon J, Malouff JM, Taylor N. Treatment of major depression: effectiveness of cognitive behavior therapy with an internet course as a central component. E J Appl Psychol. 2009;5(2):1–8. doi: 10.7790/ejap.v5i2.153. [DOI] [Google Scholar]
- 43.Askjer S, Mathiasen K. The working alliance in blended versus face-to-face cognitive therapy for depression: a secondary analysis of a randomized controlled trial. Internet Interv. 2021 Sep;25:100404. doi: 10.1016/j.invent.2021.100404. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(21)00044-0 .S2214-7829(21)00044-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Mathiasen K, Andersen TE, Lichtenstein MB, Ehlers LH, Riper H, Kleiboer A, Roessler KK. The clinical effectiveness of blended cognitive behavioral therapy compared with face-to-face cognitive behavioral therapy for adult depression: randomized controlled noninferiority trial. J Med Internet Res. 2022 Sep 07;24(9):e36577. doi: 10.2196/36577. https://www.jmir.org/2022/9/e36577/ v24i9e36577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Berger T, Krieger T, Sude K, Meyer B, Maercker A. Evaluating an e-mental health program ("deprexis") as adjunctive treatment tool in psychotherapy for depression: results of a pragmatic randomized controlled trial. J Affect Disord. 2018 Dec;227:455–62. doi: 10.1016/j.jad.2017.11.021.S0165-0327(17)31255-7 [DOI] [PubMed] [Google Scholar]
- 46.Bisson JI, Ariti C, Cullen K, Kitchiner N, Lewis C, Roberts NP, Simon N, Smallman K, Addison K, Bell V, Brookes-Howell L, Cosgrove S, Ehlers A, Fitzsimmons D, Foscarini-Craggs P, Harris SR, Kelson M, Lovell K, McKenna M, McNamara R, Nollett C, Pickles T, Williams-Thomas R. Guided, internet based, cognitive behavioural therapy for post-traumatic stress disorder: pragmatic, multicentre, randomised controlled non-inferiority trial (RAPID) BMJ. 2022 Jun 16;377:e069405. doi: 10.1136/bmj-2021-069405. http://www.bmj.com/lookup/pmidlookup?view=long&pmid=35710124 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Cloitre M, Amspoker AB, Fletcher TL, Hogan JB, Jackson C, Jacobs A, Shammet R, Speicher S, Wassef M, Lindsay J. Comparing the ratio of therapist support to internet sessions in a blended therapy delivered to trauma-exposed veterans: quasi-experimental comparison study. JMIR Ment Health. 2022 Apr 27;9(4):e33080. doi: 10.2196/33080. https://mental.jmir.org/2022/4/e33080/ v9i4e33080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Duffy D, Enrique A, Connell S, Connolly C, Richards D. Internet-delivered cognitive behavior therapy as a prequel to face-to-face therapy for depression and anxiety: a naturalistic observation. Front Psychiatry. 2019 Jan 9;10:902. doi: 10.3389/fpsyt.2019.00902. https://europepmc.org/abstract/MED/31998149 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Etzelmueller A, Radkovsky A, Hannig W, Berking M, Ebert DD. Patient's experience with blended video- and internet based cognitive behavioural therapy service in routine care. Internet Interv. 2018 Jun;12:165–175. doi: 10.1016/j.invent.2018.01.003. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(17)30089-1 .S2214-7829(17)30089-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Kemmeren LL, van Schaik A, Smit JH, Ruwaard J, Rocha A, Henriques M, Ebert DD, Titzler I, Hazo J, Dorsey M, Zukowska K, Riper H. Unraveling the black box: exploring usage patterns of a blended treatment for depression in a multicenter study. JMIR Ment Health. 2019 Jul 25;6(7):e12707. doi: 10.2196/12707. https://mental.jmir.org/2019/7/e12707/ v6i7e12707 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Kenter R, Warmerdam L, Brouwer-Dudokdewit C, Cuijpers P, van Straten A. Guided online treatment in routine mental health care: an observational study on uptake, drop-out and effects. BMC Psychiatry. 2013 Jan 31;13:43. doi: 10.1186/1471-244X-13-43. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-13-43 .1471-244X-13-43 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Kenter RM, van de Ven PM, Cuijpers P, Koole G, Niamat S, Gerrits RS, Willems M, van Straten A. Costs and effects of internet cognitive behavioral treatment blended with face-to-face treatment: results from a naturalistic study. Internet Interv. 2015 Mar;2(1):77–83. doi: 10.1016/j.invent.2015.01.001. [DOI] [Google Scholar]
- 53.Kooistra L, Ruwaard J, Wiersma J, van Oppen P, Riper H. Working alliance in blended versus face-to-face cognitive behavioral treatment for patients with depression in specialized mental health care. J Clin Med. 2020 Jan 27;9(2):347. doi: 10.3390/jcm9020347. https://www.mdpi.com/resolver?pii=jcm9020347 .jcm9020347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lungu A, Jun JJ, Azarmanesh O, Leykin Y, Chen CE. Blended care-cognitive behavioral therapy for depression and anxiety in real-world settings: pragmatic retrospective study. J Med Internet Res. 2020 Jul 06;22(7):e18723. doi: 10.2196/18723. https://www.jmir.org/2020/7/e18723/ v22i7e18723 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Ly KH, Topooco N, Cederlund H, Wallin A, Bergström J, Molander O, Carlbring P, Andersson G. Smartphone-supported versus full behavioural activation for depression: a randomised controlled trial. PLoS One. 2015 May 26;10(5):e0126559. doi: 10.1371/journal.pone.0126559. https://dx.plos.org/10.1371/journal.pone.0126559 .PONE-D-14-40400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Mol M, Dozeman E, Provoost S, van Schaik A, Riper H, Smit JH. Behind the scenes of online therapeutic feedback in blended therapy for depression: mixed-methods observational study. J Med Internet Res. 2018 May 03;20(5):e174. doi: 10.2196/jmir.9890. https://www.jmir.org/2018/5/e174/ v20i5e174 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Nakao S, Nakagawa A, Oguchi Y, Mitsuda D, Kato N, Nakagawa Y, Tamura N, Kudo Y, Abe T, Hiyama M, Iwashita S, Ono Y, Mimura M. Web-based cognitive behavioral therapy blended with face-to-face sessions for major depression: randomized controlled trial. J Med Internet Res. 2018 Sep 21;20(9):e10743. doi: 10.2196/10743. https://www.jmir.org/2018/9/e10743/ v20i9e10743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Romijn G, Batelaan N, Koning J, van Balkom A, de Leeuw A, Benning F, Hakkaart van Roijen L, Riper H. Acceptability, effectiveness and cost-effectiveness of blended cognitive-behavioural therapy (bCBT) versus face-to-face CBT (ftfCBT) for anxiety disorders in specialised mental health care: a 15-week randomised controlled trial with 1-year follow-up. PLoS One. 2021;16(11):e0259493. doi: 10.1371/journal.pone.0259493. https://dx.plos.org/10.1371/journal.pone.0259493 .PONE-D-19-32776 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Tarp K, Nielsen AS. Patient perspectives on videoconferencing-based treatment for alcohol use disorders. Alcohol Treat Q. 2017 Jul 17;35(4):344–358. doi: 10.1080/07347324.2017.1348785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Thase ME, Wright JH, Eells TD, Barrett MS, Wisniewski SR, Balasubramani G, McCrone P, Brown GK. Improving the efficiency of psychotherapy for depression: computer-assisted versus standard CBT. Am J Psychiatry. 2018 Mar 01;175(3):242–50. doi: 10.1176/appi.ajp.2017.17010089. https://europepmc.org/abstract/MED/28969439 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.van de Wal M, Thewes B, Gielissen M, Speckens A, Prins J. Efficacy of blended cognitive behavior therapy for high fear of recurrence in breast, prostate, and colorectal cancer survivors: the SWORD study, a randomized controlled trial. J Clin Oncol. 2017 Jul 01;35(19):2173–83. doi: 10.1200/JCO.2016.70.5301. [DOI] [PubMed] [Google Scholar]
- 62.Vernmark K, Hesser H, Topooco N, Berger T, Riper H, Luuk L, Backlund L, Carlbring P, Andersson G. Working alliance as a predictor of change in depression during blended cognitive behaviour therapy. Cogn Behav Ther. 2019 Jul 29;48(4):285–299. doi: 10.1080/16506073.2018.1533577. http://liu.diva-portal.org/smash/get/diva2:1270107/FULLTEXT01.pdf . [DOI] [PubMed] [Google Scholar]
- 63.Witlox M, Garnefski N, Kraaij V, de Waal MW, Smit F, Bohlmeijer E, Spinhoven P. Blended acceptance and commitment therapy versus face-to-face cognitive behavioral therapy for older adults with anxiety symptoms in primary care: pragmatic single-blind cluster randomized trial. J Med Internet Res. 2021 Mar 26;23(3):e24366. doi: 10.2196/24366. https://www.jmir.org/2021/3/e24366/ v23i3e24366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Wu MS, Chen SY, Wickham RE, O'Neil-Hart S, Chen C, Lungu A. Outcomes of a blended care coaching program for clients presenting with moderate levels of anxiety and depression: pragmatic retrospective study. JMIR Ment Health. 2021 Oct 21;8(10):e32100. doi: 10.2196/32100. https://mental.jmir.org/2021/10/e32100/ v8i10e32100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Wu MS, Wickham RE, Chen SY, Chen C, Lungu A. Examining the impact of digital components across different phases of treatment in a blended care cognitive behavioral therapy intervention for depression and anxiety: pragmatic retrospective study. JMIR Form Res. 2021 Dec 17;5(12):e33452. doi: 10.2196/33452. https://formative.jmir.org/2021/12/e33452/ v5i12e33452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Barkham M, Connell J, Stiles WB, Miles JN, Margison F, Evans C, Mellor-Clark J. Dose-effect relations and responsive regulation of treatment duration: the good enough level. J Consult Clin Psychol. 2006;74(1):160–167. doi: 10.1037/0022-006x.74.1.160. [DOI] [PubMed] [Google Scholar]
- 67.Pauley D, Cuijpers P, Papola D, Miguel C, Karyotaki E. Two decades of digital interventions for anxiety disorders: a systematic review and meta-analysis of treatment effectiveness. Psychol Med. 2023 Jan 28;53(2):567–579. doi: 10.1017/S0033291721001999. https://europepmc.org/abstract/MED/34047264 .S0033291721001999 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Titzler I, Saruhanjan K, Berking M, Riper H, Ebert DD. Barriers and facilitators for the implementation of blended psychotherapy for depression: a qualitative pilot study of therapists' perspective. Internet Interv. 2018 Jun;12:150–164. doi: 10.1016/j.invent.2018.01.002. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(17)30090-8 .S2214-7829(17)30090-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Doukani A, Free C, Araya R, Michelson D, Cerga-Pashoja A, Kakuma R. Practitioners' experience of the working alliance in a blended cognitive-behavioural therapy intervention for depression: qualitative study of barriers and facilitators. BJPsych Open. 2022 Jul 25;8(4):e142. doi: 10.1192/bjo.2022.546. https://europepmc.org/abstract/MED/35876079 .S2056472422005464 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Schuster R, Pokorny R, Berger T, Topooco N, Laireiter AR. The advantages and disadvantages of online and blended therapy: survey study amongst licensed psychotherapists in Austria. J Med Internet Res. 2018 Dec 18;20(12):e11007. doi: 10.2196/11007.v20i12e11007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Davies F, Harris M, Shepherd HL, Butow P, Beatty L, Kemp E, Shaw J. Promise unfulfilled: implementing web-based psychological therapy in routine cancer care, a qualitative study of oncology health professionals' attitudes. Psychooncology. 2022 Jul 22;31(7):1127–1135. doi: 10.1002/pon.5900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Luo C, Sanger N, Singhal N, Pattrick K, Shams I, Shahid H, Hoang P, Schmidt J, Lee J, Haber S, Puckering M, Buchanan N, Lee P, Ng K, Sun S, Kheyson S, Chung DC, Sanger S, Thabane L, Samaan Z. Addendum to a comparison of electronically-delivered and face to face cognitive behavioural therapies in depressive disorders: a systematic review and meta-analysis. EClinicalMedicine. 2020 Oct;27:100580. doi: 10.1016/j.eclinm.2020.100580. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Database searches: examples.
Quality assessment.
Blended therapy structure: content described.
Uptake: adherence described.
Meta-analyses data: graphs.